

Summary
There have been historical arguments about the boundary of the caudate lobe of the liver. Kumon M first advocated the definition of the caudate lobe based on the portal segmentation of the liver in 1985, and classified it into three parts, Spiegel lobe, paracaval portion and caudate process. Prof. Couinaud defined the dorsal liver as a union of segments I and IX in 1994, based on the spatial position to the major hepatic veins, hilar plate and inferior vena cava. In Couinaud's classification, right-side of the dorsal liver is supplied by the branches from the posterior and anterior sections. In the present study using a liver cast, we found a paracaval branch of the portal vein branching from the right portal vein on the dissecting plain along the Rex-Cantlie's line. We also found several branches from the posterior portal vein to the right-side of the paracaval portion, but they should be defined to belong to the posterior sections.
Keywords: liver cast, caudate lobe, paracaval portion
Introduction
The caudate lobe of the liver is generally considered as the deepest area of the liver in front of the inferior vena cava (IVC) surrounded by the major hepatic veins and the hilar plate. However, there have been historical arguments on the boundary of the caudate lobe.
In 1985, Kumon M proposed to define the caudate lobe based on the portal segmentation and classified it into three parts, Spiegel lobe, paracaval portion and the caudate process (1-3). On the other hand, this deep area of the liver in front of the IVC had been also called dorsal liver by Prof. Couinaud. Prof. Couinaud, a famous French anatomist, classified the dorsal liver based on the spatial position against the major hepatic veins and IVC, and classified it into segment I and IX and then, placed these two segments into several alternatives (4-8).
Right-side boundary of the caudate lobe is clinically important in the surgical treatment of liver cancer or hilar cholangiocarcinoma. Curative surgical resection of perihilar cholangiocarcinoma requires total caudate lobectomy to obtain negative surgical margins, because the biliary branches in the caudate lobe is involved with cancer in more than 40% of cases (9).
In the present study, we revealed the right-side boundary of the caudate lobe of a liver cast, discovering the paracaval branches of the portal vein and bile duct in a liver cast.
Materials and Methods
A liver cast was made after injecting colored epoxy resin into the portal vein (blue) and bile duct (yellow) of the whole liver, while the hepatic artery and hepatic vein were left as they were without injecting resin. This method follows Healey and Schroy's (10). Although the author prepared 75 human liver casts between July 1, 1981 and October 2, 1990 (3), there was only one Healey and Schroy's type cast, which is suitable for observing the anatomy of the portal vein and bile duct. The specimen was fixed in water to preserve the natural hepatic shapes, as they would be in the body. The liver tissue was corroded completely using potassium hydroxide.
After fixation, we dissected the liver cast using forceps with fine tips and extracted the small Glissonean and venous branches, gently piece by piece. The right portal vein was divided at the proximal site of the bifurcation of the anterior and posterior portal branches. After meticulous dissection, we observed the portal and biliary branches of the paracaval portion of the caudate lobe.
The information on the study's approval by the Institutional Review Board/Research Ethics Committee has been described in previous study (3).
Results and Discussion
Before dissection of the liver, the whole liver was observed from the cranial ventral side of the liver (Figure 1). Because the liver cast did not have the hepatic arteries and veins including the IVC, dissection and observation were simple and easy without any consideration on the variation of the hepatic arteries and veins. The whole liver was divided along the Rex- Cantlie line, and the right Glissonean pedicle, composed of the right portal vein and the right bile duct, was found on the dissecting plane (Figures 2 and 3). The right portal vein and the bile duct were divided at the proximal site of the bifurcation of the anterior and posterior sections (Figures 3 and 4). The cut surface of the liver coincided the plane including right edge of the IVC. The root of the paracaval portal vein was found on the proximal side of the cut point of the right portal vein. The cut edge of the right portal vein and posterior bile duct revealed the portal branches and bile ducts in the paracaval portion of the liver (Figures 4 and 5). The paracaval portal vein branched from the right and left portal veins (Figure 5), while the paracaval branch of the bile duct branched from the posterior bile duct (Figure 4). There were found some branches from the posterior portal veins behind the posterior portal vein, going to the right-side of the paracaval portion along the IVC (Figure 6), which correspond to the c and d branches of segment IX in Couinaud's classification.
Figure 1.
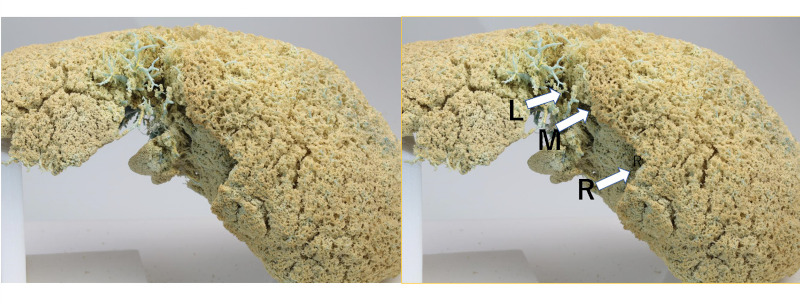
Cranial view of the liver cast from ventral position. Three arrows indicate the orifices of the major hepatic veins. L, left hepatic vein; M, middle hepatic vein; R, right hepatic vein.
Figure 2.

Cranial view of the hilar plate of the right Glissonean pedicle. Arrow head indicates the right portal vein. White arrow indicates the posterior bile duct. Black arrow indicates the paracaval branch of the bile duct. Green arrow indicates 1st portal branch of anterior portal vein.
Figure 3.

Cranial view of the division of the right Glissonean pedicle. The right and posterior hepatic duct and the right portal vein are divided. The paracaval bile duct (white arrow) branching from the posterior bile duct (white arrow head) is indicated. Black arrow head indicates anterior branches of the bile duct. Black and green arrows indicate the d-vein (Couinaud) and 1st branch of anterior portal vein, respectively. Red line indicates the right edge of IVC.
Figure 4.

Lateral view of the paracaval branch of the portal vein and the bile duct. The black arrows indicate paracaval branches of the portal vein branching from the right portal vein. The white arrow indicates the paracaval branch of the bile duct and the white arrow head indicates the posterior branch of the bile duct.
Figure 5.

Caudal view of the branches from the main portal vein and common bile duct. Black arrows indicate paracaval branches of portal veins. Yellow arrow indicates the superior portal branch of Spiegel lobe. Blue and yellow arrow head indicate the trunk of portal vein and common hepatic duct, respectively.
Figure 6.

Caudal view of the branches from the anterior and posterior portal veins. The inside portal branches from the posterior portal vein are shown behind the posterior portal vein along the inferior vena cava, which should belong to the posterior section, not paracaval potion, in our classification. The black arrow and white arrow head correspond to d-vein and c-vein in segment IX in Couinauds classification, respectively. A and P indicate the anterior and posterior portal veins, respectively. Green arrow indicates the first branch of anterior portal vein. P6 and P7 indicate portal veins of segment 6 and 7, respectively. Red line indicates the right marginal line of the inferior vena cava.
In the present study, we found the definitive portal and biliary branches to the paracaval portion of the liver in a divided liver cast. The paracaval branch of the portal vein branched from the right and left portal vein, a first-order branch of the main portal vein, thus this could be the paracaval portion based on the concept of portal segmentation. On the other hand, we confirmed that there were some accessory branches from the posterior portal vein along the IVC (Figure 6), which cannot be included in the paracaval portion. These portal veins should be included in the posterior section. As the biliary trees have considerable numbers of variants, it would be confusing to classify the hepatic segments based on the biliary segmentation as Ishiyama did (11,12).
The caudate lobe was first described as the "lobus exiguous" by Adrian van der Spiegel in 1622. Healey and Schroy first classified the liver into four sections, the lateral, medial, anterior and posterior segment. They defined the caudate lobe as areas that did not belong to the above four segments, and classified the caudate lobe into right portion, left portion and the caudate process (9). However, Kumon M was the first who classified the caudate lobe of the liver into three parts, Spiegel lobe, paracaval portion and caudate process, based on a study using 23 human liver casts (1,2). He has sustained the dogma that any hepatic segment should be defined based on portal segmentation.
On the contrary, Couinaud's definition of the caudate lobe, dorsal liver in his work varied with the times. He first described it on the dorsal liver and divided it into segment Il and Ir along the plain including middle hepatic vein in 1989 (4). He changed segment Il&Ir to segment I and IX in 1994 (5), and divided segment IX into three parts, subsegments b (between middle and right hepatic veins), c (inferior area of the right hepatic vein) and d (posterior area of the right hepatic vein) in 1998 (6). Then, he replaced segment IXb into IXL, and segment IXd to IXR (7), but finally abandoned his idea on classification of the caudate lobe in 2002 (8). As shown in the above transition, Couinaud had great difficulty defining the caudate lobe as a monosegment.
Ishiyama followed the concepts of Kumon and Couinaud. He supported the concept of dorsal liver by Couinaud from the viewpoint of biliary system, and advocated that 92.5% of the right-side area of the dorsal liver (dorso-lateral paracaval portion, dl-PCP) could not be covered only by the concept of Kumon's portal segmentation, analyzing 54 liver casts (11,12). He found that the bile ducts in the dl-PCP were supplied by the branches from the anterior and posterior bile ducts. He also mentioned that the biliary branches to the dorsal liver should include the branches from the posterior or anterior bile ducts in order to increase the curability of perihilar cholangiocarcinoma requiring left hemihepatectomy plus bile duct resection, and criticized the concept of Kumon's classification based on portal segmentation.
However, anatomical boundary of the liver should be determined based on anatomical landmarks, not on the surgeon's preference. First, Couinaud's dorsal liver is a concept of spatial position of the deep liver surrounded by the IVC and the right hepatic vein. This classification is not based on portal segmentation, and thus will cause some confusion on discriminating anatomical segments. Second, Ishiyama's concept is based on biliary segmentation. Portal branches in dl- PCP apparently carries the portal flow in the anterior or posterior portal branches, and could be better included in anterior or posterior sections based on the concept of portal segmentation.
Gadzijev et al. studied the difference between segment I and IX using 61 human liver corrosion casts. They also accepted the concepts of Couinaud's dorsal liver and defined segment IX as the dorsal part of the liver located about 2cm away from the IVC (13). His concept is also not based on portal segmentation and supported the concept of dorsal liver by Prof. Couinaud. Prof. Makuuchi, a legend of liver surgeons, commented that Couinaud's segment IX corresponds to the paracaval portion of the liver on Kumon's classification (14), however we regret that his explanation cannot be accepted.
Conclusion
Anatomical right-sided boundary of the paracaval portion of the caudate was studied in a liver cast containing colored resin in the portal vein and bile duct. The paracaval branch of the portal vein and bile duct was demonstrated on the cut surface along the Rex-Cantlie's line. The boundary of the caudate lobe should be decided based on the portal segmentation, not by biliary segmentation.
Funding: This study was supported by Grants-in-Aid for Scientific Research. Grant Number JP20K09019.
Conflict of Interest
The authors have no conflicts of interest to disclose.
References
- 1. Kumon M. Anatomy of the caudate lobe with special reference to portal vein and bile duct. Acta Hepatol Jpn. 1985; 26:1193-1199. (in Japanese) [Google Scholar]
- 2. Kumon M. Anatomical study of the caudate lobe with special reference to portal venous and biliary branches using corrosion liver casts and clinical application. Liver Cancer. 2017; 6:161-170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kumon M, Kumon T, Tsutsui E, Ebashi C, Namikawa T, Ito K, Sakamoto Y. Definition of the caudate lobe of the liver based on portal segmentation. Glob Health Med. 2020; 2:328-336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Couinaud C. Surgical anatomy of the liver revisited. Acheve Dimprimoer Sur Les Presses, Paris, 1989; pp.130-132. [Google Scholar]
- 5. Couinaud C. The paracaval segments of the liver. J Hep Bil Pancr Surg. 1994; 2:145-151. [Google Scholar]
- 6. Flipponi F, Romagnoli P, Mosca F, Couinaud C. The dorsal sector of human liver: embryological anatomical and clinical relevance. Hepatogastroenterol. 2000; 47:1726-1731. [PubMed] [Google Scholar]
- 7. Couinaud C. Dorsal sector of the Liver. Chirurgie. 1998; 123:8-15. (in French) [DOI] [PubMed] [Google Scholar]
- 8. Abdalla EK, Vauthey JN, Couinaud C. The caudate lobe of the liver.Implications of embryology and anatomy for surgery. Surg Oncol Clin N Am. 2002; 11:835-848 [DOI] [PubMed] [Google Scholar]
- 9. Mizumoto R, Kawarada Y, Suzuki H. Surgical treatment of hilar carcinoma of the bile duct. Surg Gynecol Obstet. 1986; 162:153-158. [PubMed] [Google Scholar]
- 10. Healey JE Jr, Schroy PC. Anatomy of the biliary ducts within the human liver; analysis of the prevailing pattern of branching and the major variations of the biliary ducts. AMA Arch Surg. 1953; 66:599-616. [DOI] [PubMed] [Google Scholar]
- 11. Ishiyama S. Clinical significance of Dorso-lateral Paracaval portion(dl-PCP). Tan To Sui. 2003; 24:75-80. (in Japanese) [Google Scholar]
- 12. Ishiyama S, Fuse A, Kuzu H, Kawaguchi K, Tsukamoto M. Rational resection of the right dorsal liver for hepatic hilar bile duct cancer. Jpn J Gastroenterol Surg. 1997; 30:2253-2256. (in Japanese) [Google Scholar]
- 13. Gadzijev EM, Ravnik D, Stanisavljevic D, Trotovsek B. Venous drainage of the dorsal sector of the liver: differences between segments I and IX.A study on corrosion casts of the human liver. Surg Radiol Anat. 1997; 19:79-83 [DOI] [PubMed] [Google Scholar]
- 14. Makuuchi M. Why is resection of the caudate lobe of the liver necessary? Geka. 1996; 58:387-391. (in Japanese) [Google Scholar]