

Abstract
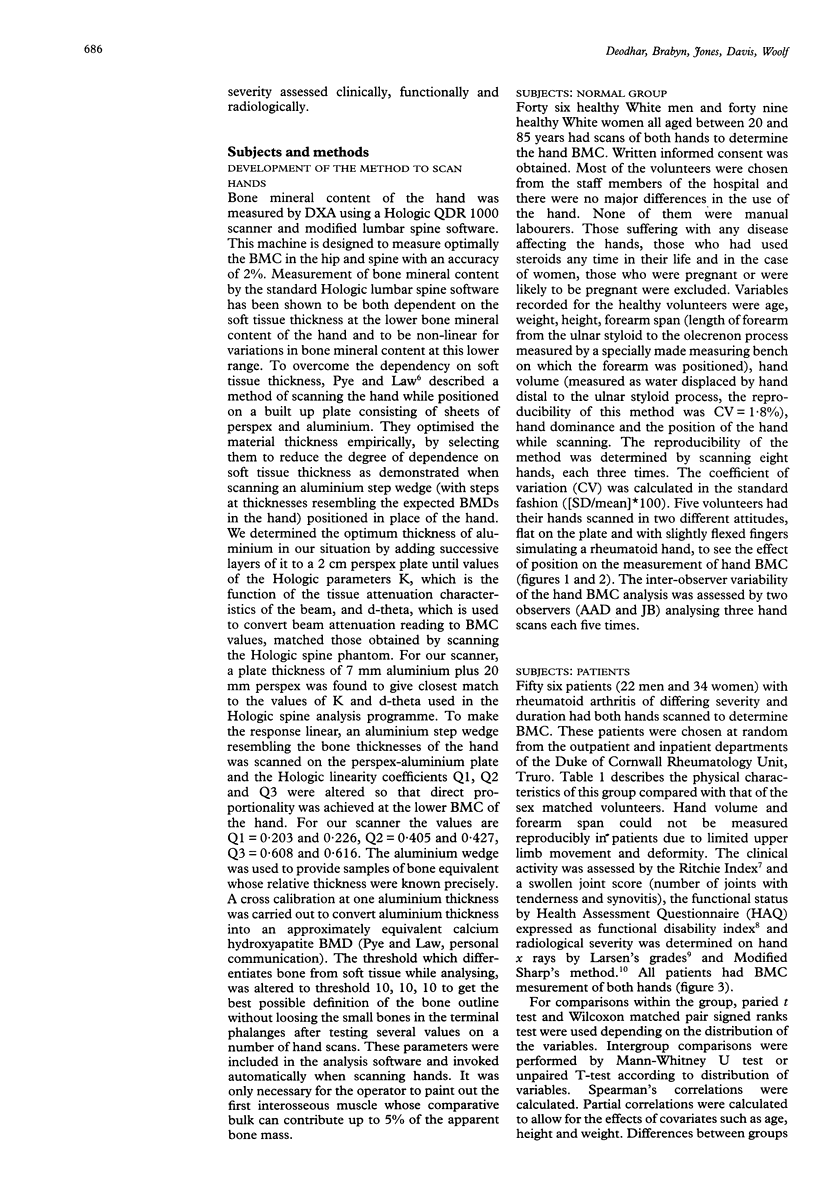
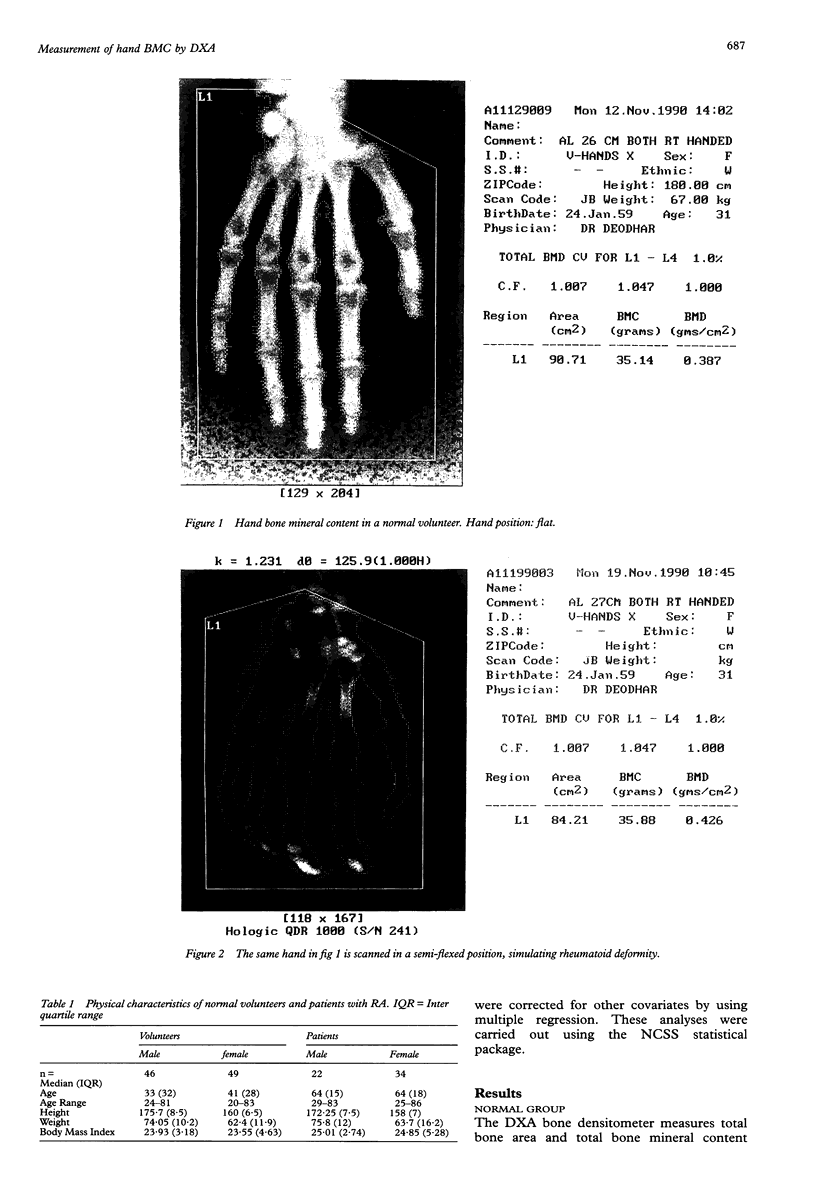
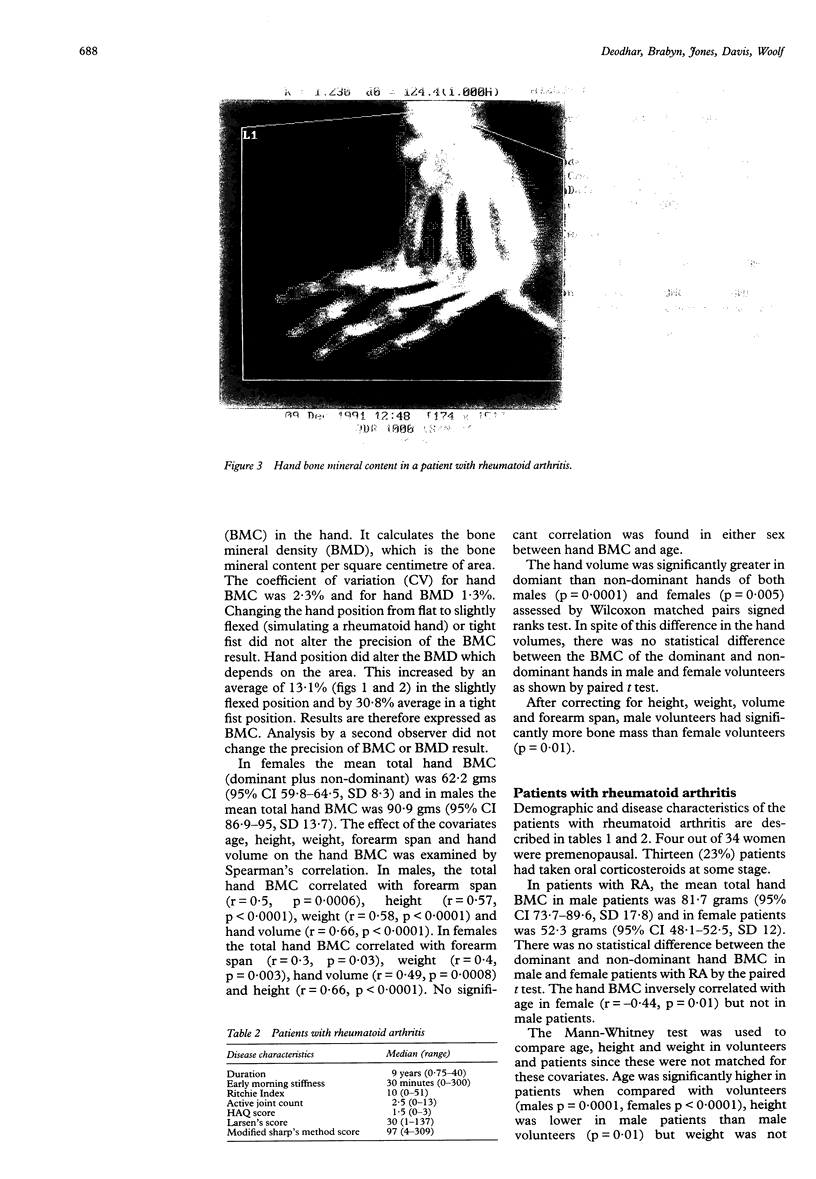
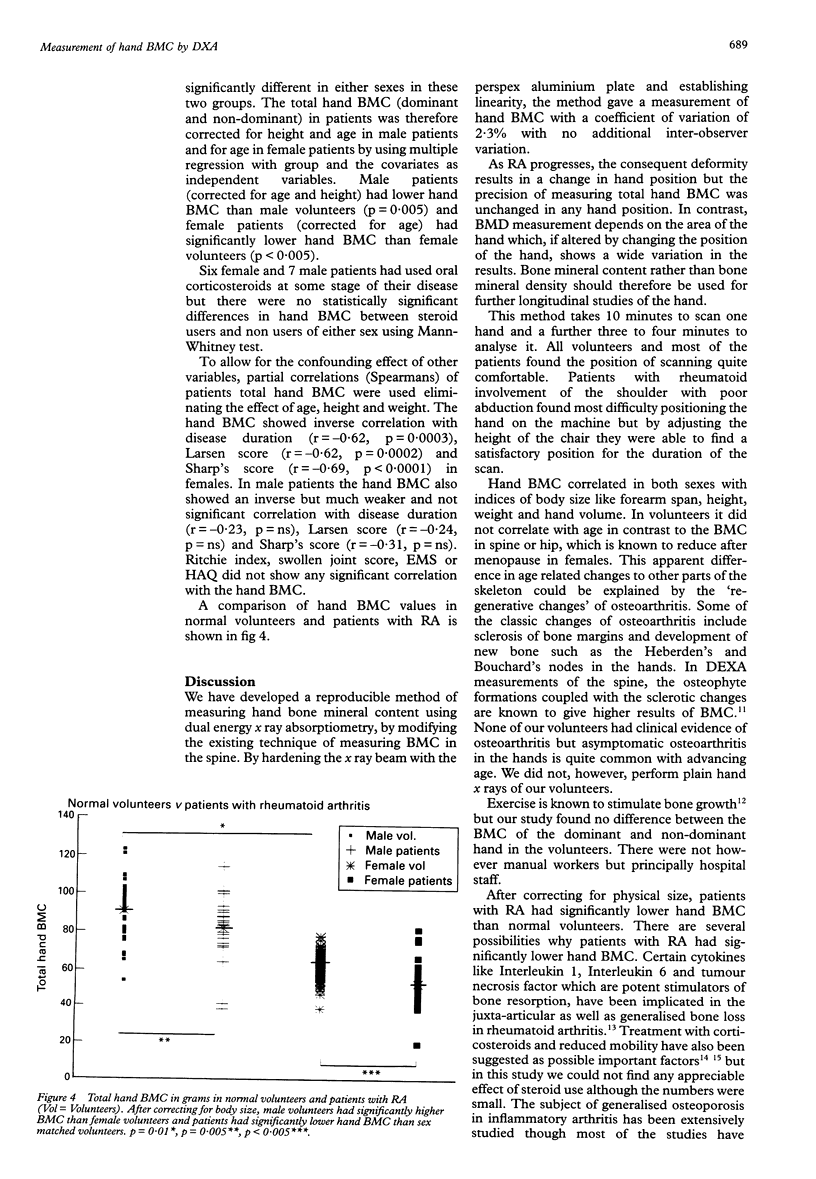
OBJECTIVES--To develop a method of measuring hand bone mineral content (BMC) by dual energy x ray absorptiometry (DXA); to apply this method of measuring hand BMC to normal volunteers to ascertain causes of variability; and to measure hand BMC in patients with rheumatoid arthritis (RA) of varying duration and severity. METHODS--The x ray beam of the Hologic QDR 1000 dual energy x ray absorptiometer was hardened by introducing a perspex-aluminium plate and the analysis software altered to allow for the small tissue bulk of the hand compared with the torso. Ninety five volunteers (46 men age 24-81 and 49 women age 20-83) had scans of both hands. Eight volunteers were assessed repeatedly to establish reproducibility and effect of hand position. Fifty six patients (22 men, 34 women, age range 25-86 years) with RA of differing duration and severity, had hand BMC measurement by DXA. RESULTS--The precision of BMC measurement was 2.3% with no additional variation due to hand position. Hand dominance had no significant effect on BMC. In men, hand BMC correlated with height (r = 0.57, p < 0.0001), weight (r = 0.58, p < 0.0001), forearm span (r = 0.5, p = 0.0006) and hand volume (r = 0.66, p < 0.0001). In women hand BMC correlated with height (r = 0.66, p < 0.0001), weight (r = 0.4, p = 0.003), forearm span (r = 0.3, p = 0.03) and hand volume (r = 0.49, p = 0.0008). After correcting for all these variables, male volunteers had significantly higher hand BMC than female volunteers (p = 0.01) and patients with RA had lower hand BMC than normal volunteers (total hand BMC in male volunteers 90.9 gms, 95% CI 86.9-95, in male patients 81.7 gms, 95% CI 73.7-89.6, p < 0.004, total hand BMC in female volunteers 62.2 gms 95% CI 59.8-64.5, female patients 52.3 gms, 95% CI 48.1-56.5, p < 0.005). In patients with RA, the hand BMC showed an inverse correlation with age (r = -0.44, p = 0.01), disease duration (r = -0.62, p = 0.0003), Larsen's grades (r = -0.62, p = 0.0002) and modified Sharp's method score (r = -0.69, p < 0.0001) in female patients only. CONCLUSIONS--A new, sensitive and reproducible technique of measurement of hand bone mineral content by DXA, has been developed and this method has been applied to normal volunteers and patients with RA. Hand dominance had no significant effect on hand BMC. After correcting for physical size, men have higher hand BMC than women. Hand BMC inversely correlates in women patients with disease duration and other validated methods of assessing radiological outcome in RA. Longitudinal studies are needed to establish its role in monitoring disease progression.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Als O. S., Gotfredsen A., Riis B. J., Christiansen C. Are disease duration and degree of functional impairment determinants of bone loss in rheumatoid arthritis? Ann Rheum Dis. 1985 Jun;44(6):406–411. doi: 10.1136/ard.44.6.406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhalla A. K., Shenstone B. Bone densitometry measurements in early inflammatory disease. Baillieres Clin Rheumatol. 1992 Jun;6(2):405–414. doi: 10.1016/s0950-3579(05)80182-7. [DOI] [PubMed] [Google Scholar]
- Brower A. C. Use of the radiograph to measure the course of rheumatoid arthritis. The gold standard versus fool's gold. Arthritis Rheum. 1990 Mar;33(3):316–324. doi: 10.1002/art.1780330303. [DOI] [PubMed] [Google Scholar]
- Fleming A., Crown J. M., Corbett M. Early rheumatoid disease. I. Onset. Ann Rheum Dis. 1976 Aug;35(4):357–360. doi: 10.1136/ard.35.4.357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fries J. F., Bloch D. A., Sharp J. T., McShane D. J., Spitz P., Bluhm G. B., Forrester D., Genant H., Gofton P., Richman S. Assessment of radiologic progression in rheumatoid arthritis. A randomized, controlled trial. Arthritis Rheum. 1986 Jan;29(1):1–9. doi: 10.1002/art.1780290101. [DOI] [PubMed] [Google Scholar]
- Gerber N. J., Rey B. Can exercise prevent osteoporosis? Br J Rheumatol. 1991 Feb;30(1):2–4. doi: 10.1093/rheumatology/30.1.2. [DOI] [PubMed] [Google Scholar]
- Larsen A., Dale K., Eek M. Radiographic evaluation of rheumatoid arthritis and related conditions by standard reference films. Acta Radiol Diagn (Stockh) 1977 Jul;18(4):481–491. doi: 10.1177/028418517701800415. [DOI] [PubMed] [Google Scholar]
- Masud T., Langley S., Wiltshire P., Doyle D. V., Spector T. D. Effect of spinal osteophytosis on bone mineral density measurements in vertebral osteoporosis. BMJ. 1993 Jul 17;307(6897):172–173. doi: 10.1136/bmj.307.6897.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meenan R. F., Gertman P. M., Mason J. H. Measuring health status in arthritis. The arthritis impact measurement scales. Arthritis Rheum. 1980 Feb;23(2):146–152. doi: 10.1002/art.1780230203. [DOI] [PubMed] [Google Scholar]
- Nanishi F., Battisto J. R. Down-regulation of adoptive adjuvant-induced arthritis by suppressor factor(s). Arthritis Rheum. 1991 Feb;34(2):180–186. doi: 10.1002/art.1780340208. [DOI] [PubMed] [Google Scholar]
- Ritchie D. M., Boyle J. A., McInnes J. M., Jasani M. K., Dalakos T. G., Grieveson P., Buchanan W. W. Clinical studies with an articular index for the assessment of joint tenderness in patients with rheumatoid arthritis. Q J Med. 1968 Jul;37(147):393–406. [PubMed] [Google Scholar]
- Sambrook P. N., Ansell B. M., Foster S., Gumpel J. M., Hesp R., Reeve J. Bone turnover in early rheumatoid arthritis. 2. Longitudinal bone density studies. Ann Rheum Dis. 1985 Sep;44(9):580–584. doi: 10.1136/ard.44.9.580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott D. L., Symmons D. P., Coulton B. L., Popert A. J. Long-term outcome of treating rheumatoid arthritis: results after 20 years. Lancet. 1987 May 16;1(8542):1108–1111. doi: 10.1016/s0140-6736(87)91672-2. [DOI] [PubMed] [Google Scholar]
- Sharp J. T., Young D. Y., Bluhm G. B., Brook A., Brower A. C., Corbett M., Decker J. L., Genant H. K., Gofton J. P., Goodman N. How many joints in the hands and wrists should be included in a score of radiologic abnormalities used to assess rheumatoid arthritis? Arthritis Rheum. 1985 Dec;28(12):1326–1335. doi: 10.1002/art.1780281203. [DOI] [PubMed] [Google Scholar]