
Fig. 22.
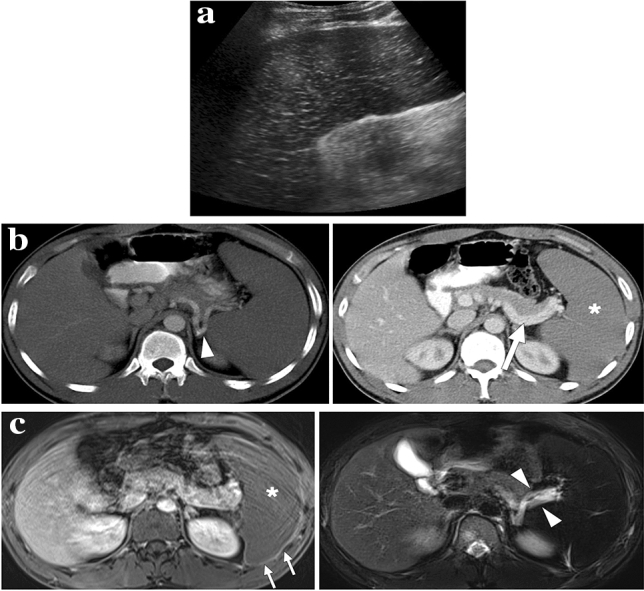
A 26-year-old male with known sickle cell-beta thalassemia trait presented to ER with left upper quadrant pain. a Longitudinal-oblique gray scale US image showed an enlarged spleen with diffuse parenchymal hypoechogenicity and multiple hyperechoic foci scattered throughout the parenchyma. b and c Axial plane arterial (b) and venous (c) phase CT images demonstrated the patency of the splenic artery (arrowhead, b) and splenic vein (arrow, C). However, diffuse hypoenhancement of the spleen was noted on the venous phase CT image (asterisk, c). d and e Axial plane T1-weighted postcontrast (d) and T2-weighted fat-suppressed (e) images showed absent parenchymal enhancement (asterisk, d), capsular rim enhancement (arrows, d) and hyperintense splenic vessels at the hilus due to slow flow (arrowheads, e). Diffuse splenic hypointensity secondary to iron deposition was also noted on axial T2-weighted image (e). Clinical and radiological findings were found to be compatible with acute splenic sequestration crisis. Histopathological examination of the splenectomy specimen revealed multiple sickle cell clusters trapped within the microvasculature and confirmed diffuse splenic infarction