

Abstract
Objectives
Industrial workers are exposed to various musculoskeletal problems especially in tasks related to production. Low back pain is the main problem in most musculoskeletal disorders. Therefore, our study aims to identify the prevalence of work-related low back pain and its risk factors among industrial workers in Bangladesh.
Materials and methods
A sample of 384 industrial workers aged 18–55 years in Bangladesh was selected to conduct this cross-sectional study to assess low back pain prevalence and identify its risk factors. Regression analysis was performed regarding socioeconomic status and risk factor related to LBP through interviews and questionnaires.
Results
Data analysis showed that the prevalence of LBP in industrial workers in Dhaka City was 238 (62%). Low back pain was associated with increasing age (odd ratio = 1.05). Other significant risks for pain in the low back were being a permanent employee (OR 3.15) and working more than 8 h (OR = 1.99). Also, LBP was associated with incorrect body mechanics use, repetitive bending, and continuous long-time sitting risk was higher than others.
Conclusion
The results of this investigation highlight a high proportion of LBP and its risk factors among industrial workers in Dhaka City. Age, type of employment, working hours, use of incorrect body mechanics, repeated bending or twisting, and prolonged sitting were among the risk factors for back pain. Therefore, exercising, providing adequate training for properly maintaining body mechanics, and avoiding bad positions may be among the most powerful steps needed to avoid or prevent development of back pain.
Keywords: Industrial worker, Low back pain, Work-related risk factors, Low wage workers, Prevalence, Bangladesh
Introduction
Low back pain (LBP) can be defined as chronic or acute pain that is felt in the lumbosacral, buttocks, or upper leg area of the human body, and lower back diseases are associated with work-related faulty postures [1]. The result of this issue is increased movement difficulty, disability, poor service, poor lifestyle, and absences for sickness in working places [2]. One of the greatest usually reported muscle or joint problem is low back pain, which is a the leading cause of burden on health systems, individuals, and the social care system [3]. Hazardous factors for pain in the lower back and its prevalence among workers are unknown in Bangladesh. One of the major public health problems is LBP, with over 80% of the world’s population reporting LBP at some point in their lives [4]. Especially in low- and middle-income countries, LBP prevalence is high [5]. Industrial workers in poor working conditions bear some responsibilities for LBP. Workers in any section of industries are often managing many unplanned works with various tasks and obligations [6]. Industrial work is a physically demanding job. Low back pain is related to a variety of occupations, such as driving, manual handling, operating, being a technician, general worker, cleaner, and many more occupations, that involve many inappropriate body movements, which in turn contribute to MSDs [7]. Work-related physical exposures include, especially standing or sitting for a long time, lifting heavily, cleaning tiles and vacuuming in every shift, repeatedly bending or leaning forward, managing manual instruments, working in faulty positions, and working out of physical capacity, working with full body vibration, to do Continuing to work despite injuries, lack of regular, adequate rest is a well-established risk factor for LBP in low-income industrial workers [8]. It forms easy to see that numerous injury types are straightly involved in the tasks performed in the industrial occupation [9]. The United States Housekeepers had the utmost total rate of injury and the maximum proportion of MSDs, most generally low back pain, among guest house workers [10]. LBP has been one of the leading causes of disease in developing countries than in underdeveloped countries in recent decades [11]. It is often seen that back pain and its frequency are considered trivial problems compared to other diseases that have a high mortality rate, like cancer or contagious diseases 12]. For the current lifestyle, low back pain has placed a significant economic burden on the government, especially in the areas of healthcare costs, reduced productivity, lost working days, and disability [13]. However, in the case of illness, the pain of back disorders is a leading effect of many factors, including the absence of work and the limitation of activities in the workplace. In addition to the extra human cost, back pain has a high impact on society’s resources [14].
Industrial work-related LBP is associated with disclosure to ergonomic pressure at work, physical, psychosocial, and/or individual hazard factors [15]. In some research, wide extents of effects related to low back pain have been characterized. Into these, carrying and lifting heavy contents [16]. The 2010 GBD (Global Burden of Disease) research approximates that LBP is among the major 10 disorders and injuries that are calculated for incapability-stable life years globally [17]. LBP affects not only the economic loss of workers and the quality of social life, such as the reduced capacity to work, decrease production, and early retirement but also the organization, society, and country as a whole [18]. Although there has been a lot of research on back pain in Bangladesh, among the several groups of workers in the bank, universities, and hospitals, such as the degree of back pain and related causes, no research has been done on industrial workers. Therefore, the research was driven to discover the prevalence and identify risk factors of low back pain among industrial workers in Dhaka, Bangladesh.
Materials and methods
Study design and participants
The study was selected as an organization-based cross-sectional study conducted from June 2022 to November, 2022. The research was driven at Gazipur area industries in Bangladesh. Gazipur is one of the leading industrial areas, which is the part of Dhaka division in Bangladesh. Data were collected from 384 participants aged 18 to 55 years industrial workers in Bangladesh who were apparently healthy and active in working. The Gazipur is the known industries area in Dhaka and workers are the largest population in this area.
Source and study population
All workers who worked in Dhaka City were the source population. Workers in Gazipur area industries, who had worked at least 1 year in the industries, were included in this study. While, workers with spinal deformities (such as excessive kyphosis, lordosis, flat back, and scoliosis), inflammatory diseases, disc prolapse, or traumatic injury affecting the musculoskeletal system were excluded from the study.
Determine sample size and procedures
The sample size was determined using a single population proportion formula, a 50% standard deviation, 5% margin of error, and 95% confidence interval resulting in 384 industrial workers randomly selected from 6 industries. A systematic randomize sampling technique was used to select the study respondent among the industries.
Data measurements
A face-to-face interview was conducted while collecting data for this study and adequate precautions against COVID-19 were taken. The semi-structured questionnaire was developed primarily in English and later translated into Bengali. After the translation, the questionnaire was checked by another translator to check its accuracy. However, the local language was used to communicate with the respondents. Then, an orientation was organized among the collectors along with 38 (10%) field tests and finally, data was collected through door-to-door questionnaires from the industrial workers.
The project was organized in Sreepur, Chandra, Sofipur, Baroipara, Khamarbari, Kobirpur, Konabari, Kaliakoir, and Naojor areas of Gazipur City in Bangladesh. We collected data from them with their permission. The survey asked subjects, using only Bengali words, “Have you had pain or tenderness in your lower back most days or month (currently or in the past)?”. One response box had o on the questionnaire for the lower back of the body (yes and no).
Statistical analysis
The χ2 test was used to see the relation of several factors with the magnitude of pain in the lower back. All answer sheets were checked for exactness, completeness, and internal consistency. Inconsistent data is discarded. Accurate data were entered into SPSS version 25 for analysis. We used logistic regression to evaluate the prevalence of specific low back pain in study populations and also fix to evaluate factors related to LBP. LBP was regressed against social-demographic, individual, and work-related factors differently. Prior fix the binary logistic regression, the quality of the model test was evaluated by Hosmer and Lemeshow test, and the hypothesis was satisfied (p value > 0.05). Qualitative data were used for thematic content analysis. Analyzes were limited to 384 Bangladeshi workers aged 18 to 55 years.
Data quality control
During data collection, supervisors checked each completed questionnaire for completeness and consistency. Throughout the data collection period, the data collectors at each site were supervised and had regular meetings with the principal investigator.
Results
All 384 completed and valid questionnaires were returned and considered for the analysis, which gives a response rate of 100%.
Socio-demographic characteristics of the study respondents
The majority 331 (86.2%) of the study participants were males. A maximum of 307 (79.9%) of the respondents had more than 1 year of work experience in an industry job. The mean (± SD) age of the participants was 31.32 ± 6.98 years and above half 210 (54.7%) of participants had an age limit of 28 to 37 years. Over two-thirds of the respondents totaling 266 (69.3%) had an average monthly income below 12,999 BDT. Only 193(50.3%) workers have health and safety tanning, and most of the 325 (84.6%) respondent’s employment patterns are permanent (Table 1).
Table 1.
Socio-demographic characteristics of the study respondents, Dhaka, Bangladesh (n = 384)
| Characteristics | Overall | Male | Female |
|---|---|---|---|
| N (%) | N (%) | N (%) | |
| Sex | |||
| 384(100%) | 331 (86.2%) | 53(13.8%) | |
| Age group (in years) | |||
| 18–27 | 118(30.7%) | 92 (24%) | 26(6.8%) |
| 28–37 | 210(54.7%) | 188(49%) | 22(5.7%) |
| 38–47 | 47(12.2%) | 43(11.2%) | 4(1%) |
| 48–59 | 9(2.3%) | 8(2.1%) | 1(0.3%) |
| Mean age in years (mean ± SD) | 31.32 ± 6.98 | 31.64 ± 6.94 | 29.28 ± 6.97 |
| Marital status | |||
| Single | 114(29.7%) | 93(24.2%) | 21(5.5%) |
| Married | 270(70.3%) | 238(62.0%) | 32(8.3%) |
| Average monthly income | |||
| 8000–12,999 | 266(69.3%) | 231(60.2%) | 35(9.1%) |
| 13,000–15,999 | 56(14.6%) | 48(12.5%) | 8(2.1%) |
| 16,000–19,999 | 40(10.4%) | 33(8.6%) | 7(1.8%) |
| 20,000 + | 22(5.7%) | 19(4.9%) | 3(0.8%) |
| Employment pattern | |||
| Temporary | 59(15.4%) | 37(9.6%) | 22(5.7%) |
| Permanent | 325(84.6%) | 294(76.6%) | 31(8.1%) |
| Specific work experience | |||
| < 1 year | 77(20.1%) | 62(16.1%) | 15(3.9%) |
| > 1 year | 307(79.9%) | 269(70.1%) | 38(9.9%) |
| Working hours (per day) | |||
| < 8 h | 313(81.50%) | 274 (71.4%) | 39(10.20%) |
| > 8 h | 71(18.5%) | 57(14.80%) | 14(3.60%) |
| Training on health and safety | |||
| No | 191(49.7%) | 156(40.6%) | 35(9.1%) |
| Yes | 193(50.3%) | 175(45.6%) | 18(4.7%) |
Working status of the participants
Workers work in the workplace with various bad postures, which are revealed based on their work patterns and their interviews. About 52 (13.54%) of the industrial workers worked in a faulty position (like hanging and leaning forward) and 53 (13.80%) worked continuously in one position for long hours. Some workers were not pleased with their working environment. Among those who had pain proneness, 59 (15.36%) worked in forward bending or lying down and 57 (14.84%) sat for long periods of time (Table 2).
Table 2.
Working position related characteristics of study from survey where survey data (n = 384)
| Characteristics | Yes N (%) | No N (%) | |
|---|---|---|---|
| Working in an faulty position | Male | 41(10.7%) | 290(75.5%) |
| Female | 11(2.9%) | 42(10.9%) | |
| Overall | 52(13.5%) | 332(86.5%) | |
| Stationary position for a long time | Male | 48(12.5%) | 283(73.7%) |
| Female | 5(1.6%) | 48(12.5%) | |
| Overall | 53(13.8%) | 331(86.2%) | |
| Incorrectly using body mechanics | Male | 39(10.2%) | 292(76.0%) |
| Female | 6(1.6%) | 47(12.2%) | |
| Overall | 45(11.7%) | 339(88.3%) | |
| Repeated bending and twisting | Male | 52(13.5%) | 279(72.7%) |
| Female | 7(1.8%) | 46(12%) | |
| Overall | 59(15.4%) | 325(84.6%) | |
| Working beyond physical ability | Male | 24(6.3%) | 307(79.9%) |
| Female | 5(1.3%) | 48(12.5%) | |
| Overall | 29(7.6%) | 355(92.4%) | |
| Continuously long time sitting | Male | 49(12.8%) | 282(73.4%) |
| Female | 8(2.1%) | 45(11.7%) | |
| Overall | 57(14.8%) | 327(85.2%) | |
| Continue work despite injury or pain | Male | 17(4.4%) | 314(81.8%) |
| Female | 2(0.5%) | 51(13.3%) | |
| Overall | 19(4.9%) | 365(95.1%) | |
| Sing ergonomically improper tools | Male | 28(7.3%) | 303(78.9%) |
| Female | 3(0.8%) | 50(13%) | |
| Overall | 31(8.1%) | 353(91.9%) | |
Prevalence of low back pain
This research display that the prevalence of pain in the lower back among industry worker in the Dhaka area was 238 (62%). In addition, 238 (62%) of the workers had back pain affecting their ability to do normal work even if it lasted for at least 1 month during their working life. Of these, the majority of study workers 102 (42.86%) reported that low back pain had prevented them from working for at least 1 month or less during their job life (Fig. 1).
Fig. 1.
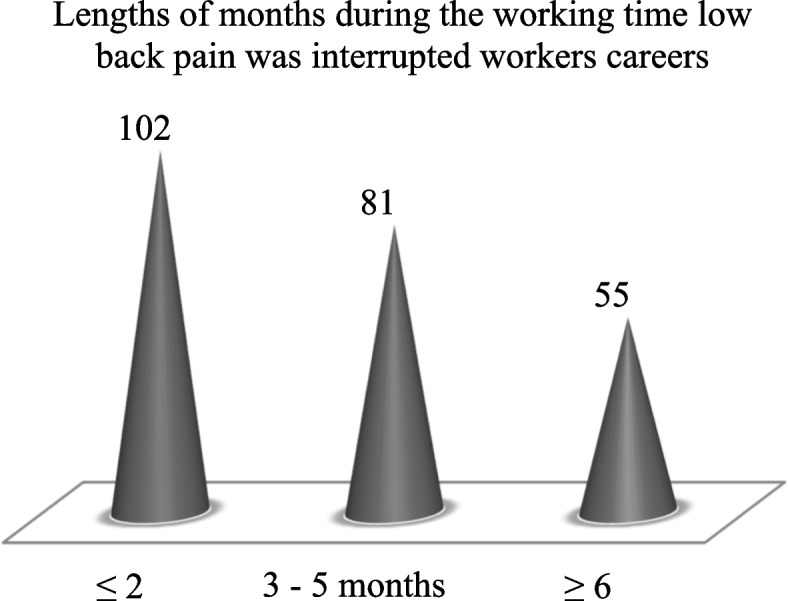
Lengths of months interrupted due to low back pain during workers job life
Factors associated with low back pain
Logistic regression showed that age, type of employment, working hours, incorrect use of body mechanics, repeated bending or twisting, and prolonged sitting had a statistically significant association with low back pain (p value ≤ 0.05). However, no significant association was observed between gender, marital status, work experience, and training in health and safety with low back pain (Table 3).
Table 3.
Logistic regression of socio-demographic characteristics and factors related characteristics
| OR (95% CI) | p value | |
|---|---|---|
| Age in year | 1.05 (1.01, 1.09)* | .017 |
| Sex | ||
| Male | Reference | |
| Female | 1.94 (.97, 3.88) | .063 |
| Marital status | ||
| Single | Reference | |
| Married | 1.37 (.76, 2.45) | .293 |
| Employment | ||
| Temporary | Reference | |
| Permanent | 3.15 (1.55, 6.39)*** | .002 |
| Experience | ||
| < 1 year | Reference | |
| > 1 year | 1.07(.53, 2.13) | .856 |
| Working hours | ||
| < 8 h | Reference | |
| > 8 h | 1.99(1.04,3.82)** | .039 |
| Training on health and safety | ||
| No | Reference | |
| Yes | 1.42(.88, 2.31) | .154 |
| Incorrectly using body mechanics | ||
| No | Reference | |
| Yes | .027(.003, .209)* | .001 |
| Repeated bending or twisting | ||
| No | Reference | |
| Yes | .079(.021, .290)* | .000 |
| Continuously long time sitting | ||
| No | Reference | |
| Yes | .139(.027, .718)* | .019 |
This investigation showed that permanent employees had a higher risk of growing and becoming more mature back pain. Industrial job holders who have permanent job status had 3.15 times greater odds of having LBP when compared to temporary job holders (OR = 3.15, 95% CI 1.55, 6.39). Respondents working above than 8 h were 1.99 times more possible to have low back pain. OR = 1.99, 95% CI 1.04, 3.82). Younger workers were less possible to have back pain. Back pain was 1.05 times more likely with increasing age by 1 year OR = 1.05, 95% CI 1.01, 1.09).
According to this study, the workers worked in various postures in the industry. Their different body postures had been shown to be hazardous factors for LBP. Workers who were associated with using incorrect body mechanics, repeatedly bending or twisting the body, and sitting for long periods of time had a higher risk of back pain than others (OR = 0.027, 95% CI 0.003, 0.209), (OR = 0.079, 95% CI 0.021, 0.290)* and (OR = 0.139, 95% CI 0.027, 0.718)* were slightly higher. There is no relation between marital status, sex, and experience with increasing respondent’s having low back pain (OR = 1.94, 95% CI 0.97, 3.88), (OR = 1.37, 95% CI 0.76, 2.45) and for less than 1 year (OR = 1.22, 95% CI 0.64, 2.33), for more than 1 year (OR = 1.07, 95% CI 0.53, 2.13).
Discussion
The objective of our investigation was to assess low back pain prevalence and its related factors. According to this survey, the prevalence of pain in the lower back was 238 (62%) among industrial workers. This investigation revealed that industrial workers are at higher risk for developing low back pain. This investigation has similarities with several studies. Among the studies, 60% of hotel workers in Malaysia [19], 46% of workers in the UK [20], 58.1% of workers in Ethiopia, and 60% of industrial workers in India [21] had low back pain prevalence. The results of this study support low back pain in workers. On the other hand, the results of this investigation are more commonly reported than studies conducted in other countries. However, a slightly higher prevalence than this study was reported in a study from Egypt, where the prevalence of pain in the lower back among workers was reported as 63.3% [22].
This study found that the prevalence of low back pain increased significantly with age. Industrial workers who were older had significantly higher rates of LBP than those who were younger. Our research data is consistent with reports from the Centers for Disease Control and Prevention. According to the CDC report, workers aged 45–64 were more likely to experience pain than younger workers [23].
This study found employment status in the industry to be an acceptable prophecy of back pain; Permanent workers were more likely to have back pain than temporary workers. A possible reason for this could be regular work for long periods of the year. Permanent workers have the same production workload throughout the year. Furthermore, groups of workers due to low income, work overtime to meet household expenses, promotions/increments, and long-term jobs [24]. Longer work hours were associated with low back pain. In this study, industrial workers who performed overtime duty or worked more than eight hours per day were significantly associated with rising low back pain. Due to the high workload in industries, many workers have to do extra work.
Low back pain was associated with worker workload. In this study, improper use of body mechanics is associated with rising pain in the lower back. Certain groups of industrial workers used incorrect body mechanics at work, making them more prone to low back pain than others. A possible reason for this may be that improper use of body mechanics requires loads on the back and muscular parts of the body, and pain increases with physical exertion. This study found that repetitive bending or twisting while performing tasks was a risk factor for low back pain. Hotel workers in Ethiopia who were associated with repetitive bending or twisting during work were more likely to develop back pain. This finding is similar to our findings. The low back pain risk was richer in employees who sat for long periods of time. A possible reason for this may be that sitting for a continuous prolonged time increases the tendency of pain in the lower back due to over-stretching or over-loading of the lower back muscles.
Conclusions
In conclusion, the results of this study explain the prevalence of LBP and its risk factors among industrial workers in Dhaka City. This study showed a higher prevalence rate of LBP in industrial workers. Age, type of employment, working hours, incorrect use of body mechanics, repeated bending or twisting, and prolonged sitting were among the risk factors associated with low back pain. Therefore, taking breaks between tasks, exercising, providing adequate training for appropriate usage of body mechanics, avoiding repetitive bending or twisting, and prolonged sitting may be among the most powerful measures necessary to prevent low back pain.
Acknowledgements
Special thanks to Almighty Allah for giving us great opportunities to complete our research. We sincerely respect the respondents for participating in this study. We deeply respect our household members for inspiring our survey.
Data access, responsibility, and analysis
The main author takes responsibility for the integrity of the data and the accuracy of the data analysis and he has full access to all study data.
Abbreviations
- LBP
Low back pain
- MSDs
Musculo-skeletal diseases
- OR
Odd ratio
- GBD
Global Burden of Disease
- SPSS
Statistical Package for the Social Sciences
- SD
Standard deviation
- BDT
Bangladesh Taka
- CI
Confidence interval
- UK
United Kingdom
- CDC
Centers for Disease Control and Prevention
Authors’ contributions
The main author conceived and designed the paper; analyzed and interpreted the data; contributed materials, analysis tools, or data; and wrote the paper. All co-authors performed experiments, collected data, and help to analyze the data. The author(s) read and approved the final manuscript.
Funding
This study did not accept any grants from non-profit, public, or commercial sector funding bodies.
Availability of data and materials
The data that take facilitate the discovery from this research will be made available from the corresponding author on logical reason. The data is not available publicly due to limitations in containing information that may lead to the privacy of the study participants and that may cause problems at the workplace.
Declarations
Ethics approval and consent to participate
The motive and goals toward its benefits, risks, and procedure were explained in the research to the respondents easily. Information was accepted by every respondent by using the perceived native language. The researcher first introduced himself to the respondents. Then the researchers gave them the assurance the facts of the responders will be used just for the research purpose. The researchers tell them that their name will be a hidden secret. All kind of privacy is confirmed and any resections from the respondent are the first priority. They also told this information will only use for benefit of the Physiotherapy profession and the improve health with decreased hazards. All participants gave written informed consent before data collection began.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Md. Omar Sharif Ahmmed Chowdhury, Email: oschowdhury33@gmail.com.
Nurul Huda, Email: ptdrnurulhuda@gmail.com.
Md. Mohsin Alam, Email: drmohsinalam2011@gmail.com.
Sayed Imran Hossain, Email: sih.akash@gmail.com.
Shohal Hossain, Email: sohel6944@gmail.com.
Shahana Islam, Email: dr.shahanaislam17@gmail.com.
Most. Rumpa Khatun, Email: rumpaphysio3@gmail.com.
References
- 1.Putz-Anderson V, Bernard BP, Burt SE, et al. Musculoskeletal Disorders, and Workplace Factors. CDC, 1997; no. (NIOSH) 97–141. Available on: https://stacks.cdc.gov/view/cdc/21745.
- 2.Sintayehu DW, Giziew A, Awrajaw D, Getachew D. Work related risk factors and prevalence of low back pain among low wage workers. BMC Public Health. 2019;19:1072. doi: 10.1186/s12889-019-7430-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Palazzo C, Ravaud J-F, Papelard A, Ravaud P, et al. The burden of musculoskeletal conditions. PLoS One. 2014;9(3). [DOI] [PMC free article] [PubMed]
- 4.Walker BF. The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000;13(3):205–17. doi: 10.1097/00002517-200006000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Hoy D, Toole MJ, Morgan D, et al. Low back pain in rural Tibet. Lancet. 2003;361:225–226. doi: 10.1016/S0140-6736(03)12254-4. [DOI] [PubMed] [Google Scholar]
- 6.Davis KG, Heaney CA. The relationship between psychosocial work characteristics and LBP. Clin Biomech. 2000;15(6):389–406. doi: 10.1016/S0268-0033(99)00101-1. [DOI] [PubMed] [Google Scholar]
- 7.Tamrin SBM, Yokoyama K, Jalaludin J, et al. The associations between risk factors and low back painamong commercial vehicle drivers in Peninsular Malaysia. Ind Health. 2007;45(2):268–78. doi: 10.2486/indhealth.45.268. [DOI] [PubMed] [Google Scholar]
- 8.Miranda H, Viikari-Juntura E, Punnett L, Riihimaki H. Occupational loading, health behavior and sleep disturbance as predictor of low-back pain. Scand J Work Environ Health. 2008;34(6):411–9. doi: 10.5271/sjweh.1290. [DOI] [PubMed] [Google Scholar]
- 9.Lasrado OE, Mollerlokken OJ, Moen BE, Van den Bergh G. Musculoskeletal symptoms among hospital cleaners. Arch Environ Occup Health. 2017;72(2):87–92. doi: 10.1080/19338244.2016.1160862. [DOI] [PubMed] [Google Scholar]
- 10.Buchanan S, Vossenas P, Krause N, Moriarty J, Frumin E, Shimek JAM, et al. Occupational injury disparities in the US hotel industry. Am J Ind Med. 2010;53(2):116–25. doi: 10.1002/ajim.20724. [DOI] [PubMed] [Google Scholar]
- 11.David GC. Ergonomic methods for assessing exposure to risk factors for work-related musculoskeletal disorders. Occup Med (Lond) 2005;55(3):190–9. doi: 10.1093/occmed/kqi082. [DOI] [PubMed] [Google Scholar]
- 12.Rapoport J, Jacobs P, Bell NR, Klarenbach S. Refining the measurement of the economic burden of chronic diseases in Canada. Chronic Dis Can. 2004;25(1):13–21. [PubMed] [Google Scholar]
- 13.Punnett L, Pruss-Utun A, Nelson DI, Fingerhut MA, Leigh J, Tak S, et al. Estimating the global burden of low back pain attributable to combined occupational exposures. Am J Ind Med. 2005;48(6):459–69. doi: 10.1002/ajim.20232. [DOI] [PubMed] [Google Scholar]
- 14.Norlund AI , Waddell G. Cost of back pain in some OECD countries. Neck and Back Pain: the Scientific Evidences of Causes, Diagnosis, and Treatment. Philadelphia: Lippincott, Williams & Wilkins,2000; 421–425.1. Available on: https://cir.nii.ac.jp/crid/1130282268632940160.
- 15.Delleman N, Dul J. International standards on working postures and movements ISO 11226 and EN 1005–4. Ergonomics. 2007;50(11):1809–19. doi: 10.1080/00140130701674430. [DOI] [PubMed] [Google Scholar]
- 16.Gawde NC. A study of musculoskeletal pain among hotel employees, India. J Ecophysiol Occup Health. 2018;18(1–2):44–51. doi: 10.18311/jeoh/2018/20012. [DOI] [Google Scholar]
- 17.Vos T, Flaxman AD, Naghavi M, Lozano R, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2163–96. doi: 10.1016/S0140-6736(12)61729-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tsuboi H, Takeuchi K, Watanabe M, et al. Psychosocial factors related to low back pain among school personnel in Nagoya. Japan. Ind Health. 2002;40(3):266–71. doi: 10.2486/indhealth.40.266. [DOI] [PubMed] [Google Scholar]
- 19.Rahman MNA, Jaffar M. Musculoskeletal symptoms and ergonomic hazards among room attendants in hotel industries. Malays J Hum Factors Ergon. 2017;1(2):25–34. [Google Scholar]
- 20.Woods V, Buckle P. Musculoskeletal ill health amongst cleaners and recommendations for work organisational change. Int J Ind Ergon. 2006;36(1):61–72. doi: 10.1016/j.ergon.2005.08.001. [DOI] [Google Scholar]
- 21.Parmar S, Dalal P. A study of musculoskeletal disorder among housekeeping staff in hotel industry. Int J Home Sci. 2017;3(3):83–5. [Google Scholar]
- 22.De Zwart B, Frings-Dresen MH, Kilbom A. Gender differences in upper extremity musculoskeletal complaints in the working population. Int Arch Occup Environ Health. 2001;74(1):21–30. doi: 10.1007/s004200000188. [DOI] [PubMed] [Google Scholar]
- 23.Kristen Iker and Sara E. Luckhaupt. Low Back Pain among Workers: The Problem and What to Do About It. CDC. July 8, 2019. Available on: https://blogs.cdc.gov/niosh-science-blog/2019/07/08/lbp/.
- 24.Picchio M, Van Ours JC. Temporary jobs and the severity of workplace accidents. J Safety Res. 2017;61:41–51. doi: 10.1016/j.jsr.2017.02.004. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that take facilitate the discovery from this research will be made available from the corresponding author on logical reason. The data is not available publicly due to limitations in containing information that may lead to the privacy of the study participants and that may cause problems at the workplace.