

Abstract
Introduction:
Increasing administrative workload is linked with lower quality of patient care and physician burnout. Conversely, models involving pharmacists can positively impact patient care and physician well-being. Research has consistently demonstrated that pharmacist-physician collaboration can improve outcomes for chronic diagnoses. Pharmacist-managed refill services may improve provider workload measures and clinical outcomes.
Methods:
This was an evaluation of a pharmacist-managed refill service at a Federally Qualified Health Center (FQHC). Under collaborative practice agreement, pharmacists addressed refill requests and recommended interventions. Data analysis evaluated effectiveness of the model, including clinical interventions, and involved descriptive statistics and qualitative approaches.
Results:
Average patient age was 55.5 years old and 53.1% were female. Turnaround time was within 48 h for 87.8% of refill encounters. During an average of 3.2 h per week, pharmacists addressed 9.2% (n = 1683 individual requests in 1255 indirect patient encounters) of the total clinic refill requests during the 1-year study period. In 453 of these encounters (36.1%), pharmacists recommended a total of 642 interventions. 64.8% of these were need for appointment (n = 211) or labs (n = 205). Drug therapy problems and medication list discrepancies were identified in 12.6% (n = 81) and 11.9% (n = 76) of encounters, respectively.
Discussion and Conclusions:
The results of this study are consistent with previous literature demonstrating the value of interprofessional collaboration. Pharmacists addressed refills in an efficient, clinically effective manner in an FQHC setting. This may positively impact primary care provider workload, patients’ medication persistence, and clinical care.
Keywords: collaborative practice, pharmacist, medication adherence, refill, medication management
Key Points
What is already known:
- Pharmacists make important contributions to chronic disease management in the outpatient and community pharmacy settings.
- Team-based care models in the outpatient setting involving pharmacists contribute to improved patient care and reduced rates of primary care provider colleague burnout.
- Pharmacist-managed refill services have been shown to improve turn-around time and patient access to medication refills, among other benefits.
What this study adds:
- One pharmacist FTE is likely sufficient to manage the refill volume for a moderately-sized FQHC system.
- Pharmacist identified interventions related to need for follow up or drug therapy changes in 23.4% and 8.8% of refill encounters respectively.
Introduction
Primary care providers (PCPs) have reported increasing administrative duties and tasks outside of the office as major contributors to burnout and low professional fulfillment. Conservative estimates show that about half of healthcare providers in the U.S. experience some degree or symptom(s) burnout, and numbers are even higher in primary care.1,2 In addition to answering patient messages, clinicians are often expected to address lab results, imaging findings, and refill requests. Such administrative duties have been estimated to add an additional 2 h of work spent for every hour of direct clinical face-to-face time with patients. 3 One study estimates that outside of office visits, full time PCPs receive about 12 prescription refill requests per day, often including multiple medications and requiring varying degrees of chart review. 4
Workflow changes aimed at reducing time pressure have been shown to improve both burnout and clinician satisfaction. 5 Further, by augmenting certain clinical and administrative responsibilities, physician-pharmacist collaboration has been shown to reduce PCP workload and lower rates of burnout. 1 Pharmacists, with their extensive training in medication therapy, are well-positioned to contribute to chronic disease management in primary care. Pharmacist-provided comprehensive medication management services have positively impacted all aspects of the Quadruple Aim: better care, reduced health care costs, an improved patient experience, and provider well-being. 6 A recent study by Porter et al demonstrated that providing guideline-driven primary care to all adults would require 26.7 h per day per PCP in our current medical system without team-based care. 7
Together, these factors indicate an important opportunity and urgent need for the expansion of clinical pharmacy services. Historically, many physician-pharmacist collaborative clinical services have involved focused disease state management and comprehensive medication management wherein pharmacists provide intensive patient education and make medication-related interventions. Community and ambulatory care pharmacist involvement in chronic disease care has been shown to improve outcomes for conditions including diabetes, asthma, COPD, hypertension, heart failure, hyperlipidemia, and HIV/AIDS among others.8,9 This includes disease-related clinical outcomes (eg, A1C, blood pressure, lung function), as well as reductions in serious adverse drug events, improved medication adherence or persistence, and humanistic measures such as increased patient satisfaction.9-11
Pharmacist-managed refill services have been successfully implemented in primary care practices, with more recent expansion into specialty clinics such as rheumatology.12,13 These services may involve one or more pharmacists providing indirect patient care, including evaluation and approval of refills, under a collaborative practice agreement. The published literature includes examples of effective pharmacist-managed refill services dating as far back as the late 1970s.14-16 These services have demonstrated multiple benefits, including decreased turnaround time for refills, improved patient care through interventions such as identification of drug therapy problems (DTPs), scheduling follow-up care, and medication monitoring. Refill services have also been found to increase patient satisfaction, and reduce physician workload.13,17,18 By reducing the administrative workload, pharmacist-managed refill services have demonstrated the potential to improve provider perception of burnout, and also to reduce delays and errors in patient care. 19
There is, however, a need for additional research in this area involving clinics that provide care to underserved communities and populations. Additionally, very few studies have focused on the rates and types of medication therapy interventions completed by pharmacists in collaborative refill services.
Objectives
To assess the administrative and pharmacist workflow effectiveness of a refill service.
To evaluate the clinical value of a refill service through assessment of identified and resolved drug therapy problems.
Methods
This is a reporting of experiences and a prospective assessment of a pilot pharmacist-managed refill clinical service at a multi-site Federally Qualified Health Center (FQHC) in a major metropolitan center from September 1, 2020 through August 31, 2021. Similar to other FQHCs, the clinic system serves primarily disadvantaged communities. A large majority have income below the federal poverty limit, rely on state and/or county medical coverage (eg, Medi-Cal, California’s Medicaid program), and experience a range of other socioeconomic barriers. Through more than 122 000 total patient visits, the clinic served more than 22 000 people in 2021, over 70% of whom represent racial and/or ethnic minority groups. There are approximately 12.5 PCP full-time equivalents (FTEs). In addition to primary care, the clinic provides pediatric, dental, pharmacy, behavioral health, and specialty medical services; it is also a teaching site for medical and pharmacy residents and students.
Pharmacists and supervised student and resident pharmacists provided refill services under a collaborative practice agreement with interprofessional PCPs, including physicians, nurse practitioners and physician assistants practicing at all 4 clinic sites.
Under the collaborative practice agreement, pharmacists authorize, decline, or recommend interventions on refill requests as clinically appropriate. A number of factors were evaluated to determine the appropriateness of refill approval and/or need for intervention for requests sent to PCPs from internal and external dispensing pharmacies (Figure 1). Pharmacists review each request for inclusion and exclusion criteria (described below), whether the order was consistent with the patient’s active medication list in the clinic EHR, need for labs or provider appointments, and finally clinical appropriateness or need for optimization. Issues with any of these were addressed through communication to PCPs or other staff to schedule appointments.
Figure 1.

Pharmacist refill service workflow and process.
Requests may have continued through the process when recommended interventions were identified based on case-by-case assessment at each step (dashed arrows).
*List of standard drug therapy problems: indication (requires additional drug therapy), indication (unnecessary drug therapy), effectiveness (requires different drug product), effectiveness (dosage too low), safety (adverse drug reaction), safety (dosage too high), adherence (non-adherence), other drug interaction issue.
Requests that did not meet inclusion and exclusion criteria were forwarded to the patient’s PCP. Inclusion criteria were as follows: (1) Established patients ≥18 years old who have had an in-office or telemedicine encounter with an clinic PCP within the preceding 12 months (2) Refill requests for medication(s) used to treat chronic conditions OR included in one of the following for which pharmacists in California have independent authority to provide treatment: naloxone, self-administered hormonal contraception, tobacco cessation medications, HIV pre-exposure prophylaxis (PrEP). The following drug classes and categories comprised exclusion criteria: controlled substances, medications used to treat any acute condition except naloxone, medications used to treat chronic or acute pain (NSAIDs, acetaminophen, muscle relaxants, and others), proton pump inhibitors, and medications used to treat bacterial or fungal infections.
Pharmacists determined whether the requested medication matched the patient’s current medication list and reviewed relevant laboratory and other monitoring parameters. To ensure continuity of care, the patient’s most recent and upcoming visit dates were assessed. Clinical appropriateness of medication regimens was determined according to clinical guidelines and disease-specific standards of care.
When clinically appropriate, pharmacists approved one or more refills up to a total of 180 days’ supply. If a DTP was identified or other intervention was needed, pharmacists recommended a course of action to the patient’s PCP and/or other clinic staff for purposes of scheduling appointments or addressing other needs. Information was also communicated to requesting pharmacies via phone, electronic messaging or prescription notes when necessary.
The primary outcome of this study was the feasibility and workflow effectiveness of the service. This was measured by the number of encounters and refill orders addressed per hour of pharmacist work, and proportion of requests addressed within 48 h.
Secondarily, we evaluated the clinical value of the pharmacist-managed refill service based on the quantity and type of interventions made, as well as trends in the medications, medication classes, and diagnoses involved. Types of interventions included recommendations to resolve DTPs, discrepancy with current electronic health record medication list, follow-up appointment or lab due, referral to pharmacy clinic, information clarified with patient, insurance issues resolved, and whether the requesting pharmacy was contacted. Data on drug-related problems for individual patients were collected, and the most common types of problems were identified. Multiple interventions may have applied to a single encounter or requested refill, and did not necessarily preclude a refill from being approved.
Study variables collected for those encounters where an intervention was made included date of birth (age), gender, history of visit(s) in physician residency clinic, time between receipt of request and response (ie, turnaround time), and type of intervention(s) recommended. Demographic variables were collected from patient electronic health record. Mean age was calculated using the age of each patient at the time the refill request was responded to.
Interventions were categorized as “follow up due,” “lab due,” “discrepancy with medication list,” “drug therapy problem identified,” “referral to internal clinical pharmacy service” (eg, diabetes clinic, anticoagulation clinic, tobacco cessation clinic), or “coverage issue resolved.” Need for follow up and labs was determined based on general and clinic standards of care with consideration for patient-specific medical complexity. Medication list or profile discrepancies were defined as mismatch between the refill request and patient’s current medication profile with regard to drug, dose, frequency, or route of administration. DTPs were categorized according to commonly used standardized lists.20,21 Patients were referred for clinical pharmacy services if they met internal referral criteria and had not yet been referred. Coverage issues included need for prior authorization or therapeutic interchange according to existing procedures established by clinic pharmacy and therapeutics committee or in consultation with the patient’s PCP. Further, information was clarified with either the patient, requesting pharmacy, or PCP if needed.
Finally, a retrospective chart review was completed in order to evaluate the proportion of DTP interventions that were resolved by PCPs within 3 months. An intervention was considered to be resolved if the PCP acted on or responded to the recommendation. An intervention need not have been accepted exactly as recommended to be considered resolved.
Descriptive statistical analysis and qualitative assessment were used to quantify and describe trends in pharmacist productivity and medication interventions. The mean age, proportion of female and male patients, and percentage of patients who saw resident physicians were calculated. Additionally, the percentage of refill encounters that required pharmacist intervention as well as the types of interventions and proportion of various drug therapy problems are reported. Finally, the percentage of drug therapy problems that were resolved or responded to was calculated.
A protocol for this project has been approved (IRB#: HS#2020-6300, e-APP# 15724) by the IRB at the University of California, Irvine. Data collection was completed concurrently with provision of indirect patient care. As such, informed consent was not feasible nor required by IRB; this type of work carries minimal risk of patient harm. This research was unfunded.
Results
The mean age of patients for whom a pharmacist intervention was made on the refill requests (N = 407 unique patients) was 55.5 years old, and 53.1% were female. Nearly half of patients (47.9%) were part of the physician residency clinic ([Table 1). These measures were reflective of the adult clinic patient population, and thus likely representative of the total study population. Turnaround time for a large majority of the refill requests (87.8%) was within 48 business hours.
Table 1.
Selected Patient Characteristics For Encounters That Included One or More Intervention(s) [N = 407].
| Mean age | 55.5 years (range 18-89 years) |
|---|---|
| Female | 53.1% (n = 241) |
| Residency clinic patients | 47.9% (n = 229) |
Data collection ran from September 2020 through August 2021, during which time pharmacists addressed 1683 individual refill requests in 1255 indirect patient encounters. This accounts for 9.2% of the total refill volume for adult PCPs in the clinic system during the study period. This represents the proportion of requests pharmacists were able to manage given a relatively small number of weekly hours dedicated to the pilot service. The remainder of requests were managed by individual primary care providers according to previously established procedures. Primarily, this meant PCPs addressing refill requests for their own panel of patients, but there were instances of cross coverage. Data was not available to determine the proportion of all primary care refill requests that met the inclusion criteria or were excluded. However, it is presumed to be high as essentially all primary care patients are over age 18, and the group of excluded medications is relatively narrow. Pharmacists addressed (either approved or declined) an average of 10.1 refill requests in 7.5 unique refill encounters per hour. Because of COVID-19 related factors, pharmacist time dedicated to the refill service was variable between 1 and 10 h per week during the study period, with an average of 3.2 h per week.
Summarized in Figure 2, a total of 453 encounters (36.1%) resulted in 642 pharmacist recommendations for medication interventions. The 2 most common types of interventions were patients being due for follow-up visits (32.9%, n = 211) and/or due for labs (31.9%, n = 205). Pharmacists also identified 83 DTPs in 81 encounters (12.6%) and 76 instances (11.9%) of medication profile discrepancies. Forty-six patients (7.2%) were identified to benefit from being referred to one of the other internal clinical pharmacy services, and 22 (3.4%) required clarification of information with the patient or pharmacy or resolution of a coverage issue. More than one type of intervention may have been identified for a given patient and/or medication.
Figure 2.
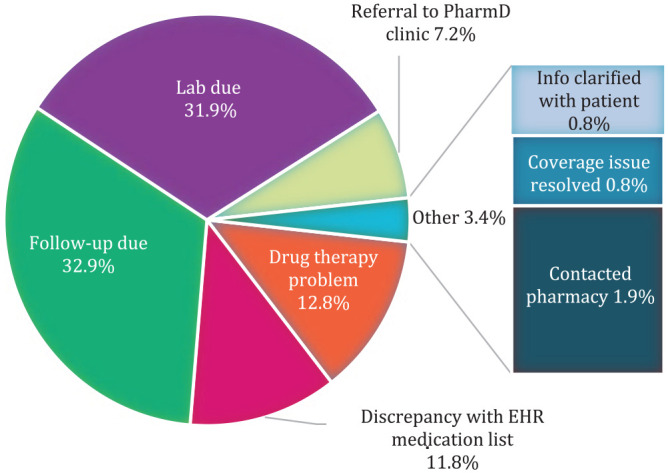
Pharmacist refill interventions by type [N = 642].
Table 2 details the categories of DTPs identified (N = 83). The most frequently identified DTPs were “dose too high” (n = 17, 20.5%) and “dose too low” (n = 20, 24.1%). Frequent examples of dosing issues include need for taper, titration, or renal dosing. “Requires different drug product” also represented a significant proportion of DTP interventions (n = 18, 21.7%). The most common specific intervention in this category involved recommendations to change sulfonylureas to preferred therapies for patients with type 2 diabetes consistent with current treatment guidelines. “Unnecessary drug therapy” comprised an additional significant proportion of interventions (n = 17, 20.5%). Examples here include recommendations to discontinue orders for aspirin for ASCVD prophylaxis in low-risk patients, as well as various therapeutic duplications. Other DPTs identified include “requires additional drug therapy” (n = 6, 7.2%), such as a statin for ASCVD prevention, “non-adherence” (n = 3, 3.6%), and “adverse drug reaction” (n = 1, 1.2%). The adverse reaction identified was a clinically significant increase in serum creatinine following initiation of lisinopril.
Table 2.
Standardized Drug Therapy Problems (DTP) Identified (N = 83).
| Drug Therapy Problem category | n (%) |
|---|---|
| Indication | |
| Requires additional drug therapy | 6 (7.2) |
| Unnecessary drug therapy | 17 (20.5) |
| Effectiveness | |
| Requires different drug product | 18 (21.7) |
| Dosage too low | 20 (24.1) |
| Safety | |
| Adverse drug reaction | 1 (1.2) |
| Dosage too high | 17 (20.5) |
| Adherence | |
| Non-adherence | 3 (3.6) |
| Other drug interaction issue | 1 (1.2) |
Of the 83 recommended medication therapy interventions, 31 (37.5%) were resolved within 3 months, and 46 (55.4%) were not addressed. For 6 interventions (7.2%), PCP response was indeterminate or the patient was lost to follow-up (eg, transferred care to another clinic; Table 3).
Table 3.
Status of Drug Therapy Problem Interventions and Recommendations at 3 Months (N = 83).
| Status | n (%) |
|---|---|
| Addressed/resolved | 31(37.3) |
| Not addressed/not resolved | 46 (55.4) |
| Undetermined or lost to follow up | 6 (7.2) |
Discussion
The results from this study highlight the effectiveness and importance of pharmacist involvement in the medication refill process. The finding that 9.2% of requests were managed via an average of 3.2 pharmacist hours per week indicates that one dedicated clinical pharmacist FTE is likely sufficient to manage the majority of refill volume for a similarly-sized clinic system as measured by annual patient visits (about 120 000) or PCP FTEs (about 12.5). A recommendation may be for 32 h of pharmacist time allocated to manage requests that meet inclusion criteria with an additional 8 h of administrative time to follow-up on specific refill issues or other related activities such as prior authorizations. These results are consistent with recent literature demonstrating that team-based care is necessary for PCPs to provide quality patient care and manage administrative tasks given the high ratio of patients to providers. 7 Integrating a pharmacist has the potential to augment other efforts to address PCP administrative workload in an FQHC setting. Turnaround time within 2 business days for the large majority of requests indicates efficiency of this process, and demonstrates potential to positively affect medication adherence and persistence. Workflow changes associated with a pharmacist-managed refill service may translate to increased face-to-face patient interaction time for PCPs and support sustainable interprofessional practices, similar to those reported by Rim et al 17 Moreover, even in cases where the pharmacist did not make a final decision on the refill renewal request, recommendations were provided to facilitate or inform PCPs’ decision making.
In the context of previously published literature, this study represents a unique reporting of the medication interventions completed as part of a pharmacist-managed refill service. Intervention recommendations resulted from 36.1% of refill encounters in this study; this is mostly consistent with research by Nguyen and Zare that reported that interventions were needed in 42% of pharmacist-managed refills in an evaluation of over 5000 refill requests over 2 years. 13 The present work also found that laboratory monitoring was needed in 31.9% of refill encounters, similar to a past report from Billups et al that found laboratory or other monitoring to be needed in 28% of refill authorization requests. 18 These speak to the external validity of other findings related to types of interventions and drug therapy problems addressed, which are not reported on fully in previous studies.
Pharmacists are uniquely qualified to identify medication related problems and make related medication interventions and recommendations. The types of interventions identified also indicate the value of the pharmacist collaboration in responding to refill requests. The most frequent interventions (need for follow up or labs) are likely to have an impact on continuity of care and the patient experience. Identifying discrepancies between requested refill and standing medication list may also help ensure patient adherence and persistence with optimized medication therapy. Additionally, referrals to pharmacist-managed chronic disease services are important as a large body of evidence has demonstrated positive clinical outcomes associated with these care models.8-11
Clinically significant interventions for DTPs were also identified. This includes need for dose adjustment, optimization of regimen by changing to more effective or safer drugs or discontinuing those where benefit does not outweigh risk. These are particularly important for improving the efficacy and safety of medication therapy. Of note, many similar DTPs were identified and more than 80% of the DTPs identified represented only 3 categories of intervention (“dose too high/low,” “requires different drug product,” and “unnecessary drug therapy”). This demonstrates the potential of this care model to detect needs for in-service or other educational programing for PCPs.
The large proportion of patients who were under the physician residency clinic is likely related to the volume of requests received by attending physicians who precept residents, and may have played a role in increasing the number of DTPs identified. The majority of DTPs remaining unresolved at 3 months shows that there is a need to communicate recommendations to PCPs differently, including pharmacist follow up and reminders, or to allow pharmacists the authority to implement certain types of interventions directly.
The main limitation of this study is difficulty in generalizing our results outside of an FQHC or medical system setting where clinical pharmacists are already providing comprehensive medication management services. Assessment of needs and opportunities would be required prior to implementation in smaller or private practices. Additionally, this work does not comprise a full evaluation of the economic and patient outcomes related to the refill service.
Future directions for expansion of this service include increased pharmacist hours dedicated to the refill service as well as potential integration of on-site dispensing pharmacists and pharmacy technicians to facilitate prior authorizations, resolve other insurance formulary issues, and further reconcile patients’ electronic health record medication profiles with dispensing history. Follow up research may also include survey of provider satisfaction, assessment of the economic impacts of this service and clinic-wide measures related to the use of medications, as well as multi-center research by analyzing data from similar services at other FQHC clinics and/or larger FQHC groups.
Conclusions
Pharmacists can effectively contribute to the medication refill renewal process in an FQHC setting. In practices where clinical pharmacy services are already in place, a refill service represents a beneficial addition. There are positive implications for PCP workload and workflow efficiency. Additionally, patient care can be impacted with the potential to facilitate medication adherence and persistence, promote continuity of care, and optimize medication regimens.
Footnotes
Previous Presentation (poster): American Pharmacists Association Annual Meeting, March 2022
CRediT Author Statement: Keri Hurley-Kim: Conceptualization, methodology, investigation, data curation, formal analysis, visualization, writing—original draft, writing—review and editing, Azin Keyvani: investigation, data curation, writing—original draft, writing—review and editing, Raed Ahmed: supervision, project administration, writing—original draft, writing—review and editing, Hei-Wah Wong: supervision, project administration, writing—original draft, writing—review and editing, Sarah McBane: methodology, supervision, writing—original draft, writing—review and editing.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD: Keri Hurley-Kim  https://orcid.org/0000-0002-7988-3250
https://orcid.org/0000-0002-7988-3250
References
- 1.White N.Reducing primary care provider burnout with pharmacist-delivered comprehensive medication management. Am J Lifestyle Med. 2021;15(2):133-135. doi: 10.1177/1559827620976539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc. 2015;90(12):1600-1613. doi: 10.1016/j.mayocp.2015.08.023 [DOI] [PubMed] [Google Scholar]
- 3.Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753. doi: 10.7326/m16-0961 [DOI] [PubMed] [Google Scholar]
- 4.Baron RJ.What’s keeping us so busy in primary care? A snapshot from one practice. N Engl J Med. 2010;362(17):1632-1636. doi: 10.1056/nejmon0910793 [DOI] [PubMed] [Google Scholar]
- 5.Linzer M, Poplau S, Grossman E, et al. A cluster randomized trial of interventions to improve work conditions and clinician burnout in primary care: results from the Healthy Work Place (HWP) study. J Gen Intern Med. 2015;30(8):1105-1111. doi: 10.1007/s11606-015-3235-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McFarland MS, Buck ML, Crannage E, et al. Assessing the impact of comprehensive medication management on achievement of the quadruple aim. Am J Med. 2021;134(4): 456-461. doi: 10.1016/j.amjmed.2020.12.008 [DOI] [PubMed] [Google Scholar]
- 7.Porter J, Boyd C, Skandari MR, Laiteerapong N.Revisiting the time needed to provide adult primary care. J Gen Intern Med. 2023;38(1):147-155. doi: 10.1007/s11606-022-07707-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Newman TV, San-Juan-Rodriguez A, Parekh N, et al. Impact of community pharmacist-led interventions in chronic disease management on clinical, utilization, and economic outcomes: an umbrella review. Res Soc Adm Pharm. 2020;16(9):1155-1165. doi: 10.1016/j.sapharm.2019.12.016 [DOI] [PubMed] [Google Scholar]
- 9.Abdulrhim S, Sankaralingam S, Ibrahim MIM, Awaisu A.The impact of pharmacist care on diabetes outcomes in primary care settings: an umbrella review of published systematic reviews. Prim Care Diabetes. 2020;14(5):393-400. doi: 10.1016/j.pcd.2019.12.007 [DOI] [PubMed] [Google Scholar]
- 10.Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US pharmacists’ effect as team members on patient care: systematic review and meta-analyses. Med Care. 2010;48(10):923-933. doi: 10.1097/mlr.0b013e3181e57962 [DOI] [PubMed] [Google Scholar]
- 11.Antoine S-L, Pieper D, Mathes T, Eikermann M.Improving the adherence of type 2 diabetes mellitus patients with pharmacy care: a systematic review of randomized controlled trials. BMC Endocr Disord. 2014;14(1):53. doi: 10.1186/1472-6823-14-53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rottmann EI, Cote J, Thomas S, et al. Use of protocol-driven medication refills by pharmacists decreases rheumatologist in-basket work and improves rheumatologist satisfaction. BMJ Open Qual. 2022;11(1):e001566. doi: 10.1136/bmjoq-2021-001566 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nguyen M, Zare M.Impact of a clinical pharmacist-managed medication refill clinic. J Prim Care Community Health. 2015;6(3):187-192. doi: 10.1177/2150131915569068 [DOI] [PubMed] [Google Scholar]
- 14.D’Achille KM, Swanson LN, Hill WT.Pharmacist-managed patient assessment and medication refill clinic. Am J Health Syst Pharm. 1978;35(1):66-70. doi: 10.1093/ajhp/35.1.66 [DOI] [PubMed] [Google Scholar]
- 15.Jones RJ, Goldman MP, Rockwood RP, Imhoff TE.Beneficial effect of a pharmacist refill evaluation clinic. Hosp Pharm. 1987;22(2):166-168. [PubMed] [Google Scholar]
- 16.Cassidy IB, Keith MR, Coffey EL, Noyes MA.Impact of Pharmacist-operated General Medicine Chronic Care Refill clinics on practitioner time and quality of Care. Ann Pharmacother. 1996;30(7-8):745-751. doi: 10.1177/106002809603000707 [DOI] [PubMed] [Google Scholar]
- 17.Rim MH, Thomas KC, Hatch B, Kelly M, Tyler LS.Development and implementation of a centralized comprehensive refill authorization program in an academic health system. Am J Health Syst Pharm. 2018;75(3):132-138. doi: 10.2146/ajhp170333 [DOI] [PubMed] [Google Scholar]
- 18.Billups SJ, Delate T, Newlon C, Schwiesow S, Jahnke R, Nadrash A.Outcomes of a pharmacist-managed medication refill program. J Am Pharm Assoc. 2013;53(5):505-512. doi: 10.1331/japha.2013.13008 [DOI] [PubMed] [Google Scholar]
- 19.Bhakta K, Lee KC, Luke T, Bouw J.Impact of a pharmacist-run refill and prior authorization program on physician workload. J Am Pharm Assoc. 2022;62(3):727-733.e1. doi: 10.1016/j.japh.2021.12.002 [DOI] [PubMed] [Google Scholar]
- 20.Cipolle RJ, Strand L, Morley P.Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management, 3rd ed.McGraw Hill Professional; 2012. [Google Scholar]
- 21.McDonough RP, Doucette WR.Drug therapy management: an Empirical Report of drug therapy problems, pharmacists’ interventions, and results of pharmacists’ actions. J Am Pharm Assoc. 2003;43(4):511-518. doi: 10.1331/154434503322226266 [DOI] [PubMed] [Google Scholar]