
Figure 4. Suppressing SIRPα prevents cardiac fibrosis.
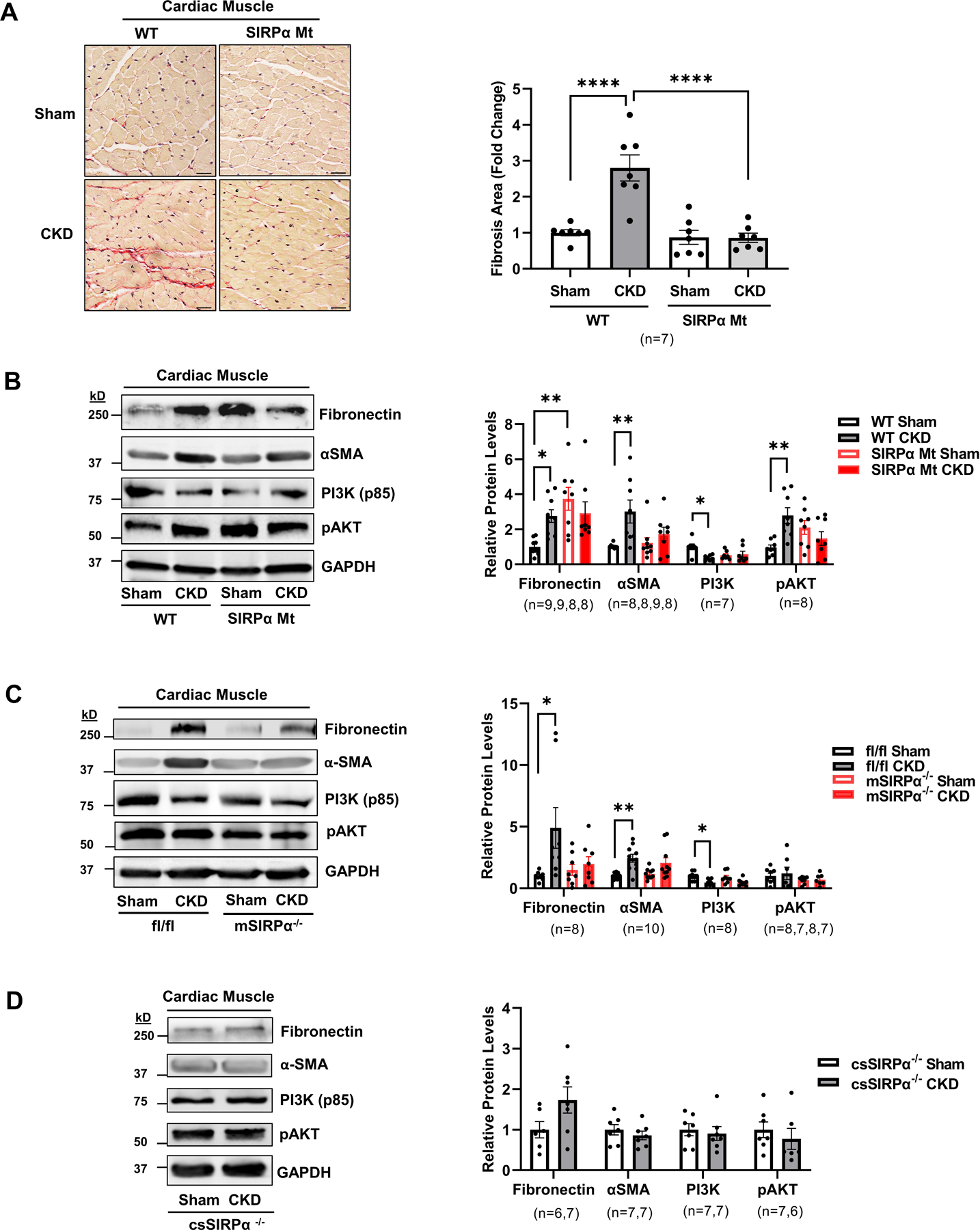
(A) Picrosirius red staining of myocardial sections for fibrosis which include representative images of averaged data are shown (left panel, scale bar=25 µm) with the fold change for fibrosis area which were analyzed in the WT and SIRPα Mt with or without CKD (right panel). After subtotal nephrectomy, heart lysates of (B) WT vs. SIRPα Mt with or without CKD, (C) muscle-specific KO (mSIRPα−/−) vs. flox (SIRPαfl/fl) with or without CKD or (D) cardiac-specific KO (csSIRPα−/−) mice with or without CKD were immunoblotted to detect fibronectin, α-SMA, PI3K (p85), and pAKT and representative immunoblots of averaged data (left panel) with relative densities to GAPDH (right panel) are shown. Statistical significance was calculated using one-way ANOVA with Bonferroni's multiple comparisons test (A-C) and unpaired two-tailed Studen's t-test (D). Values are expressed as means ± SEM; *p<0.05, ** p<0.01, **** p<0.0001.