
Figure 3. Model of neutrophil-mediated T cell injury and immunoparalysis in the TME.
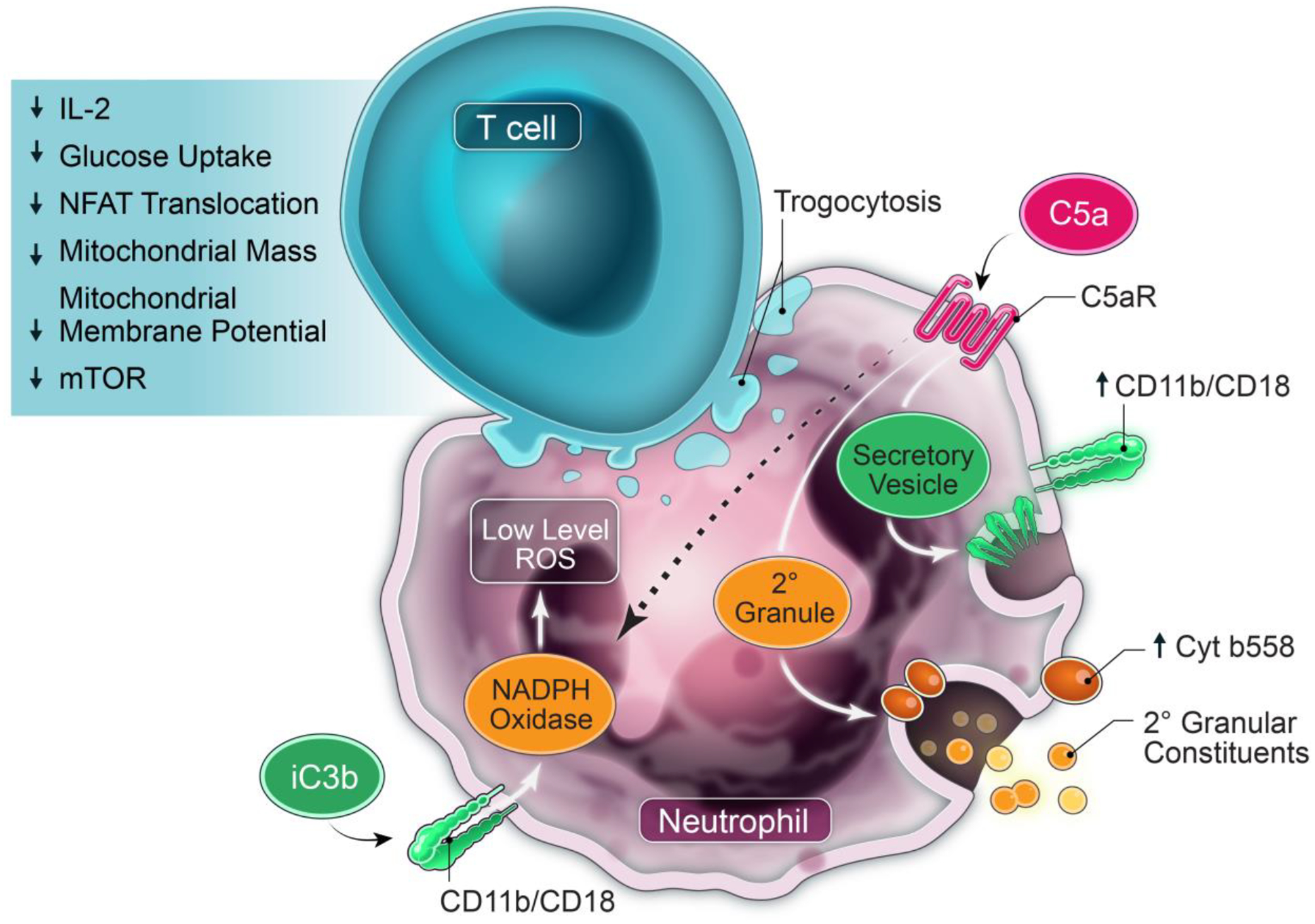
Circulating neutrophils are recruited to the TME where they acquire suppressor function directed at T cells. Malignant effusions have multiple products, including DAMPs, cytokines, chemokines, and activated complement that chemoattract and activate neutrophils and induce suppressor function. Multiple neutrophil effector functions including complement signaling, CD11b/CD18 (CR3; receptor for iC3b), NADPH oxidase, SNARE-mediated intracellular transport and exocytosis of granular and/or vesicular constituents, and phosphatidylserine drive this suppressor phenotype. A positive feedback loop through C5aR activation increases surface expression of CD11b/CD18 and cytochrome b558 (membrane-bound gp91phox/p22phox component of NADPH oxidase), predicted to amplify complement signaling and surface NADPH oxidase. Activated neutrophils also cause CD11b-dependent trogocytosis of T cell membranes, expected to cause membrane injury. These neutrophil-generated signaling and injury cues to T cells cumulatively result in non-responsiveness, characterized by suppression of stimulated cytokine responses, NFAT translocation, glucose uptake, mitochondrial mass and depolarization, and mTOR activation. Model is from Emmons et al.67.