
Figure 1.
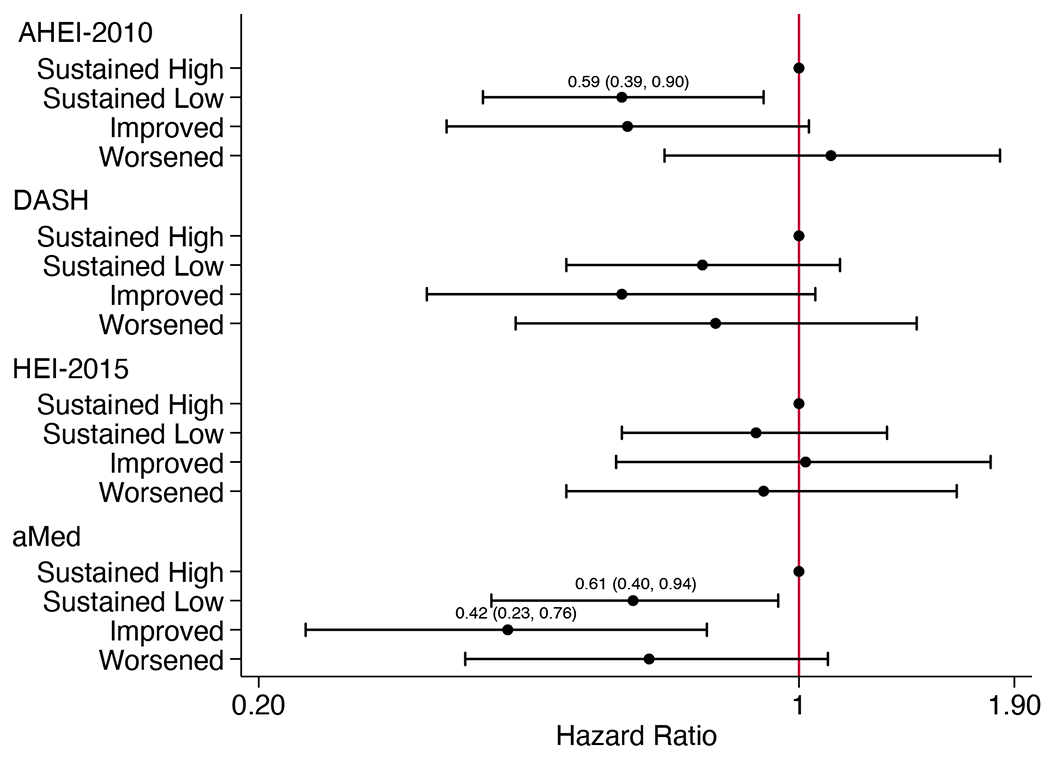
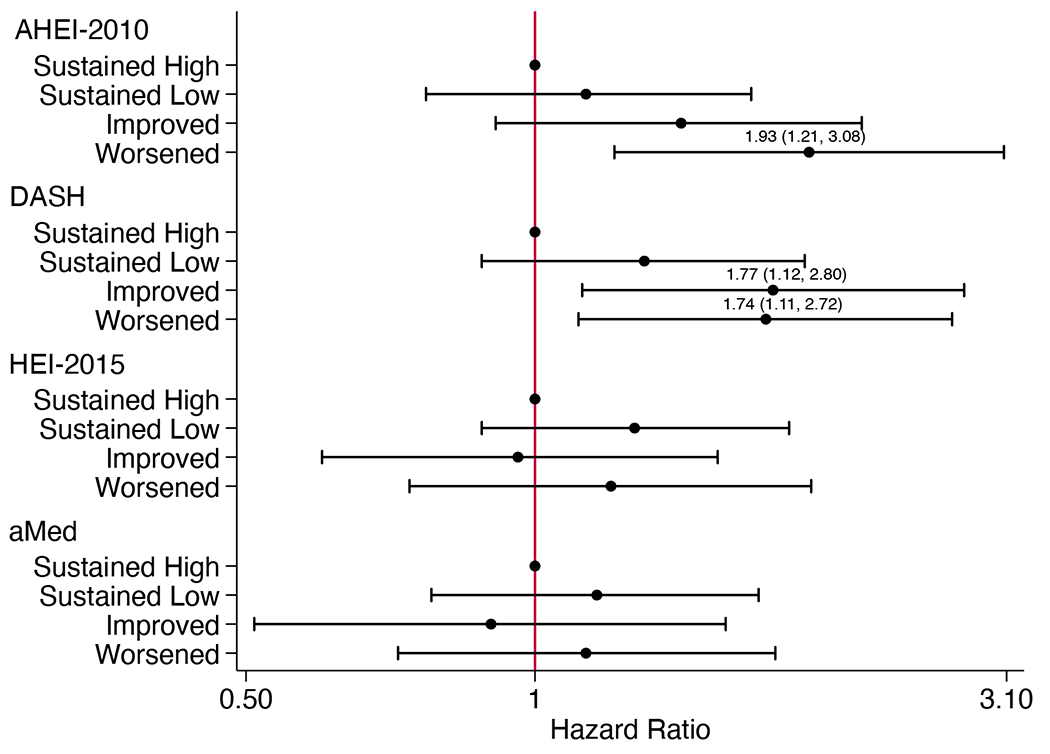
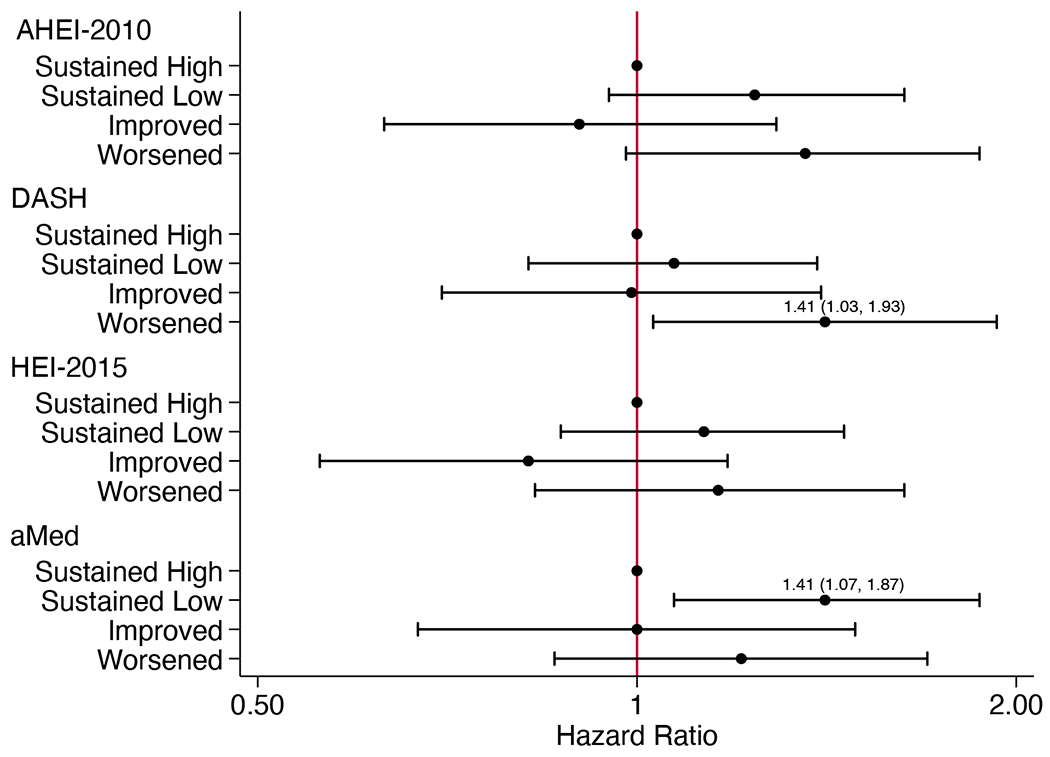
Adjusted hazard ratios (95% CI) for (A) chronic kidney disease progression in participants without diabetes (n=790), (B) chronic kidney disease progression in participants with diabetes (n=606), and (C) all-cause mortality (n=1461), according to categorized 4-year changes in diet quality scoresa
aHazard ratios (95% CI) estimated using Cox proportional hazards models adjusted for CRIC study site, age, sex, race, education, income, eGFR, total energy intake, physical activity, BMI, change in smoking status, change in physical activity, change in BMI, change in energy intake, cardiovascular disease, hypertensive status, use of lipid-lowering medications, use of ARB or ACE inhibitor medications, and use of antiplatelet medications. For DASH and HEI-2015 scores, alcohol use and change in alcohol intake were also included. Models for all-cause mortality additionally adjust for diabetes status. ACE, angiotensin-converting enzyme; AHEI, Alternative Healthy Eating Index; aMed, alternate Mediterranean diet score; ARB, angiotensin II receptor blocker; BMI, body mass index; CI, confidence interval; DASH, Dietary Approaches to Stop Hypertension; eGFR, estimated glomerular filtration rate; HEI, Healthy Eating Index