

Abstract
The interatrial septum is a structure with complex embryological development. The true atrial septum is a circumscribed structure, and transgression outside of this area during transseptal puncture may result in entry into the extracardiac space or aorta that may result in a pericardial effusion or cardiac tamponade. (Level of Difficulty: Intermediate.)
Key Words: atrial fibrillation, complication, electrophysiology, pericardial effusion
Abbreviations and Acronyms: IAS, interatrial septum; SVC, superior vena cava
Graphical abstract

A 76-year-old man with a history of paroxysmal atrial fibrillation (CHA2DS2-VASc score of 4), hypertension, heart failure with recovered ejection fraction, and history of cardiac resynchronization therapy-defibrillator implantation underwent colonoscopy for gastrointestinal bleeding, while receiving anticoagulation therapy with rivaroxaban. Colonoscopy demonstrated multiple colonic polyps along with a 3 cm × 5 cm-ulcerated mass that appeared to be malignant in the transverse colon, subsequently diagnosed as moderately differentiated adenocarcinoma. His HAS-BLED score of 4 and ongoing unresolved risk of gastrointestinal bleeding prompted a referral for left atrial appendage occlusion (1).
Learning Objectives
-
•
To understand the anatomical boundaries of the true interatrial septum.
-
•
To understand the relationship between the interatrial septum and extracardiac structures and the potential for complication with inappropriate transseptal puncture technique.
Medical History
Intravenous heparin was administered prior to attempts at transseptal access. The 11-F sheath in the right femoral vein was exchanged for a 16-F Check-Flo (Cook Medical, Bloomington, Indiana) sheath over the wire. A 10-F SL1 sheath (Abbott Medical, Chicago, Illinois) was advanced through the Check-Flo sheath into the left subclavian vein over the guidewire. A radiofrequency transseptal needle (Bayless Medical, Mississauga, Ontario, Canada) was advanced to the tip of the 10-F SL1 sheath and dilator. Transesophageal echocardiographic and fluoroscopic guidance were used to bring the entire apparatus down; however, tenting of the fossa ovalis was not appreciated. Significant lipomatous interatrial septal hypertrophy was noted (Figure 1). To further aid in visualization, operators switched from transesophageal echocardiography to intracardiac echocardiography. Following multiple attempts at transseptal puncture in the fossa ovalis, the radiofrequency needle was advanced beyond the tip of the SL1 sheath, and radiofrequency energy was delivered (15 W for 2 s). Bubbles were visualized in the left atrium, and pressure recordings also confirmed left atrial access (Figures 2 and 3). Given the unusual difficulty of transseptal access, confirmation of left atrial location was sought using contrast through the SL1 sheath. However, contrast was visualized in the pericardial space (Figures 4 and 5, Videos 1 and 2). It was believed the transseptal needle punctured the anterosuperior plane of the interatrial septum, traversing the transverse pericardial sinus before entering the left atrium.
Figure 1.

Transesophageal Echocardiography Bicaval View
(Star) Interatrial septum hypertrophy. Sparing of the fossa ovalis (arrow).
Figure 2.

Right and Left Anterior Oblique Projections of Wire Advancement Following Transseptal Puncture
Figure 3.

Left Atrial Pressure Recording
Figure 4.

Right Anterior Oblique Projection of Contrast Extravasation Into Transverse Pericardial Space and Simultaneous Contrast Flow Into the Left Ventricle
Figure 5.

Left Anterior Oblique Projection of Contrast Extravasation Into Transverse Pericardial Space
Differential Diagnosis
As a result of contrast visualization within the pericardial space, inadvertent pericardial access was the primary differential diagnosis.
Investigations
The patient was monitored using transesophageal echocardiography and intracardiac echocardiography for 60 min. There was minimal pericardial effusion.
Management
Given inadvertent pericardial access, the procedure was aborted. A follow-up transthoracic echocardiogram obtained the next day revealed no significant pericardial effusion or evidence of hemodynamic compromise. The patient was discharged home.
Discussion
Transseptal access of the left atrium was first described in 1947 by Cournand (2) for the purpose of directly measuring the left atrial and pulmonary vein pressure and refined by Brockenbrough and Mullins (3). In the current era, transseptal puncture is widely used during many common cardiac procedures and is performed without the aid of transesophageal echocardiography or intracardiac echocardiography in many countries. Transseptal access, despite being increasingly performed and having an excellent safety profile, can be associated with complications regardless of indication (4).
Understanding the embryological development and anatomy of the interatrial septum is critical for operators performing this procedure. The classic description of the interatrial septum represents an extensive area of muscular tissue interposed between the left and right atria which is bound superiorly by the SVC ostium, posteriorly by the folds of the atrial wall, inferiorly by the inferior vena cava ostium, anteroinferiorly by the coronary sinus orifice, anteriorly by the septal leaflet of the tricuspid valve, and anterosuperiorly by the noncoronary sinus of Valsalva (5,6). It is important to note that on ex vivo anatomic dissection, removal of most of these structures will result in opening of the right atrial wall and arrival outside of the heart and into the pericardial space (7). The “true” atrial septum separating the left and right atrial chambers is a relatively small area encompassing approximately 20% of the total interatrial septum (IAS) area, and includes the floor of the fossa ovalis and its immediate muscular inferoanterior rim (Figure 6) (8).
Figure 6.

Component Parts of the Definitive Atrial Septum
IVC = inferior vena cava; SVC = superior vena cava.
Reprinted from Naqvi et al. (8).
The anterosuperior portion of the septal plane is located immediately posterior to the transverse pericardial sinus and the aortic root. This is highlighted by an observation that increased aortic size is correlated with decreased size and mobility of the atrial septum (9). Interventional procedures in this part of the septal plane carry a risk of exiting the heart or entering the aortic root, as the septal structures directly separating the right and left atria are considerably less than the entire septal plane that is visualized on imaging. Attempts at transseptal puncture outside of the fossa ovalis, although in the septal plane, may result in penetration into extracardiac tissues before entering the left atrium and can cause cardiac tamponade acutely or subacutely after the transseptal sheath has been retracted (6). Moreover, small “pits” and “crevices” have been described in this region, which may lodge the tip of a transseptal puncture device, giving a false impression of having “tented” the IAS (10). This complexity may be compounded by lipomatous interatrial hypertrophy, which can hinder transseptal needle penetration, lead to increased difficulty with instrument maneuverability, and dissection into the vascularized fibrofatty tissue plane, ultimately resulting in hemopericardium, as in the present case (Table 1) (11).
Table 1.
Tips for Successful Transseptal Puncture
| Problem | Tips and Tricks |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ICE = intracardiac echocardiography; IVC = inferior vena cava.
Amplatz; Cook Medical, Bloomington, Indiana;
SafeSept; Baylis Medical, Toronto, Ontario, Canada;
Protracts; Baylis Medical.
Additionally, the membranous ventricular septum can be divided into 2 segments based on the attachment of the septal leaflet of the tricuspid valve: a superior atrioventricular segment and an inferior interventricular segment. Inadvertent puncture into the superior atrioventricular portion of the membranous ventricular septum may result in direct right atrial-left ventricular communication, analogous to the Gerbode defect (Figure 7) (12).
Figure 7.
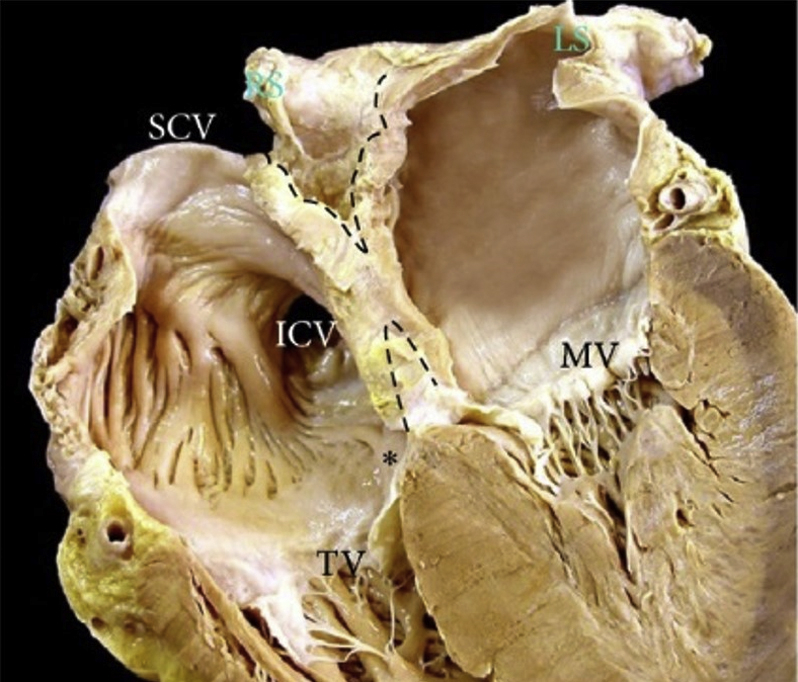
4-Chamber Section Through the Heart
Four-chamber section through the heart showing the offset arrangement of the mitral valve (MV) and tricuspid valve (TV) which produces the so-called muscular atrioventricular septum (∗) and the deep in folding (dotted lines) of the atrial wall superior and inferior to the floor of the oval fossa. IVC = inferior vena cava; SVC = superior vena cava.
Reprinted with permission from Sánchez-Quintana et al. (11).
Follow-Up
Approximately 1 month later, the patient was seen in the outpatient clinic and had no adverse clinical sequelae.
Conclusions
Appreciation of the anatomic relationship between the interatrial septum and the transverse pericardial sinus is crucial to the interventional cardiologist or electrophysiologist during transseptal puncture. Identification and puncture of the true IAS may aid in avoidance of complications including transgression into the pericardial space, aorta, or left ventricle.
Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Footnotes
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the Author Center.
Appendix
For supplemental videos, please see the online version of this paper.
Appendix
RAO 40° projection of contrast injection following transseptal puncture demonstrates simultaneous contrast flow into the left ventricle and extravasation into the transverse pericardial space.
LAO 50° projection of contrast injection following transseptal puncture demonstrates contrast flow into the transverse pericardial space.
References
- 1.January C.T., Wann L.S., Calkins H. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74:104–132. doi: 10.1016/j.jacc.2019.01.011. [DOI] [PubMed] [Google Scholar]
- 2.Cournand A.M.H. Recording of blood pressure from the left auricle and the pulmonary veins in human subjects with interauricular septal defect. Am J Physiol. 1947;150:267–271. doi: 10.1152/ajplegacy.1947.150.2.267. [DOI] [PubMed] [Google Scholar]
- 3.Brockenbrough E.C., Braunwald E.R.J. Transseptal left heart catheterization. A review of 450 studies and description of an improved technic. Circulation. 1962;25:15–21. doi: 10.1161/01.cir.25.1.15. [DOI] [PubMed] [Google Scholar]
- 4.Katritsis G.D., Siontis G.C.M., Giazitzoglou E., Fragakis N., Katritsis D.G. Complications of transseptal catheterization for different cardiac procedures. Int J Cardiol. 2013;168:5352–5354. doi: 10.1016/j.ijcard.2013.08.004. [DOI] [PubMed] [Google Scholar]
- 5.Anderson R.B.N. The anatomy of the heart revisited. Anat Rec. 1996;246:1–7. doi: 10.1002/(SICI)1097-0185(199609)246:1<1::AID-AR1>3.0.CO;2-Y. [DOI] [PubMed] [Google Scholar]
- 6.Klimek-Piotrowska W., Hołda M.K., Koziej M., Piatek K., Hołda J. Anatomy of the true interatrial septum for transseptal access to the left atrium. Ann Anat. 2016;205:60–64. doi: 10.1016/j.aanat.2016.01.009. [DOI] [PubMed] [Google Scholar]
- 7.Anderson R.H., Webb S., Brown N.A. Clinical anatomy of the atrial septum with reference to its developmental components. Clin Anat. 1999;12:362–374. doi: 10.1002/(SICI)1098-2353(1999)12:5<362::AID-CA6>3.0.CO;2-F. [DOI] [PubMed] [Google Scholar]
- 8.Naqvi N., McCarthy K.P., Ho S.Y. Anatomy of the atrial septum and interatrial communications. J Thorac Dis. 2018;10(Suppl 24):S2837–S2847. doi: 10.21037/jtd.2018.02.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bertaux G., Eicher J.C., Petit A., Dobšák P., Wolf J.E. Anatomic interaction between the aortic root and the atrial septum: a prospective echocardiographic study. J Am Soc Echocardiogr. 2007;20:409–414. doi: 10.1016/j.echo.2006.09.008. [DOI] [PubMed] [Google Scholar]
- 10.Ho S.Y., Cabrera J.A., Sanchez-Quintana D. Left atrial anatomy revisited. Circ Arrhythm Electrophysiol. 2012;5:220–228. doi: 10.1161/CIRCEP.111.962720. [DOI] [PubMed] [Google Scholar]
- 11.Sánchez-Quintana D., López-Mínguez J.R., Macías Y., Cabrera J.A., Saremi F. Left atrial anatomy relevant to catheter ablation. Cardiol Res Pract. 2014;2014:1–16. doi: 10.1155/2014/289720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chavarria N., Goldbarg S. Left ventricle penetration---a rare complication of transseptal puncture and catheter ablation for supraventricular tachycardia. Heart Rhythm Case Rep. 2015;1:382–383. doi: 10.1016/j.hrcr.2015.03.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
RAO 40° projection of contrast injection following transseptal puncture demonstrates simultaneous contrast flow into the left ventricle and extravasation into the transverse pericardial space.
LAO 50° projection of contrast injection following transseptal puncture demonstrates contrast flow into the transverse pericardial space.