
Fig. 2.
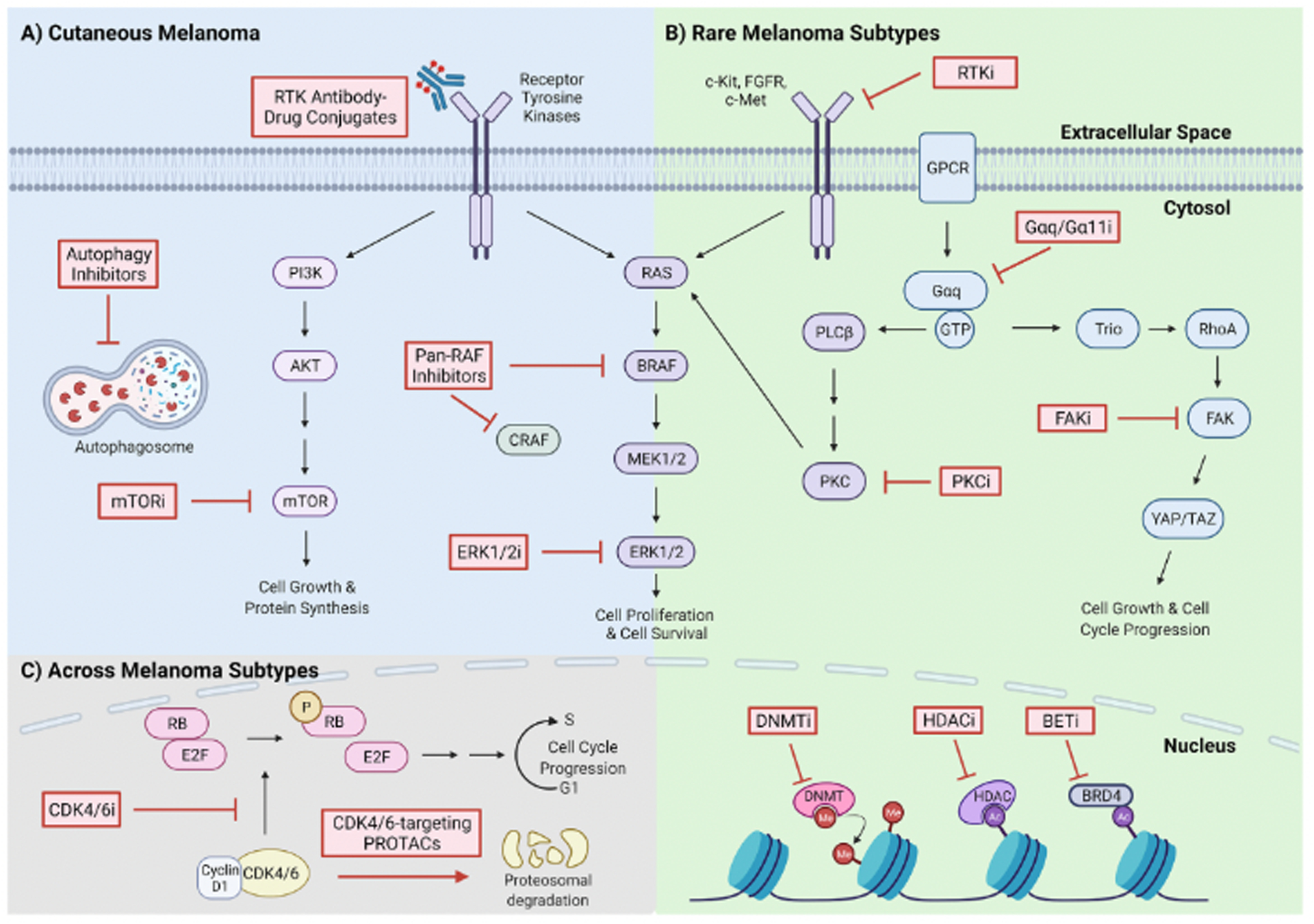
Selected actionable drug targets, for monotherapy or in combination with BRAFi and/or MEKi, in CM and rare melanoma subtypes. A) Combination therapies for CM. RTKs, which activate both the MAPK and PI3K/AKT/mTOR survival pathways, can be inhibited by RTK-targeting antibody-drug conjugates. mTORi act downstream of RTKs on the PI3K/AKT/mTOR pathway. Pan-RAF inhibitors, which prevent RAF monomer and/or dimer activity, ERK1/2i, which prevent ERK1/2 phosphorylation, and autophagy inhibitors, which prevent autophagosome maturation, are also being tested in combination with BRAFi and/or MEKi. B) Combination therapies for rare melanoma subtypes. RTKs activate MAPK signaling in rare melanomas and can be targeted by small-molecule RTK inhibitors (RTKi), such as cMET or FGFR inhibitors in UM and c-Kit inhibitors in AM and MM. Active G-protein signaling contributes to MAPK pathway signaling and cell survival in UM via PLCß/PKC. Targeted inhibitors of Gαq/11 and PKC can be combined with MEKi for UM. In parallel, Trio/RhoA/FAK/YAP pathway activation leads to increased cell growth and cell cycle progression and can be targeted with FAKi. Epigenetic modifications, which are common in UM, can be targeted with DNA methyltransferase inhibitors (DNMTi), HDACi, and BETi. C) Combination therapies across melanoma subtypes. Cell cycle dysregulation in melanoma is driven by cyclin D1-CDK4/6 complex phosphorylation (P) of retinoblastoma protein (RB), and the subsequent release of the E2F transcription factor, which drives G1 to S phase cell cycle progression. CDK4/6i and CDK4/6-targeting PROTACs block cell cycle progression by preventing the kinase activity of CDK4/6 or by destining CDK4/6 for proteolytic degradation, respectively, and can be used in combination with MEKi.