

Abstract
Introduction:
Falls from heights contribute to 34% of fatal accidents in Singapore. Of these, 51% of the accidents occur in the construction industry. This retrospective review, of all persons falling from heights in the construction industry from 2006 to 2012 and attending a major hospital, analysed injury patterns and related them to mechanisms and contributory factors.
Methods:
Information collected included injury and casualty characteristics, safety measures, pre-existing medical conditions and clinical outcomes.
Results:
Of 1,085 patients, 951 were male with a mean age of 39.8 years, mean height of 165.9 cm and mean weight of 69.7 kg. Most of the casualties fell between 0800 and 2000 hours. Among the severely injured patients, 2.4% had head injuries, 54.9% had chest injuries and 39.2% had abdominal and pelvic injuries. For these casualties, the mortality rate was 60.8%. For patients with less than major trauma, the commonest injuries were in the lower limbs (41.8%), upper limbs (40.8%) and spine (22.2%). All the casualties survived. Falls from scaffolding, formwork and platforms were the most common causes of severe injuries (41.1%). Safety helmets and harnesses were reported to be used in 1.8% and 4.1% of instances of falls, respectively.
Conclusion:
Studying the patterns of injuries following falls at construction sites has the potential for injury prevention through safe practices, use of safety equipment and targeted training.
Keywords: Chest trauma, construction industry, falls from height, head injury, injury severity score
INTRODUCTION
From 2006 to 2007, falls from height contributed to 38% of all fatal accidents in Singapore and 60% of those were in the construction industry.[1] The construction industry alone was responsible for 62% of all fall-from-height related fatal accidents. In Singapore, the Work Safety and Health (WSH) (Risk Management) Regulations came into operation in September 2006,[2] and these included procedures to reduce the risk of falls in the construction industry. There were also many initiatives by the Occupational Safety and Health Department of the Ministry of Manpower (MOM) and the WSH Council to instil awareness among site personnel and assist workplaces to strengthen their risk management programmes. A Work-at-Height (WAH) Safety Taskforce was also set up with the task of enhancing the intervention framework for WAH. This was with intensive inspections, safety compliance assistance visits, development of National WAH competency standards and organisation of WSH forums and technical workshops involving WSH experts to promote the benefits of WAH Safety through outreach and educational programmes.
These efforts resulted in the reduction of the overall fatality rate of industrial accidents from 4.9/100,000 workers in 2004[3] to 2.2/100,000 workers in 2010.[4] However, in the construction industry, the overall fatality rate only decreased slightly from 9.4/100,000 workers in 2006 to 8.1/100,000 workers in 2010.[5]
The falls occurred despite the adoption of the ‘Code of Practice for Working Safely at Heights’, or simply the ‘Code’, in October 2009.[6] Fatality or morbidity in falls is often determined by the pattern of injuries.[7]
To date, there have been no local, and very few comprehensive, international studies on the patterns of injuries that result from falls in the construction industry.[8,9,10,11] Although the types of injuries from falls in general[12] and on specific body systems[13,14] have been documented previously, injuries in the construction industry occur in a special environment. The person who falls at a construction site is, usually, not only exposed to a direct free fall. He may encounter other objects during the fall, such as scaffolding, metal objects and sharp objects that may cause penetrating injuries, and may also be exposed to special machinery, especially at construction sites. Persons who use special personal protection gear may or may not suffer the same pattern of injuries. There is a need to understand the patterns of injury that may occur in unprotected falls from height in the construction industry environment. Such an understanding can contribute to better management of the factors that contribute to injuries and fatalities from such accidents and can lead to further implementation of measures to either prevent such falls or mitigate the occurrence of such injuries.
The objectives of this study were, therefore, as follows: (a) to determine the pattern of injuries that occur in those who fall from heights and the severity of these injuries using objective scores and scales such as the Abbreviated Injury Scale (AIS) and Injury Severity Scores (ISS); and (b) to relate the specific injuries with the locations of the fall and other circumstances that affect the outcomes.
METHODS
This was a retrospective study involving the collection of data of patients seen at the Department of Emergency Medicine, Singapore General Hospital, Singapore, after a fall at construction sites. An initial list of such patients who presented to the hospital for these incidents over a seven-year period from 1 January 2006 to 31 December 2012 was provided by the MOM's WSH Institute. For each of these patients, the records of the emergency department (ED) were perused to determine patient details, location of fall, types of injuries and outcomes. The hospital's electronic medical records were also searched for further information on outcomes, duration of hospital stay and of absence from work.
Inclusion criteria for the study included the following: fall from height, at construction site, not being pregnant, and age of 21 years and above.
The raw data received from MOM included the day and date of the accident; the worker's biodata; estimated height from which they fell, if available; the location of the fall; and information on the use of a safety harness or helmet, if available. The data obtained from hospital records included the presence or absence of medical comorbidities; details of injuries sustained by body region; initial outcomes of patients after initial care at the ED; medical leave provided, if any; disposition of the patients; and whether the patient died because of the incident. For those who were either admitted or followed up, the total duration of medical leave given by the hospital was also documented.
Simple data analysis involved determining the frequencies of injuries and outcomes. For all patients, AIS scores were determined and ISS scores were calculated.[15] The locations of the falls sustained were grouped as follows, to determine patterns of injury in each case.
-
(a)
Group A: falls from scaffolding, formwork and platforms and landings
-
(b)
Group B: falls from the storey of a building, mezzanine, loft, roof and top of a container
-
(c)
Group C: falls from mobile elevating work platforms, ship deck, tower, fork lifts, vehicles or top of machinery/equipment
-
(d)
Group D: falls from ladders, steps or stairs
-
(e)
Group E: falls from cranes
-
(f)
Group F: falls at ground level, into holes and excavation pits and bottoms of vessels
Correlations between injury patterns and possible contributory factors such as pre-existing medical comorbidities and heights and locations of fall were also determined. Finally, correlation of injury patterns with overall severity and clinical outcomes were determined. The study was approved by the Institutional Review Board of the Singapore Health Services, which granted complete waiver of informed consent.
RESULTS
From a total of 1,121 patients listed by MOM, 1,085 fulfilled the entry criteria for analysis [Figure 1]. Most casualties were of Chinese ethnicity (54.7%), followed by Indians (18.0%), Malays (12.4%) and other nationalities (14.9%). 951 (87.6%) of the casualties were men. The average height of the casualties was 165.9 cm, and their average weight was 69.7 kg. The mean age was 39.8 years.
Figure 1.
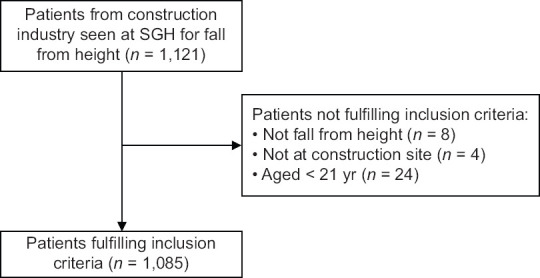
Consort table shows analysis of patients seen with fall from heights.
The highest number of falls were on Wednesdays and Thursdays. Sunday had the lowest number of falls. The proportions of falls from mobile elevating work platforms, ship deck, tower, fork lifts, vehicles, top of machinery/equipment (Group C) and also at ground level, into holes, excavation pits and bottom of vessels (Group F) were higher on Sundays than on any other day (17.1% vs. 10.1% [P = 0.036] for Group C and 10.5% vs. 7.5% for Group F [P = 0.018]). Overall, as expected, the total number of falls on Sundays was less than half that of any other day of the week. On average, the falls usually occurred from 0800 hours to 2000 hours, with a peak between 1200 hours and 1600 hours [Figure 2]. There was no significant difference by fall location in the proportion of falls in the different time zones, except during the period of 2000 hours and 2359 hours, when an increased proportion of falls was noted at Group C locations (20.3% vs. an average of 10.6% for the whole day; P = 0.012), and a lower proportion of falls from Group D (35.1% vs. an average of 51.2% for the rest of the day; P = 0.008).
Figure 2.
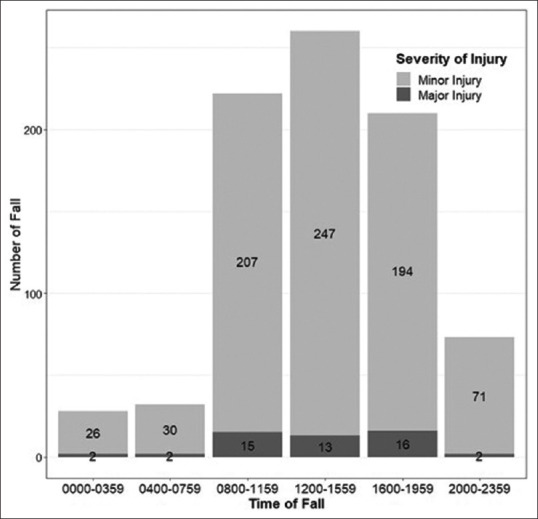
Bar graph shows distribution of falls at construction sites by time of day.
Most falls (50.8%) were from a height of less than 2 m. From other heights, the frequency of falls was 38.3% from 2.0 m to 3.9 m, 4.2% from 4.0 m to 5.9 m and 6.6% from >6.0 m. There was good correlation (analysis of variance; P = 0.001) between the height of fall and severity of injury, with patients having an ISS >15 for falling from a significantly greater height. The relationship between ISS and fall height in our patient population is expressed graphically in Figure 3.
Figure 3.
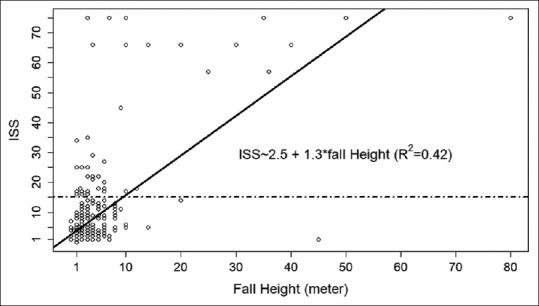
Graph shows injury severity by height of fall. ISS: Injury Severity Score
The falls were from a variety of locations at the construction sites. Although Group D accounted for 51.2% of all falls, it only contributed to 19.6% of severe injuries, unlike Group A, which accounted for only 22.4% of the falls but contributed to 41.1% of the severely injured [Table 1]. Similarly, although in much smaller numbers, those who fell from cranes constituted only 2.7% of all falls but made up 8.9% of the severely injured. Those falling from cranes had the highest likelihood (17.2%) of serious injury compared to those who fell from other locations; among the latter, the incidence of serious injury varied from 2.0% to 9.5%. Of the 134 female workers who fell, only one was from a height of 3 m; all the others were either at ground level or up to 2 m above ground level in or near construction site offices. Most of these were from slipping or tripping at ground level (28.2%); chairs, steps and stairs (26.8%); ladders (22.4%); and falling into pits and holes (12.7%).
Table 1.
Frequency of falls by location at the construction site and injury severity.
| Location group | Locations | Frequency (%) | n (%) | ||
|---|---|---|---|---|---|
|
| |||||
| ISS >15 (n=56) | ISS <15 (n=948) | ISS not indicated (n=81) | |||
| A | Scaffolding, formwork and platforms and landings | 243 (22.4) | 23 (41.1) | 198 (20.9) | 22 (27.2) |
|
| |||||
| B | Storey of building, mezzanine, loft, roof and top of container | 51 (4.7) | 4 (7.1) | 42 (4.4) | 5 (6.2) |
|
| |||||
| C | Mobile elevating work platforms, ship deck, tower, fork lifts, vehicles or top of machinery/equipment | 115 (10.6) | 6 (10.7) | 100 (10.5) | 9 (11.1) |
|
| |||||
| D | Ladders, steps or stairs | 555 (51.2) | 11 (19.6) | 505 (53.3) | 39 (48.1) |
|
| |||||
| E | Cranes | 29 (2.7) | 5 (8.9) | 24 (2.5) | 0 (0) |
|
| |||||
| F | At ground level, into holes, excavation pits and bottom of vessels | 84 (7.7) | 6 (10.7) | 73 (7.7) | 5 (6.2) |
|
| |||||
| Not indicated | 8 (0.7) | 1 (1.8) | 6 (0.6) | 1 (1.2) | |
ISS: Injury Severity Score
The mean height of falls was greatest from scaffoldings at 3.19 m, whereas falls on the ground traversed the shortest distance at 0.70 m. Overall, Group B (formwork, roof, mezzanine and tops of container) falls had the highest mean height at 2.53 m and Group D (ladders, steps and stairs) had the lowest at 1.70 m.
Data on the use or otherwise of safety devices at the workplace was obtained from 833 (76.8%) patients. Of these, 1.8% of the patients reported using a safety helmet, 0.7% of the patients reported using it incorrectly and the remainder reported not using it at the time of the incident. In addition, 4.1% of the patients reported using a safety harness, whereas 95.9% of the patients reported using it either incorrectly or not at all at the time of the incident. The non-usage of safety helmets or harnesses ranged from 80.7% for those who fell from scaffoldings to 99.6% for those who fell from ladders.
In total, 912 (84.1%) casualties did not report any prior medical condition at the time they were being managed at the hospital. A total of 89 (8.2%) casualties had hypertension, 45 (4.1%) had diabetes mellitus, 20 (1.8%) had heart disease, and 106 (9.8%) had other medical conditions. A total of 58 (5.3%) casualties had multiple medical conditions. The mean age of those with known prior medical conditions was 47.8 years and 38.3 years for those without known medical problems (P < 0.001).
The presence of prior medical conditions [Table 2] was not associated with any significant difference in ISS, duration of medical leave given, rates of discharge, outpatient follow-up or inpatient admission. None of the 31 casualties who died had any known prior medical condition. Patients with prior medical conditions were more likely to sustain falls when in Group C locations.
Table 2.
Association of known pre-existing medical condition with injury severity, clinical outcomes, days lost from work and location of injury occurrence.
| Variable | n (%)/Mean±standard deviation | P | ||
|---|---|---|---|---|
|
| ||||
| Total (n=1,085) | Have medical condition (n=173) | No medical condition (n=912) | ||
| Age (yr) | 39.8±11.5 | 47.8±11.5 | 38.3±10.8 | <0.001 |
|
| ||||
| ISS | 5.7±9.3 | 4.3±3.7 | 6.0±10.0 | 0.138 |
|
| ||||
| Medical leave (day) | 67±80.7 | 63.8±83.9 | 67.7±80.0 | 0.685 |
|
| ||||
| Outcome (treat and discharge, no follow-up) | 210 (19.4) | 27 (15.6) | 183 (20.1) | 0.047 |
|
| ||||
| Outcome (treat and discharge with outpatient follow-up) | 495 (45.6) | 81 (46.8) | 414 (45.4) | – |
|
| ||||
| Outcome (admitted as inpatient) | 349 (32.2) | 65 (37.6) | 284 (31.1) | – |
|
| ||||
| Outcome (inpatient death) | 10 (0.9) | 0 (0) | 10 (1.1) | – |
|
| ||||
| Outcome (death at ED) | 21 (1.9) | 0 (0) | 21 (2.3) | – |
|
| ||||
| Mechanism of injury by location | ||||
|
| ||||
| Group A | 243 (22.4) | 23 (13.3) | 220 (24.1) | 0.002 |
|
| ||||
| Group B | 51 (4.7) | 10 (5.8) | 41 (4.5) | – |
|
| ||||
| Group C | 115 (10.6) | 31 (17.9) | 84 (9.2) | – |
|
| ||||
| Group D | 555 (51.2) | 93 (53.8) | 462 (50.7) | – |
|
| ||||
| Group E | 29 (2.7) | 4 (2.3) | 25 (2.7) | – |
|
| ||||
| Group F | 84 (7.7) | 11 (6.4) | 73 (8.0) | – |
|
| ||||
| NA | 8 (0.7) | 1 (0.6) | 7 (0.8) | – |
ED: emergency department, ISS: Injury Severity Score, NA: not available, SD: standard deviation
Figure 4 shows the distribution of injuries by body organ system for all casualties. Most persons sustained injuries in the upper limbs (40.7% of casualties) and lower limbs (40.9%), followed by the spine (22.6%), head (15.9%) and thorax (11.5%).
Figure 4.
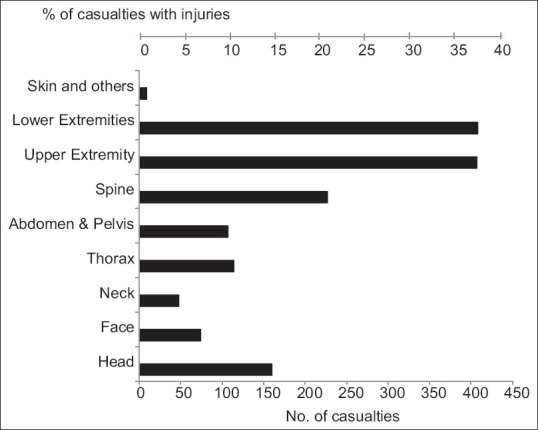
Bar graph shows distribution of injuries for fall from height by casualties and body region.
Altogether, there were 56 (5.2%) patients with major injuries (ISS >15). Of these major trauma patients [Table 3], 83.9% had head injuries, 57.1% had thoracic injuries and 37.5% had injuries in the abdomen and pelvis. Among those with minor trauma (ISS ≤15), most patients had upper (40.8%) and lower (41.8%) extremity injuries. Although 22.2% of patients with minor injuries had spinal trauma, only 7.2% of such injuries were serious (AIS ≥3). Among patients with ISS >15, 23.2% had serious spinal injury (AIS ≥3). Injuries that were serious, severe, critical and maximal (AIS ≥3) occurred mainly in patients with major trauma (ISS >15) and affected the head (82.1%), thorax (53.6%) and abdomen and pelvis (35.7%). The proportion of upper and lower extremity injuries were not significantly different in the groups with major or minor trauma.
Table 3.
Body region injuries by ISS and AIS.
| Body region | n (%) | |||||
|---|---|---|---|---|---|---|
|
| ||||||
|
|
|
|||||
| All body system injuries | Severe body system injuries (AIS ≥3) | |||||
| ISS >15 (n=56) | ISS ≤15 (n=948) | P | ISS >15 (n=56) | ISS≤15 (n=948) | P | |
| Head | 47 (83.9) | 117 (12.3) | <0.001 | 46 (82.1) | 31 (3.3) | <0.001 |
|
| ||||||
| Face | 15 (26.8) | 61 (6.4) | <0.001 | 13 (23.2) | 21 (2.2) | <0.001 |
|
| ||||||
| Neck | 8 (14.3) | 40 (4.2) | 0.001 | 7 (12.5) | 4 (0.4) | <0.001 |
|
| ||||||
| Thorax | 32 (57.1) | 87 (9.2) | <0.001 | 30 (53.6) | 41 (4.3) | <0.001 |
|
| ||||||
| Abdomen and pelvis | 21 (37.5) | 86 (9.1) | <0.001 | 20 (35.7) | 36 (3.8) | <0.001 |
|
| ||||||
| Spine | 16 (28.6) | 210 (22.2) | 0.300 | 13 (23.2) | 68 (7.2) | <0.001 |
|
| ||||||
| Upper extremity | 21 (37.5) | 387 (40.8) | 0.720 | 18 (32.1) | 276 (29.1) | 0.851 |
|
| ||||||
| Lower extremity | 13 (23.2) | 396 (41.8) | 0.015 | 11 (19.6) | 236 (24.9) | 0.492 |
|
| ||||||
| Skin + external | 0 (0) | 9 (0.9) | 1.000 | 0 (0) | 1 (0.1) | 1 |
AIS: Abbreviated Injury Scale, ISS: Injury Severity Score
Outcomes for the patients who went to the ED are shown in Table 4. For those with ISS >15, 58.9% were admitted as inpatients. Of these, nine patients died after admission, and 21 others were earlier pronounced dead at the ED. For those with ISS <15, 33.5% were admitted as inpatients. All such patients survived.
Table 4.
Effect of injury severity on clinical outcomes.
| Clinical outcome | n (%) | ||
|---|---|---|---|
|
| |||
| ISS >15 (n=56) | ISS ≤15 (n=948) | ISS missing (n=81) | |
| Treated and discharged | 2 (3.6) | 630 (66.4) | 73 (90.1) |
|
| |||
| Admitted as inpatient and alive | 24 (42.9) | 318 (33.5) | 7 (8.6) |
|
| |||
| Admitted as inpatients and died | 9 (16.1) | 0 (0) | 1 (1.2) |
|
| |||
| Died at emergency department | 21 (37.5) | 0 (0) | 0 (0) |
ISS: Injury Severity Score
The average age of the patients who died was 38.5 years. All were male. The ethnic distribution was: Chinese 54.8%, Malays 6.5%, Indians 22.6% and other nationalities 16.1%. Of the patients who died, 22.6% fell from less than 5 m, 12.9% from 5 m to 10 m and the remaining 48.4% from more than 10 m. Only one of the 31 had a documented use of a safety helmet and six had a documented use of a safety harness. Head injuries were noted in 67.7% of these fatalities, thoracic injuries in 64.5%, abdominal and pelvic injuries in 45.2%, spinal injuries in 29%, and injuries of the upper and lower extremities in 19.4% each. All of them had ISS exceeding 15. Five had a score of 16–30, three between 31 and 45, three between 46 and 60 and the remainder between 61 and 75.
DISCUSSION
This study of 1,085 patients who fell from a height in the construction industry has, by careful documentation of the patterns of injury, highlighted the need for greater use of safety devices in the prevention of falls. Safety devices were not used by 94.1% of the persons injured at construction sites. The use of safety harnesses needs to be effectively implemented for protection against falls. Safety enforcement is an area that needs to be given greater emphasis if we wish to decrease instances of falls in these locations. In addition, it is clear that ladders, stairs and steps together constitute the greatest hazard in workplaces, amounting to approximately half of the falls. These activity areas involve the worker climbing up or down, thus offering opportunities to slip or to otherwise miss a foothold and fall.
The study also highlighted that the commonest injuries occurring in the severely injured were those in the upper half of the body (i.e. the head, thorax, abdomen and pelvis). Even falls from a height of 2 m or less can be injurious. Mortality and morbidity were greatest in those with severe injuries. There is a need to consider compulsory and strict implementation of the use of protective devices, especially of the head, chest and abdomen, to mitigate the possible effects of falls, especially for those who work at heights such as on scaffolding, formwork, platforms and cranes. Because ladder falls are the most frequent, emphasis on ladder safety such as checking the ladder structure for any damage, positioning the ladder properly and implementing regular on-site educational programmes on ladder safety may need to be considered. Helmets and safety harnesses are less likely to be needed for ladders, steps and stairs. Continuous supervision and compulsory use of devices such as safety helmets and effective safety harnesses at work sites, with regular and frequent site-safety inspections and penalties for employers who are unable to ensure strict enforcement, need to be implemented and strictly enforced to minimise these incidents.
Falls at construction sites are unlike free falls from heights. The scaffolding at construction sites usually breaks the falls and can modify the mechanism of landing. This can result in a variety of injuries depending on the parts of the body that bear the brunt of the multiple impacts that may occur. An autopsy study of 52 cases of falls from height from 2005 to 2007 conducted in Bangalore, India, revealed that 69.2% had head injuries and 61.5% had thoracic injuries, very similar to our findings.[7] This reflects the predilection for these body parts to be severely impacted during falls from heights.
The lesser severity of injuries among those with previously known medical conditions such as hypertension, diabetes mellitus and ischaemic heart disease may be associated with such persons not being involved in work involving additional risks or great heights. We cannot be certain whether this may also reflect a greater tendency for these persons, who would generally be older and more experienced, to take greater care when handling their tasks in the construction industry. Previous literature appears to suggest that older individuals and those with pre-existing illnesses may have a greater tendency to fall.[16,17]
It was generally noted that most casualties arriving from construction work sites were usually not provided any on-site first aid soon after the incident and would generally await the arrival of the prehospital ambulances; in cases of severe falls, the first care is received when they either visit a doctor's clinic or the ED of a hospital. The lack of provision of such first aid by coworkers and work supervisors results in delay of administration of emergency care and may need to be rectified as a priority.
The current Singapore WSH Act (Chapter 354A, Section 65) WSH First Aid Regulations[18] specify that if there are more than 25 persons employed in a workplace, there shall be one first-aider for every 100 persons employed. In a construction industry environment, where the workers are usually fairly dispersed rather than all working in very close proximity to each other, such a first-aider may not be activated often or early enough to render appropriate assistance. Immediate availability of first aid may be a positive intervention measure, rather than waiting for an ambulance or paramedic to arrive from afar.
Buddy first aid in the form of the first available person providing such care should be an option. This, however, would require a significant change in the help culture at the workplace, including ensuring that every worker, rather than just a small number, is trained in basic first aid, has the implements to provide buddy first aid at close quarters and has confidence in providing such care. Investment in training and safety education must be seen as essential to industrial safety. A number of studies have shown decreased mortality when bystander first aid was provided on site.[19,20,21,22] Such provision of first aid at construction sites can only be achieved through practising a culture of safety that includes universal training in these basic core life-saving skills for construction workers.
This study had a number of limitations. First, it was a retrospective study. The authors had to depend on the comprehensiveness of the clinical notes of the doctors who first attended to the patients and manage the limitations these would have on accurate definition of injury scores. Second, information on the actual safety practices used by the workers at the time of the accidents was sometimes not available to the research team. Prospective collection of such data each time an injury occurs would enhance accurate data collection for future studies. Third, this study was confined to patients seen in only one hospital in the country. This would limit the types of injuries to those seen in the construction industry in the catchment area of the hospital. Access to the prehospital, accident investigation and detailed medical records of all such industrial accidents in the country could, potentially, tremendously enhance the value of future studies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors acknowledge the assistance provided by Dr Gan Siok Lin and Mr Tan Boon Kiat, WSH Institute, MOM, with the list of patients who were seen at the Singapore General Hospital after sustaining falls at their work sites, and Ms Anjali Baglody for creating the study case record forms and electronic database file for the documentation and capture of the study data.
REFERENCES
- 1.Work Safety and Health Statistics Report 2007. Singapore: Ministry of Manpower Archives; 2008. Ministry of Manpower, Singapore. [Google Scholar]
- 2.Ministry of Manpower, Singapore. A guide to the workplace safety and health (risk management) regulations. 2006. [Last accessed on 15 May 2020]. Available from: https://www.mom.gov.sg/-/media/mom/documents/safety-health/guidetoriskmgtregver 20.pdf.
- 3.Ministry of Manpower, Singapore. Occupational Safety and Health Profile. 2006 Report. [Last accessed on 12 Nov 2019]. Available from: https://www.mom.gov.sg/-/media/mom/documents/safety-health/reports-stats/wsh-profile/osh-profile-2006.pdf.
- 4.Workplace Safety and Health Council, Singapore. Workplace Safety and Health Report. 2010. [Last accessed on 12 Nov 2019]. Available from: https://www.mom.gov.sg/-/media/mom/documents/press-releases/2011/annex-a---wsh-statistics-report-2010-(160311).pdf.
- 5.Teoh K. WSH approach on the construction sector in Singapore. International Labour Organization. [Last accessed on 12 Mar 2018]. Available from: https://www.ilo.org/safework/info/WCMS_169573/lang--en/index.htm.
- 6.Ministry of Manpower, Singapore. Code of practice for working safely at heights. [Last accessed on 10 May 2016]. Available from: https://www.tal.sg/wshc/Resources/Publications/Codes-of-Practice/Code-of-Practice-for-Working-Safely-at-Heights---English.
- 7.Murthy CRV. Study of pattern of injuries in fatal cases of fall from height (dissertation) Bangalore: Rajiv Gandhi University of Health Sciences; 2008. [Google Scholar]
- 8.Chok S. Risky business: Death & injury on Singapore's construction sites. HealthServe. [Last accessed on 03 Dec 2020]. Available from: https://www.researchgate.net/publication/312913824_Risky_Business_Death_Injury_on_Singapore's_Construction_Sites_Examining_Worksite_UnSafety_Through_Conversations_with_Migrant_Construction_Workers.
- 9.Ling FYY, Liu M, Woo YC. Construction fatalities in Singapore. Int J Proj Manag. 2009;27:717–26. [Google Scholar]
- 10.Report on fatal and non-fatal injuries in the Ontario construction industry. January. Infrastructure Health & Safety Association. 2006. [Last accessed on 17 Jun 2016]. Available from: https://www.ihsa.ca/pdfs/research_docs/Fatals-LTIs.pdf.
- 11.Haslam RA, Hide SA, Gibb AGF, Gyi DE, Pavitt T, Atkinson S, et al. Contributing factors in construction accidents. Appl Ergon. 2005;36:401–15. doi: 10.1016/j.apergo.2004.12.002. [DOI] [PubMed] [Google Scholar]
- 12.Atanasijevic TC, Savic SN, Nikolic SD, Djoki VM. Frequency and severity of injuries in correlation with the height of fall. J Forensic Sci. 2005;50:608–12. [PubMed] [Google Scholar]
- 13.Turk EE. Fatal falls from height. In: Tsokos M, editor. Forensic Pathology Reviews 5, Part II. New Jersey: Humana Press; 2008. pp. 25–38. [Google Scholar]
- 14.Atanasijevic TC, Popovic VM, Nikolic SD. Characteristics of chest injury in falls from heights. Leg Med (Tokyo) 2009;11(Suppl 1):S315–7. doi: 10.1016/j.legalmed.2009.02.017. [DOI] [PubMed] [Google Scholar]
- 15.Association for the Advancement of Automotive Medicine. Abbreviated Injury Scale (AIS©) [Last accessed on 03 May 2012]. Available from: https://www.aaam.org/abbreviated-injury-scale-ais/
- 16.Gauchard G, Chau N, Mur JM, Perrin P. Falls and working individuals: Role of extrinsic and intrinsic factors. Ergonomics. 2001;44:1330–9. doi: 10.1080/00140130110084791. [DOI] [PubMed] [Google Scholar]
- 17.Nadhim EA, Hon C, Xia B, Stewart I, Fang D. Falls from height in the construction industry: A critical review of the scientific literature. Int J Environ Res Public Health. 2016;13:638. doi: 10.3390/ijerph13070638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Singapore Statutes Online. Workplace Safety and Health Act (Chapter 354A, Section 65) [Last accessed on 05 Jul 2018]. Available from: https://sso.agc.gov.sg/SL/WSHA2006-RG4.
- 19.Mock CN, Tiska M, Adu-Ampofo M, Boakye G. Improvements in prehospital trauma care in an African country with no formal emergency medical services. J Trauma. 2002;53:90–7. doi: 10.1097/00005373-200207000-00018. [DOI] [PubMed] [Google Scholar]
- 20.Larsson EM, Mártensson NL, Alexanderson KA. First-aid training and bystander actions at traffic crashes--A population study. Prehosp Disaster Med. 2002;17:134–41. doi: 10.1017/s1049023x00000352. [DOI] [PubMed] [Google Scholar]
- 21.Mauritz W, Pelinka LE, Kaff A, Segall B, Fridrich P. [First aid measures by bystanders at the place of accident. A prospective, epidemiologic study in the Vienna area] Wien Klin Wochenschr. 2003;115:698–704. doi: 10.1007/BF03040885. German. [DOI] [PubMed] [Google Scholar]
- 22.Tannvik TD, Bakke HK, Wisborg T. A systematic literature review on first aid provided by laypeople to trauma victims. Acta Anaesthesiol Scand. 2012;56:1222–7. doi: 10.1111/j.1399-6576.2012.02739.x. [DOI] [PMC free article] [PubMed] [Google Scholar]