

Abstract
Objective
To characterize patients who utilize services for migraine in a large integrated health care network, and describe patterns of care and utilization.
Background
Within health care systems, migraine is a common reason for seeking primary and neurology care, but relatively little is documented about who seeks care and the factors that explain variation in utilization.
Methods
We conducted a retrospective cohort study using electronic health record (EHR) data from Sutter Health primary care (PC) patients who had at least one office visit to a PC clinic between 2013 and 2017. Migraine status was ascertained from diagnosis codes and medication orders. Control status was assigned to those with no evidence of care for any type of headache. We divided the primary care migraine cohort into two groups: those who received all their care for migraine from PC (denoted PC‐M) and those who had ≥1 encounter with a neurologist for migraine (denoted N‐M). Migraine cases were also designated as having preexisting migraine if they had an encounter with a migraine diagnosis within (±) 6 months of their first study period PC visit and, otherwise, designated as first migraine consult. Two levels of contrasts included: patients with migraine and controls; and within the group of patients with migraine, PC‐M and N‐M groups. Comorbid conditions were determined from EHR encounter diagnosis codes.
Results
We identified 94,149 patients with migraine (including 21,525 N‐M and 72,624 PC‐M) and 1,248,763 controls. Comorbidities: Proportions of psychiatric [29.8% (n = 28,054) vs. 11.8% (n = 147,043)], autoimmune [(4.4% (n = 4162) vs. 2.6% (n = 31,981)], pain [13.2% (n = 12,439) vs. 5.8% (n = 72,049)], respiratory [24.6% (n = 23,186) vs. 12.3% (n = 153,692)], neurologic [2.9% (n = 2688) vs. 0.9% (n = 11,321)], and cerebrovascular [1.0% (n = 945) vs. 0.6% (n = 7500)] conditions were higher in the migraine group compared to controls, all p < 0.001. Among patients with migraine, the N‐M group was similar to the PC‐M group in sex, age, ethnicity, and marital status, but were more likely to have preexisting migraine (49.9% (n = 10,734) vs. 36.2% (n = 26,317), p < 0.001). Proportions of comorbid conditions were higher among the N‐M group than the PC‐M group {psychiatric [38.5% (n = 8291) vs. 27.2% (n = 19,763)], autoimmune [6.3% (n = 1365) vs. 3.9% (n = 2797)], pain [19.6% (n = 4218) vs. 11.3% (n = 8211)], respiratory [30.3% (n = 6516) vs. 23.0% (n = 16,670)], neurologic [6.0% (n = 1288) vs. 1.9% (n = 1400)], cardiovascular [9.7% (n = 2091) vs. 7.0% (n = 5076)], and cerebrovascular [2.3% (n = 500) vs. 0.6% (n = 445)], all p < 0.001}. Medications: During the study period, 82.6% (n = 77,762) of patients with migraine received ≥1 prescription order for an acute migraine medication [89.4% (n = 19,250) of N‐M vs. 80.6% (n = 58,512) of PC]. Opioids were prescribed to 52.9% (n = 49,837) of patients with migraine [63.5% (n = 13,669) for N‐M and 49.8% (n = 36,168) for PC‐M patients). During the study period, 61.4% (n = 57,810) of patients received ≥1 prescription for a migraine preventive medication [81.4% (n = 17,521) of N‐M and 55.5% (n = 40,289) of PC‐M patients]. The most commonly prescribed classes of preventive medications were antidepressants.
Conclusions
Among patients with migraine in a large health system, those who were also cared for in neurology were more likely to receive both acute and preventive medication migraine orders than those patients who did not see a neurologist, with triptans and antidepressants the most commonly prescribed classes of acute and preventive pharmacotherapies, respectively. Opioids were prescribed to approximately half of the total sample and more common in the N‐M group. Adjusting for demographics, patients with migraine had higher rates of nearly every comorbidity we assessed and were more likely to utilize services compared to those without migraine. Overall, patients with migraine also cared for in neurology practices used more of all health care resource types under consideration and had more medical issues, which may be due in some part to a more severe, frequent and disabling disease state compared to those who sought care exclusively from PC practices.
Keywords: electronic health record, headache, health care system, migraine, neurology, primary care
Abbreviations
- aOR
adjusted odds ratio
- aP
adjusted probability
- DVT
deep vein thrombosis
- ED
emergency department
- EHR
electronic health record
- FC
frequent consulters
- FMC
first migraine consult
- GERD
gastro‐esophageal reflux disorder
- IBS
irritable bowel syndrome
- ICD9/10
International Classification of Disease
- MAST
Migraine in America Symptoms and Treatment
- MPR
Medication Possession Ration
- N‐M
neurologist for migraine
- NH
non‐Hispanic
- PC
primary care
- PC‐M
primary care for migraine
- PCP
primary care provider
- PE
pulmonary embolism
- SH
Sutter Health
- US
United States
INTRODUCTION
Migraine is a common and often disabling chronic neurologic disease affecting more than one billion people globally, and an estimated 12% of the United States (US) population (nearly 40 million). 1 , 2 It is the most common neurological reason for primary care (PC) visits, with approximately 3% of the general population consulting PC for migraine on an annual basis. 3 Migraine is a common reason for referral from PC—referrals are associated with severity of illness, frequency of PC consultation, and rates of psychiatric comorbidities 4 , 5 ; It is also a common reason for neurology visits. 4 , 6 , 7 , 8 Despite its import as a reason for health care use, there is relatively little data comparing characteristics and the use of medical care in patients with and without migraine in health care networks or comparing patients in health care system settings with those in the population. 9 , 10 , 11 There are also limited data comparing the characteristics or treatment patterns of patients with migraine who are treated in specialty care with those treated in PC settings. Most of the available data on patterns of migraine treatment come from epidemiologic surveys, clinical trials, or analysis of medical and pharmacy claims data. 5 , 12 All of these sources have strengths and limitations. One limitation of epidemiologic surveys is that consultation, diagnosis, and treatment status are based on patient self‐report without corroboration from objective sources. Studies that rely on medical and pharmacy claims data are prone to error compared to electronic health record (EHR) data and also are less accurate and complete than EHR data in defining the indication for care. 13 , 14
Within health care systems, migraine is a common reason for consultation both in PC and in neurologic settings; however, there is little documented about how patients with migraine utilize care. 15 , 16 , 17 This is due at least in part to the fact that relatively little research has been conducted using EHR data to characterize persons treated in PC settings and in neurologic practices and to contrast patient profiles, patterns of treatment and outcomes in these two care settings.
Migraine management can be a complex and multidimensional process starting with accurate diagnosis and proceeding through treatment planning and ongoing treatment optimization. Treatment of migraine may include acute and preventive therapies using both pharmacologic and non‐medication approaches. The overwhelming majority of patients with migraine use acute medications. Most use over‐the‐counter medications and many use prescription medications, some of which are not migraine specific. 12 , 16 , 18 , 19 , 20 , 21 Opioids are widely used by those treated with prescription medications though they are not recommended in treatment guidelines in part because long‐term use has been shown to worsen headaches. 12 , 16 , 18 , 22 , 23 , 24 Preventive treatments are used to decrease the frequency and severity of migraine and are recommended for individuals with four or more monthly migraine days, particularly if headaches interfere with function despite optimized acute treatment. 25 Given the many barriers to preventive treatment use it is not surprising that these treatments are underused. 2 , 12 Non‐pharmacologic treatments for migraine management are equally as important in a treatment plan but there are many reasons that these therapies are not initiated or have poor adherence. 26 , 27 , 28
To better understand health care use for migraine, we analyzed EHR data from a large integrated health care network in Northern California from 2013 to 2017. In this study, we identified a cohort of PC patients who sought care for migraine from Sutter Health (SH) providers and a control group who sought care, but not for migraine. We compared the demographics and comorbidities of patients who sought care for migraine with those who did not. For these comparisons, we hypothesized that the demographics and presence of comorbid conditions would differ between the two groups. We also contrasted patterns of health care use, prescribing patterns and adherence in the individuals whose migraine was treated exclusively in PC with those of individuals whose migraine was also treated in a neurology clinic. For these contrasts, we hypothesized that the utilization of services, prescription orders, and adherence to medications would differ between the two groups.
METHODS
Design and setting
We conducted a retrospective cohort study using EHR data from SH PC patients. This is a primary analysis of secondary data collected for clinical purposes. SH is a large, not‐for‐profit integrated health care network serving more than 100 communities across 22 counties in Northern California. The Sutter Health Medical Network includes 272 outpatient PC practices with nearly 1200 primary care providers (PCPs), 9 neurology practices with 126 neurologists, and a diversity of other ambulatory and inpatient‐care services. Sutter Heath uses EpicCare across all of its health care delivery facilities in an integrated EHR system. All EHR data are organized around encounters or patient interactions outside of encounters. Encounters include ambulatory, inpatient, emergency department (ED), telephone, and video. External interactions include prescriptions, call‐center activities, and SH's patient web portal (MyHealth Online). For this study, we define SH PC population as patients who had at least one office visit to a PC department during the 5‐year study period from 1/1/2013 to 12/31/2017.
Identifying the cohort
From the cohort of SH PC patients, we ascertained migraine status based on diagnosis codes from utilization, medication orders, and problem list. SH migraine cases (utilizers) were identified from PC patients who met criteria below using data from the EHR, including clinic encounters (PC, neurology, or both), inpatient hospitalizations (IH), outpatient hospitalizations (OH), ED, migraine‐specific medications, and migraine noted on the problem list. We required at least one encounter in neurology with a diagnosis of migraine (International Classification of Disease [ICD9] = 346.xx or ICD10 = G43.xxx), migraine listed on the problem list, or a combination of at least two of the following: encounters for migraine (ICD9 = 346.xx or ICD10 = G43.xxx) in PC, IH, OH, ED, and prescription orders for triptans or ergots. Controls were defined as all PC patients with no EHR records containing diagnoses or medication orders as evidence of care for headache of any type. Patients with headache not otherwise specified were excluded as prior evidence suggests that this group includes a high proportion of patients with migraine, though these individuals cannot be readily identified. 29 All individuals (migraine and control) had at least one office visit during the study period. Using this EHR‐based definition, we identified 94,149 migraine patients (utilizers) and 1,248,763 controls from the SH 5‐year PC population.
Migraine subgroups
We divided the migraine cohort into two groups: PC patients who received all their care for migraine in the primary care setting (PC‐M) and primary care patients who had at least one encounter with a neurologist for migraine (N‐M). We also defined preexisting (prevalent) migraine as a patient who had an office, urgent care, or ED encounter with a migraine diagnosis within (±) 6 months of their first study‐period PC visit. Patients who do not fit the definition of preexisting are labeled as first migraine consult (FMC). By this definition, FMC patients did not have had any migraine‐related utilization within 12 months prior to their FMC. While we recognize that some FMC patients may have had migraine utilization outside the window of observation, this group represents patients new to medical care for migraine or patients who have had at least a 12‐month period without medical care for migraine.
Other variables
For all patients, we extracted EHR data on demographics (age, sex, and race), marital status, smoking and alcohol status, height and weight, medication orders and fills (from Surescripts, see below), problem list, and primary and secondary diagnoses for ambulatory, urgent care, ED, and acute care encounters. SH's EHR explicitly documents patient encounters within SH, including medication orders and the reason (i.e., indication) for the order, and, as noted, other interactions (such as the patient portal and Surescripts). Age was first considered as a continuous variable, and then, categorized into the following groups: 18–29, 30–44, 45–54, 55–64, and 65+. Race and ethnicity were defined by Hispanic identity, followed by racial group. If a patient did not self‐identify as Hispanic, we classified them based on their self‐identified race, as follows: Hispanic, non‐Hispanic (NH) Asian, NH Black, NH White, and Other. Marital status was classified into five categories, Married/Partnered, Single, Divorced/Separated, Widowed, and Other/Unknown. Common chronic and chronic‐episodic diseases were identified and coded (Y/N) if there were two or more encounter diagnoses ICD‐9/10—Clinical Modification codes during the study period. Appendix A lists the ICD codes used to identify each disease.
Medication orders
Acute and preventive migraine medication orders were extracted from the EHR according to the list in Appendix B, and are identified by indication. These orders do not provide evidence that the prescription was filled or that it was taken as directed. It should be noted that this study is from the perspective of the patient, and that we have not determined which type of provider is prescribing each medication, rather we are considering which medications are prescribed to members of each migraine group. Medication orders are presented in two ways: as mean orders per person‐year, and as percentage with order counts.
Medication dispensed—Surescripts
Surescripts is a third‐party national network connecting clinicians, EHRs, hospitals, pharmacy benefit managers, pharmacies, and technology vendors to provide comprehensive patient‐medication information at the point of care. To achieve this, each time a patient has an encounter for any reason with SH, data are transferred to the SH EHR. These data include information about all prescriptions filled by the patient including: medication name, date of fill, amount prescribed, directions for use, and number of refills regardless of which provider ordered them. This information can be used to augment the picture of medication use for each patient.
Adherence
We estimated medication adherence by calculating a medication possession ratio (MPR) for preventive medication use for each specific medication that had a reasonably large number of patients prescribed the drug. MPR includes data from patients with two or more prescriptions for the same medication, and is calculated as the days’ supply divided by the number of days between first and last prescription. MPR’s were compared between groups using two‐sample t‐tests and presented as means and 95% confidence intervals.
Person time
We defined person time as time lapsed between first and last PC visits. Prescribing rates and encounter rates are standardized by time at risk, and reported as mean number of encounters per person‐year and ratio of means between groups. For adjusted tables and models of utilization, we required a minimum of 6 months follow‐up time.
Frequent consultation
We defined frequent consulters (FC) by plotting the SH utilization and choosing a cut point of 4+ visits, based on the subjectively identified point at which the utilization leveled off.
Statistical methods
A statistical analysis plan was devised prior to conducting the study, however, this was a descriptive analysis, without intervention, and therefore, the concept of a clinically meaningful effect did not apply. Rather, the primary analyses of interest were contrasts between patients with migraine and migraine‐free controls. We hypothesized that these two groups would differ on demographics and comorbidities. Within the group of patients with migraine, we contrasted the N‐M group with the PC‐M group. We hypothesized that these two groups would also differ on utilization of services, and prescription orders and adherence. Descriptive data are summarized using customary summary measures (e.g., means, medians, percentages, and standard deviations), and comparisons were conducted using two‐sample z‐tests (proportions of comorbidities and medication use), and two‐sample t‐tests (medication and utilization per person‐year), and Wilcoxon rank sum tests (age) for continuous variables and chi‐square tests (sex, race, ethnicity, and marital status) for categorical variables. All tests were two‐sided, with an overall significance level set at p < 0.05. Where relevant, regression (linear and logistic) modeling was used to identify variables or features that accounted for meaningful variation. Logistic regression models, used to determine significant differences in comorbidities between groups were constructed by adjusting for demographic variables (age, sex, race, ethnicity, and marital status), as these are known to be confounding. Poisson regression models, used to determine significant differences in utilization between groups, were also adjusted for potential confounding demographic variables (age, sex, race, ethnicity, and marital status). For each statistical model, assumptions were assessed empirically by viewing the data. Age and sex were recorded for everyone, and race/ethnicity and marital status were both included in the “other” classification if they were not reported.
No statistical power calculation was conducted prior to the start of the study because we analyzed all available data from the SH PC population. Every individual in the cohort was required to have at least one encounter during the study period, therefore, there were no missing values for any utilization‐based data including comorbidities, encounters, and medications.
Data extraction and analyses were conducted in SAS 9.4, SAS Enterprise Guide 7.15, SQL Server Management Studio 2016, and R 3.5.2.
Ethical considerations
The study was approved by the SH Institutional Review Board.
RESULTS
Demographic features
From a total of 1,489,156 patients in SH's 5‐year PC population, we identified 94,149 patients with migraine and 1,248,763 controls who did not meet the migraine case definition, and had no evidence of headache (e.g., no visits coded for headache or diagnoses in EHR) (Figure 1). Migraine patients were more likely to be female than controls (82.3% vs. 59.5%, p < 0.001), and tended to be younger [ages 65+: 8.0% vs. 14.9%, p < 0.001 for migraine vs. control, respectively; median 42 years (range: 18 to >89) vs. 43 years (range: 18 to >89), p < 0.001] (Table 1). Migraine patients were also more likely to be white than controls (57.4% vs. 48.6%, p < 0.001), and less likely to be Asian (9.4% vs. 16.7%, p < 0.001). There was little difference in marital status between the migraine and control groups. Migraine patients who sought care from a neurologist were similar to those treated in PC in sex, age, ethnicity, and marital status. The neurology patients were more likely to have preexisting migraine than those who only sought care from a PCP (49.9% vs. 36.2%, p < 0.001).
FIGURE 1.

Study flow diagram [Color figure can be viewed at wileyonlinelibrary.com]
TABLE 1.
Demographic details for migraine and control population
| All migraine | All migraine | Control | ||
|---|---|---|---|---|
| PC‐M | N‐M | |||
| N = 72,624 | N = 21,525 | N = 94,149 | N = 1,248,763 | |
| Sex | ||||
| Femalea | 59,697 (82.2%) | 17,801 (82.7%) | 77,485 (82.3%) | 743,014 (59.5%) |
| Age, in years | ||||
| 18–29 | 14,888 (20.5%) | 4025 (18.7%) | 18,924 (20.1%) | 263,489 (21.1%) |
| 30–44 | 26,435 (36.4%) | 8223 (38.2%) | 34,647 (36.8%) | 399,604 (32%) |
| 45–54 | 15,542 (21.4%) | 4606 (21.4%) | 20,148 (21.4%) | 221,031 (17.7%) |
| 55–64 | 10,095 (13.9%) | 2820 (13.1%) | 12,898 (13.7%) | 178,573 (14.3%) |
| 65+ | 5665 (7.8%) | 1851 (8.6%) | 7532 (8%) | 186,066 (14.9%) |
| Ethnicity/race | ||||
| Hispanic | 9659 (13.3%) | 2927 (13.6%) | 12,616 (13.4%) | 147,354 (11.8%) |
| NH Asian | 6899 (9.5%) | 1937 (9.0%) | 8850 (9.4%) | 207,295 (16.6%) |
| NH Black or African American | 2469 (3.4%) | 796 (3.7%) | 3295 (3.5%) | 41,209 (3.3%) |
| NH White | 41,468 (57.1%) | 12,635 (58.7%) | 54,042 (57.4%) | 605,650 (48.5%) |
| Other | 12,128 (16.7%) | 3229 (15.0%) | 15,346 (16.3%) | 247,255 (19.8%) |
| Migraine status | ||||
| Preexisting (prevalent) migraine | 26,290 (36.2%) | 10,741 (49.9%) | 37,095 (39.4%) | |
| Marital status | ||||
| Married/significant other/life partner | 40,597 (55.9%) | 12,442 (57.8%) | 53,006 (56.3%) | 656,849 (52.6%) |
| Single | 19,028 (26.2%) | 5532 (25.7%) | 24,573 (26.1%) | 314,688 (25.2%) |
| Divorced/separated | 4285 (5.9%) | 1421 (6.6%) | 5743 (6.1%) | 46,204 (3.7%) |
| Widowed | 1525 (2.1%) | 495 (2.3%) | 1977 (2.1%) | 38,712 (3.1%) |
| Other/unknown | 7190 (9.9%) | 1636 (7.6%) | 8850 (9.4%) | 192,310 (15.4%) |
| Follow‐up time | ||||
| Mean (years) | 2.6 | 3.1 | 2.7 | 2.1 |
p‐value = 0.127 for PC‐M versus N‐M comparison, all other comparisons p‐value < 0.001.
Co‐occurring disorders and comorbid conditions
Patients with migraine were more likely to have at least one autoimmune condition than controls and this relationship remained statistically significant after adjusting for demographics (4.4% vs. 2.6%, adjusted odds ratio (aOR) = 1.71, p < 0.001) (Table 2). This pattern was consistent across all autoimmune conditions except type 1 diabetes, which was similar in both groups. Other pain conditions were more than twice as common among patients with migraine as controls (13.2% vs. 5.8%, aOR = 2.97, p < 0.001). This pattern was similar for respiratory (24.6% vs. 12.3%, aOR = 2.40, p < 0.001), neurological (2.9% vs. 0.9%, aOR = 3.36, p < 0.001), and cerebrovascular (1.0% vs. 0.6%, aOR = 2.65, p < 0.001), but not for cardiovascular diseases which was more common among controls (7.6% for migraine vs. 9.1% for control). However, after adjusting for demographics, cardiovascular disease was more likely to be present among those with migraine (aOR = 1.26, p < 0.001). Several other diseases also were more common among patients with migraine including sleep apnea, irritable bowel syndrome (IBS), gastro‐esophageal reflux disorder (GERD), deep vein thrombosis (DVT), and pulmonary embolism (PE).
TABLE 2.
Medically diagnosed (EHR) comorbidities for migraine and control populations
| Condition | All migraine | All migraine | Control | Adjusted odds ratio | p‐values | |||
|---|---|---|---|---|---|---|---|---|
| PC‐M | N‐M | Adjusted odds ratio | p‐values | |||||
| N = 72,624 | N = 21,525 | N = 94,149 | N = 1,248,763 | |||||
| Psychiatric | 19,763 (27.2%) | 8291 (38.5%) | 1.66 | <0.001 | 28,054 (29.8%) | 147,043 (11.8%) | 2.84 | <0.001 |
| Anxiety | 13,988 (19.3%) | 6217 (28.9%) | 1.68 | <0.001 | 20,205 (21.5%) | 97,800 (7.8%) | 2.78 | <0.001 |
| Depression | 11,114 (15.3%) | 4720 (21.9%) | 1.53 | <0.001 | 15,834 (16.8%) | 76,349 (6.1%) | 2.78 | <0.001 |
| Autoimmune | 2797 (3.9%) | 1365 (6.3%) | 1.64 | <0.001 | 4162 (4.4%) | 31,981 (2.6%) | 1.71 | <0.001 |
| Multiple sclerosis | 195 (0.3%) | 353 (1.6%) | 6.10 | <0.001 | 548 (0.6%) | 2141 (0.2%) | 2.51 | <0.001 |
| Ulcerative colitis or Crohn's disease | 503 (0.7%) | 173 (0.8%) | 0.11 | 0.237 | 676 (0.7%) | 4752 (0.4%) | 1.86 | <0.001 |
| Psoriasis | 811 (1.1%) | 285 (1.3%) | 1.16 | 0.040 | 1096 (1.2%) | 11,155 (0.9%) | 1.40 | <0.001 |
| Arthritis—psoriasis arthritis | 171 (0.2%) | 88 (0.4%) | 1.66 | 0.002 | 259 (0.3%) | 1912 (0.2%) | 1.80 | <0.001 |
| Arthritis—rheumatoid arthritis | 716 (1.0%) | 337 (1.6%) | 1.52 | <0.001 | 1053 (1.1%) | 7071 (0.6%) | 1.86 | <0.001 |
| Diabetes type I | 292 (0.4%) | 95 (0.4%) | 1.06 | 0.623 | 388 (0.4%) | 5252 (0.4%) | 1.03 | 0.637 |
| Systemic lupus erythematosus | 370 (0.5%) | 176 (0.8%) | 1.59 | <0.001 | 546 (0.6%) | 1962 (0.2%) | 2.78 | <0.001 |
| Pain | 8221 (11.3%) | 4218 (19.6%) | 1.95 | <0.001 | 12,439 (13.2%) | 72,049 (5.8%) | 2.97 | <0.001 |
| Temporomandibular disorder | 487 (0.7%) | 375 (1.7%) | 2.60 | <0.001 | 862 (0.9%) | 1791 (0.1%) | 5.52 | <0.001 |
| Arthritis—type unknown | 1278 (1.8%) | 590 (2.7%) | 1.55 | <0.001 | 1868 (2.0%) | 12,734 (1.0%) | 2.19 | <0.001 |
| Arthritis—osteoarthritis | 3913 (5.4%) | 1520 (7.1%) | 1.32 | <0.001 | 5433 (5.8%) | 50,239 (4.0%) | 1.85 | <0.001 |
| Fibromyalgia | 4201 (5.8%) | 2668 (12.4%) | 2.28 | <0.001 | 6869 (7.3%) | 16,852 (1.3%) | 4.83 | <0.001 |
| Respiratory | 16,670 (23.0%) | 6516 (30.3%) | 1.42 | <0.001 | 23,186 (24.6%) | 153,692 (12.3%) | 2.40 | <0.001 |
| Allergies or hay fever | 9911 (13.6%) | 4107 (19.1%) | 1.45 | <0.001 | 14,018 (14.9%) | 84,857 (6.8%) | 2.44 | <0.001 |
| Asthma | 8670 (11.9%) | 3422 (15.9%) | 1.36 | <0.001 | 12,092 (12.8%) | 69,828 (5.6%) | 2.32 | <0.001 |
| COPD | 2786 (3.8%) | 1146 (5.3%) | 1.37 | <0.001 | 3932 (4.2%) | 33,775 (2.7%) | 1.95 | <0.001 |
| Cardiovascular | 5076 (7.0%) | 2091 (9.7%) | 1.41 | <0.001 | 7167 (7.6%) | 113,688 (9.1%) | 1.26 | <0.001 |
| Angina | 201 (0.3%) | 109 (0.5%) | 1.72 | <0.001 | 310 (0.3%) | 3219 (0.3%) | 2.08 | <0.001 |
| Angina/heart disease | 1351 (1.9%) | 574 (2.7%) | 1.36 | <0.001 | 1925 (2.0%) | 34,283 (2.7%) | 1.34 | <0.001 |
| Congestive heart failure | 609 (0.8%) | 235 (1.1%) | 1.23 | 0.008 | 844 (0.9%) | 16,082 (1.3%) | 1.12 | 0.002 |
| Coronary heart disease | 922 (1.3%) | 396 (1.8%) | 1.35 | <0.001 | 1318 (1.4%) | 25,897 (2.1%) | 1.29 | <0.001 |
| Peripheral vascular disease | 953 (1.3%) | 604 (2.8%) | 2.11 | <0.001 | 1557 (1.7%) | 18,823 (1.5%) | 1.82 | <0.001 |
| Diabetes type II | 3285 (4.5%) | 1155 (5.4%) | 1.16 | <0.001 | 4440 (4.7%) | 75,585 (6.1%) | 1.07 | <0.001 |
| Acute myocardial infarction | 129 (0.2%) | 48 (0.2%) | 1.15 | 0.430 | 177 (0.2%) | 3.098 (0.2%) | 1.18 | 0.032 |
| Neurologic | 1400 (1.9%) | 1288 (6.0%) | 3.14 | <0.001 | 2699 (2.9%) | 11,321 (0.9%) | 3.36 | <0.001 |
| Restless leg syndrome | 927 (1.3%) | 530 (2.5%) | 1.87 | <0.001 | 1457 (1.5%) | 6119 (0.5%) | 3.30 | <0.001 |
| Seizures, epilepsy | 489 (0.7%) | 789 (3.7%) | 5.48 | <0.001 | 1278 (1.4%) | 5286 (0.4%) | 3.40 | <0.001 |
| Cerebrovascular | 363 (0.5%) | 430 (2.0%) | 3.69 | <0.001 | 945 (1.0%) | 7500 (0.6%) | 2.65 | <0.001 |
| Stroke (thrombotic/embolic) | 229 (0.3%) | 258 (1.2%) | 3.61 | <0.001 | 487 (0.5%) | 4455 (0.4%) | 2.31 | <0.001 |
| Transient ischemic attack | 176 (0.2%) | 207 (1.0%) | 3.70 | <0.001 | 383 (0.4%) | 2537 (0.2%) | 3.09 | <0.001 |
| Hemorrhage (subarachnoid/intracerebral) | 92 (0.1%) | 97 (0.5%) | 3.34 | <0.001 | 471 (0.5%) | 4995 (0.4%) | 3.37 | <0.001 |
| Miscellaneous | 12,029 (16.6%) | 5601 (26.0%) | 1.79 | <0.001 | 17,630 (18.7%) | 118,023 (9.5%) | 1.58 | <0.001 |
| Sleep apnea | 3355 (4.6%) | 1998 (9.3%) | 2.13 | <0.001 | 5353 (5.7%) | 40,631 (3.3%) | 2.46 | <0.001 |
| Irritable bowel syndrome | 1871 (2.6%) | 1012 (4.7%) | 1.84 | <0.001 | 2883 (3.1%) | 9005 (0.7%) | 3.68 | <0.001 |
| Gastro esophageal reflux | 8184 (11.3%) | 3581 (16.6%) | 1.56 | <0.001 | 11,765 (12.5%) | 71,061 (5.7%) | 2.79 | <0.001 |
| Deep vein thrombosis | 554 (0.8%) | 294 (1.4%) | 1.73 | <0.001 | 848 (0.9%) | 6727 (0.5%) | 1.99 | <0.001 |
| Pulmonary embolism | 796 (1.1%) | 429 (2.0%) | 1.74 | <0.001 | 1225 (1.3%) | 10,881 (0.9%) | 1.96 | <0.001 |
All odds ratios and p‐values adjusted for age, sex, race, ethnicity, and marital status.
Among persons with migraine, some of the documented comorbidities were higher for N‐M consulters versus PC‐M consulters. For example, depression occurred in 21.9% of N‐M and 15.3% of PC‐M consulters (aOR = 1.53, p < 0.001), and the corresponding percentages for anxiety were 28.9% and 19.3% (aOR = 1.68, p < 0.001). Pain disorders were also more common in N‐M versus PC‐M consulters (19.6% vs. 11.3%, aOR = 1.95, p < 0.001) with higher rates of temporomandibular joint disorder, arthritis, and fibromyalgia (Table 2). Similarly, respiratory disorders were more common in neurology consulters (30.3% vs. 23.0%, aOR = 1.42, p < 0.001) with higher proportions of N‐M patients with diagnoses of allergies or hay fever and asthma.
Health care resource utilization
Tables 3 and 4 show utilization of care rates (per person‐year) for migraine patients and controls by age, sex, and race, and the same for PC‐M and N‐M. The table is restricted to those with more than 6 months of follow‐up time, and therefore, describes 79,097 migraines and 942,885 controls. Migraine patients had more encounters per person‐year with PCPs, neurologists, and the ED for every subgroup than patients in the control group. As expected, neurology encounters had, by far, the largest discrepancy between migraine and control patients (risk ratios ranged from 3.00 to 10.33). Patients with migraine were twice as likely to have encounters in the ED as their control counterparts, and ranged from 1.17 to 1.47 times more likely to have PC visits. Overall, in Poisson models comparing encounter counts for migraine versus control, adjusting for age, sex, race, ethnicity, marital status, and person time, this pattern remained and was statistically significant for all three utilization types (adjusted probability [aP] < 0.001).
TABLE 3.
Encounters per person‐year: migraine versus control populations
| All migraine | Control | Ratio (all migraine/control) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PCP | ED | Neurology | PCP | ED | Neurology | PCP | ED | Neurology | |
| 18–29 years | 3.77 | 0.29 | 0.31 | 2.60 | 0.12 | 0.03 | 1.45 | 2.42 | 10.33 |
| 30–44 years | 3.74 | 0.21 | 0.37 | 2.54 | 0.07 | 0.04 | 1.47 | 3.00 | 9.25 |
| 45–54 years | 3.71 | 0.17 | 0.43 | 2.64 | 0.07 | 0.06 | 1.41 | 2.43 | 7.17 |
| 55–64 years | 3.86 | 0.17 | 0.42 | 2.94 | 0.08 | 0.08 | 1.31 | 2.13 | 5.25 |
| 65+ years | 4.49 | 0.20 | 0.48 | 3.84 | 0.14 | 0.16 | 1.17 | 1.43 | 3.00 |
| Female | 3.94 | 0.22 | 0.40 | 3.07 | 0.10 | 0.07 | 1.28 | 2.20 | 5.71 |
| Male | 3.24 | 0.17 | 0.37 | 2.67 | 0.09 | 0.08 | 1.21 | 1.89 | 4.63 |
| Hispanic | 4.29 | 0.28 | 0.37 | 3.21 | 0.14 | 0.06 | 1.34 | 2.00 | 6.17 |
| NH Asian | 3.20 | 0.08 | 0.26 | 2.51 | 0.03 | 0.04 | 1.27 | 2.67 | 6.50 |
| NH Black | 4.80 | 0.64 | 0.48 | 3.57 | 0.29 | 0.10 | 1.34 | 2.21 | 4.80 |
| NH White | 3.83 | 0.21 | 0.43 | 3.01 | 0.11 | 0.09 | 1.27 | 1.91 | 4.78 |
| Other | 3.59 | 0.10 | 0.33 | 2.68 | 0.05 | 0.05 | 1.34 | 2.00 | 6.60 |
| Overall | 3.83 | 0.21 | 0.39 | 2.91 | 0.10 | 0.07 | 1.32 | 2.10 | 5.57 |
TABLE 4.
Encounters per person‐year among migraine patients: primary care versus neurology
| PC‐M | N‐M | Ratio (N‐M/PC‐M) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PCP | ED | Neurology | PCP | ED | Neurology | PCP | ED | Neurology | |
| 18–29 years | 3.58 | 0.27 | 0.04 | 4.35 | 0.33 | 1.11 | 1.22 | 1.22 | – |
| 30–44 years | 3.52 | 0.19 | 0.06 | 4.30 | 0.26 | 1.21 | 1.22 | 1.37 | – |
| 45–54 years | 3.52 | 0.16 | 0.08 | 4.25 | 0.21 | 1.42 | 1.21 | 1.31 | – |
| 55–64 years | 3.71 | 0.17 | 0.10 | 4.31 | 0.19 | 1.40 | 1.16 | 1.12 | – |
| 65+ years | 4.36 | 0.18 | 0.17 | 4.84 | 0.27 | 1.34 | 1.11 | 1.50 | – |
| Female | 3.74 | 0.20 | 0.07 | 4.52 | 0.26 | 1.31 | 1.21 | 1.30 | – |
| Male | 3.16 | 0.16 | 0.10 | 3.48 | 0.19 | 1.15 | 1.10 | 1.19 | – |
| Hispanic | 4.09 | 0.26 | 0.08 | 4.82 | 0.33 | 1.17 | 1.18 | 1.27 | – |
| NH Asian | 3.04 | 0.07 | 0.05 | 3.70 | 0.11 | 0.91 | 1.22 | 1.57 | – |
| NH Black | 4.54 | 0.62 | 0.12 | 5.43 | 0.70 | 1.37 | 1.20 | 1.13 | – |
| NH White | 3.64 | 0.20 | 0.08 | 4.33 | 0.26 | 1.39 | 1.19 | 1.30 | – |
| Other | 3.42 | 0.10 | 0.06 | 4.11 | 0.12 | 1.16 | 1.20 | 1.20 | – |
| Overall | 3.64 | 0.19 | 0.08 | 4.35 | 0.25 | 1.28 | 1.20 | 1.32 | – |
Among those patients with migraine, N‐M (N = 19,322) had slightly more encounters per patient year in every category than the PC‐M patients (N = 59,775) (Table 4). Overall, in Poisson models comparing encounter counts for PC‐M versus N‐M, adjusting for age, sex, race, ethnicity, marital status, and person time, this pattern remained and was statistically significant for all three utilization types (aP < 0.001).
Patterns of treatment—Acute
(triptans, ergotamines, nonnarcotic analgesics, and narcotic analgesics—see Appendix B for complete list): During the 5‐year period, overall, 77,762 (82.6%) of patients received at least one prescription order for an acute migraine medication, with a higher percentage of neurology consulters receiving orders than the PCP‐only consulters (89.4% vs. 80.6%, respectively). Among FC, these percentages were higher for both groups, and the relationship was attenuated (97.2% vs. 96.3% for N‐M vs. PC‐M, respectively) (Table 5).
TABLE 5.
Medication use 2013–2017
| Migraine patients | Frequent consulters – FC a | |||||
|---|---|---|---|---|---|---|
| N‐M | PC‐M | Total | N‐M | PC‐M | Total | |
| N = 21,525 | N = 72,624 | N = 94,149 | N = 10,610 | N = 7873 | N = 18,483 | |
| Any acute | 19,250 (89.4%) | 58,512 (80.6%) | 77,762 (82.6%) | 10,313 (97.2%) | 7581 (96.3%) | 17,894 (96.8%) |
| Nonnarcotic analgesics | 8461 (39.3%) | 18,509 (25.5%) | 26,970 (28.7%) | 4716 (44.4%) | 2988 (38.0%) | 7704 (41.7%) |
| 1–2 orders | 8124 (37.7%) | 18,100 (24.9%) | 26,224 (27.9%) | 4464 (42.1%) | 2846 (36.2%) | 7310 (39.6%) |
| 3+ orders | 337 (1.6%) | 409 (0.6%) | 746 (0.8%) | 252 (2.4%) | 142 (1.8%) | 394 (2.1%) |
| Narcotic analgesics | 13,669 (63.5%) | 36,168 (49.8%) | 49,837 (52.9%) | 7851 (74.0%) | 5737 (72.9%) | 13,588 (73.5%) |
| 1–2 orders | 9964 (46.3%) | 28,754 (39.6%) | 38,718 (41.1%) | 5283 (49.8%) | 3921 (49.8%) | 9204 (49.8%) |
| 3+ orders | 3705 (17.2%) | 7414 (10.2%) | 11,119 (11.8%) | 2568 (24.2%) | 1816 (23.1%) | 9204 (23.7%) |
| Triptans | 13,640 (63.3%) | 41,064 (56.5%) | 54,704 (58.1%) | 8447 (79.6%) | 5784 (73.5%) | 14,231 (77.0%) |
| 1–2 orders | 12,040 (55.9%) | 40,276 (55.5%) | 52,316 (55.6%) | 7020 (66.2%) | 5420 (68.8%) | 12,440 (67.3%) |
| 3+ orders | 1600 (7.4%) | 788 (1.1%) | 2388 (2.5%) | 1427 (13.5%) | 364 (4.6%) | 1791 (9.7%) |
| Other migraine‐specific medications | 1786 (8.3%) | 1673 (2.3%) | 3459 (3.7%) | 1405 (13.2%) | 368 (4.7%) | 1773 (9.6%) |
| 1–2 orders | 1763 (8.2%) | 1668 (2.3%) | 3431 (3.6%) | 1382 (13.0%) | 367 (4.7%) | 1749 (9.5%) |
| 3+ orders | 23 (0.1%) | 5 (0.0%) | 28 0.0% | 23 (0.2%) | 1 (<1%) | 23 (0.1%) |
| Any preventive | 17,524 (81.4%) | 40,289 (55.5%) | 57,813 (61.4%) | 9903 (93.4%) | 6475 (82.2%) | 16,378 (88.6%) |
| Beta blockers, any | 6053 (28.1%) | 11,753 (16.2%) | 17,806 (18.9%) | 3908 (36.8%) | 2427 (30.8%) | 6335 (34.3%) |
| 1–2 orders | 5859 (27.2%) | 11,450 (15.8%) | 17,309 (18.4%) | 3792 (35.7%) | 2359 (30.0%) | 6151 (33.3%) |
| 3+ orders | 194 (0.9%) | 303 (0.4%) | 497 (0.5%) | 116 (1.1%) | 68 (0.9%) | 184 (1.0%) |
| Calcium channel blockers, any | 3517 (16.3%) | 6507 (9.0%) | 10,024 (10.7%) | 2221 (20.9%) | 1188 (15.1%) | 3409 (18.4%) |
| 1–2 orders | 3445 (16.0%) | 6396 (8.8%) | 9841 (10.5%) | 2221 (20.9%) | 1188 (15.1%) | 3409 (18.4%) |
| 3+ orders | 72 (0.3%) | 111 (0.2%) | 183 (0.2%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Antidepressants, any | 13,359 (62.1%) | 29,479 (40.6%) | 42,838 (45.5%) | 8030 (75.7%) | 5018 (63.7%) | 13,048 (70.6%) |
| 1–2 orders | 9868 (45.8%) | 24,015 (33.1%) | 33,883 (36.0%) | 6601 (62.2%) | 4277 (54.3%) | 10,878 (58.9%) |
| 3+ orders | 3491 (16.2%) | 5464 (7.5%) | 8955 (9.5%) | 1429 (13.5%) | 741 (9.4%) | 2170 (11.7%) |
| Anticonvulsants, any | 11,575 (53.8%) | 17,263 (23.8%) | 28,838 (30.6%) | 7375 (69.5%) | 3604 (45.8%) | 10,979 (59.4%) |
| 1–2 orders | 9851 (45.8%) | 15,967 (22.0%) | 25,818 (27.4%) | 6154 (58.0%) | 3288 (41.8%) | 9442 (51.1%) |
| 3+ orders | 1724 (8.0%) | 1296 (1.8%) | 3020 (3.2%) | 1221 (11.5%) | 316 (4.0%) | 1537 (8.3%) |
| OnabotulinumtoxinA, any | 1617 (7.5%) | 231 (0.3%) | 1848 (2.0%) | 1502 (14.2%) | 60 (0.8%) | 1562 (8.5%) |
| 1–2 orders | 1617 (7.5%) | 231 (0.3%) | 1848 (2.0%) | 1502 (14.2%) | 60 (0.8%) | 1562 (8.5%) |
Frequent consulters = migraine patients with 4+ visits.
Table 6 displays medication orders per person‐year among those with at least one prescription, and shows that for both acute and preventive medications N‐M patients had more orders per‐person year than PC‐M consulters (acute: 1.0 vs. 0.8, p < 0.001, respectively; preventive: 0.9 vs. 0.7, p < 0.001, respectively).
TABLE 6.
Acute and preventive migraine prescription orders during the 5‐year study period
| PC‐M (N = 72,624) | N‐M (N = 21,525) | |||
|---|---|---|---|---|
| Medication orders per person‐year a | N (%) | Medication orders per person‐year a | N (%) | |
| Acute migraine medication order(s) | 0.8 | 58,512 (80.6%) | 1.0 | 19,250 (89.4%) |
| Preventive migraine medication order(s) | 0.7 | 40,289 (55.4%) | 0.9 | 17,524 (81.4%) |
| Any migraine medication order(s) | 1.3 | 63,110 (86.9%) | 1.8 | 20,596 (95.7%) |
Among those patients with ≥1 migraine medication order.
Patterns of treatment—Opioids
Opioids (narcotic analgesics) were prescribed to 49,837 (52.9%) patients with migraine, and this was more common among N‐M than PC‐M patients (63.5% vs. 49.8%) (Table 5). Opioids were less likely to be prescribed for Hispanic and NH Asian women. Hispanic patients had 12% lower odds of receiving a prescription for opioids than NH whites. Furthermore, NH Asian patients had 50% lower odds of receiving a prescription for opioids than NH whites. In general, women had 50% greater odds of receiving opioids than men (Figure 2).
FIGURE 2.
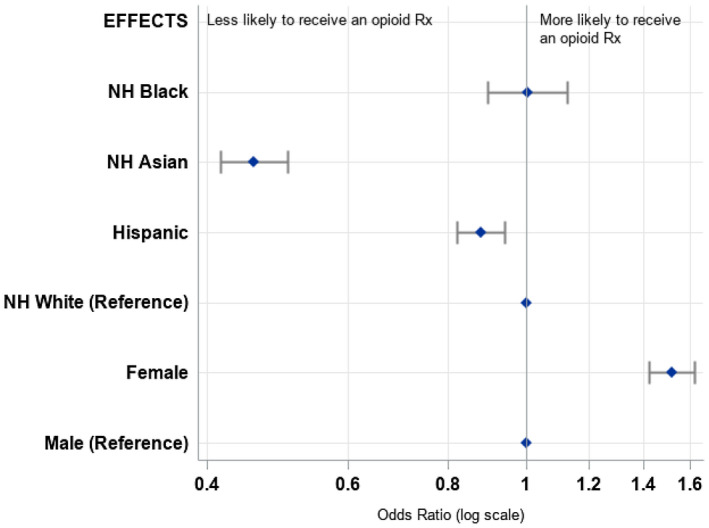
Opioid prescribing by sex and race among persons with migraine. ORs adjusted for age, sex, race, ethnicity, and cohort
Patterns of treatment—Preventive
During the 5‐year period, overall, 57,813 (61.4%) of patients received at least one prescription for a migraine preventive medication. Preventive treatment was higher in the N‐M group than in the PC‐M group (81.4% vs. 55.5%, p < 0.001). The most commonly used classes of migraine preventive medications were antidepressants, followed by anticonvulsants drugs, beta blockers, and calcium channel blockers. OnabotulinumtoxinA was the least prescribed (for the entire group, we were unable to determine chronic migraine status as we did not have migraine and headache day frequency but only EHR diagnosis when it was entered). Contrasting prescribing among N‐M versus PC‐M, all classes of preventive medication were given more frequently by neurologists with the greatest differences for anticonvulsants drugs and OnabotulinumtoxinA. Table 6 shows that preventive medication orders per person‐year for neurology‐consulting patients were slightly higher than PCP‐only consulters (0.9 vs. 0.7).
Among those FC, utilization of preventive medication was generally higher than in the whole group, though even in this frequent consulting group, those seeing neurologists were prescribed more preventive medication than those seeing PCPs only (03.4% vs. 82.2%).
For the three most commonly prescribed preventive medications classes (beta blockers, antidepressants, and anticonvulsants), average MPR was >75% (range: 70%–84%) and did not differ by PC‐M versus N‐M. Data are not shown.
DISCUSSION
We identified 94,149 PC adult patients who sought care for migraine from providers at SH, representing one of the largest and most diverse migraine cohorts from a health system reported in the literature. Unlike many population‐based migraine survey studies, these data report EHR‐based classifications of migraine, medication use, and comorbidities. The control group consisting of 1,248,763 patients included only those with no evidence of consultation for any headache‐related health issue or any related diagnosis. Although this migraine cohort represents 7% of the PC population, an estimate well below most found in the literature, it is important to note that this cohort represents patients who utilize health care for migraine, not all patients with migraine as is typically reported in population‐based surveys. Furthermore, the criteria we have chosen identify those patients who are highly likely to have migraine. We exclude those patients who have only a single diagnosis or medication order from a PC physician and have been previously demonstrated to be unlikely to have migraine. 30
Characterization of the migraine population
Compared with the control cohort, patients with migraine were more likely to be female, younger, and white, and less likely to be Asian. This is consistent with the literature in that migraine is more prevalent among NH whites, women, and younger individuals, and less prevalent among Asians. 31 Furthermore, in a study of the migraine patients in the General Practice Research Database in the United Kingdom from 1992 to 2000 younger female individuals were more likely to seek consultation for their migraines than older individuals and males. 3
Comorbidities and co‐occurring conditions
Adjusting for demographics, migraine patients were statistically significantly much more likely than the non‐migraine controls to have diagnosed comorbidities in a range of diseases and conditions, including: psychiatric, autoimmune, pain, respiratory, neurological, cerebrovascular, and other conditions (sleep apnea, IBS, GERD, DVT, and PE), and cardiovascular. Although many population‐based studies have reported comorbidity profiles based on self‐report, and have found similarities, to our knowledge, this is the first report of provider‐diagnosed comorbidities in a large health care network. An analysis of 15,133 people with migraine (73.0% women, 77.7% Caucasian, and mean age 43 years) and 77,453 controls (46.4% women, 76.8% Caucasian, and mean age 52 years) from the Migraine in America Symptoms and Treatment (MAST) Study found that respondents who met criteria for migraine were statistically significantly more likely to positively endorse having received a medical diagnosis of 21 common cardiovascular, neurologic, psychiatric, sleep, respiratory, dermatologic, pain, and medical comorbidities compared to the control group without migraine. 32 Comorbidities included depression, anxiety, insomnia, gastric ulcers/gastrointestinal bleeding, angina, and epilepsy, among other conditions. All cardiovascular events and conditions assessed including myocardial infarction (heart attack), high cholesterol, hypertension (high blood pressure), and stroke/transient ischemic attack were statistically significantly more commonly endorsed by people with migraine compared to the controls. This is similar to other studies comparing rates of various cardiac conditions between people with and without migraine. 33 , 34 , 35 Similarly, Korolainen et al., in a health care resource use study in Finland, reported among more than 17,000 people with migraine that there was a statistically significantly higher rate of comorbid conditions, especially psychiatric, sleep, and other pain disorders. 36 Our findings were not entirely consistent with the literature though. Bicakci, in a review article, summarizes commonly accepted comorbid conditions with migraine including all major cardiovascular conditions. 37 , 38 However, several studies have reported an association between cardiovascular diseases and only certain subgroups of migraine. 38 , 39 , 40 We found an association between migraine and cerebrovascular disease, and after adjusting for demographics, we found a similar relationship with cardiovascular disease. It is also possible that some of the differences between those with migraine and controls are inflated because people with migraine utilize health care more, and that may lead to higher probability of a comorbid diagnosis. This Berkson's bias could also exist in the comparisons between PC‐M and N‐M. 41
It should also be noted all of these comorbidities are associated with an increased risk of migraine progression, and temporal sequence is uncertain. We cannot determine from these data whether patients with migraine and a comorbidity develop more severe disease and are referred to a neurologist, or if comorbidity complicates treatment and leads to earlier referral.
Type of health care provider(s) for migraine
We found that in SH, among patients with migraine treated in PC settings, only 22.9% were also treated by neurologists (N‐M). Our study finds that more than 75% of migraine care at SH is provided by non‐neurologists. Previous studies have shown that there are differences in treatment and outcomes between patients treated in neurology versus only in PC settings. In order to examine differences between patients with migraine cared for by PCPs compared to those referred to neurologists, an analysis of 488 eligible patients consulting general practitioners with primary headache over 7 weeks and 81 patients referred to neurologists over 1 year in south‐east England collected data on migraine‐related disability (Migraine Disability Assessment Scale), headache impact (Headache Impact Test‐6), depression and anxiety using the Hospital Anxiety and Depression Scale, and illness perception using the Illness Perception Questionnaire. 5 Among 303 participants, there were no differences in mean headache disability, impact, anxiety, depression, or satisfaction with care. However, those referred to neurology consulted more frequently than those not referred in the 3 months before referral, were statistically significantly more likely to report a greater number of headache symptoms, to have stronger emotional representations of their headaches, to worry more, and were made anxious by their headache symptoms.
Health resource utilization for migraine and all cause
Patients who sought care for migraine from neurologists utilized health care services more than those who only sought care from PCPs, and accounting for person time, patients with migraine sought care for any reason at higher rates than controls. Hispanic and NH Black patients had more ED utilization than their NH White and Asian counterparts. This pattern held regardless of group.
Acute medication use for migraine
Acute prescription orders were higher than those reported in previous literature. We found that 82.6% of patients received at least one prescription order for an acute migraine medication, with a higher percentage of neurology consulters receiving acute migraine medication orders (89.4% vs. 80.6%, respectively). We found a similar, but attenuated relationship for FC with nearly 100% receiving these orders (97.2% vs. 96.3% for N‐M vs. PC‐M, respectively). These small yet statistically significant percentages are higher than expected considering that we are only accounting for prescription order, and most observational studies also include over‐the‐counter medication use. 12 , 20 , 24 , 42 , 43 , 44 This may be an artifact of the differing underlying populations from our study's health care‐seeking sample versus the population‐based studies reported in the literature. In addition, population‐based studies rely on self‐reported information which is subject to recall and other forms of bias.
Because there is a national opioid epidemic, and opioids are not recommended for the treatment of migraine, we were particularly interested in opioid use in this cohort over time, and prescribing by patient sex and race. 22 , 23 We were surprised to see that opioids were prescribed to more than half of patients with migraine in our sample, and an ever higher rate among the N‐M group. It is possible that the patients who seek care from neurologists represent a more complex cohort who have failed previous regimens. It is also possible that the greater comorbidity associated with N‐M is also associated with inability to use conventional treatments like triptans. Previous population‐based patient survey studies have reported lower use of opioids: 16% of American Migraine Prevalence and Prevention (AMPP) study respondents reported current use, and 30% ever; 15% of patients in the MAST study reported current use; and 19% of patients in the Observational Survey of the Epidemiology, Treatment and Care of Migraine study reported current use. 12 , 23 , 45 All these studies rely on self‐report, and because of the stigma attached to opioid use, may represent underestimates while the data reported here are from the EHR of a health care network, and are therefore objective. In addition, these other studies may reflect only the medications that were taken rather than those prescribed, as some of the studies asked about what a respondent “had on hand to treat headache” or “had taken in the past 30 days.” Hispanic and Asian patients were less likely to receive a prescription for opioids than NH whites, and women were more likely than men. Although, this finding is consistent with most literature which reports that women are more likely than men to take opioids, one recent study (MAST study) found the opposite pattern with men reporting more use of opioids than women (14.5% vs. 9.2%). The MAST study respondents were asked if they were currently taking opioids to treat their attacks while we report percentages of patients given a prescription for opioids, and we do not have information about whether they took the opioids or not. In any case, our findings highlight a great opportunity for improved care for migraine patients. These findings also identify an opportunity for further study into the patterns of prescribing of opioids, whether the neurologists or the PCPs are the first to prescribe, and the course of medication use after the initial prescription.
Preventive medication use for migraine
We found that among those who received more than one prescription, adherence (measured by MPR) to preventive medications was generally high (>75% on average), and did not differ by migraine group. This is somewhat unusual as it is generally accepted that both use and adherence to prophylactic migraine medications is lower possibly due to medication‐related side effects, complex dosing, perceived poor efficacy, and high costs. 2 , 42 , 46 , 47 Our higher‐than‐expected adherence measures are likely due to requirements for and assumptions we made when calculating MPRs such as the requirement of two or more prescriptions, and the assumption that the pills that were dispensed were also consumed. Restricting to more than one prescription, by design, biased the sample to patients who found it effective enough to keep taking it, and therefore, are more likely to be adherent. This calculation was made only for the period during which patients were getting refills, and this analysis cannot be used to make any inference about patients who stopped the medication. Rather, this analysis addresses the following question: what is the adherence to preventive medications during the period for which they have been prescribed their medication? However, when considering the question of stopping within a year after initiation, we observed that two‐thirds of patients who started Topiramate only received a single order during the study period.
Strengths
This study has several strengths. First, the SH setting offers large amounts of electronic health data from an integrated health care system, providing a comprehensive and representative picture of patient care for migraine in the US. Because of this rich data source, we are able to identify migraine patients without direct patient contact or a sampling structure typically required for population‐based studies. We have accurate data on patient demographics and utilization, and we are able to make comparisons between patients who receive all their migraine care from PCPs and those who seek care from neurology specialty clinics. In the SH system, we have identified nearly 100,000 patients with migraine, and we can leverage this large cohort to answer many types of research questions. By utilizing this rich data source, we determine patterns of consultation and treatment, not through the filter of self‐report, but based on objective data captured in the EHR.
Limitations
The primary limitation of this study is that the data are from the EHR of patients in an open health care system. This creates two potential issues. First, because the data are from the EHR, and we do not have actual contact with the patients, we cannot confirm or assess the severity of the migraine attacks, symptomology, or associated disability. Furthermore, we expect to undercount migraine because we can only identify those individuals who utilize the SH care system and report symptoms to their SH providers. Second, SH is an open health care system, so those patients who seek care for migraine outside of the SH network will not have their complete utilization recorded in the EHR.
By design, our data are limited as to what is available in the EHR, which does not include patient‐reported outcomes or other data from a patient perspective. In addition, comorbidities may be present but not documented and other data such as symptomology, pain intensity, and associated disability were limited. While utilization of health care and treatments have also been captured by surveys, recall over longer periods of time (e.g., past year) may be unreliable and often underestimate number of encounters, use of specialty and ED care, and procedures (e.g., imaging).
We have addressed these issues in two ways. First, as noted above, we have restricted our cohort to those patients who receive PC from SH. This will mitigate the missing data problem and increase the likelihood that everyone in the cohort will receive most or all of their care from SH providers. Second, we have supplemented the SH EHR with data from Surescripts pharmacy health information network. A consequence of restricting the cohort to those who receive PC is the loss of all migraine patients who utilize SH only for its specialty care. However, this study was not designed to estimate migraine prevalence, and does not require data from all migraine patients to complete its objectives.
A second limitation concerns our use of pharmacy fill data. Surescripts data include all dispensed medications filled at pharmacies that are part of the Surescripts network, including orders that did not originate from SH providers. While it is not possible to link dispensed medications in Surescripts with either encounters or orders originating at SH, in most cases we can infer from drug name and fill date, the order with which the dispensed medication is associated. For migraine‐specific medications, the Surescripts data are quite useful to quantify how many orders are filled, and how often. For preventive medications with a migraine indication in the EHR record, these data can be used to calculate medication possession ratios for estimating adherence. It should be noted, however, that because acute medications are to be taken as needed, measuring adherence is not meaningful for that category of drugs.
Finally, from one of our greatest strengths, our sample size, comes another limitation: an exaggerated tendency to identify statistical significance in the absence of clinical or practical significance. 48 We address this by pointing out which differences appear to be small, yet, statistically significant. As the notion of clinical significance is subjective, and may depend upon circumstance, we also rely on the expertise of the consumer, to determine which differences are relevant.
Conclusions
Patients who utilized the health care system for migraine were younger, more likely to be female and white than their counterparts who did not seek care for migraine. Those with migraine were more likely than controls to have nearly every comorbidity we classified from EHR data, except for Type 1 diabetes. Neurology patients at SH were more likely to receive both acute and preventive medication migraine orders than those patients who sought migraine care only from a PCP, with triptans and antidepressants the most commonly prescribed classes of acute and preventive pharmacotherapies, respectively. However, among FC, neurology patients were similarly highly likely to receive acute treatments, and although neurology patients were more likely to receive preventive treatments than those treated only in PC, the difference was smaller than that in the whole sample. Opioid use was higher than expected and was prescribed to more than half of patients with migraine.
During the 5‐year period, migraine patients were more likely to utilize care at SH compared to those without migraine across all types of encounters assessed, with the majority of visits occurring in the PC setting. Migraine patients who sought care from a neurologist were more likely to have ED encounters and those encounters were more likely to be for migraine. The results from this study are intended to inform health care systems, and can be extended to any open health care network.
Future directions
In a subsequent project, we have surveyed a random sample of both migraine and control patients to validate the data we have, to supplement data with patient reported outcomes and data which are not available in the EHR, and to determine the proportion of control participants who meet criteria for migraine using a validated self‐report screening instrument. Using these data, in this subset of patients, we plan to look more closely at the reasons for prescribing, and test our methods against the patient‐reported preventive use in the subsample for whom we have survey data. We also plan to study more in‐depth, patterns of opioid prescribing among the different types of physicians.
CONFLICT OF INTEREST
Dawn C. Buse has served as a consultant to Amgen/Novartis, Allergan, Biohaven, Eli Lilly, Promius/Dr. Reddy's, and Teva Pharmaceuticals. She is on the editorial board of Current Pain and Headache Reports. Walter F. Stewart has served as a consultant to Amgen, Inc. Richard B. Lipton serves on the editorial board of Neurology, as senior advisor to Headache, and as associate editor of Cephalalgia; holds stock options in eNeura Therapeutics and Biohaven Holdings; serves as consultant, advisory board member, or has received honoraria from: American Academy of Neurology, Alder, Allergan, American Headache Society, Amgen, Autonomic Technologies, Avanir, Biohaven, Biovision, Boston Scientific, Dr. Reddy's, Electrocore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKline, Merck, Pernix, Pfizer, Supernus, Teva, Trigemina, Vector, Vedanta; and receives royalties from Wolff's Headache 7th and 8th Edition, Oxford University Press, 2009, Wiley and Informa. Victoria M. Chia and Christine A. Szekely are employees of, and shareholders in, Amgen Inc. Alice R. Pressman, Shruti J. Vaidya, Alice S. Jacobson, and Alexandra B. Scott do not have any conflicts to report.
AUTHOR CONTRIBUTIONS
Study concept and design: Alice R. Pressman, Richard B. Lipton, Dawn C. Buse, Walter F. Stewart, and Alice S. Jacobson. Acquisition of data: Alice S. Jacobson and Shruti J. Vaidya. Analysis and interpretation of data: Alice R. Pressman, Richard B. Lipton, Dawn C. Buse, Walter F. Stewart, Alice S. Jacobson, and Shruti J. Vaidya. Drafting of the manuscript: Alice R. Pressman, Richard B. Lipton, Dawn C. Buse, Walter F. Stewart, Alice S. Jacobson, Shruti J. Vaidya, and Alexandra B. Scott. Revising it for intellectual content: Alice R. Pressman, Richard B. Lipton, Dawn C. Buse, Walter F. Stewart, Alice S. Jacobson, Shruti J. Vaidya, Alexandra B. Scott, Victoria M. Chia, and Christine A. Szekely. Final approval of the completed manuscript: Alice R. Pressman, Richard B. Lipton, Dawn C. Buse, Walter F. Stewart, Alice S. Jacobson, Shruti J. Vaidya, Alexandra B. Scott, Victoria M. Chia, and Christine A. Szekely.
ACKNOWLEDGMENTS
Michelle Goodreau, Alexandra Restall, Zijun Shen, Reeti Sharma.
APPENDIX A.
PSYCHIATRIC
Anxiety
ICD‐9
| 293.84 | Anxiety disorder in conditions classified elsewhere |
| 300.00 | Anxiety state, unspecified |
| 300.02 | Generalized anxiety disorder |
| 300.09 | Other anxiety states |
| 309.21 | Separation anxiety disorder |
| 309.24 | Adjustment disorder with anxiety |
| 309.28 | Adjustment disorder with mixed anxiety and depressed mood |
ICD‐10
| F41.1 | Generalized anxiety disorder |
| F41.3 | Other mixed anxiety disorders |
| F41.8 | Other specified anxiety disorders |
| F41.9 | Anxiety disorder, unspecified |
| F43.22 | Adjustment disorder with anxiety |
| F43.23 | Adjustment disorder with mixed anxiety and depressed mood |
| F93.0 | Separation anxiety disorder of childhood |
| F06.4 | Anxiety disorder due to known physiological condition |
Depression
ICD‐9
| 296.2* | Major depressive disorder single episode |
| 296.3* | Major depressive disorder recurrent episode |
| 309.0 | Adjustment disorder with depressed mood |
| 311 | Depressive disorder, not elsewhere classified |
ICD‐10
| F32.0 | Major depressive disorder, single episode, mild |
| F32.1 | Major depressive disorder, single episode, moderate |
| F32.2 | Major depressive disorder, single episode, severe without psychotic features |
| F32.3 | Major depressive disorder, single episode, severe with psychotic features |
| F32.4 | Major depressive disorder, single episode, in partial remission |
| F32.5 | Major depressive disorder, single episode, in full remission |
| F32.9 | Major depressive disorder, single episode, unspecified |
| F33.0 | Major depressive disorder, recurrent, mild |
| F33.1 | Major depressive disorder, recurrent, moderate |
| F33.2 | Major depressive disorder, recurrent severe without psychotic features |
| F33.3 | Major depressive disorder, recurrent, severe with psychotic symptoms |
| F33.4* | Major depressive disorder, recurrent, in remission |
| F32.9 | Major depressive disorder, recurrent, unspecified |
| F43.21 | Adjustment disorder with depressed mood |
AUTOIMMUNE
Multiple sclerosis
ICD‐9
| 340 | Multiple sclerosis |
ICD‐10
| G35 | Multiple sclerosis |
Ulcerative colitis/Crohn’s disease
ICD‐9
| 555.* | Regional enteritis |
| 556.* | Ulcerative enterocolitis |
ICD‐10
| K50.* | Crohn's disease |
| K51.* | Ulcerative colitis |
| K59.31 | Toxic megacolon |
Psoriasis
ICD‐9
| 696.1 | Psoriasis |
ICD‐10
| L40.0 | Psoriasis vulgaris |
| L40.1 | Generalized pustular psoriasis |
| L40.2 | Acrodermatitis continua |
| L40.3 | Pustulosis palmaris et plantaris |
| L40.4 | Guttate psoriasis |
| L40.8 | Other psoriasis |
Arthritis—Psoriatic arthritis
ICD‐9
| 696.0 | Psoriatic arthropathy |
ICD‐10
| L40.50 | Arthropathic psoriasis unspecified |
| L40.53 | Psoriatic spondylitis |
| L40.59 | Other psoriatic arthropathy |
Arthritis—Rheumatoid arthritis
ICD‐9
| 714.* | Rheumatoid arthritis and other inflammatory polyarthropathies |
ICD‐10
| M05.* | Rheumatoid arthritis with rheumatoid factor |
| M06.* | Other rheumatoid arthritis |
| M08.* | Juvenile arthritis |
| M12.0* | Chronic post‐rheumatic arthropathy |
Diabetes type I
ICD‐9
| 250.01 | Diabetes mellitus without mention of complication, type I [juvenile type], not stated as uncontrolled |
| 250.03 | Diabetes mellitus without mention of complication, type I [juvenile type], uncontrolled |
| 250.11 | Diabetes with ketoacidosis, type I [juvenile type], not stated as uncontrolled |
| 250.13 | Diabetes with ketoacidosis, type I [juvenile type], uncontrolled |
| 250.21 | Diabetes with hyperosmolarity, type I [juvenile type], not stated as uncontrolled |
| 250.23 | Diabetes with hyperosmolarity, type I [juvenile type], uncontrolled |
| 250.31 | Diabetes with other coma, type I [juvenile type], not stated as uncontrolled |
| 250.33 | Diabetes with other coma, type I [juvenile type], uncontrolled |
| 250.41 | Diabetes with renal manifestations, type I [juvenile type], not stated as uncontrolled |
| 250.43 | Diabetes with renal manifestations, type I [juvenile type], uncontrolled |
| 250.51 | Diabetes with ophthalmic manifestations, type I [juvenile type], not stated as uncontrolled |
| 250.53 | Diabetes with ophthalmic manifestations, type I [juvenile type], uncontrolled |
| 250.61 | Diabetes with neurological manifestations, type I [juvenile type], not stated as uncontrolled |
| 250.63 | Diabetes with neurological manifestations, type I [juvenile type], uncontrolled |
| 250.71 | Diabetes with peripheral circulatory disorders, type I [juvenile type], not stated as uncontrolled |
| 250.73 | Diabetes with peripheral circulatory disorders, type I [juvenile type], uncontrolled |
| 250.81 | Diabetes with other specified manifestations, type I [juvenile type], not stated as uncontrolled |
| 250.83 | Diabetes with other specified manifestations, type I [juvenile type], uncontrolled |
| 250.91 | Diabetes with unspecified complication, type I [juvenile type], not stated as uncontrolled |
| 250.93 | Diabetes with unspecified complication, type I [juvenile type], uncontrolled |
ICD‐10
| E10.* | Type 1 diabetes mellitus |
Systemic lupus erythematosus
ICD‐9
| 373.34 | Discoid lupus erythematosus of eyelid |
| 695.4 | Lupus erythematosus |
| 710.0 | Systemic lupus erythematosus |
ICD‐10
| D68.62 | Lupus anticoagulant syndrome |
| M32.* | Systemic lupus erythematosus (SLE) |
| L93.* | Lupus erythematosus |
| H01.12* | Discoid lupus erythematosus of eyelid |
PAIN
Temporomandibular disorder
ICD‐9
| 524.6* | Temporomandibular joint disorders |
ICD‐10
| M26.6* | Temporomandibular joint disorders |
Arthritis—Type unknown
ICD‐9
| 716.2* | Allergic arthritis |
| 716.3* | Climacteric arthritis |
| 716.4* | Transient arthropathy |
| 716.5* | Unspecified polyarthropathy or polyarthritis |
| 716.6* | Unspecified monoarthritis |
| 716.8* | Other specified arthropathy |
| 716.9* | Unspecified arthropathy |
ICD‐10
| M07.6* | Enteropathic arthropathies |
| M12.8* | Other specific arthropathies, not elsewhere classified |
| M13.1* | Monoarthritis, not elsewhere classified |
| M13.8* | Other specified arthritis |
| E08.618 | Diabetes mellitus due to underlying condition with other diabetic arthropathy |
| E09.618 | Drug or chemical induced diabetes mellitus with other diabetic arthropathy |
| E10.618 | Type 1 diabetes mellitus with other diabetic arthropathy |
| E11.618 | Type 2 diabetes mellitus with other diabetic arthropathy |
Arthritis—Osteoarthritis
ICD‐9
| 715.* | Osteoarthrosis and allied disorders |
ICD‐10
| M15.* | Polyosteoarthritis |
| M16.* | Osteoarthritis of hip |
| M17.* | Osteoarthritis of knee |
| M18.* | Osteoarthritis of first carpometacarpal joint |
| M19.* | Other and unspecified osteoarthritis |
Fibromyalgia
ICD‐9
| 729.1 | Myalgia and myositis, unspecified |
ICD‐10
| M60.8* | Other myositis |
| M60.9 | Myositis, unspecified |
| M79.1* | Myalgia |
| M79.7 | Fibromyalgia |
RESPIRATORY
Allergies/hay fever
ICD‐9
| 477.* | Allergic rhinitis |
ICD‐10
| J30.* | Vasomotor and allergic rhinitis |
Asthma
ICD‐9
| 493.* | Asthma |
ICD‐10
| J44.* | Other chronic obstructive pulmonary disease |
| J45.* | Asthma |
COPD
ICD‐9
| 416.8 | Other chronic pulmonary heart diseases |
| 416.9 | Chronic pulmonary heart disease, unspecified |
| 490 | Bronchitis, not specified as acute or chronic |
| 496 | Chronic airway obstruction, not elsewhere classified |
| 500 | Coal workers' pneumoconiosis |
| 501 | Asbestosis |
| 502 | Pneumoconiosis due to other silica or silicates |
| 503 | Pneumoconiosis due to other inorganic dust |
| 504 | Pneumonopathy due to inhalation of other dust |
| 505 | Pneumoconiosis, unspecified |
| 506.4 | Chronic respiratory conditions due to fumes and vapors |
| 508.1 | Chronic and other pulmonary manifestations due to radiation |
| 508.8 | Respiratory conditions due to other specified external agents |
| 491.* | Chronic bronchitis |
| 492.* | Emphysema |
| 494.* | Bronchiectasis |
| 495.* | Extrinsic allergic alveolitis |
ICD‐10
| J60 | Coal worker's pneumoconiosis |
| J61 | Pneumoconiosis due to asbestos and other mineral fibers |
| J40 | Bronchitis, not specified as acute or chronic |
| J42 | Unspecified chronic bronchitis |
| J64 | Unspecified pneumoconiosis |
| J68.4 | Chronic respiratory conditions due to chemicals, gases, fumes, and vapors |
| J70.1 | Chronic and other pulmonary manifestations due to radiation |
| J70.8 | Respiratory conditions due to other specified external agents |
| I27.81 | Cor pulmonale (chronic) |
| I27.89 | Other specified pulmonary heart diseases |
| I27.9 | Pulmonary heart disease, unspecified |
| J41.* | Simple and mucopurulent chronic bronchitis |
| J43.* | Emphysema |
| J44.* | Other chronic obstructive pulmonary disease |
| J47.* | Bronchiectasis |
| J67.* | Hypersensitivity pneumonitis due to organic dust |
| J62.* | Pneumoconiosis due to dust containing silica |
| J63.* | Pneumoconiosis due to other inorganic dusts |
| J66.* | Airway disease due to specific organic dust |
| I27.2* | Other secondary pulmonary hypertension |
CARDIOVASCULAR
Angina
ICD‐9
| 413.* | Angina pectoris |
ICD‐10
| I20.1 | Angina pectoris with documented spasm |
| I20.8 | Other forms of angina pectoris |
| I20.9 | Angina pectoris, unspecified |
| I25.111 | Atherosclerotic heart disease of native coronary artery with angina pectoris with documented spasm |
| I25.118 | Atherosclerotic heart disease of native coronary artery with other forms of angina pectoris |
| I25.119 | Atherosclerotic heart disease of native coronary artery with unspecified angina pectoris |
| I25.701 | Atherosclerosis of coronary artery bypass graft(s), unspecified, with angina pectoris with documented spasm |
| I25.708 | Atherosclerosis of coronary artery bypass graft(s), unspecified, with other forms of angina pectoris |
| I25.709 | Atherosclerosis of coronary artery bypass graft(s), unspecified, with unspecified angina pectoris |
| I25.711 | Atherosclerosis of autologous vein coronary artery bypass graft(s) with angina pectoris with documented spasm |
| I25.718 | Atherosclerosis of autologous vein coronary artery bypass graft(s) with other forms of angina pectoris |
| I25.719 | Atherosclerosis of autologous vein coronary artery bypass graft(s) with unspecified angina pectoris |
| I25.721 | Atherosclerosis of autologous artery coronary artery bypass graft(s) with angina pectoris with documented spasm |
| I25.728 | Atherosclerosis of autologous artery coronary artery bypass graft(s) with other forms of angina pectoris |
| I25.729 | Atherosclerosis of autologous artery coronary artery bypass graft(s) with unspecified angina pectoris |
| I25.731 | Atherosclerosis of non‐autologous biological coronary artery bypass graft(s) with angina pectoris with documented spasm |
| I25.738 | Atherosclerosis of non‐autologous biological coronary artery bypass graft(s) with other forms of angina pectoris |
| I25.739 | Atherosclerosis of non‐autologous biological coronary artery bypass graft(s) with unspecified angina pectoris |
| I25.751 | Atherosclerosis of native coronary artery of transplanted heart with angina pectoris with documented spasm |
| I25.758 | Atherosclerosis of native coronary artery of transplanted heart with other forms of angina pectoris |
| I25.759 | Atherosclerosis of native coronary artery of transplanted heart with unspecified angina pectoris |
| I25.761 | Atherosclerosis of bypass graft of coronary artery of transplanted heart with angina pectoris with documented spasm |
| I25.768 | Atherosclerosis of bypass graft of coronary artery of transplanted heart with other forms of angina pectoris |
| I25.769 | Atherosclerosis of bypass graft of coronary artery of transplanted heart with unspecified angina pectoris |
| I25.791 | Atherosclerosis of other coronary artery bypass graft(s) with angina pectoris with documented spasm |
| I25.798 | Atherosclerosis of other coronary artery bypass graft(s) with other forms of angina pectoris |
| I25.799 | Atherosclerosis of other coronary artery bypass graft(s) with unspecified angina pectoris |
Angina/heart failure
ICD‐9
| 402.* | Hypertensive heart disease |
| 411.* | Other acute and subacute forms of ischemic heart disease |
| 413.* | Angina pectoris |
| 398.9* | Other and unspecified rheumatic heart diseases |
| 414.0* | Coronary atherosclerosis |
| 414.2 | Chronic total occlusion of coronary artery |
| 414.3 | Coronary atherosclerosis due to lipid rich plaque |
| 414.4 | Coronary atherosclerosis due to calcified coronary lesion |
| 414.8 | Other specified forms of chronic ischemic heart disease |
| 414.9 | Chronic ischemic heart disease, unspecified |
| 416.0 | Primary pulmonary hypertension |
| 416.1 | Kyphoscoliotic heart disease |
| 416.8 | Other chronic pulmonary heart diseases |
| 416.9 | Chronic pulmonary heart disease, unspecified |
| 429.8* | Other ill‐defined heart diseases |
ICD‐10
| I11.* | Hypertensive heart disease |
| I20.* | Angina pectoris |
| I24.* | Other acute ischemic heart diseases |
| I27.* | Other pulmonary heart diseases |
| I09.8* | Other specified rheumatic heart diseases |
| I09.9 | Rheumatic heart disease, unspecified |
| I25.1* | Atherosclerotic heart disease of native coronary artery |
| I25.5 | Ischemic cardiomyopathy |
| I25.6 | Silent myocardial ischemia |
| I25.7* | Atherosclerosis of coronary artery bypass graft(s) and coronary artery of transplanted heart with angina pectoris |
| I25.8* | Other forms of chronic ischemic heart disease |
| I25.9 | Chronic ischemic heart disease, unspecified |
| I51.3 | Intra‐cardiac thrombosis, not elsewhere classified |
| I51.8* | Other ill‐defined heart diseases |
Congestive heart failure (CHF)
ICD‐9
| 428.* | Heart failure |
| 398.91 | Rheumatic heart failure (congestive) |
| 402.01 | Malignant hypertensive heart disease with heart failure |
| 402.11 | Benign hypertensive heart disease with heart failure |
| 402.91 | Unspecified hypertensive heart disease with heart failure |
| 404.01 | Hypertensive heart and chronic kidney disease, malignant, with heart failure and with chronic kidney disease stage I through stage IV, or unspecified |
| 404.03 | Hypertensive heart and chronic kidney disease, malignant, with heart failure and with chronic kidney disease stage V or end stage renal disease |
| 404.11 | Hypertensive heart and chronic kidney disease, benign, with heart failure and with chronic kidney disease stage I through stage IV, or unspecified |
| 404.13 | Hypertensive heart and chronic kidney disease, benign, with heart failure and chronic kidney disease stage V or end stage renal disease |
| 404.91 | Hypertensive heart and chronic kidney disease, unspecified, with heart failure and with chronic kidney disease stage I through stage IV, or unspecified |
| 404.93 | Hypertensive heart and chronic kidney disease, unspecified, with heart failure and chronic kidney disease stage V or end stage renal disease |
| 425.4 | Other primary cardiomyopathies |
| 425.5 | Alcoholic cardiomyopathy |
| 425.7 | Nutritional and metabolic cardiomyopathy |
| 425.8 | Cardiomyopathy in other diseases classified elsewhere |
| 425.9 | Secondary cardiomyopathy, unspecified |
ICD‐10
| I50.* | Heart failure |
| I09.81 | Rheumatic heart failure |
| I11.0 | Hypertensive heart disease with heart failure |
| I13.0 | Hypertensive heart and chronic kidney disease with heart failure and stage 1 through stage 4 chronic kidney disease, or unspecified chronic kidney disease |
| I13.2 | Hypertensive heart and chronic kidney disease with heart failure and with stage 5 chronic kidney disease, or end stage renal disease |
| I43 | Cardiomyopathy in diseases classified elsewhere |
| I42.5 | Other restrictive cardiomyopathy |
| I42.6 | Alcoholic cardiomyopathy |
| I42.8 | Other cardiomyopathies |
| I42.9 | Cardiomyopathy, unspecified |
Coronary heart disease
ICD‐9
| 414.0* | Coronary atherosclerosis |
ICD‐10
| I25.1* | Atherosclerotic heart disease of native coronary artery |
| I25.7* | Atherosclerosis of coronary artery bypass graft(s) and coronary artery of transplanted heart with angina pectoris |
| I25.81* | Atherosclerosis of other coronary vessels without angina pectoris |
Peripheral vascular disease
ICD‐9
| 093.0 | Aneurysm of aorta, specified as syphilitic |
| 437.3 | Cerebral aneurysm, non‐ruptured |
| 447.1 | Stricture of artery |
| 557.1 | Chronic vascular insufficiency of intestine |
| 557.9 | Unspecified vascular insufficiency of intestine |
| 440.* | Atherosclerosis |
| 441.* | Aortic aneurysm and dissection |
| 442.* | Other aneurysm |
| 443.* | Other peripheral vascular disease |
ICD‐10
| A52.01 | Syphilitic aneurysm of aorta |
| E08.51 | Diabetes mellitus due to underlying condition with diabetic peripheral angiopathy without gangrene |
| E08.52 | Diabetes mellitus due to underlying condition with diabetic peripheral angiopathy with gangrene |
| E09.51 | Drug or chemical induced diabetes mellitus with diabetic peripheral angiopathy without gangrene |
| E09.52 | Drug or chemical induced diabetes mellitus with diabetic peripheral angiopathy with gangrene |
| E10.51 | Type 1 diabetes mellitus with diabetic peripheral angiopathy without gangrene |
| E10.52 | Type 1 diabetes mellitus with diabetic peripheral angiopathy with gangrene |
| E11.51 | Type 2 diabetes mellitus with diabetic peripheral angiopathy without gangrene |
| E11.52 | Type 2 diabetes mellitus with diabetic peripheral angiopathy with gangrene |
| E13.51 | Other specified diabetes mellitus with diabetic peripheral angiopathy without gangrene |
| E13.52 | Other specified diabetes mellitus with diabetic peripheral angiopathy with gangrene |
| I67.0 | Dissection of cerebral arteries, non‐ruptured |
| I67.1 | Cerebral aneurysm, non‐ruptured |
| K55.1 | Chronic vascular disorders of intestine |
| K55.8 | Other vascular disorders of intestine |
| K55.9 | Vascular disorder of intestine, unspecified |
| Z95.82* | Presence of other vascular implants and grafts |
| I70.* | Atherosclerosis |
| I71.* | Aortic aneurysm and dissection |
| I72.* | Other aneurysm |
| I73.* | Other peripheral vascular diseases |
| I79.* | Disorders of arteries, arterioles and capillaries in diseases classified elsewhere |
| I77.1 | Stricture of artery |
| I77.7* | Other arterial dissection |
Diabetes type II
ICD‐9
| 250.00 | Diabetes mellitus without mention of complication, type II or unspecified type, not stated as uncontrolled |
| 250.02 | Diabetes mellitus without mention of complication, type II or unspecified type, uncontrolled |
| 250.10 | Diabetes with ketoacidosis, type II or unspecified type, not stated as uncontrolled |
| 250.12 | Diabetes with ketoacidosis, type II or unspecified type, uncontrolled |
| 250.20 | Diabetes with hyperosmolarity, type II or unspecified type, not stated as uncontrolled |
| 250.22 | Diabetes with hyperosmolarity, type II or unspecified type, uncontrolled |
| 250.30 | Diabetes with other coma, type II or unspecified type, not stated as uncontrolled |
| 250.32 | Diabetes with other coma, type II or unspecified type, uncontrolled |
| 250.40 | Diabetes with renal manifestations, type II or unspecified type, not stated as uncontrolled |
| 250.42 | Diabetes with renal manifestations, type II or unspecified type, uncontrolled |
| 250.50 | Diabetes with ophthalmic manifestations, type II or unspecified type, not stated as uncontrolled |
| 250.52 | Diabetes with ophthalmic manifestations, type II or unspecified type, uncontrolled |
| 250.60 | Diabetes with neurological manifestations, type II or unspecified type, not stated as uncontrolled |
| 250.62 | Diabetes with neurological manifestations, type II or unspecified type, uncontrolled |
| 250.70 | Diabetes with peripheral circulatory disorders, type II or unspecified type, not stated as uncontrolled |
| 250.72 | Diabetes with peripheral circulatory disorders, type II or unspecified type, uncontrolled |
| 250.80 | Diabetes with other specified manifestations, type II or unspecified type, not stated as uncontrolled |
| 250.82 | Diabetes with other specified manifestations, type II or unspecified type, uncontrolled |
| 250.90 | Diabetes with unspecified complication, type II or unspecified type, not stated as uncontrolled |
| 250.92 | Diabetes with unspecified complication, type II or unspecified type, uncontrolled |
ICD‐10
| E11.* | Type 2 diabetes mellitus |
| E13.* | Other specified diabetes mellitus |
Acute myocardial infarction (AMI)
ICD‐9
| 410.* | Acute myocardial infarction |
ICD‐10
| I21.* | Acute myocardial infarction |
NEUROLOGICAL
Restless legs syndrome
ICD‐9
| 333.94 | Restless legs syndrome (RLS) |
ICD‐10
| G25.81 | Restless legs syndrome |
Seizure/epilepsy
ICD‐9
| 345.* | Epilepsy and recurrent seizures |
ICD‐10
| G40.* | Epilepsy and recurrent seizures |
| I69.* | Sequelae of cerebrovascular disease |
CEREBROVASCULAR
Stroke (thrombotic and embolic)
ICD‐9
| 433.01 | Occlusion and stenosis of basilar artery with cerebral infarction |
| 433.11 | Occlusion and stenosis of carotid artery with cerebral infarction |
| 433.21 | Occlusion and stenosis of vertebral artery with cerebral infarction |
| 433.31 | Occlusion and stenosis of multiple and bilateral pre cerebral arteries with cerebral infarction |
| 433.81 | Occlusion and stenosis of other specified pre cerebral artery with cerebral infarction |
| 433.91 | Occlusion and stenosis of unspecified pre cerebral artery with cerebral infarction |
| 434.01 | Cerebral thrombosis with cerebral infarction |
| 434.11 | Cerebral embolism with cerebral infarction |
| 434.91 | Cerebral artery occlusion, unspecified with cerebral infarction |
ICD‐10
| I63.* | Cerebral infarction |
Transient ischemic attack
ICD‐9
| 435.* | Transient cerebral ischemia |
ICD‐10
| G45.* | Transient cerebral ischemic attacks and related syndromes |
Hemorrhage (SAH and ICH)
ICD‐9
| 430 | Subarachnoid hemorrhage |
| 431 | Intracerebral hemorrhage |
ICD‐10
| I60.* | Non‐traumatic subarachnoid hemorrhage |
| I61.* | Non‐traumatic intracerebral hemorrhage |
APPENDIX B.
| Drug category | Generic name |
|---|---|
| Acute medications | |
| Ergotamines | Dihydroergotamine mesylate |
| Ergotamine tartrate | |
| Ergotamine tartrate + caffeine | |
| Ergotamine tartrate + caffeine + belladonna + pentobarbital | |
| Triptans | Almotriptan |
| Eletriptan | |
| Frovatriptan | |
| Naratriptan | |
| Rizatriptan | |
| Sumatriptan (with and without naproxen) | |
| Zolmitriptan | |
| NSAIDs a | Celecoxib |
| Diclofenac | |
| Diflunisal | |
| Etodolac | |
| Fenoprofen | |
| Flurbiprofen | |
| Ibuprofen | |
| Indomethacin | |
| Ketoprofen | |
| Ketorolac | |
| Meclofenamic acid | |
| Mefenamic acid | |
| Meloxicam | |
| Nabumetone | |
| Naproxen | |
| Oxaprozin | |
| Piroxicam | |
| Rofecoxib | |
| Salsalate | |
| Sulindac | |
| Tolmetin | |
| Valdecoxib | |
| Opioids b | Codeine |
| Fentanyl | |
| Hydrocodone | |
| Hydromorphone | |
| Morphine sulfate | |
| Oxycodone | |
| Oxymorphone | |
| Tramadol | |
| Opioid other—Alfentanil, Buprenorphine, Butorphanol tartrate, Dezocine, Dihydrocodeine, Levomethadyl, Levorphanol, Meperidine, Methadone, Nalbuphine, Opium/belladonna alkaloids/opium alkaloids, Pentazocine, Propoxyphene, Remifentanil, Sufentanil, Tapentadol |
| Drug category | Drug subcategory | Generic name |
|---|---|---|
| Preventive medications | ||
| Antiepileptic agents | n/a | Carbamazepine |
| Gabapentin | ||
| Levetiracetam | ||
| Pregabalin | ||
| Topiramate | ||
| Valproate sodium/valproic acid/divalproex sodium | ||
| Zonisamide | ||
| Antihypertensive agents | Beta blocker | Atenolol |
| Bisoprolol | ||
| Metoprolol | ||
| Nadolol | ||
| Nebivolol | ||
| Pindolol | ||
| Propranolol | ||
| Timolol | ||
| Calcium channel blocker | Flunarizine | |
| Verapamil | ||
| Antihypertensives, other | Candesartan | |
| Clonidine | ||
| Lisinopril | ||
| Antidepressants | Serotonin norepinephrine reuptake inhibitors | Duloxetine |
| Desvenlafaxine | ||
| Venlafaxine | ||
| Tricyclics | Amitriptyline | |
| Desipramine | ||
| Doxepin | ||
| Imipramine | ||
| Nortriptyline | ||
| Protriptyline | ||
| Selective serotonin reuptake inhibitors | Escitalopram | |
| Citalopram | ||
| Sertraline | ||
| Botulinum toxin | n/a | AbobotulinumtoxinA |
| IncobotulinumtoxinA | ||
| OnabotulinumtoxinA | ||
| RimabotulinumtoxinB | ||
| Other migraine preventive agents | n/a | Carisoprodol |
| Cyproheptadine | ||
| Guanfacine | ||
| Memantine | ||
| Methysergide | ||
| Milnacipran | ||
| Tizanidine | ||
| Anti‐calcitonin gene related peptides | CGRP receptor blocker | Erenumab |
| CGRP ligand binder | Fremanezumab | |
| Galcanezumab | ||
Main NSAID generic names are listed for brevity, the analysis will include drugs that contain the generic drug plus other ingredients.
List of opioid generic names based on Johnston et al. (2016); main opioid generic names are listed for brevity, the analysis will include drugs that contain the generic drug plus other ingredients as well as various formulations (i.e., NaCl and HCl).
REFERENCES
- 1. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789‐1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):343‐349. [DOI] [PubMed] [Google Scholar]
- 3. Latinovic R, Gulliford M, Ridsdale L. Headache and migraine in primary care: consultation, prescription, and referral rates in a large population. J Neurol Neurosurg Psychiatry. 2006;77(3):385‐387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Stone J, Carson A, Duncan R, et al. Who is referred to neurology clinics? The diagnoses made in 3781 new patients. Clin Neurol Neurosurg. 2010;112(9):747‐751. [DOI] [PubMed] [Google Scholar]
- 5. Ridsdale L, Clark LV, Dowson AJ, et al. How do patients referred to neurologists for headache differ from those managed in primary care? Br J Gen Pract. 2007;57(538):388‐395. [PMC free article] [PubMed] [Google Scholar]
- 6. Patterson VH, Esmonde TF. Comparison of the handling of neurological outpatient referrals by general physicians and a neurologist. J Neurol Neurosurg Psychiatry. 1993;56(7):830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lipton RB, Stewart WF, Simon D. Medical consultation for migraine: results from the American Migraine Study. Headache. 1998;38(2):87‐96. [DOI] [PubMed] [Google Scholar]
- 8. Davies PTG, Lane RJM, Astbury T, Fontebasso M, Murphy J, Matharu M. The long and winding road: the journey taken by headache sufferers in search of help. Prim Health Care Res Dev. 2019;20:e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Bigal ME, Kolodner KB, Lafata JE, Leotta C, Lipton RB. Patterns of medical diagnosis and treatment of migraine and probable migraine in a health plan. Cephalalgia. 2006;26(1):43‐49. [DOI] [PubMed] [Google Scholar]
- 10. Lafata JE, Tunceli O, Cerghet M, Sharma KP, Lipton RB. The use of migraine preventive medications among patients with and without migraine headaches. Cephalalgia. 2010;30(1):97‐104. [DOI] [PubMed] [Google Scholar]
- 11. Patel NV, Bigal ME, Kolodner KB, Leotta C, Lafata JE, Lipton RB. Prevalence and impact of migraine and probable migraine in a health plan. Neurology. 2004;63(8):1432‐1438. [DOI] [PubMed] [Google Scholar]
- 12. Lipton RB, Munjal S, Alam A, et al. Migraine in America Symptoms and Treatment (MAST) study: baseline study methods, treatment patterns, and gender differences. Headache. 2018;58(9):1408‐1426. [DOI] [PubMed] [Google Scholar]
- 13. Hepp Z, Rosen NL, Gillard PG, Varon SF, Mathew N, Dodick DW. Comparative effectiveness of onabotulinumtoxinA versus oral migraine prophylactic medications on headache‐related resource utilization in the management of chronic migraine: retrospective analysis of a US‐based insurance claims database. Cephalalgia. 2016;36(9):862‐874. [DOI] [PubMed] [Google Scholar]
- 14. Runken MC, Goodwin B, Shah M, et al. Migraine‐related healthcare resource use and costs for subjects prescribed fixed‐dose combination sumatriptan/naproxen sodium vs. single‐entity oral triptans in a managed care population in the USA. Appl Health Econ Health Policy. 2015;13(1):109‐120. [DOI] [PubMed] [Google Scholar]
- 15. Esteban‐Vasallo M, Dominguez‐Berjon M, Astray‐Mochales J, et al. Epidemiological usefulness of population‐based electronic clinical records in primary care: estimation of the prevalence of chronic diseases. Fam Pract. 2009;26(6):445‐454. [DOI] [PubMed] [Google Scholar]
- 16. Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies. Headache. 2015;55(1):21‐34. [DOI] [PubMed] [Google Scholar]
- 17. Violán C, Foguet‐Boreu Q, Hermosilla‐Pérez E, et al. Comparison of the information provided by electronic health records data and a population health survey to estimate prevalence of selected health conditions and multimorbidity. BMC Public Health. 2013;13:251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: the American Headache Society evidence assessment of migraine pharmacotherapies. Headache. 2015;55(1):3‐20. [DOI] [PubMed] [Google Scholar]
- 19. Woolley JM, Bonafede MM, Maiese BA, Lenz RA. Migraine prophylaxis and acute treatment patterns among commercially insured patients in the United States. Headache. 2017;57(9):1399‐1408. [DOI] [PubMed] [Google Scholar]
- 20. Smitherman TA, Burch R, Sheikh H, Loder E. The prevalence, impact, and treatment of migraine and severe headaches in the United States: a review of statistics from national surveillance studies. Headache. 2013;53(3):427‐436. [DOI] [PubMed] [Google Scholar]
- 21. Stewart WF, Celentano DD, Linet MS. Disability, physician consultation, and use of prescription medications in a population‐based study of headache. Biomed Pharmacother. 1989;43(10):711‐718. [DOI] [PubMed] [Google Scholar]
- 22. American Headache Society: Choosing W isely Campaign . Five Things Physicians and Patients Should Question. Philadelphia, PA: ABIM Foundation; 2013. [Google Scholar]
- 23. Buse DC, Pearlman SH, Reed ML, Serrano D, Ng‐Mak DS, Lipton RB. Opioid use and dependence among persons with migraine: results of the AMPP study. Headache. 2012;52(1):18‐36. [DOI] [PubMed] [Google Scholar]
- 24. Lipton RB, Munjal S, Buse DC, et al. Unmet acute treatment needs from the 2017 migraine in America Symptoms and Treatment study. Headache. 2019;59(8):1310‐1323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Silberstein S, Loder E, Diamond S, et al. Probable migraine in the United States: results of the American Migraine Prevalence and Prevention (AMPP) study. Cephalalgia. 2007;27(3):220‐229. [DOI] [PubMed] [Google Scholar]
- 26. Jalloh A, Begasse de Dhaem O, Seng E, Minen MT. Message framing and the willingness to pursue behavioral therapy: a study of people with migraine. J Neuropsychiatry Clin Neurosci. 2020;32(2):196‐200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Matsuzawa Y, Lee YSC, Fraser F, et al. Barriers to behavioral treatment adherence for headache: an examination of attitudes, beliefs, and psychiatric factors. Headache. 2019;59(1):19‐31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Minen MT, Azarchi S, Sobolev R, et al. Factors related to migraine patients’ decisions to initiate behavioral migraine treatment following a headache specialist's recommendation: a prospective observational study. Pain Med. 2018;19(11):2274‐2282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Hasse LA, Ritchey PN, Smith R. Quantifying headache symptoms and other headache features from chart notes. Headache. 2004;44(9):873‐884. [DOI] [PubMed] [Google Scholar]
- 30. Pressman A, Jacobson A, Eguilos R, et al. Prevalence of migraine in a diverse community—Electronic methods for migraine ascertainment in a large integrated health plan. Cephalalgia. 2016;36(4):325‐334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States: figures and trends from government health studies. Headache. 2018;58(4):496‐505. [DOI] [PubMed] [Google Scholar]
- 32. Buse DC, Reed ML, Fanning KM, et al. Comorbid and co‐occurring conditions in migraine and associated risk of increasing headache pain intensity and headache frequency: results of the migraine in America symptoms and treatment (MAST) study. J Headache Pain. 2020;21(1):23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Tsai C‐L, Chou C‐H, Lee P‐J, et al. The potential impact of primary headache disorders on stroke risk. J Headache Pain. 2016;17(1):108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Mahmoud AN, Mentias A, Elgendy AY, et al. Migraine and the risk of cardiovascular and cerebrovascular events: a meta‐analysis of 16 cohort studies including 1 152 407 subjects. BMJ Open. 2018;8(3):e020498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Adelborg K, Szépligeti SK, Holland‐Bill L, et al. Migraine and risk of cardiovascular diseases: Danish population based matched cohort study. BMJ. 2018;360:k96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Korolainen MA, Kurki S, Lassenius MI, et al. Burden of migraine in Finland: health care resource use, sick‐leaves and comorbidities in occupational health care. J Headache Pain. 2019;20(1):13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Biçakci Ş. Comorbidity of migraine. Noro Psikiyatr Ars. 2013;50(suppl. 1):S14‐S20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Kurth T, Gaziano JM, Cook NR, Logroscino G, Diener HC, Buring JE. Migraine and risk of cardiovascular disease in women. JAMA. 2006;296(3):283‐291. [DOI] [PubMed] [Google Scholar]
- 39. Bigal ME, Kurth T, Santanello N, et al. Migraine and cardiovascular disease: a population‐based study. Neurology. 2010;74(8):628‐635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Schürks M, Rist PM, Bigal ME, Buring JE, Lipton RB, Kurth T. Migraine and cardiovascular disease: systematic review and meta‐analysis. BMJ. 2009;339:b3914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Westreich D. Berkson's bias, selection bias, and missing data. Epidemiology. 2012;23(1):159‐164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Diamond S, Bigal ME, Silberstein S, Loder E, Reed M, Lipton RB. Patterns of diagnosis and acute and preventive treatment for migraine in the United States: results from the American Migraine Prevalence and Prevention study. Headache. 2007;47(3):355‐363. [DOI] [PubMed] [Google Scholar]
- 43. Bigal ME, Buse DC, Chen Y‐T, et al. Rates and predictors of starting a triptan: results from the American Migraine Prevalence and Prevention study. Headache. 2010;50(9):1440‐1448. [DOI] [PubMed] [Google Scholar]
- 44. Chu MK, Buse DC, Bigal ME, Serrano D, Lipton RB. Factors associated with triptan use in episodic migraine: results from the American Migraine Prevalence and Prevention study. Headache. 2012;52(2):213‐223. [DOI] [PubMed] [Google Scholar]
- 45. Tepper SJ. Opioids should not be used in migraine. Headache. 2012;52(suppl. 1):30‐34. [DOI] [PubMed] [Google Scholar]
- 46. Hepp Z, Dodick DW, Varon SF, Gillard P, Hansen RN, Devine EB. Adherence to oral migraine‐preventive medications among patients with chronic migraine. Cephalalgia. 2015;35(6):478‐488. [DOI] [PubMed] [Google Scholar]
- 47. Vanya M, Desai P, Clifford S, Howard K, Lisle TC, Sapra S. Understanding patient adherence to prophylactic migraine medications. Neurology. 2016;86(suppl. 16):P1.164. [Google Scholar]
- 48. Faber J, Fonseca LM. How sample size influences research outcomes. Dental Press J Orthod. 2014;19(4):27‐29. [DOI] [PMC free article] [PubMed] [Google Scholar]