
Figure 3.
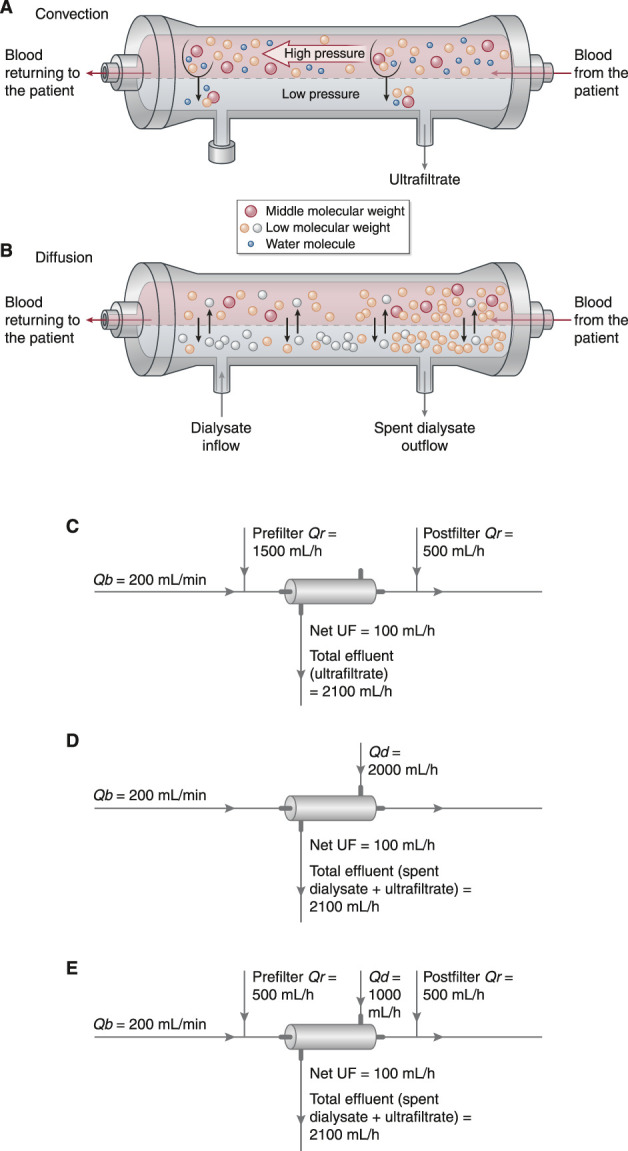
Modalities of CKRT utilize primarily convective clearance (hemofiltration), diffusive clearance (hemodialysis), or both. (A) In hemofiltration, solute clearance occurs primarily by convection. In convection, solutes are transported across the hemofilter membrane along with plasma water as a result of a hydrostatic pressure (i.e., transmembrane pressure) generated on the blood side of the membrane. Solutes cleared by convection include urea and other small molecules along with larger “middle molecules.” (B) In HD, solute clearance occurs primarily by diffusion, which is driven by a concentration gradient across the semipermeable membrane. Small solutes in high concentration in the blood diffuse across the membrane into the dialysate, which contains either little (e.g., potassium) or none (e.g., urea) of the solutes being cleared. Small solutes in higher concentration in the dialysate (e.g., bicarbonate) diffuse into the blood. Dialysate runs across the HD membrane countercurrent to the direction of blood flow to maintain a concentration gradient for removal of small solutes along the entire length of the semipermeable membrane. Modern hemodialyzers are virtually all “high-flux” dialyzers, which clear substances larger than historical low-flux dialyzers. However, unlike hemofiltration, HD does not effectively clear larger middle molecules. Ultrafiltration can be performed with HD by applying a transmembrane pressure across the membrane, but, in contrast to the high volume of ultrafiltration used to achieve significant solute clearance in hemofiltration, the volumes of ultrafiltration performed in HD are relatively small, contribute little to solute clearance, and are instead used only to achieve net volume removal. (C) In CVVH, a high volume of ultrafiltrate is generated and is replaced with an equal or (if net volume removal is desired) a somewhat smaller amount of physiologic crystalloid solution to effect net solute removal. The physiologic solution may be infused before the hemofilter (prefilter replacement fluid), into the return line (postfilter replacement fluid), or both. The net ultrafiltration rate (UF) is equal to the difference between the effluent rate and the replacement fluid rates (Qr), and it is adjusted to achieve net volume removal as desired. A typical CVVH prescription is shown, which, for a 70-kg patient, would provide a total dose of 30 ml/kg per hour and a net ultrafiltration rate of 100 ml/h (1.4 ml/kg per hour). To maintain efficient solute clearance in CVVH, blood flow rate (Qb) should be kept approximately five to six times higher than the replacement fluid rates. (D) In CVVHD, dialysate is driven through the dialyzer across the membrane from the blood flow in a direction countercurrent to blood flow. In most settings, the dialysate solution used in CVVHD is very similar or identical to the replacement fluid used in CVVH. In contrast to CVVH, ultrafiltration in CVVHD makes only minor contribution to solute removal but is performed primarily for the purposes of volume management, with ultrafiltrate generated at a rate equal to the desired rate of fluid removal. The effluent consists of both the spent dialysate and ultrafiltrate, and the net ultrafiltration rate is equal to the difference between the total effluent flow rate and the dialysate flow rate (Qd). A typical CVVHD prescription is shown, which, for a 70-kg patient, again provides a total dose of 30 ml/kg per hour and a net ultrafiltration rate of 100 ml/h (1.4 ml/kg per hour). To maintain efficient solute clearance in CVVHD, blood flow rate should be kept approximately 2.5 times higher than the dialysate flow rate. (E) CVVHDF combines a high volume of ultrafiltration coupled with replacement fluid (to achieve solute clearance by convection) with dialysate perfused across the membrane countercurrent to blood flow (to achieve solute clearance by diffusion). As in CVVH, ultrafiltrate volume in excess of the desired rate of fluid removal is replaced with a physiologic crystalloid solution that may be infused before the hemofilter (prefilter replacement fluid), into the return line (postfilter replacement fluid), or both. The effluent consists of both the spent dialysate and ultrafiltrate with the net ultrafiltration rate equal to the difference between the total effluent flow rate and the sum of dialysate and total replacement fluid flow rates. A typical CVVHD prescription is shown, which, for a 70-kg patient, again provides a total dose of 30 ml/kg per hour and a net ultrafiltration rate of 100 ml/h (1.4 ml/kg per hour). Adapted from refs. 88 and 89, with permission.