

Abstract
Background
Appropriate health services and health promotion strategies for young people with mental health and substance use (MHSU) concerns are critical for recovery. Foundry, an integrated youth services (IYS) initiative for young people ages 12-24 in British Columbia (BC), Canada, has recently added leisure and recreational activities (referred to as the Wellness Program) into its services. The objectives of this study were to: (1) describe how the Wellness Program was implemented over a two-year period into IYS (2) provide an overview of what the Wellness Program is, who accessed the program since inception and initial evaluation results.
Methods
This study was part of the developmental evaluation of Foundry. A phased approach was used to implement the program at nine centres. Data was accessed from Foundry’s centralized platform ‘Toolbox’ and included activity type, number of unique youth and visits, additional services sought, information about how youth found out about the centre, and demographics. Qualitative data was also accessed from focus groups (n=2) conducted with young people (n=9).
Results
Over the two-year period, 355 unique youth accessed the Wellness Program, with 1319 unique visits. Almost half (40%) of youth identified the Wellness Program as the first point of access to Foundry. A total of 384 different programs were offered targeting five wellness domains (physical, mental/emotional, social, spiritual, and cognitive/intellectual). The majority of youth identified as young girls/women (58.2%), 22.6% as gender diverse, and 19.2% as young men/boys. The mean age was 19 years, and most participants were between the ages of 19-24 years (43.6%). From the thematic analysis of focus groups, we found young people enjoyed the social aspect of the program with peers and facilitators, and identified program improvements that are being considered as the program grows.
Conclusions
This study provides insight into the development and implementation of leisure-based activities (known as the Wellness Program) into IYS and can be used as a guide by international IYS initiatives. The initial reach of programs over two years is promising, and these programs are acting as a potential gateway for young people to access other health services.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12888-023-04809-6.
Keywords: Wellness, Youth, Mental health, Substance use, Integrated youth services, Health promotion, Leisure activities
Background
Mental health and substance use (MHSU) challenges present early in life, as 50-70% develop during childhood or adolescence [1], and the peak age of onset is 14.5 years [2]. In Canada, MHSU disorders affect 1 in 4 youth, with 12-24-year-old individuals experiencing the highest incidence of MHSU disorders of any age group [3, 4]. Population mental health concerns exist across all ages and have been exasperated by the COVID-19 pandemic, with some suggesting a global mental health crisis [5, 6]. Young people are a particularly at-risk population during this time with increasing mental health concerns [7, 8]. It has been suggested that young people have been disproportionately affected by the pandemic with employment loss, social isolation, and loss of infrastructures and supports such as school closures [9, 10]. Stemming from this, an international call has been made to invest in services to support the long-term mental health needs of young people, including health promotion/prevention, early intervention, and crisis care [6, 10]. As we navigate pandemic phases and recovery, it is vital now more than ever to intervene with the full range of MHSU services and interventions including health promotion strategies for young people.
Leisure-based activities (defined as voluntary and non-workplace or educational aspects of social life) have been highly debated throughout the COVID-19 pandemic [11]. Norman and colleagues [11] analyzed how leisure activities were understood and represented in media coverage during the pandemic in Canada. The authors acknowledge the contention about restrictions and closures perpetuating anger and frustrations, but also about leisure activities being a source of hope when re-opening and their potential for the health and economic recovery for Canadians. Leisure activities have the potential to play an important role for health promotion and prevention of worsening mental and physical health for young people. They can reduce stress, provide protective health benefits, play a role in recovery from mental illness [12], improve self worth and self-esteem [13], and promote quality of life [14]. Jae-Kim and Cho [15] identified the potential role leisure activities can play during the current pandemic and future pandemics in South Korea. A Finnish study identified that high social leisure time in adolescence was associated with a lower incidence of psychiatric disorders, particularly affective, anxiety, and substance use disorders [16]. Participation in leisure-based activities with peers has been shown to reduce feelings of social isolation and to promote psychological stability during the pandemic [15]. However, activities with peers need infection control and modification. For instance, physical activity (bodily movement that results in energy expenditure) can be modified to either do safely with peers (e.g., outdoors, virtually from home) or individually. Physical activity has been recommended as an important strategy to reduce the increased MHSU challenges brought on by the pandemic and lockdowns [17, 18], and acknowledged as a valuable health promotion tool for young people [19–21].
Integrated Youth Services (IYS) are community-based (preferably in a single location), youth- and family-centred, and provide multidisciplinary care in a youth-friendly environment [6, 22, 23]. The needs of young people and their families/caregivers are prioritized in the design of services and care [24]. IYS initiatives include headspace™ in Australia [25], Jigsaw™ in Ireland [26], Les Maisons des Adolescents in France [27], and Youth One Stop Shops (YOSS) in New Zealand [28]. Canadian IYS initiatives include Foundry [24, 29] and Youth Wellness Hubs Ontario (YWHO) [29]. IYS are a model of care that can also provide leisure-based activities as part of their services. Participation in leisure is identified as a goal for many youths accessing IYS [24], however little is known about the implementation of leisure-based activities for health promotion within this model. Leisure-based activities encompass and will be referred to as the Wellness Program for the purpose of this study. As part of developmental evaluation, the objectives of this study were to (1) describe how the Wellness Program was implemented and evaluated over a two-year period into IYS in British Columbia (BC), Canada, and (2) provide an overview of what the Wellness Program is,who accessed the program since inception, and initial program evaluation results.
Methods
Context
Foundry is an IYS that provides care for young people ages 12-24 years in BC, Canada [24] and as of May 2023, fifteen Foundry centres are open, with seven more in development. The centres exist in communities representative of small, medium, and large population centres in Canada [30]. Virtual services also support youth from across the province [8]. Foundry has five core service streams, including mental health, substance use, peer support, physical (including sexual) health, and social services. Based on an internal 2019 survey of 10,000 youth, Foundry identified a need to build leisure and physical activity into services not only as an adjunct to MHSU supports but in recognition that holistic care is central to individual wellness. With the support of private donors, Foundry implemented the Wellness Program at nine centres. Communities were asked to co-design programming that met the needs of youth accessing their centres.
Study design
Ethics approval was received from the University of British Columbia (ID: H21-01510). This study was done as a component of Foundry’s developmental evaluation which has supported the implementation of Foundry’s complex, diverse, and innovative interventions and allowed the capacity for real time decision-making to change and adapt the evolving system [31, 32]. The program was designed and implemented over six phases (defined below) and evaluated using mixed methods primarily in Phase 5 and Phase 6. To support implementation, a multidisciplinary team of researchers, a research and evaluation associate, youth peer evaluators, and various leadership team members was created at Foundry Central Office (FCO), Foundry’s central administrative and implementation team.
Program design and implementation
The following describes the phased approach used to design and implement the Wellness Program, and is a summary from a written log kept by the project coordinator during the timeline provided.
Phase 1: Community asset development September-October 2019
Communities were given the opportunity to assess the needs of youth in their region. The project coordinator informed centre staff at eight Foundry centres of the initiative to implement the Wellness Program. Staff then shared this by word of mouth with youth, family and peer support workers and those interested in providing input were given the project coordinator’s contact information. An environmental scan was conducted in collaboration with centre staff to identify assets, gaps and community need in services through team meetings, individual meetings, centre tours, discussions, and the administration of a survey (survey questions provided as supplementary material). The interested community members were asked to describe how meaningful activities – such as spending time outdoors, exploring creative expression, or participating in physical activities – could impact the wellness of diverse, Foundry-accessing youth. Examples of questions posed include, “What does Wellness mean to you? What does Wellness mean to the youth you serve? What community resources/services would you use? What are the main barriers for youth in accessing these resources/services?” The only restriction from the first funder was that programs needed to be offered in-person to reduce screen time. Proposals, budgets and requests for funding was reviewed with centre managers and teams and discussions were had about opportunities for community partnerships and resource sharing.
Phase 2: Gathering momentum September-December 2019
The project coordinator worked closely with eight centres and communities to support project management, access and flow funds, program co-development and ongoing engagement. The project coordinator liaised with a provincial dietician, and supported centre staff to identify assets and strengths in their communities. They also liaised with implementation coordinators at centres for collaborative work, and began exploring opportunities for youth empowerment with employment roles such as peer support workers or cultural coordinators, and explored Indigenous program opportunities. The project coordinator collaborated with FCO to: identify evaluation tools/protocols (e.g., integrating and tracking through Toolbox) and research opportunities, and implement group programming within IYS. Formal community partnerships were established with local and provincial agencies. Centres worked with their community members to develop and draft an outline for their Wellness Program and co-design a custom curriculum to meet their unique needs. The project coordinator sent initial draft curriculum content to centres. Centres then sought input from Youth Advisory Committees, peer support workers, and Indigenous youth and families. Content was also reviewed by FCO staff. Changes were then made to the content, specifically inclusion of the voice of youth in conceptualizing wellness, tools and templates for group development and facilitation, and risk management.
Phase 3: Pilot programs and partnerships January 2020-April 2020
Pilot Programs began at each centre (e.g., Healthy by Nature outdoor program). The project coordinator identified centre champions, developed waivers, liability and consent forms, as well as service agreements and contracts with community partner organizations. They also provided ongoing centre support and practical toolkits and resources while continuing to develop the wellness curriculum. In parallel, an evaluation team co-designed the evaluation framework and research questions to understand the impact of this pilot phase. Youth Peer Evaluators working with FCO’s Research and Evaluation teams were consulted when establishing a framework.
Phase 4: Pandemic pivot April 2020-December 2020
The COVID-19 global pandemic was declared in March 2020 [33]. Public health measures required communities to adapt programs to conform with provincial restrictions and regulations for in-person gatherings. To meet the coordination needs of communities, an FCO working group was formed to support implementation of the Wellness Program within the new pandemic restrictions. As it became apparent that the public health measures would last for an extensive period of time, several workshops were offered from FCO to support program facilitation. For instance, a group facilitation training session was offered for peer support workers across the centres. A need was identified to change the original curriculum into a user-friendly engaging practical resource (which became the Wellness Program Guide further described in Phase 6). The project coordinator explored definitions of wellness from the youth perspective at centres and from staff at Foundry Central Office.
Phase 5: Knowledge exchange and adaption January 2021-April 2021
The project coordinator continued to collaborate with community partners, provided a report and updates to funders, and held a Foundry network-wide knowledge exchange workshop to share information about the Wellness Program offered at different centres. They also supported centres with creative problem-solving during pandemic restrictions to offer hybrid program ideas or smaller in-person scenarios and began exploring opportunities for youth peer engagement within the Wellness Program and development of the program with an Indigenous perspective. A team comprised of a researcher, a research and evaluation associate, and four youth peer evaluators began program evaluation (including conducting of focus groups with young people).
Phase 6: Wellness program guide and evaluation April 2021-December 2021
The project coordinator consulted and worked with the Foundry Indigenous Wellness Team, centre champions and FCO team members to develop and publish the Wellness Program Guide which outlines program vision, intent, examples and working templates to run programs [34]. The Table of Contents of the Wellness Program Guide is included in Table 1 for reference. The aim established is the Wellness Program should complement other health services offered and target five domains of wellness: physical, social, emotional/mental, cognitive/intellectual, spiritual/cultural (See Table 2 for definitions) [35]. The vision statement is “Move your body, Calm your mind” [34]. Program objectives include the emphasis on social inclusion and connection with self, others, nature, engagement with community partners, and the enhancement of the service model by infusing wellness opportunities. Ongoing support was provided for centres to provide programming with constantly changing provincial restrictions.
Table 1.
Table of contents of the wellness guide [34]
| Section | Section content | Pages |
|---|---|---|
| Acknowledgements | 1 | |
| Introduction | Background and Context of Wellness Program | 2-4 |
| Purpose of This Guide | ||
| What is Wellness? | Youth Perspective | 6-12 |
| Accessible Wellness | ||
| Domains of Wellness | ||
| Indigenous Wellness | ||
| Tools and Resources | ||
| Developing a Wellness Program at Your Centre | Assess Participant Needs and Community Assets | 13-41 |
| Develop a Proposal | ||
| Plan and Design Program | ||
| Engage in Pre-Program Tasks | ||
| Implement Program | ||
| Evaluate Program | ||
| Types of Wellness Activities | Community-Based Activities | 45-49 |
| Nature-Based and Land-Based Activities | ||
| Small Group Activities | ||
| Large Group Activities | ||
| Individual Activities | ||
| Virtual Activities | ||
| Tools and Resources | ||
| Activities Within the Domains of Wellness | Physical Wellness | 50-62 |
| Emotional/Mental Wellness | ||
| Social Wellness | ||
| Cognitive/Intellectual Wellness | ||
| Spiritual/Cultural Wellness | ||
| Community Partnerships | BC Parks Foundation | 65-67 |
| Power To Be | ||
| Women’s National Field Hockey Team | ||
| YMCA | ||
| Creating New Partnerships | ||
| Research | Wellness Research Projects | 68-69 |
| Digital Storytelling as a Research Technique | ||
| Partnerships | ||
| Tools and Resources | ||
| Sustaining Wellness | 70 | |
| Tools and Resources | 71-72 | |
| Contact List | 73 | |
| Contributors | 74 | |
| References | 75 |
Table 2.
Wellness domains and definitions adapted from Payne, Ainsworth, and Godbey [35]
| Wellness domain | Definition | Activity aim |
|---|---|---|
| Physical | Move more, eat well, sleep better | Physical activity, nutrition, sleep, connections to nature, outdoor recreation |
| Social | Build connections, share experiences, find role models | Making friends and feeling included, sharing lived experiences, connecting with mentors and Elders, low-pressure activities, healthy relationship skills |
| Emotional/Mental | Express yourself, live in the moment, cope with stress | Stress management, self-care, relaxation and mindfulness, self-awareness and self-acceptance, hope and optimism |
| Cognitive/Intellectual | Boost your brain, try new things, empower yourself to lead | Creative and brain-boosting activities, leadership and volunteering opportunities, goal setting, exploring interests, learning new skills |
| Spiritual/Cultural | Feed your soul, find purpose, connect with your culture | Discovering purpose in life, spiritual practices, cultural activities, cultural teachings, creating harmony and connection with the earth |
Data collection and analyses
Ethics approval was received from the University of British Columbia Behavioural Research Ethics Board (ID: H21-01510). Data for this study were collected from two sources, the first being Foundry’s centralized data platform called ‘Toolbox’ for all young people who accessed the Wellness Program over a two-year period (September 2019- September 2021). These data are routinely collected in accordance with the BC Freedom of Information and Protection of Privacy Act (FIPPA) and the BC Personal Information Protection Act (PIPA) for the purposes of service delivery, evaluation and research. Informed consent was received from youth prior to survey completion, and youth do not have to complete the survey in order to receive services (i.e., completion of the surveys is voluntary). Youth voluntarily consent to the data being used for research purposes by indicating they have read and understood the purpose of the survey and how data are collected, stored and reported. Data are de-identified, stored, accessed, and analyzed in a secure research environment. Data are not linked in any way back to personal identifiers. Specific to the Wellness Program, data was collected on activity type, number of unique youth and visits. The forms also collected information about the type of services sought in addition to the Wellness Program (physical health, sexual health, mental health, substance use, youth peer support or social service); information about how the youth found out about Foundry; and demographic data including identity, age, sexual orientation, ethnic/cultural background. Descriptive analyses were conducted calculating proportions (n/N, %) for all variables.
In addition to ‘Toolbox’ data, qualitative data collected as part of Foundry’s developmental evaluation was also accessed. Young people (aged 16-24 years) who participated in the Wellness Program at any Foundry centre across BC, Canada since program inception (September 2019) were eligible to participate. Young people were invited to participate and recruited through Foundry’s social media and through staff offering the program at centres and offered a $30 gift card for participation. Verbal consent was gained by young people at the time of the focus group. These data are routinely collected in accordance with the BC FIPPA and the BCPIPA for the purposes of service delivery, evaluation and research (as further described above). Semi-structured virtual focus groups (n=2) were conducted with young people (n=9 participants) via the platform Zoom© from April-September 2021. It was optional for participants to have their video camera on, and participants could use the chatroom feature and type versus answer verbally. Focus groups were conducted to meet evaluation objectives outlined in (Table 3), and explore the experiences of young people. The focus group guide is provided as Supplementary Material.
Table 3.
Program evaluation objectives
| Objective 1. | To understand the extent to which the program was implemented as intended |
| Objective 2. | To understand the extent to which the wellness activities have enhanced Foundry’s services |
| Objective 3. | To understand young people’s satisfaction and involvement with the program and to understand the extent to which participants report the program impacted their health and wellness |
| Objective 4. | To understand the extent to which awareness and understanding of how technology is impacting youth is increased |
| Objective 5. | To understand the extent to which the activities have resulted in opportunities for collaboration and partnership |
All focus groups were audio-recorded and transcribed verbatim. All exact text from the chat feature of zoom was integrated into the transcripts at the appropriate times. To maintain confidentiality, participant numbers were assigned to each participant, and any identifying information was removed from transcripts. QSR International’s NVivo © 12 Software was used to facilitate qualitative data analysis. A blend of deductive and inductive analytical approach was used in a multi-step process to conduct a thematic analysis [36]. This included becoming familiar with data- audio recordings were listened to, then re-listened to while reading and re-reading transcripts and notes were taken. Next, open broad codes were generated in NVivo© software based on the evaluation objectives and interview guide topics. Researcher (author KG) coded half of one focus group transcript with two youth peer evaluators to discuss coding, answer any questions and ensure understanding of the research process. The broader codes were then reviewed to search for and identify data-driven ideas and patterns (and ultimately developed into themes) and this step was considered inductive. Themes were then reviewed across and within the entire data set, defined and named. Writing of themes was an iterative and an integrated process throughout to aim for a comprehensive analysis. KG met with the youth peer evaluators, reviewed all coding and the identified themes to stimulate discussion and encourage reflexive acknowledgment of results and perspectives in the research process [37]. To aim for quality thematic analysis, the 15-point “checklist” for good thematic analysis was consulted (pg 96) [38].
Results
Results are based on ‘Toolbox’ data collected at Foundry centres over the two-year period after program launch (September 2019-September 2021). The results suggest a wide range of leisure activities offered within the Wellness Program across this IYS network. A total of 384 different leisure activities were offered within five wellness domains (Fig. 1). Table 2 provides an overview of each wellness domain, its definition, and examples of domain-promoting activities. Work by author BM (Fig. 2) provides a summary of the number of activities offered in each of the five wellness domains. The most commonly represented domain was cognitive/intellectual (n = 129; 36%), followed by emotional/mental (n = 59; 17%), social (n = 54; 15%), physical (n = 45; 13%) and spiritual (n = 2; 0.1%). There were 64 (18%) activities with acronyms and names that could not be classified and thus labelled as “other”. Examples include ‘KOB CMP’; ‘KVR RADAR’; ‘BLIP’; and ‘Drop-in’ (See Table 4 for a list of all activities). The Wellness Program offered a combination of individual, small or large group; community-based; in person and virtual activities. Examples of activities included Bob Ross Paint Nights, Book Clubs, Dungeons and Dragons, Hiking, Yoga, and Community Cooking. See Table 4 for a list of all names of activities in the Wellness Program offered and the corresponding wellness domain the activity targeted.
Fig. 1.
Wellness domains
Fig. 2.
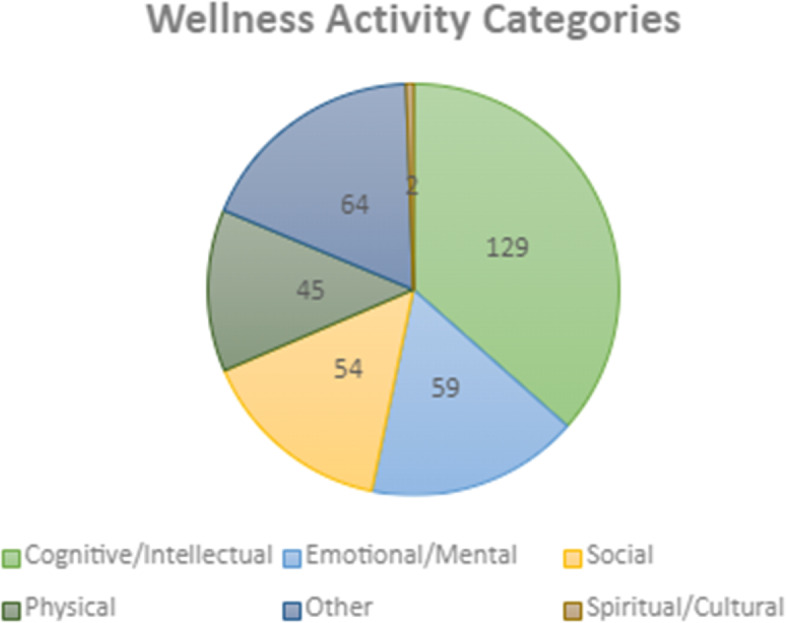
Wellness activities offered within each wellness domain
Table 4.
Wellness program activities within wellness domains
| Wellness domain | Activities offered |
|---|---|
| Cognitive/Intellectual | Activate: Tie Dye (Virtual) |
| Activate: Tie Dying (In Person) | |
| Aromatherapeutic Crafts | |
| Art Social Group | |
| Art Therapy | |
| Art Therapy | |
| Art Therapy | |
| Art with Creative Life | |
| Arts and Crafts | |
| Beading Poppy | |
| Bob Ross Paint and Pizza | |
| Bob Ross Paint Night | |
| Book Club: Harry Potter © | |
| Brownies on Thursday | |
| Candy Apples | |
| Cheap Eats Granville | |
| Cheap Eats St. Helen's | |
| Coffee & Creative Monday | |
| Community Meal Planning | |
| Cooking and Lifeskills | |
| Cooking Classes | |
| Craft Event | |
| Crayon Art | |
| Creative Journaling | |
| DIY Zen Garden | |
| Dungeons and Dragons | |
| Dungeons and Dragons | |
| Game nights | |
| GAME READY | |
| GAME READY | |
| Gamer's Unite | |
| Gamer's Unite | |
| Games Granville | |
| Gourd Painting | |
| Healthy Relationships Dialogue | |
| How to Survive a Pandemic: A Mindful and Artful Way | |
| Knitting | |
| Life Hacks | |
| Life Hacks | |
| Nintendo Switch Party | |
| Online: Rock Decorating | |
| Paint and Pizza | |
| Paint and Pizza | |
| Paper Quilling | |
| PCA Cooking | |
| Peer Support Baking | |
| Pottery Group | |
| Pottery Group | |
| Pottery | |
| Pottery | |
| Preserving Food | |
| Quilling | |
| Renfrew Cooking Group | |
| Renfrew Games Group | |
| Renfrew Gardening Group | |
| Renfrew Lifeskills | |
| Rock Painting | |
| Saint Helen's Clean Sweep | |
| Saint Helen's Cooking | |
| Saint Helen's Meal Planning | |
| Self-Esteem Workshop | |
| Self-Esteem | |
| Sketching in Nature | |
| Slime Making | |
| Sundaes | |
| TYES- D&D | |
| Virtual Bingo | |
| Virtual Games 0520 | |
| Virtual Group: Drawing Tutorial | |
| Young Adult Game Night (17+) | |
| Youth D&D | |
| Community Cooking Group | |
| Cookies for Mental Health Week | |
| Kettle Breakfast | |
| Kettle Cooking | |
| Kettle Gardening Group | |
| Kettle Home Skills Drop-In | |
| Kettle Meal Planning | |
| Kettle on Burrard - Cheap Eats / Community Walk | |
| KOB Gardening Group | |
| KOB Gardening | |
| Make and Take Bannock Bites | |
| Maker Monday - Activity | |
| Mason Jar Crafts | |
| Mosaic Colouring | |
| Paint Like Bob Ross | |
| St. Helen's Cheap Eats | |
| Thursday Mosaic | |
| Thursday Painting | |
| Tie Dye on Thursday | |
| T-shirt Designs | |
| TYES - Arts & Crafts: Playdough | |
| TYES - Arts and Crafts - Coloring Page | |
| TYES - Arts and Crafts Bracelet Making | |
| TYES - Arts and Crafts Independence | |
| TYES - Arts and Crafts Rock Painting | |
| TYES - Arts and Crafts | |
| TYES - Bead Animal Making | |
| TYES - Collage Making | |
| TYES - Lava Lamps | |
| TYES - Mascaraed Mask | |
| TYES Arts and Crafts - Origami | |
| TYES Arts and Crafts - Rock Painting | |
| TYES Arts and Crafts - Tye Dye | |
| TYES ARTS AND CRAFTS GARDENING | |
| TYES Arts and Crafts | |
| TYES Arts and Crafts: Free for All Paint | |
| TYES Arts and Crafts: Light Sabers | |
| TYES Arts and Crafts-Bracelets | |
| TYES Arts and Crafts-Dream Catchers | |
| TYES Arts and Crafts-Firefly Jar | |
| TYES Arts and Crafts-Nutrition | |
| TYES Arts Crafts | |
| TYES- Healthy Boundary's | |
| TYES- Muffins | |
| TYES- Splatter Painting | |
| Tyes/arts and crafts Brownies | |
| Wellness Wednesday Goals | |
| Wellness Wednesdays - Internet Safety/Social Media | |
| Wellness Workshop Series - Belonging: Finding Our Kind | |
| Wellness Workshop Series - Food and You | |
| Wellness Workshop Series - Stuck on Sleep | |
| Wellness Workshop Series | |
| Emotional/Mental | BCCYIC Week 2021: Movie Night |
| Body Image 101 | |
| CBT for Social Anxiety | |
| CBT Foundations for Anxiety/Depression | |
| CBT Foundations | |
| CBT Mood Management | |
| CBT Skills Group | |
| CBT Skills May 2021 | |
| CBT | |
| Chill Out Friday - Disney's Mulan | |
| Chill Out Fridays - Disney Soul | |
| Cinema Therapy | |
| DBT Comp | |
| DBT Prep | |
| DBT Skills Group | |
| DBT Skills Training | |
| DBT Skills | |
| DBT Skills | |
| DIALECTICAL BEHAVIOUR THERAPY | |
| Eco Art Therapy | |
| EFFT Caregiver Group | |
| EFFT Caregiver Workshop | |
| Get Grounded | |
| Get Grounded | |
| Girls Group- Meditation | |
| ICY Art Group | |
| Mending Mindsets (Anxiety Group) | |
| Mind Me | |
| Mind Me | |
| Mindful Gardening Group | |
| Mindful | |
| MindShift Anxiety Group | |
| Positive Affirmations | |
| SP20 YMIND | |
| Spa Day | |
| Stress Management | |
| Therapeutic Arts | |
| Therapeutic Performance | |
| Wellness Wednesday Depression | |
| WW Anxiety | |
| YMIND | |
| Y-mind | |
| YMIND | |
| Youth Mind | |
| Youth Mindfulness | |
| Youth Mindfulness | |
| Physical | Disc Golf |
| Garden Group | |
| Healthy By Nature- Boundary Bay | |
| Healthy By Nature | |
| Healthy By Nature: Mike Lake | |
| Hiking Group - POWER TO BE | |
| Hixon Falls | |
| Indoor Rock Climbing | |
| KOB Coffee Walk | |
| LOUTET FARM GROUP | |
| Loutet Farm | |
| Lower Falls Hike | |
| Mindful Movement A | |
| Mindful Movement B | |
| Mindful Movement Yoga | |
| Mindful Movement | |
| Outdoor Sports | |
| Quarantine Fitness Crew | |
| Quarantine Fitness Crew | |
| Quarantine Fitness Group | |
| Rec Outing | |
| Renfrew Recreational Group | |
| Renfrew Walks | |
| RockWall Climbing Outing | |
| Self Defense with KB | |
| Skate Boarding | |
| Virtual Yoga | |
| Virtual Yoga | |
| Walking Group | |
| Water Balloon Fight | |
| Wild Play Adventures | |
| Workout for Wellness | |
| Workout in the Park | |
| Yoga Group | |
| Yoga Group | |
| Yoga | |
| Youth Group - Skating | |
| Youth Rec Night | |
| Zoomba Group | |
| Zoom-ba Group | |
| Social | 2SLGBTQAl+ |
| BBQ Night | |
| Caregiver Support Group | |
| Community HangOut | |
| Costume Community Clean Up | |
| D&D | |
| Foundry PG Youth Group | |
| Foundry Youth Group | |
| FPG Youth Group | |
| Girls Group | |
| Girls Group | |
| Girls Social Group | |
| LGBTQ2S+ | |
| LGBTQ2S+ | |
| Peer Group - | |
| PG Foundry Youth Group | |
| Pumpkin Carving Day | |
| Pumpkin Carving Event | |
| Queer Cafe© (FODxQC) | |
| Queer Cafe© | |
| Queer Cafe (18-24) | |
| Queer Cafe | |
| Queer Cafe | |
| STH Breakfast Group | |
| Talking Heads (Renfrew) | |
| Tuesday Chat on Zoom | |
| Youth Advisory Committee | |
| Youth Group | |
| Community CMP | |
| Fall 2021 UNYA 2S Group | |
| Friday 13th Youth Group | |
| FYG Movie Night | |
| Girls Group MC College | |
| Halloween Movie Night | |
| Hearing Voices Group | |
| Inner City Jamz | |
| Jurassic World Watch Party | |
| Monday Kettle Drop-In | |
| Social Summer Series | |
| Toast and Tea | |
| TransMission Peer Group | |
| TYES - Arts and Crafts - Karaoke | |
| TYES - Arts and Crafts Charades | |
| TYES - Arts and Crafts Movie The Simpsons | |
| TYES - Arts and Crafts Movie | |
| TYES - Arts and Crafts Movies | |
| TYES - Chill Out Friday Movie Night | |
| TYES Arts and Crafts - Bingo/Board Games | |
| Young & Recovering | |
| Young & Recovering | |
| Young and Recovering | |
| YOUnity Lounge | |
| Spiritual/Cultural | Henna on a Thursday |
| Thursday Beading |
Three hundred and fifty-five unique youth accessed the Wellness Program, with 1319 unique visits. Figure 3 provides a summary of the number of unique youth and visits by month. The highest number of unique visits occurred in July 2021 (n=122; 9.2 %) and August 2021 (n=119; 9%), and no visits occurred in April and May 2020. The highest number of unique youth visited the program in August 2021 (n=89; 25%), and no youth visited in April and May 2020. Almost half (40%; n= 142) of youth identified that the Wellness Program was the first point of access to Foundry. In addition, 75% (n= 265) of youth accessed other programs at Foundry either before or after accessing the Wellness Program. The most commonly accessed services in addition to the Wellness Program were mental health (n=119; 45%), walk-in counselling (n=85; 32%), and physical health (n=76; 29%) (Fig. 4). When asked about how youth found out about Foundry (n = 175 responses), most identified a healthcare provider (n=36; 20.6%), school counselor/teacher (n=35; 20%), family member (n=32; 18.3%), friend (n=25; 14.3%), or a worker (n=20; 11.4%). When asked, “If the centre was unavailable, I would have gone to … ” (n = 173 responses), 56 (32.9%) said nowhere/I wouldn’t have gotten help, 38 (22%) said family members/friends, and 30 (17.3%) answered my healthcare provider.
Fig. 3.

Number of unique youth and visits by month
Fig. 4.

Summary of other foundry services accessed by youth participating in the wellness program
The demographic profile of youth accessing programs is provided in Table 5. All demographic questions were optional, so the number of responses differ from the total number of youth accessing the program. The majority identified as young girls/women (n= 103; 58.2%), followed by gender diverse (n=40; 22.6%) or young boys/men (n=34; 19.2%). The mean age was 19 years, and most participants were between the ages of 19-24 years (n= 154; 43.6%). Youth identified as heterosexual (n= 69; 40%), bisexual (n= 41; 24%), gay or lesbian (n=15; 9%) or preferred not to answer (n=19; 11%). For ethnicity/cultural background, 104 (58.2%) young people were White, 35 (19.2%) Indigenous, 7 (3.9 %) Chinese, and 7 (3.9%) Filipino.
Table 5.
Demographic characteristics of youth who accessed the wellness program
| Gender identification, n (%) | Total responses n = 177 |
| Young girl/woman | 103 (58.2) |
| Gender diverse | 40 (22.6) |
| Young boy/man | 34 (19.2) |
| Age in years, n (%) | Total responses n = 353 |
| <12 years | 4 (1.1) |
| 12-15 years | 102 (28.9) |
| 16-18 years | 80 (27.7) |
| 19-24 years | 154 (43.6) |
| >24 years | 13 (3.7) |
| Ethnic or cultural background, n (%) | Total responses n = 179 |
| White | 104 (58.2) |
| Additional options | 41 (22.6) |
| Indigenous | 35 (19.2) |
| Chinese | 7 (3.9) |
| Filipino | 7 (3.9) |
| Sexual Orientation, n (%) | Total responses n = 172 |
| Heterosexual | 69 (40) |
| Bisexual | 41 (24) |
| Prefer not to answer | 19 (11) |
| Gay or lesbian | 15 (9) |
| Additional options | 14 (8) |
| Questioning | 10 (6) |
| Asexual | 3 (2) |
Results of thematic analysis
A total of 9 young people participated in 2 focus groups. See Table 6 for a full break down of demographic information of participants. A total of 7 young people filled out the optional demographic survey. The average age of participants was 17 years, almost half (n=3) identified as female, and in regard to ethnic/cultural background almost half were Caucasian/white (n=3). Results specific to the evaluation objectives (described in Table 3) are presented here, further in-depth results of the thematic analysis will be presented elsewhere.
Table 6.
Demographic characteristics of youth who participated in focus groups
| Demographic informationa | Young people (n=7) |
|---|---|
| Age (years) | Mean = 17 |
| Range = 15-23 | |
| Gender Identity | Female (n=3) |
| Not sure/Questioning (n=2) | |
| Gender Fluid (n=1) | |
| Non-binary (n=1) | |
| Ethnic/Cultural background | Cauasian/White (n=3) |
| South Asian (n=2) | |
| Indigenous/Caucasian/Black (n=1) | |
| Indigenous/Caucasian (n=1) |
aAll demographic questions were optional, thus number of responses are different from the number of participants
Theme 1: Program successes
Young people explained that they appreciated and valued the social aspects of the program to connect with peers, and the facilitators, especially at a particularly isolating time during the global pandemic. Young people described the program facilitators with words such as “Welcoming; inclusive; accommodating; respectful; open to suggestions”. One young person explained the social aspect in further detail:
“ … people had the chance to sort of have banter and talk, if it's while cooking or painting and things like that which uh I think helped immensely when trying to make friends amid a pandemic... specifically for the online events, acquaintances and companionships were made”.
Another young person stated, “It helped with isolation and kept me from completely losing my marbles during quarantine”.
In addition to the social aspect, young people appreciated the opportunity to branch out and try new things. A young person explained:
“I found myself picking up different hobbies that I don't think I would've ever turned to if it wasn't for Foundry, such as painting, such as even making what was it, I think it was like mood boards. What I may have deemed as sort of like arts craftsy maybe childish, the Foundry embraced and really kind of captured it as an artistic and wellness activity”.
Theme 2. Desired program improvements
Young people talked about wanting more options for virtual or hybrid programming, specifically with accessibility interests in mind. Participants talked about how online events can reduce barriers to participation (such as transportation or social anxiety). One young person explained, “Having it virtually so we feel included and less isolated in person and virtually”. Another young person stated,
“ I mean it's nice through COVID it was definitely still through a screen, but even just baking cookies with everybody like on the phone kind of thing, it was nice, it was a good connection, it was good to get like hands on”.
Young people identified they wanted better communication about and within the programs. From program leaders, they wanted discussions around mental health and other health topics. One person stated “More in depth conversation would have helped me feel more connected”. Youth also discussed a lack of clarity around the program, and a lack of advertising about it. One person explained this, “My one criticism is there's like no marketing so like people don't know that Foundry holds socials and the only reason I know is ‘cause the youth worker in my school told me”. Another young person explained this communication breakdown as an accessibility issue:
“I do think it is a little bit hard to get involved in them … just because there tends to be tighter knit groups and also just like, not as much accessibility if you don't know what you're doing. I think it could be more clear, at least for my location where it is and what's happening and how to get into them”.
Theme 3. The ideal Wellness Program
Young people shared that their ideal program would be accessible, educational and fun, arts-based, social, and include a range of activities. One young person highlighted the need for social interactions and education, “I dislike the repetition of the same conversation topics that seems surface level. The topics don’t let us get to know each other very well”. Another young person summarized the need for a range of physical activities, “I would love to do activities like canoeing for example, because just being in the water, being out in nature, I have like a list written down of things I want to do after the pandemic is over. I would love to go bowling, go ice-skating, like using your body”.
Discussion
To the best of our knowledge, this is the first study to describe development and phased implementation of leisure-based activities (known as the Wellness Program) across an IYS network. This study was done as part of a developmental evaluation [31, 32] to understand the complex system that is Foundry. At a provincial level, the BC Ministry of Mental Health and Addictions announced significant investment of government dollars for child and youth mental health support with prevention, early intervention, and wellness promotion being identified as key pillars [39]. This study helps to understand how an IYS such as Foundry can quickly adapt to the needs of youth and emerging circumstances (e.g., COVID) to co-design services that can be offered alongside traditional health services to address these key pillars. Promisingly, 355 unique youth accessed the Wellness Program over a two two-year period after program launch with 1319 unique visits. The highest number of visits occurred in July 2021 (n=122; 9.2 %) and August 2021 (n=119; 9%), with the greatest number of unique youth also visiting in August 2021 (n=89; 25%). No visits occurred in April and May 2020. This corresponds with the start of the COVID-19 pandemic lockdown, subsequent waves, and ease of restrictions in the province of BC. The province entered Step 3 of its Restart Plan July 1st, 2021, marked as a major milestone allowing indoor and outdoor group gatherings [40]. Almost half (40%) of youth identified that the Wellness Program was the first point of access to Foundry, indicating that these programs could be a gateway to other services and have the potential for early identification, intervention and treatment for other conditions. Youth commonly accessed mental health services (45%) in addition to the Wellness Program, indicating that young people may be participating in leisure activities as an adjunct service for their mental health. Perhaps this is due to program aspects (such as physical activity) having the potential to reduce anxiety and depression symptoms for young people [20] and potential to be a valuable mental health promotion tool [41]. Results from the focus groups with young people are important and being considered as the program continues to evolve and is scaled-up across the province at new centres. This includes the positive social aspect, a desire for hybrid in-person and online programming, improved communication in regard to what the program entails, and for Foundry to strive to offer an ideal program that is accessible, educational and fun, arts-based, social, and include a range of activities.
At a national level, youth mental health has been identified as a top priority for health care in Canada [42]. However, studies done during the pandemic have suggested mental health and substance use concerns for young Canadians [9, 43–45], identifying trans and gender diverse youth a particularly at-risk population during this time [45]. Hawke and colleagues [45] identified that trans and gender diverse youth are experiencing more mental health concerns, have fewer social supports, and have more unmet mental health and substance use service needs. In our study, 40 (22.6%) of youth identified as gender diverse (the second highest gender identity), and the most commonly accessed service in addition to the program was mental health services (45%). It is possible that these gender diverse youth accessed the program for reasons such as social supports, mental health concerns, and unmet service needs. A longitudinal study identified that mental health concerns of young people are evolving over time (in alignment with COVID-19 infection rates and potentially seasonal factors) [43]. The authors have recommended that it is essential to “engage directly with youth to cocreate pandemic response strategies and mental health service adaptations” (pg. 9) [43]. This study is an example of how the Wellness Program was co-created with diverse communities putting youth and families at the forefront and implemented as an adaptation to existing mental health services in one province. Co-designed leisure activities warrant consideration in other provinces within IYS and other health services as we continue to navigate the ongoing pandemic and future recovery.
At an international level, investment in and consideration of the long-term mental health needs of young people have been deemed essential [46]. Other work has been done in Sweden to advocate for the importance of leisure activities for young people for health promotion [47]; however, such programs are offered in youth centres separate from health and social services, placing a burden on youth and families to navigate different systems. In the United States of America, subsidized leisure activities for youth are offered within ‘afterschool programs’ and are embedded with other content (e.g. linked to education curriculum), not stand alone or considered part of health services [48]. A review done by Hetrick and colleagues [22] describes international IYS as offering services for mental health, substance use, physical health, and vocational and educational programs. The authors’ synthesis of IYS principles and characteristics included “Services may also provide recreational or arts activities and drop-in or hang-out space” (p. 56) [22]. Consistently, the engagement of young people in the design of services is an integral part of IYS [22, 24], and development and implementation of the Wellness Program was in response to an identified need of young people. This work provides a template to guide other international IYS and health service settings to develop, tailor, and implement customized programming.
Strengths and limitations
This study provides novel insight into the development and implementation of unique leisure-based activities over a phased approach into IYS and offering alongside traditional health services as a means of health promotion. Although the sample size was small (n=9) the perspective of young people and their experience participating in the program as initial program evaluation has helped to understand the program and how it can be improved. The COVID-19 pandemic posed difficulties with navigating the offering, implementation, and tracking of programs. 'Toolbox' data did not capture youth participating virtually, thus the numbers reported in this study are likely an underrepresentation. Staff required 'Toolbox' training and had limited resources/capacity for data entry during the pandemic. The rapid development and expansion of Foundry centres pose challenges for research and program evaluation to keep up alongside. Each Foundry centre could develop its own unique program, which ultimately led to a wide variety of activities offered, and at times it was challenging to understand details (such as frequency, activities, group size).
Future directions
As this work was part of developmental evaluation, multiple iterations over the course of the evaluation period are being done [31, 32]. Our team is working to analyze additional qualitative data (1-1 interviews with program staff) to better understand youth and program staff experiences for program improvement, and to establish how ‘Toolbox’ can be utilized for tracking virtual programs. Youth peer evaluators have presented the results from the focus groups with young people to FCO staff to initiate knowledge exchange. Our team is continuing to share results with staff offering programs (and developing new ones) as Foundry scales up across BC. Future research should explore the impact of the Wellness Program on short- and long-term health outcomes for young people and morbidity prevention considering pre-post and longitudinal designs. Future research could also explore cost-effectiveness of programs and the potential to reduce or mitigate wait times to other costly mental health services, as has been done in other settings such as a university campus and access to counselling services [49].
Conclusions
This study provides novel insight into the development and implementation of leisure-based activities known as the Wellness Program into IYS which can be leveraged as a health promotion tool. This work provides a template for guidance that can be utilized within international IYS settings to develop, tailor, and implement similar programming suited to needs of young people, their families/caregivers, and communities. The initial reach of the Wellness Program over two years is promising, and it may be acting as a gateway for young people to access other health services. From initial program evaluation, young people enjoyed the social aspect with peers and facilitators, and identified important program improvements that are being considered as the program grows. Further work is needed to understand youth health outcomes and experiences associated with participation in such programs. A multidisciplinary team is continuing to conduct evaluation of the Wellness Program using mixed-methods over multiple iterations as part of developmental evaluation.
Supplementary Information
Acknowledgements
The authors would like to acknowledge the help of Kelli Wuerth for proofreading this article.
Abbreviations
- MHSU
Mental health and substance use
- IYS
Integrated youth services
- BC
British Columbia
- FCO
Foundry Central Office
- FIPA
Freedom of Information Privacy Act
- PIPA
Personal Information Privacy Act
Authors’ contributions
Author KG led writing of the manuscript, interpretation of the 'Toolbox' data, and analysis of the qualitative data. Authors JA, BM, AE, KT, MW, SB and SM all contributed to revision and writing of the manuscript. GC analyzed data. All authors read and approved the final manuscript.
Funding
Funding for The Wellness Program and for this study was received from donors to St. Paul’s Hospital Foundation, with significant contributions from the Morris Foundation and Nicola Family Foundation. Dr. Glowacki received a Michael Smith Health Research BC/Centre for Health Evaluation and Outcome Sciences research trainee award. Dr. Barbic received a Michael Smith Foundation for Health Research scholars award.
Availability of data and materials
The dataset generated and analysed during the current study are not publicly available due to privacy reasons but are available from author SB on reasonable request.
Declarations
Ethics approval and consent to participate
All research was carried out in accordance with relevant guidelines and regulations in the Declaration of Helsinki. Ethics approval was received from the University of British Columbia Behavioural Research Ethics Board (ID: H21-01510). Informed consent was received from youth prior to survey completion, and youth do not have to complete the survey in order to receive services (i.e., completion of the surveys is voluntary). Verbal consent was attained prior to completion of focus groups for the purposes of program evaluation. In accordance with the BC Infants Act of 1996 [50] it is deemed unnecessary to require parental/legal guardian consent for all minors (under the age of 19) to access health services. The capacity of a minor to provide informed consent is determined by assessing the ability of the minor’s physical, mental, and emotional development to determine an understanding and full appreciation of the nature and consequences of the proposed services, including the refusal of such services.
Consent for publication
Not applicable, no individual data is presented or identifying.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Canadian Institute for Health Information. Child and Youth Mental Health in Canada. Ottawa, ON: Canadian Institute for Health Information; 2020. Available from: https://www.cihi.ca/en/child-and-youth-mental-health-in-canada-infographic
- 2.Solmi M, Radua J, Olivola M, Croce E, Soardo L, de Pablo GS, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2021;2021(27):281–295. doi: 10.1038/s41380-021-01161-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Canadian Institute for Health Information. Mental Health of Children and Youth in Canada. Ottawa, ON: Canadian Institute for Health Information; 2020. Available from: https://www.cihi.ca/en/mental-health-of-children-and-youth-in-canada.
- 4.Statistics Canada. Census of Canada. Canada: Statistics Canada; 2011. Retrieved from https://cmha.bc.ca/documents/mental-illnesses-in-children-and-youth-2/
- 5.Jakovljevic M, Bjedov S, Jaksic N, Jakovljevic I. COVID-19 pandemia and public and global mental health from the perspective of global health security. Psychiatr Danub. 2020;32(1):6–14. doi: 10.24869/psyd.2020.6. [DOI] [PubMed] [Google Scholar]
- 6.McGorry PD, Mei C, Chanen A, Hodges C, Alvarez-Jimenez M, Killackey E. Designing and scaling up integrated youth mental health care. World Psychiatry. 2022;21(1):61–76. doi: 10.1002/wps.20938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Samji H, Wu J, Ladak A, Vossen C, Stewart E, Dove N, Long D, Snell G. Mental health impacts of the COVID-19 pandemic on children and youth–a systematic review. Child Adolesc Mental Health. 2022;27(2):173–189. doi: 10.1111/camh.12501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zenone MA, Cianfrone M, Sharma R, Majid S, Rakhra J, Cruz K, Barbic S. Supporting youth 12–24 during the COVID-19 pandemic: how Foundry is mobilizing to provide information, resources and hope across the province of British Columbia. Glob Health Promot. 2021;28(1):51–59. doi: 10.1177/1757975920984196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Labana, R. V. The public mental health while in a community quarantine due to COVID-19 pandemic: a scoping review of literature using Google Scholar. 2020. 10.20944/preprints202005.0050.v1
- 10.Hawke LD, Barbic SP, Voineskos A, Szatmari P, Cleverley K, Hayes E, Relihan J, Daley M, Courtney D, Cheung A, Darnay K. Impacts of COVID-19 on youth mental health, substance use, and well-being: a rapid survey of clinical and community samples: répercussions de la COVID-19 sur la santé mentale, l’utilisation de substances et le bien-être des adolescents: un sondage rapide d’échantillons cliniques et communautaires. Can J Psychiatry. 2020;65(10):701–709. doi: 10.1177/0706743720940562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Norman M, Silva D, Kennedy L, Cipolli III W. ‘Essential for the soul’?: leisure as a flashpoint during COVID-19 lockdowns in Ontario, Canada. Ann Leis Res. 2022:1–20. 10.1080/11745398.2022.2055586.
- 12.Iwasaki Y, Coyle C, Shank J, Messina E, Porter H, Salzer M, Baron D, Kishbauch G, Naveiras-Cabello R, Mitchell L, Ryan A. Role of leisure in recovery from mental illness. Am J Psychiatric Rehabil. 2014;17(2):147–165. doi: 10.1080/15487768.2014.909683. [DOI] [Google Scholar]
- 13.Blomfield CJ, Barber BL. Developmental experiences during extracurricular activities and Australian adolescents’ self-concept: particularly important for youth from disadvantaged schools. J Youth Adolesc. 2011;40:582–594. doi: 10.1007/s10964-010-9563-0. [DOI] [PubMed] [Google Scholar]
- 14.Sato M, Jordan JS, Funk DC. The role of physically active leisure for enhancing quality of life. Leis Sci. 2014;36(3):293–313. doi: 10.1080/01490400.2014.886912. [DOI] [Google Scholar]
- 15.Kim YJ, Cho JH. Correlation between preventive health behaviors and psycho-social health based on the leisure activities of South Koreans in the COVID-19 crisis. Int J Environ Res Public Health. 2020;17(11):4066. doi: 10.3390/ijerph17114066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Timonen J, Niemelä M, Hakko H, Alakokkare A, Räsänen S. Associations between Adolescents’ social leisure activities and the onset of mental disorders in young adulthood. J Youth Adolesc. 2021;50(9):1757–1765. doi: 10.1007/s10964-021-01462-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hiremath P, SuhasKowshik CS, Manjunath M, Shettar M. COVID-19: impact of lockdown on mental health and tips to overcome. Asian J Psychiatr. 2020;51:102088. doi: 10.1016/j.ajp.2020.102088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, Rubin GJ. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912. doi: 10.1016/S0140-6736(20)30460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Abu-Omar K, Rütten A, Burlacu I, Schätzlein V, Messing S, Suhrcke M. The cost-effectiveness of physical activity interventions: a systematic review of reviews. Prev Med Rep. 2017;8:72–78. doi: 10.1016/j.pmedr.2017.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Larun L, Nordheim LV, Ekeland E, Hagen KB, Heian F. Exercise in prevention and treatment of anxiety and depression among children and young people. Cochrane Database syst Rev. 2006;3:CD004691. doi: 10.1002/14651858.CD004691.pub2. [DOI] [PubMed] [Google Scholar]
- 21.Mammen G, Faulkner G. Physical activity and the prevention of depression: a systematic review of prospective studies. Am J Prev Med. 2013;45(5):649–657. doi: 10.1016/j.amepre.2013.08.001. [DOI] [PubMed] [Google Scholar]
- 22.Hetrick SE, Bailey AP, Smith KE, Malla A, Mathias S, Singh SP, et al. Integrated (one-stop shop) youth health care: best available evidence and future directions. Med J Aust. 2017;207(S10):S5–18. doi: 10.5694/mja17.00694. [DOI] [PubMed] [Google Scholar]
- 23.Settipani CA, Hawke LD, Cleverley K, Chaim G, Cheung A, Mehra K, et al. Key attributes of integrated community-based youth service hubs for mental health: a scoping review. Int J Ment Health Syst. 2019;13(1):1–26. doi: 10.1186/s13033-019-0306-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mathias S, Tee K, Helfrich W, Gerty K, Chan G, Barbic SP. Foundry: Early learnings from the implementation of an integrated youth service network. Early Interv Psychiatry. 2021 doi: 10.1111/eip.13181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hilferty F, Cassells R, Muir K, Katz I. Is headspace making a difference to young people's lives? Sydney (AU): Social Policy Research Centre; 2015. p. 253. [Google Scholar]
- 26.O’Keeffe L, O’Reilly A, O’Brien G, Buckley R, Illback R. Description and outcome evaluation of Jigsaw: an emergent Irish mental health early intervention programme for young people. Ir J Psychol Med. 2015;32(1):71–77. doi: 10.1017/ipm.2014.86. [DOI] [PubMed] [Google Scholar]
- 27.Boisser P. Evaluation de la mise en place du dispositif “maison des adolescents” (MDA): rapport] [French] Paris: Membres de I’Inspection Generale des Aff aires Sociales; 2013. [Google Scholar]
- 28.Bailey R, Torrie R, Osborne R, Bagshaw S, Blyth Blyth, Davidson J, et al. How we know what we’re doing works: measuring youth outcomes at kapiti youth support. New Zealand: Health Research Council of New Zealand, KYS and Evauation Works Ltd; 2013. p. 58. [Google Scholar]
- 29.Halsall T, Manion I, Iyer SN, Mathias S, Purcell R, Henderson J. Trends in mental health system transformation: Integrating youth services within the Canadian context. Healthc Manage Forum. 2019;32(2):51–55. doi: 10.1177/0840470418808815. [DOI] [PubMed] [Google Scholar]
- 30.Statistics Canada. Rural and Urban Population Centres. Canada: Statistics Canada; 2016 [updated 2018 Sept 17; cited 2022 Mar 28] Available from: https://www150.statcan.gc.ca/n1/pub/92-195-x/2011001/geo/pop/def-eng.htm.
- 31.Patton MQ. Developmental evaluation: Applying complexity concepts to enhance innovation and use. New York: Guilford press; 2010.
- 32.Patton MQ, McKegg K, Wehipeihana N, editors. Developmental evaluation exemplars: Principles in practice. New York: Guilford publications; 2015.
- 33.World Health Organization . Director-General’s opening remarks at the media briefing on COVID19. 2020. [Google Scholar]
- 34.Providence Health Care Society. Vancouver: Wellness Program Guide, 2021.
- 35.Payne L, Ainsworth B, Godbey G. Leisure, health, and wellness: making the connections. Urbana, IL: Venture Publishing, Inc.; 2010. [Google Scholar]
- 36.Clarke V, Braun V, Hayfield N. Thematic analysis. Qual Psychol. 2015;3:222–248. [Google Scholar]
- 37.Smith B, McGannon KR. Developing rigor in qualitative research: problems and opportunities within sport and exercise psychology. Int Rev Sport Exerc Psychol. 2018;11(1):101–121. doi: 10.1080/1750984X.2017.1317357. [DOI] [Google Scholar]
- 38.Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi: 10.1191/1478088706qp063oa. [DOI] [Google Scholar]
- 39.Government of British Columbia. A Pathway to Hope. 2021. Available from: https://www2.gov.bc.ca/assets/gov/government/ministries-organizations/ministries/mental-health-addictions/pathway_to_hope_update_report_final.pdf.
- 40.Government of British Columbia. B.C. shifts to Step 3 of restart plan. Office of the Premier. 2021. Retrieved from: https://news.gov.bc.ca/releases/2021PREM0043-001268
- 41.Pascoe M, Bailey AP, Craike M, Carter T, Patten R, Stepto N, Parker A. Physical activity and exercise in youth mental health promotion: a scoping review. BMJ Open Sport Exerc Med. 2020;6(1):e000677. doi: 10.1136/bmjsem-2019-000677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Malla A, Shah J, Iyer S, Boksa P, Joober R, Andersson N, Lal S, Fuhrer R. Youth mental health should be a top priority for health care in Canada. Can J Psychiatry. 2018;63(4):216–222. doi: 10.1177/0706743718758968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hawke LD, Szatmari P, Cleverley K, Courtney D, Cheung A, Voineskos AN, et al. Youth in a pandemic: a longitudinal examination of youth mental health and substance use concerns during COVID-19. BMJ Open. 2021;11(10):e049209. doi: 10.1136/bmjopen-2021-049209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hawke LD, Monga S, Korczak D, et al. Impacts of the COVID-19 pandemic on youth mental health among youth with physical health challenges. Early Interv Psychiatry. 2021;15:1146–1153. doi: 10.1111/eip.13052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Hawke LD, Hayes E, Darnay K, et al. Mental health among transgender and gender diverse youth: an exploration of effects during the COVID-19 pandemic. Psychol Sex Orientat Gend Divers. 2021;8:180–187. doi: 10.1037/sgd0000467. [DOI] [Google Scholar]
- 46.Holmes EA, O'Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, Ballard C, Christensen H, Silver RC, Everall I, Ford T. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020;7(6):547–560. doi: 10.1016/S2215-0366(20)30168-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Fredriksson I, Geidne S, Eriksson C. Leisure-time youth centres as health-promoting settings: Experiences from multicultural neighbourhoods in Sweden. Scand J Public Health. 2018;46(20). 10.1177/1403494817743900. [DOI] [PubMed]
- 48.Haglund B, Anderson S. Afterschool Programs and Leisure-Time Centres: Arenas for Learning and Leisure. World Leisure J. 2009;51(2):116–129. doi: 10.1080/04419057.2009.9674594. [DOI] [Google Scholar]
- 49.Glowacki K, Cina I, Kandola M, Faulkner G. Mind in Motion: an exercise intervention for university students seeking mental health treatment on campus. Executive Summary. Population-Physical Activity Lab, UBC. 2019.
- 50.Government of British Columbia. Infants Act, Chapter 223. King’s Printer, British Columbia. 1996.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The dataset generated and analysed during the current study are not publicly available due to privacy reasons but are available from author SB on reasonable request.