
FIGURE 2.
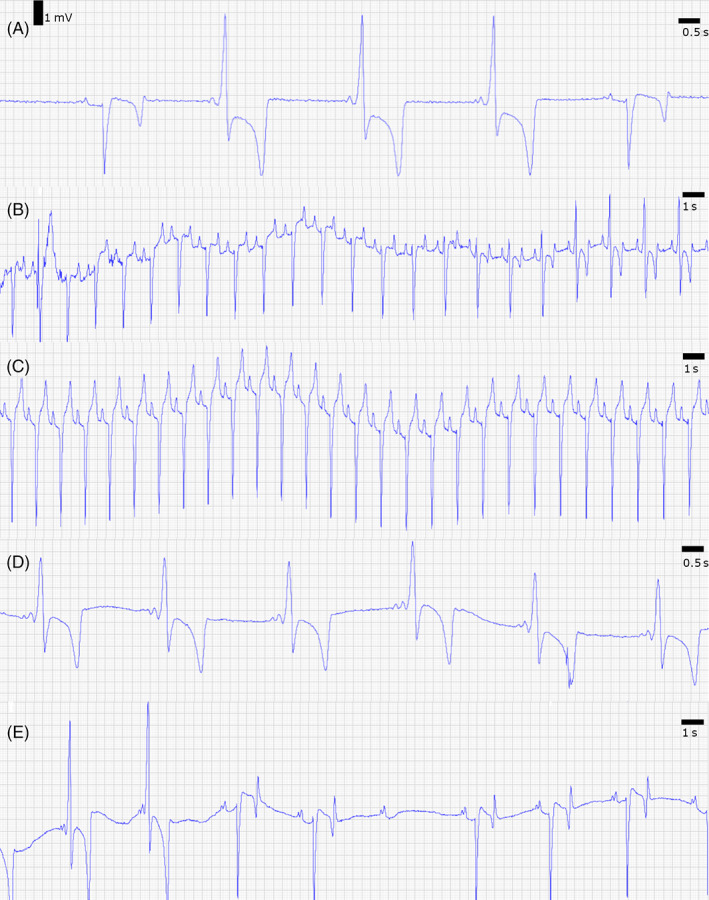
Modified base‐apex electrocardiogram (ECG) at rest (A), exercise (B), and after pharmacologic testing (C–E). 1 (A) An ECG at a resting heart rate of 44 bpm shows sinus rhythm (first and last complexes) and intermittent pre‐excitation (2rd‐4th complex). The normal complexes have a PQ interval and PQ segment of 230 and 124 ms, respectively, and a normal QRS morphology with a duration of 129 ms. The pre‐excitation complexes show a short PQ interval and PQ segment of 137 and 57 ms, respectively, and an abnormal QRS morphology with a prolonged QRS duration of 201 ms. (B) ECG during recovery after exercise at a heart rate of 88 bpm: there is a gradual transition from normal conduction to conduction along the accessory pathway. This can be observed by the progressive increase of the R wave amplitude and a shortening of the PQ intervals and segments. The pre‐excitation complexes have a PQ interval and PQ segment of 151 and 67 ms, respectively, and a QRS duration of 172 ms. (C) ECG during isoprenaline infusion (0.02 μg/kg/min) at a heart rate of 103 bpm. Isoprenaline induced sinus tachycardia with normal conduction via the AV node. These complexes have a PQ interval and PQ segment of 170 and 94 ms, respectively, and a QRS duration of 118 ms. (D) Intravenous administration of detomidine (7.5 μg/kg) IV induced ventricular pre‐excitation, with disappearance of the PQ segment. These complexes have a PQ interval of 141 ms; no PQ segment and a QRS duration of 197 ms. Blocked P waves were never observed immediately after detomidine administration. Mean heart rate is 35 bpm. (E) ECG 2 hours after detomidine injection. The first 2 QRS complexes are the result of pre‐excitation whereas the other complexes have normal PQ interval and QRS morphology. The second‐degree AV block is visible as a blocked P wave, which means that conduction over the accessory pathway also is blocked, which is rare in human patients.