
Fig. 25.
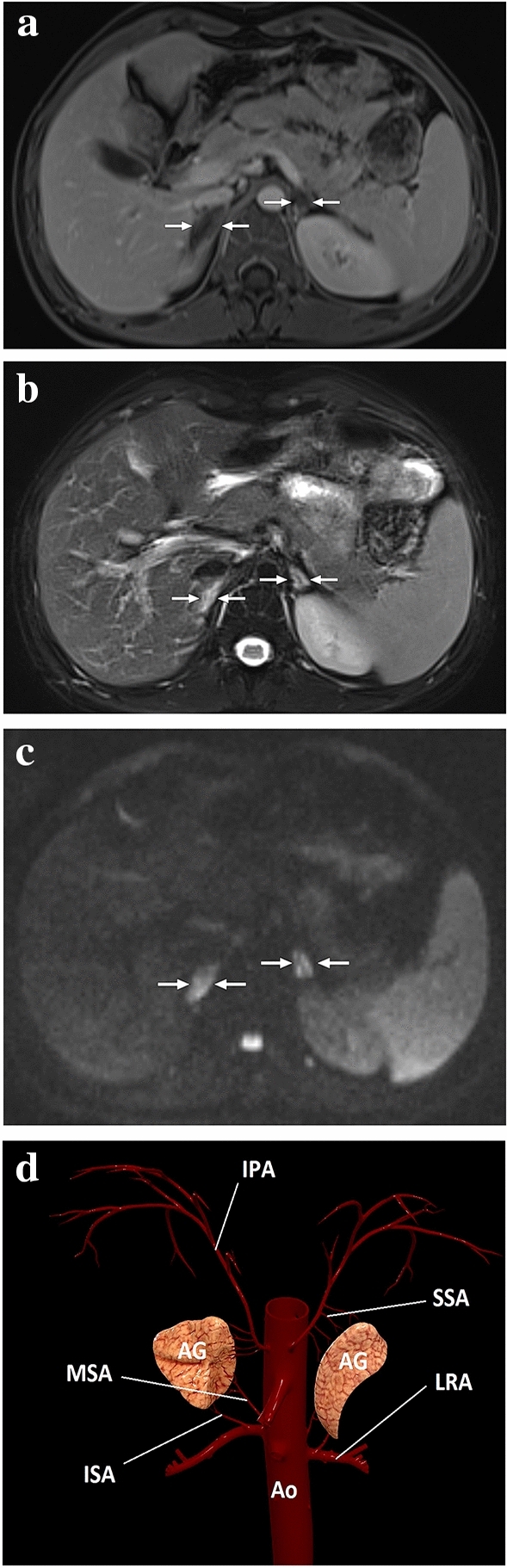
A 20-year-old male patient with adrenal insufficiency due to antiphospholipid antibody syndrome. After bilateral mild adrenal hematomas had been detected on the initial abdominal CT, the patient was immediately placed on proper steroid replacement treatment, to which he quickly responded. a One week after the initial presentation, follow-up postcontrast abdominal MRI showed non-enhancing adrenal glands with a slight rim enhancement (arrows) and resolution of the adrenal hematomas. b Adrenal glands were significantly hyperintense on T2-weighted axial images (arrows). c On DWI images, both adrenal glands were diffusely hyperintense suggestive of restricted diffusion (arrows), which was also confirmed on the ADC map (not shown). The constellation of these imaging findings and his clinical symptoms was thought to represent bilateral adrenal infarction. Follow-up MRI obtained 2 years after the initial presentation showed bilateral glandular atrophy (not shown). D A 3D illustration shows the adrenal arterial supply. IPA inferior phrenic artery, SSA superior suprarenal arteries, MSA middle suprarenal artery, ISA inferior suprarenal arteries, LRA left renal artery, AG adrenal gland, Ao abdominal aorta