

Abstract
BACKGROUND:
Metamemory can be described as an intentional endeavor to guide or control one's memory processes. In other words, awareness and knowledge of one's own memory process and strategies for using the memories effectively. Planning, allocating cognitive resources, selecting strategies, assessing understanding, and evaluating performance all rely heavily on metamemorial information. For efficient learning, good memory abilities are necessary. This study aimed to understand metamemory functioning and to see if there were any gender differences in metamemory functioning among medical students.
MATERIALS AND METHODS:
This cross-sectional study was conducted by collecting data from 350 medical students using the Memory Functioning Questionnaire in 2021. The sample group was selected from medical colleges in South India such as Kerala, Karnataka, Tamil Nadu, Telangana, and Andhra Pradesh using a purposive sampling technique. This questionnaire focused on the seriousness of forgetting, the rate at which people recalled things over time, and frequency of use of mnemonics and techniques that assist memory. Descriptive statistics, independent sample t-test, correlation, and regression were used for analysis.
RESULTS:
There was a significant difference based on gender among medical students in general memory functioning and frequency of forgetting (P < 0.001). Similarly, it was also found that gender was a major predictor of general memory functioning and frequency of forgetting among medical students (P < 0.001).
CONCLUSION:
Most medical students believe they have a minor memory issue. Even if the majority of medical students forget information, the vast majority of them believe they have an exceptional memory. Gender acts as a significant predictor of general memory performance and forgetfulness.
Keywords: Health education, health promotion, medical education, medical students, memory, metamemory
Introduction
Metamemory can be described as an awareness of one's own memory processes, often involving a conscious attempt to direct or control them. People's thoughts about memory and how memory works are referred to as metamemory. Although the phrase metamemory may appear esoteric to others, humans rely on it to execute a variety of tasks. Metamemory is significantly responsible for a person's capacity to recall information and perform effectively on memory-related tasks.[1]
Metamemory consists of two fundamental, structural components: declarative knowledge and procedural knowledge. Declarative knowledge is the ability to assess memory contents and procedural knowledge focuses on a person to keep track of and control their memory performance. At least three distinct subcomponents make up the declarative component: content and capacity information, task knowledge, and conditional knowledge about optimal memory performance. The content subcomponent allows a person to determine whether he has sufficient knowledge to perform the task. The task subcomponent allows a person to assess whether he fully comprehends the task's requirements and has sufficient resources to complete said task. The conditional knowledge subcomponent, which many consider to be the most essential of the three, assists a person in determining why, when, and where to utilize a certain approach and under what circumstances he may be most likely to achieve optimal performance.
In self-regulation, conditional knowledge is very crucial. Control and monitor subcomponents make up the procedural component. Planning, selection of relevant information, resource allocation decisions, selection of relevant tactics, and inference are all part of the control subcomponent. The monitoring subcomponent comprises of self-assessment procedures including ease-of-learning judgments, learning judgments before starting a task, feeling-of-knowing assessments made while learning, and comprehension-monitoring judgments made during or after a task. Control processes are assumed to directly regulate cognition and performance in most metamemory theories, whereas monitoring processes inform the precision of control decisions. Control processes are thus higher than monitoring processes, even though both mutually inform one another.
An individual's performance may be influenced not only by their actual talents, but also by their understanding of the situation's cognitive demand features and their expectations of the potential outcomes of their actions. Cognitive changes during early adulthood can be observed. According to Piaget (1972),[2] young adults are advanced in quantitative thinking. However, they are similar in thinking qualitatively as well. Similarly, he also believes that young adults increase their knowledge in a specific area. According to Schaie (1978),[3] young adults acquired knowledge and apply it to their everyday lives. He states that there are two cognitive changes in adults, that is, the “achieving stage” and the “responsibility stage.” In the achieving stage, an individual focuses on using one's intelligence in situations that focus on achieving long-term goals, which involve careers. This stage also involves mastering cognitive skills that require monitoring one's own behavior. Similarly, the responsibility stage begins in early adulthood and extends to middle adulthood, where they focus on establishing a family and focus on the family members’ needs and take on some level of responsibility for others at work and in the community. Young adulthood is the time when they learn and experience their life from finding a career. As students enter college, they focus on career growth and attempt to perform well academically. Students may first struggle to acclimate to college life.[4] A young adult's cognitive and psychological capacities are continually developed and honed as they advance through the developmental phases.[5] To make their learning effective and to use the stored information in their daily lives, knowledge about one's own memory is required.
Several studies have been conducted to determine the learning style of medical students.[6] It is believed that a student's learning style is a malleable attribute rather than an innate trait and that this can increase the quality of teaching and learning experiences.[7] Learning style also facilitates the acquisition, processing, and retention of new information and skills.[8] Unlike learning styles, memory functioning and strategies among medical students are not very well explored. It is important to understand subjective memory impairment among medical students as memory plays a very important role in planning and allocating cognitive resources, selecting strategies, assessing understanding, and evaluating performance. This can help the students understand their memory and improve their learning. The objective of the study is to understand the metamemory functioning, memory strategies used, and to see if there are gender differences among medical college students based on their subjective memory.
Materials and Methods
Study design and setting
A cross-sectional research study was done to understand general memory functioning, retrospective functioning, frequency of forgetting, remembering past events, seriousness of memory failure, and mnemonics usage among medical college students.
Study participants and sampling
A total of 350 medical students from different states in South India such as Kerala, Karnataka, Tamil Nadu, Telangana, and Andhra Pradesh were included in the study, out of which 173 were male and 177 were female [Table 1]. A purposive sampling technique was used in the study where participants between the ages of 18 and 35 years were included and participants above the age of 35 were excluded. Similarly, participants diagnosed with severe cognitive impairment and other psychiatric disorders were also excluded.
Table 1.
Demographic details of the participants
| Variables | Frequency (%) |
|---|---|
| Gender | |
| Male | 173 (49.43) |
| Female | 177 (50.57) |
| Age (years) | |
| 18-22 | 155 (44.29) |
| 23-27 | 195 (55.71) |
Data collection tool and technique
The data was collected using the Memory Functioning Questionnaire[9] which assesses metamemory functioning in young adults. This questionnaire consisted of the General Rating Scale, Retrospective Functioning Scale, Frequency of Forgetting Scale, Frequency of Forgetting During Reading Scale, Remembering Past Events Scale, Seriousness Scale, and Mnemonic Usage Scale. The questionnaire consisted of 64 items, but in the present study, the frequency of forgetting during reading subscale was not used. Thus, a total of 54 items were used. The questionnaire uses numeric rating scale technique. The participants were asked to rate their memory from 1 to 7 in this questionnaire. The internal consistency of the questionnaire ranges from 0.83–0.94 which indicates high reliability. Similarly, the scale established concurrent validity with respect to memory performance and depression.
Procedure
The Memory Functioning Questionnaire was available both online and offline. Based on the participants’ comfort and requests, the researchers provided the questionnaire. Before providing the questionnaire, the participants were given an informed consent form, and only after obtaining consent was the Memory Functioning Questionnaire provided for collecting the data. It was explained to the participants that “There is no correct or incorrect response. Kindly, circle/click the numbers between 1 and 7 that best reflects your judgement about your memory. Think carefully and try to be honest. Your responses would be kept confidential. Please answer all the questions.” The participants were also informed about their right to withdraw and were also assured that the information collected from them would be kept confidential and would only be strictly used for research purposes. Out of 350 participants, 151 were given a Memory Functioning Questionnaire to complete, and 199 preferred to fill out the data via the Memory Functioning Questionnaire's online form.
After the data was collected, it was analyzed using the Statistical Package for the Social Sciences (SPSS) version 20.0. Descriptive statistics, independent sample t-test, correlation, and regression were used for analysis to obtain an in-depth understanding of general memory functioning, retrospective functioning, frequency of forgetting, remembering past events, seriousness of memory failure, and mnemonic usage among medical students.
Ethical consideration
Informed consent was obtained from the participants who were willing to volunteer in the study. The information collected from the participants were kept confidential. Ethical clearance for the project was obtained from the Ethical Review Committee (IHEC-II/0037/21).
Results
The mean age of the 350 students who participated in the study was 21.65 years (Standard Deviation ± 2.50). One hundred fifty-five participants (44.29%) were between the ages of 18 and 22, and 195 (55.71%) were between the ages of 23 and 27. One hundred forty-one (40.3%) of the 350 students were male while 209 (59.7%) were female [Table 1].
The Memory Functioning Questionnaire uses a numeric rating scale consisting of subscales, one of which is general rating scale that spans from 1 (indicating “major problem”) to 7 (indicating “no problem”). The average general memory performance of the medical students was 4.65 (indicating “some minor problem”), indicating that the majority of them believed they had a minor memory problem. In a similar manner, the retrospective functioning scale evaluated the efficacy of the present and past memories. This subscale similarly employed a numeric rating scale, ranging from 1 (“much worse”) to 7 (“much better”). The results of this scale indicated that the years ranged from 1 to 20, and the mean scores of the medical students ranged from 4.75 to 4.80 (same), showing that the majority of medical students did not believe their memory had altered considerably in contrast to previous years [Figure 1 and Table 2].
Figure 1.

Retrospective memory functioning of medical students
Table 2.
Results of the Memory Functioning Questionnaire among medical students (n=350)
| Memory Functioning Questionnaire | Mean±SD |
|---|---|
| General Rating Scale | 4.65±1.46 |
| How would you rate your memory in terms of the kinds of problems that you have? | |
| Retrospective Functioning Scale | |
| One year ago? | 4.75±1.44 |
| Five year ago? | 4.65±1.60 |
| Ten year ago? | 4.55±1.64 |
| Twenty year ago? | 4.80±1.57 |
| When you were 18? | 4.60±1.53 |
| Frequency of Forgetting Scale | |
| Names | 5.10±1.65 |
| Faces | 5.90±1.41 |
| Appointments | 5.60±1.04 |
| Where you put things (e.g., keys) | 4.65±1.60 |
| Performing household chores | 4.85±1.63 |
| Direction to places | 5.0±1.68 |
| Phone numbers you’ve just checked | 5.15±1.27 |
| Phone numbers you use frequently | 5.45±1.23 |
| Things people tell you | 5.0±0.97 |
| Keeping up correspondence | 4.95±1.47 |
| Personal dates (e.g., birthdays) | 4.75±2.22 |
| Words | 4.85±1.39 |
| Going to the store and forgetting what you wanted to buy | 4.85±1.75 |
| Taking a test | 4.90±1.29 |
| Beginning to do something and forgetting what you were doing | 4.25±1.71 |
| Losing the thread of thought in conversation | 4.40±1.35 |
| Losing the thread of thought in public speaking | 4.55±1.57 |
| Knowing whether you’ve already told someone something | 4.70±1.78 |
| Remembering Past Events Scale | |
| Last month | 5.05±1.14 |
| Between six months and one year ago | 4.60±1.35 |
| Between one year and five years ago | 4.15±1.53 |
| Between six years and ten years ago | 4.05±1.60 |
| Seriousness Scale | |
| Names | 4.70±1.59 |
| Faces | 5.05±1.54 |
| Appointments | 3.90±1.45 |
| Where you put things (e.g., keys) | 4.15±1.46 |
| Performing household chores | 4.45±1.67 |
| Direction to places | 4.45±1.19 |
| Phone numbers you’ve just checked | 5.05±1.23 |
| Phone numbers you use frequently | 4.40±1.63 |
| Things people tell you | 3.75±1.51 |
| Keeping up correspondence | 4.15±1.66 |
| Personal dates (e.g., birthdays) | 4.30±1.62 |
| Words | 4.05±1.19 |
| Going to store and forgetting what you wanted to buy | 4.20±1.47 |
| Taking a test | 3.65±1.75 |
| Beginning to do something and forgetting what you were doing | 4.55±1.31 |
| Losing the thread of thought in conversation | 4.30±1.52 |
| Losing the thread of thought in public speaking | 3.85±1.50 |
| Knowing whether you’ve already told someone something | 4.35±1.22 |
| Mnemonic Usage Scale | |
| Keep an appointment book | 4.70±1.75 |
| Write yourself reminder notes | 4.30±1.81 |
| Make list of things to do | 4.80±1.50 |
| Make grocery lists | 4.60±1.96 |
| Plan your daily schedule in advance | 4.85±1.35 |
| Mental repetition | 4.80±1.47 |
| Associations with other things | 4.00±1.72 |
| Keep things you need to do in a prominent place where you will notice them | 4.25±1.58 |
In the frequency of forgetting scale, statements regarding everyday scenarios were given to rate frequency of forgetting. The rating ranged from 1 (“always”) to 7 (“never”). The mean score varied from 4.25 to 5.90 (“sometimes”), which indicates that most of the medical students felt that they sometimes forget. Similarly, the past events scale rating ranged from 1 (“very bad”) to 7 (“very good”) which focuses on a person's capacity to recall information from the previous month to 10 years ago. The average score ranged from 4.05 to 5.05 (“fair”), indicating that most medical students believed they were good at remembering past events.
When it came to the seriousness scale, the rating ranged from 1 (“very serious”) to 7 (“not serious”). The mean scores ranged from 3.65 to 4.70 (“somewhat serious”), indicating that most medical students consider memory failure as somewhat serious. In the mnemonic usage scale— techniques used by the individual to remember information—the rating ranged from 1 (“always”) to 7 (“never”). The mean score varied from 4.00 to 4.85 (“sometimes”), which indicated that the medical students sometimes used memory techniques to remember information [Figure 2].
Figure 2.
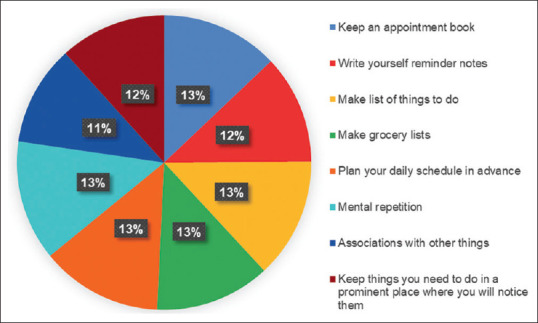
Mnemonic usage among medical students
A variation in metamemory functioning based on gender and age can be observed among medical students. P < 0.001 indicated a statistically significant difference between gender and general memory and the frequency of forgetting. The difference between the mean general memory scores of male (4.36) and female (4.86) participants indicated that female participants believed their general memory was better. Similarly, the mean score of frequency of forgetting for male (85.11) and female (91.55) participants suggested that the female medical students tended to forget less frequently than their male counterparts.
Similarly, there appeared to be a statistically significant difference between age and general memory functioning, retrospective functioning, frequency of forgetting, seriousness, and mnemonic usage among medical students at both P < 0.001 and P < 0.05. Based on the mean scores of each subscale for each age group, we can conclude that with the exception of the seriousness scale students between the ages of 23 and 27 have good general memory, retrospective functioning, forget less, and have a better use of mnemonics than those aged 18 to 22. In contrast, 18- to 22-year-olds described memory problems as a more serious concern than 23- to 27-year-olds [Table 3].
Table 3.
Demographic characteristics and Memory Functioning Questionnaire scores (n=350)
| Variable | n (%) | General Functioning | Retrospective Functioning | Frequency of Forgetting | Remembering Past Events | Seriousness | Mnemonics Usage | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
||||||||
| Mean (SD) | t | Mean (SD) | t | Mean (SD) | t | Mean (SD) | t | Mean (SD) | t | Mean (SD) | t | ||
| Gender | |||||||||||||
| Male | 141 (40.3) | 4.36 (1.51) | 3.01* | 23.41 (6.14) | −0.32 | 85.11 (17.24) | 3.35* | 17.85 (4.33) | 0.06 | 78.58 (16.33) | −1.14 | 35.77 (9.17) | 0.17 |
| Female | 209 (59.7) | 4.83 (1.36) | 23.21 (5.65 | 91.55 (17.91) | 17.89 (5.37) | 76.50 (17.06) | 35.96 (10.79) | ||||||
| Age Group (years) | |||||||||||||
| 18-22 | 155 (44.29) | 4.24 (1.60) | −6.86* | 21.98 (5.89) | −5.37* | 86.97 (16.97) | −2.58** | 18.06 (5.15) | 0.89 | 80.05 (14.77) | 3.82* | 34.32 (11.93) | −3.61* |
| 23-27 | 195 (55.71) | 5.25 (0.83) | 25.29 (5.18) | 91.99 (18.90) | 17.58 (4.67) | 73.17 (18.77) | 38.27 (5.81) | ||||||
Statistical significance level: *(P<0.001) **(P<0.05)
Using Pearson's correlation, the relationship between gender and Memory Functioning Questionnaire variables were analyzed. The results indicate that general memory and the frequency of forgetting are significantly associated to gender (P < 0.05 and P < 0.01, respectively) [Figure 3]. Then regression analysis was conducted, where gender was presented as an independent variable and the variables of memory functioning questionnaire as dependent variables. The results reveal that gender is a major predictor of medical students’ general memory functioning and frequency of forgetting [Table 4].
Figure 3.

Pearson's r heatmap (Significance level: *P< 0.05, **P< 0.01, ***P< 0.001)
Table 4.
Regression analysis of gender with Memory Functioning Questionnaire (n=350)
| Variables | Coefficient | SE | t | Sig. | R 2 | 95% CI | |
|---|---|---|---|---|---|---|---|
| General Functioning | 0.159 | 0.155 | 3.01* | 0.003 | 0.250 | 0.162 | 0.771 |
| Retrospective Functioning | −0.017 | 0.638 | −0.322 | 0.747 | 0.000 | −1.46 | 1.048 |
| Frequency of Forgetting | 0.177 | 1.923 | 3.348* | 0.001 | 0.031 | 2.657 | 10.221 |
| Remembering Past Events | 0.003 | 0.542 | 0.063 | 0.950 | 0.000 | −1.032 | 1.100 |
| Seriousness | −0.061 | 1.828 | −1.138 | 0.256 | 0.004 | −5.674 | 1.516 |
| Mnemonics Usage | 0.009 | 1.108 | 0.172 | 0.863 | 0.000 | −1.989 | 2.371 |
CI=Confidence interval; Significance Level: *(P<0.001)
Discussion
Metamemory is a subcomponent of metacognition which is closely linked with academic performance.[10] Metamemory is a broad term; in this study, we focus on a few aspects of metamemory such as general memory functioning, retrospective functioning, frequency of forgetting, remembering past events, seriousness of memory failure, and the use of mnemonics. Metamemory, or subjective understanding of memory, aids an individual in improving their learning and cognitive and memory functioning. Memory and learning are crucial components of medical education.[11] In medical colleges, the ability to study efficiently is crucial for acquiring the large quantity of information and abilities required for medical knowledge.[12] There are many studies on learning but very few on the memory of medical students. Hence, the goal of this study was to understand the metamemory functioning, memory strategies used, and to see if there were any gender differences in metamemory functioning among medical students.
On the basis of the results, it can be concluded that the majority of medical students believed they had a minor memory problem in terms of general memory functioning. In retrospective functioning, medical students did not perceive that their memory had changed significantly compared to previous years. In a similar manner, the majority of medical students reported that they occasionally forgot information. Most medical students believed that they had a strong memory of past events. The majority of medical students, however, viewed memory loss as a moderately significant issue. Medical students sometimes used memory strategies to remember information.
When it came to demographic characteristics and memory functioning, there was a statistically significant difference between gender and general memory and the frequency of forgetting. Understanding of an individual's own memory functioning is referred to as general memory functioning. The results revealed that there was a substantial difference between male and female when it came to general memory performance. In general memory, female students believed their general memory was better. Similarly, female students believed that they tended to forget less frequently than their male counterparts. This could be attributed to gender-based subjective opinion differences on memory. Similarly, Almkvist et al.[13] reported that there was a substantial difference between memory problems and gender, with females reporting significantly less complaints than males. The frequency of forgetting scale results indicates the gender difference among the selected participants. Another demographic variable such as age also showed that there was a statistically significant difference between age and general functioning, retrospective functioning, frequency of forgetting, seriousness, and mnemonic usage among medical students (P < 0.001 and P < 0.05). Hence, they have good general memory, retrospective functioning, forget less, and have a better use of mnemonics.
After performing correlation analysis, regression analysis was performed to understand the relationship between gender and Memory Functioning Questionnaire variables. The correlation concluded that there is a relationship between gender, general memory, and the frequency of forgetting. Regression analysis results revealed that gender is a major predictor of medical students’ general memory functioning and frequency of forgetting. Similarly, a study done by Niedźwieńska and Zielińska[14] was congruent with our findings. Gender differences exist between two genders and are exacerbated (i.e., when individuals are in a relationship with opposite gender) but disappear when individuals are single. Additionally, a study done by McDougall et al.[15] was consistent with our study findings. Females believed they had better memory than males.
Limitation and Recommendation
The study was conducted in a limited time period and focused specially on the South Indian population. Since the study focused on medical students, the findings cannot be applied to other course students. This study focused only on individuals’ subjective memory and not objective memory. Hence, more research is needed to better understand both the aspects of memory. The research was limited to students and did not include people from various occupations and areas. Doing so can aid in determining metamemory performance and differences based on other demographic factors.
Conclusion
Metamemory has a broader scope as it focuses on different memory domains, comprising of general memory functioning, retrospective functioning, frequency of forgetting, remembering past events, seriousness of memory failure, and mnemonic usage. The results of the study conclude that the majority of medical students believe they have a minor memory problem. Medical students do not believe that their memories have altered with time. Even though the majority of medical students forget information, most medical students feel that they possess excellent memory. Memory loss is a significant issue for the majority of medical students and sometimes, medical students utilize memory strategies. Also, gender acts a major predictor of medical students’ general memory functioning and frequency of forgetting. The results of the study could be valuable in promoting and educating medical students about memory and memory strategies which improves their memory performance and reduces the negative perception about their memory.
Financial support and sponsorship
Chettinad Academy of Research and Education, Junior Research Fellowship (CARE - JRF) fund.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Schneider W. The development of metamemory. In: Schneider W, editor. Memory Development from Early Childhood Through Emerging Adulthood. Cham: Springer International Publishing; 2015. pp. 255–308. [Google Scholar]
- 2.Piaget J. Intellectual evolution from adolescence to adulthood. Human development. 1972;15(1):1–2. [Google Scholar]
- 3.Schaie KW. Toward a stage theory of adult cognitive development. The International Journal of Aging and Human Development. 1978;8(2):129–38. doi: 10.2190/1tea-m6pk-28a0-49hv. [DOI] [PubMed] [Google Scholar]
- 4.Pedrelli P, Nyer M, Yeung A, Zulauf C, Wilens T. College students: Mental health problems and treatment considerations. Acad Psychiatry. 2015;39:503–11. doi: 10.1007/s40596-014-0205-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bonnie RJ, Stroud C, Breiner H, editors. Investing in the Health and Well-Being of Young Adults. Washington (DC): National Academies Press (US); 2015. [PubMed] [Google Scholar]
- 6.Bokhari N, Zafar M. Learning styles and approaches among medical education participants. J Educ Health Promot. 2019;8:1–5. doi: 10.4103/jehp.jehp_95_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Koohestani HR, Baghcheghi N. A comparison of learning styles of undergraduate health-care professional students at the beginning, middle, and end of the educational course over a 4-year study period (2015–2018) J Educ Health Promot. 2020;9:208. doi: 10.4103/jehp.jehp_224_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sheikhbardsiri H, Sheikhasadi H, Mahani SA, Mohamadi MMD. Emotional intelligence and learning strategies of postgraduate students at Kerman University of Medical Sciences in the southeast of Iran. J Educ Health Promot. 2020;9:66. doi: 10.4103/jehp.jehp_544_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gilewski M, Zelinski E. Memory Functioning Questionnaire (MFQ) Psychopharmacol Bull. 1988;24:665–670. [PubMed] [Google Scholar]
- 10.Omprakash A, Kumar AP, Kuppusamy M, Sathiyasekaran B, Ravinder T, Ramaswamy P. Validation of metacognitive awareness inventory from a private medical university in India. J Educ Health Promot. 2021;10:324. doi: 10.4103/jehp.jehp_39_21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Azzam MB, Easteal RA. Pedagogical strategies for the enhancement of medical education. Med Sci Educ. 2021;31:2041–2048. doi: 10.1007/s40670-021-01385-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Niroula S, Niroula A. Effective way of studying and learning in medical school. JNMA J Nepal Med Assoc. 2020;58:954–956. doi: 10.31729/jnma.5258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Almkvist O, Bosnes O, Bosnes I, Stordal E. Selective impact of disease on short-term and long-term components of self-reported memory: A population-based HUNT study. BMJ Open. 2017;7:e013586. doi: 10.1136/bmjopen-2016-013586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Niedźwieńska A, Zielińska M. Gender differences in remembering about things to do depend on partnership status. Sex Roles. 2021;84:139–151. [Google Scholar]
- 15.McDougall GJ, Pituch KA, Stanton MP, Chang W. Memory performance and affect: Are there gender differences in community-residing older adults? Issues Ment Health Nurs. 2014;35:620–627. doi: 10.3109/01612840.2014.895071. [DOI] [PMC free article] [PubMed] [Google Scholar]