

Abstract
Background Fentanyl provides systemic analgesia and enhances the sedative effect of benzodiazepines. When midazolam-only sedation is ineffective, fentanyl can be considered as an adjunct, but this advanced sedation technique requires additional training. Studies reporting on the safety and effectiveness of dentist-led conscious sedation using fentanyl and midazolam are lacking.
Aims To review the indication of use, safety and effectiveness of fentanyl and midazolam sedation at The Royal London Dental Hospital since its introduction into the service.
Method Retrospective data collection of sedation cases from October 2016 to October 2021 was carried out.
Results Of the 109 cases included, the majority of patients who had fentanyl (90.8%) had a history of unsuccessful sedation with midazolam. A lower average dose of midazolam was administered when fentanyl was used; the difference was statistically significant (p <0.0001). A higher proportion of patients who had fentanyl and midazolam presented with lower Ellis scores (better operating condition) compared to midazolam-only sedation. No adverse incidents were recorded.
Conclusion In this evaluation, the synergistic effects of fentanyl and midazolam resulted in enhanced sedation, anxiolysis and intraoperative conditions. This service evaluation showed some encouraging data regarding the potential safety profile and effectiveness of fentanyl in dental sedation when used by experienced clinicians; however, larger scale studies are required to validate this.
Key points
Adding fentanyl to midazolam sedation improved operating condition, especially in patients with a history of failed midazolam sedation.
Fentanyl reduced the average dose of midazolam required to achieve the sedation endpoint.
The fentanyl-midazolam sedation technique showed low adverse events when carried out by trained personnel in a sedation-compliant environment; however, further larger scale studies are required to validate its safety profile.
Introduction
Intravenous conscious sedation is a commonly used pharmacological method of anxiety control in dentistry and various drugs have been developed and utilised over the years. Fentanyl is a synthetic opioid analgesic that is similar to morphine but is 50-100 times more potent. It is a prescription-only medicine and regarded as a Schedule 2 controlled drug under the Misuse of Drugs Act 1971 in the UK. Fentanyl is usually prescribed for peri-operative pain control and management of malignant and non-malignant chronic pain. It can be prescribed in different forms, such as self-adhesive transdermal skin patches; solution for injection intramuscularly, intrathecally or intravenously; buccal or sublingual tablets; transmucosal lozenges; and intranasal or sublingual spray. Fentanyl can be used alone or in combination with other drugs for induction, maintenance, and recovery from general or regional anaesthesia. For the induction of general anaesthesia or sedation, it is administered intravenously, either as a bolus dose or continuous infusion via an indwelling cannula.
In dentistry, adding fentanyl to midazolam has proven popular for patients undergoing surgical procedures, such as wisdom tooth removal and implant placement, to complement the use of local anaesthetic at the site of surgery. The benefits are potentially two-fold: to establish systemic analgesics before surgery and to enhance the effect of sedation for anxiolysis. Benzodiazepines and opioids are used for induction of anaesthesia and sedation across dental and medical specialties. The concomitant use of opioids with a benzodiazepine has been identified as a factor contributing to morbidity and mortality in sedation for gastrointestinal endoscopy,1,2 though this has never been studied and reported in dentistry. Using midazolam with fentanyl for conscious sedation in dentistry has been classed by The Intercollegiate Advisory Committee for Sedation in Dentistry (IACSD) as an advanced sedation technique which requires additional training. There is a lack of studies reporting on dentist-led conscious sedation using fentanyl and midazolam in adults in the UK and beyond, and most of the regulations governing the practice of sedation in dentistry have been based on expert opinion, mainly in the field of anaesthesiology.
Fentanyl and midazolam have different mechanisms of action (Table 1), but both have a rapid onset of action and are short-acting, which make them suitable for use in outpatient sedation settings. The effects of the drugs peak at around 30 minutes, which is ideal for surgical dental interventions. The administration dose of fentanyl in conscious sedation in dentistry is usually 50 micrograms irrespective of weight; however, this can be reduced in high-risk or older patients. Midazolam is subsequently titrated in increments to a clinical sedation endpoint while monitoring the patient's response.
Table 1.
Clinical pharmacokinetics of intravenous fentanyl and midazolam
| Category | Fentanyl | Midazolam |
|---|---|---|
| Drug group | Synthetic opioid (phenylpiperidine derivative) | Imidazobenzodiazepine derivative |
| Drug schedule | Schedule 2 | Schedule 3 |
| Mechanism of action | Mu (μ) opioid receptors | GABA receptors |
| Volume of distribution | 4 L/kg (3-8 L/kg) | 1-3.1 L/kg |
| Plasma protein binding | 80-85% | 96-98% |
| Distribution half-life | 1-18 minutes | 6-15 minutes |
| Elimination half-life | 3-8 hours | 1.5-2.5 hours |
| Onset of action | 1-2 minutes | 1.0-2.5 minutes |
| Duration of action | 0.5-1 hour | 1-6 hours |
| Therapeutic index* | 400 | 1,131 |
| Clearance | Renal: 574 ml/min | Renal: 300-500 ml/min |
| Metabolism | Hepatic | Hepatic |
| Metabolites | Norfentanyl, despropionylfentanyl, hydroxyfentanyl, hydroxynorfentanyl (pharmacologically inactive) |
1(alpha)-hydroxy-midazolam (pharmacological active) 4-hydroxymidazolam 1-hydroxymidazolam glucuronide 4-hydroxymidazolam glucuronide |
| Excretion |
Urine: 75% Faeces: 9% |
Urine: 90% Faeces: 2% |
| Reversal | Naloxone | Flumazenil |
|
Key: * = The ratio of median lethal dose to median effective dose. The larger the therapeutic index, the safer the drug is. | ||
Aims
The aim of this service evaluation was to review the use of fentanyl since its introduction into the service in 2016 as an advanced sedation technique when used with midazolam for conscious sedation in a dental outpatient setting.
The objectives of the service evaluation included:
To audit the indications for a multi-drug (fentanyl and midazolam) sedation technique in the dental outpatient setting
To compare the dose of midazolam use with and without fentanyl and to determine if fentanyl reduces the amount of midazolam required to achieve the sedation endpoint
To assess the effectiveness of fentanyl and midazolam sedation (Ellis and sedation scoring)
To determine the incidence of adverse events, including the need for reversal with naloxone or flumazenil.
Methodology
Retrospective data collection was carried out for all patient care episodes involving sedation with fentanyl and midazolam in the Special Care and Sedation Clinic at Bart's Health NHS Trust over a five-year period from October 2016 to October 2021. Data collected included: age at the time of sedation; sex; medical history; American Society of Anaesthesiologists (ASA) classification grade; indication for using fentanyl; dose of midazolam used with and without fentanyl; Ellis grading; sedation score; treatment carried out; complications; and need for reversal. The data were collected by a group of dentists involved in the practice of conscious sedation within the service. Any discrepancies were crosschecked with a consultant supervising the data collection (Fig. 1). Patients with incomplete documentation or missing vital records, such as Ellis grade and midazolam dose without fentanyl, were excluded from the evaluation.
Fig. 1.
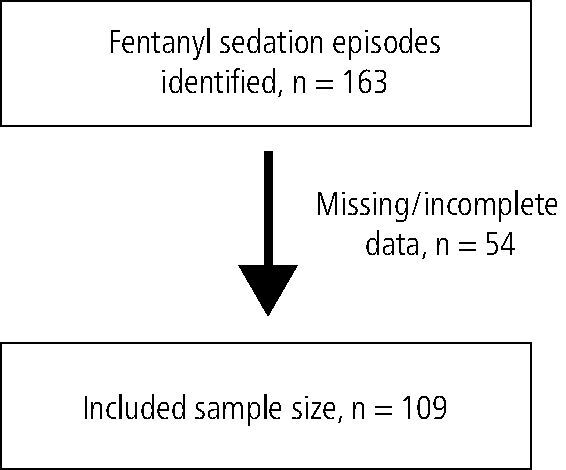
Data collection process
Sedation regimens were standardised across sedationists within the unit with a fentanyl-first protocol in accordance with the local Standard Operating Procedure. In total, 50 μg of fentanyl was given over three minutes, followed by titration of midazolam in the recommended way (2 mg bolus, followed by 1 mg titrated increments every 30 seconds while monitoring the patient) until the sedation endpoint was achieved (characterised by slurred speech, drooping eyelids and reduced anxiety level allowing treatment to commence). A slower and more cautious titration regimen was employed for older patients above 65 years old. Patients were not required to fast but had been advised they can have a light meal up to two hours before the appointment time.
Results
In total, 109 sedation episodes fulfilled the inclusion criteria for this service evaluation.
Demographic of patients
More than 75% of fentanyl-midazolam sedation cases were carried out on women (n = 86). This finding is similar to that of the 2009 UK Adult dental health survey,3 where women were more than twice as likely to report a dental phobia compared to men (16.8% versus 7%) (Fig. 2).
Fig. 2.
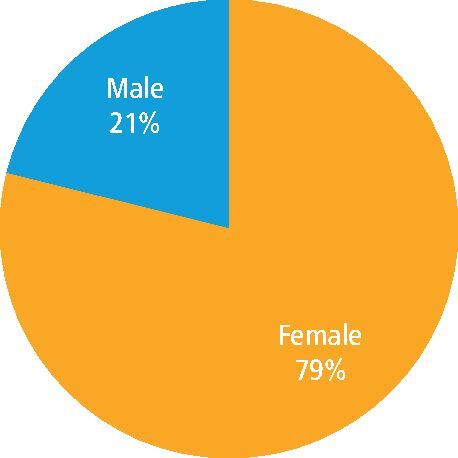
Sex distribution of patients (in %)
The mean age of patients seen was 31.7 years, with a range between 16-63 years.
Of the 109 sedation cases carried out, 25 cases were on patients with special care needs and 84 cases were on neurotypical patients with dental anxiety or phobia (Fig. 3).
Fig. 3.
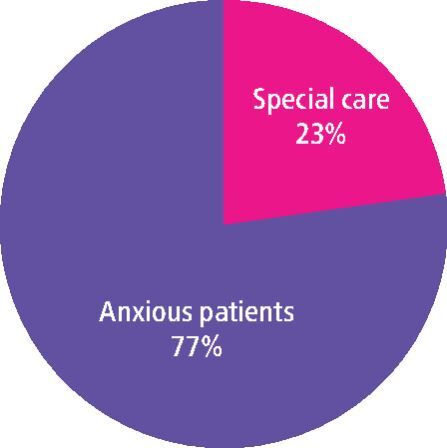
Patient mix of fentanyl-midazolam sedation cases
ASA classification grade
The majority of the patients were ASA grade I and II (91.7%). According to the IACSD recommendations4, only ASA grade I and II adults (>16 years of age) should be treated in primary care, but this service evaluation, which took place in a secondary care setting (with access to the resuscitation team and equipment), had included nine ASA grade III patients (Fig. 4).
Fig. 4.
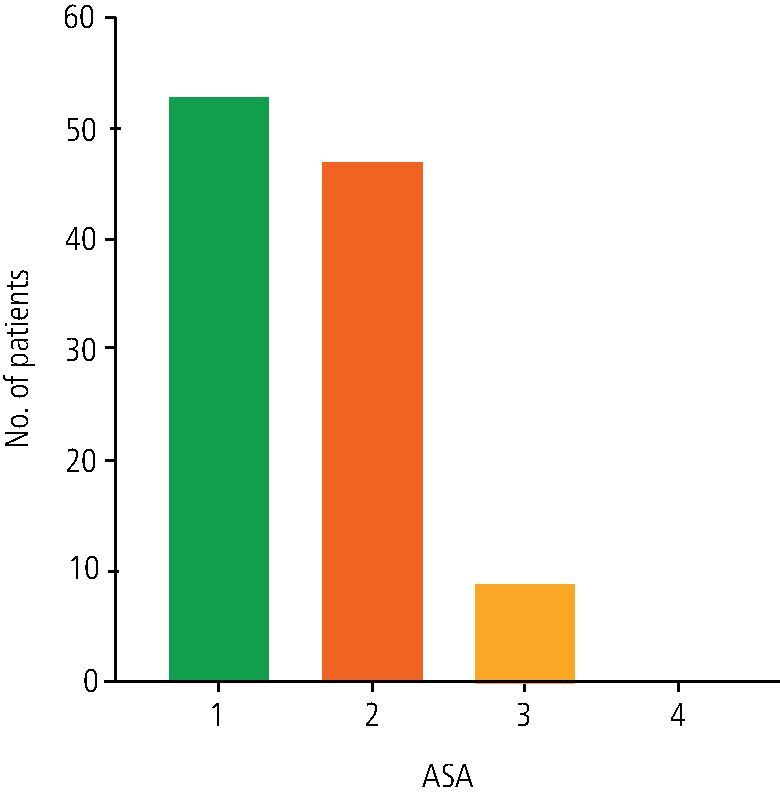
Physical health status (ASA grading) of patients
Indication for use
Most patients who had fentanyl (90.8%) had a history of unsuccessful sedation with midazolam (Table 2).
Table 2.
Indications recorded for fentanyl use
| Indication for fentanyl use | Number of sedation episodes |
|---|---|
| Previous failed sedation with midazolam at Royal London Hospital | 83 |
| Previous failed sedation elsewhere | 16 |
| Analgesia for implant surgery | 2 |
| To increase working time | 7 |
| Unknown reason/undocumented | 1 |
Comparison of effectiveness of fentanyl as a sedative adjunct
Sedative dose requirement
A lower average dose of midazolam was administered when fentanyl was used (Fig. 5) and the difference was statistically significant (t (108) = 9.609; p <0.0001) and clinically relevant. The difference in the average dose of midazolam use with and without fentanyl was 2.95 mg with a 95% confidence interval of 2.34-3.55.
Fig. 5.
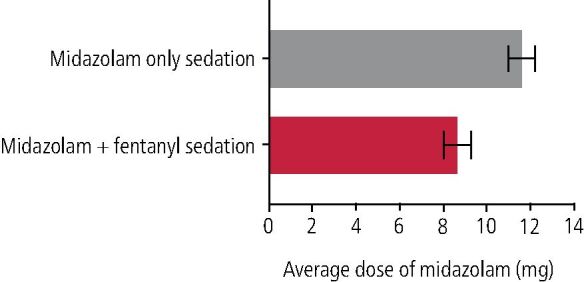
Comparison of average midazolam dose used (in mg) with and without fentanyl
Operating conditions
Better operating conditions for dental treatment were reflected in a lower documented Ellis grade5(Table 3). When fentanyl was not used, the majority of cases (92.7%) recorded an Ellis grade of III and above, whereas when fentanyl was used in addition to midazolam, cooperation improved, and 87% had an Ellis grade of I and II (Fig. 6).
Table 3.
Ellis grading5
| Ellis grade | Descriptions |
|---|---|
| I | No interference with treatment; total cooperation and no restlessness |
| II | Small amount of uninvited movement; still total cooperation and no restlessness |
| III | More uninvited movement; small degree of restlessness and anxiety. Patient less cooperative but still able to perform all dental procedures |
| IV | Considerable degree of limb movement; perhaps also unhelpful head movements; cooperation poor; patient quite restless and anxious; able to perform only basic dentistry |
| V | Restlessness, anxiety and limb movements severe; impossible to perform any dentistry |
Fig. 6.

Operating condition (Ellis grade) with and without fentanyl
Two out of 109 patients had an unsuccessful outcome with fentanyl and midazolam (Ellis score of V) and were subsequently placed on a general anaesthetic waiting list, though in both instances, limited examination and temporary dressings were managed, despite difficult operating conditions.
Sedation scores were extrapolated from the notes (Table 4). However, this was an under-reported measure, as sedation scoring was not part of the sedation note template and hence not widely documented.
Table 4.
Sedation scoring with and without fentanyl
| Sedation scoring | Definition | Midazolam without fentanyl | Midazolam with fentanyl |
|---|---|---|---|
| 1 | Fully awake and orientated | 51 | 2 |
| 2 | Drowsy | 28 | 43 |
| 3 | Eyes closed but responds promptly to verbal command | 8 | 39 |
| 4 | Eyes closed but rousable on mild physical stimulus | 0 | 7 |
| 5 | Eyes closed and unrousable on mild physical stimulus | 0 | 0 |
| Not recorded | 22 | 18 |
Complications
Vomiting
There was no incidence of vomiting reported and patients were not asked to starve pre-operatively.
Respiratory depression/desaturation
Nine out of 109 cases (8.2%) experienced desaturation (defined as the inability to maintain oxygen saturation at or above 90% despite efforts to stimulate the patient to take deep breaths) and required supplemental oxygen. However, none of these nine patients required reversal with flumazenil or naloxone due to over-sedation, as supplemental oxygen alone was sufficient.
Need for reversal
The incidence of reversal was one (0.9%) with flumazenil, and none with naloxone. It was an elective reversal to aid discharge in a special care patient with mobility issues and the use of flumazenil was justified and documented.
Discussion
Fentanyl and midazolam have a synergistic effect, where the combination of drugs results in an enhanced clinical sedative effect, greater anxiety relief and better intraoperative conditions, compared to when either drug is used on its own.6 This combination of drug regimen has been widely used to sedate patients undergoing various medical and surgical procedures, most commonly for gastroendoscopy, intubation in anaesthesiology/emergency medicine, spinal surgery and oral surgery.
This concomitant technique is recommended by the IACSD guidance for patients when midazolam alone does not produce adequate anxiolysis. The administration of fentanyl does not negate the use of sufficient local anaesthesia. It may, however, facilitate better cooperation with unpleasant sensations, such as pressure during extractions, and improve compliance with accepting local anaesthetic, as well as providing some post-operative pain relief.
This service evaluation revealed that 94.5% of patients who had failed sedation with benzodiazepine proceeded to have dental treatment completed successfully using fentanyl and midazolam sedation. The result of a 25.4% reduction in midazolam dose required following fentanyl administration is in agreement with Moore7 and Lobb8 studies, which demonstrated a statistically significant reduction in the amount of midazolam needed (36% and 29%, respectively) to titrate to a suitable endpoint for dental treatment using the fentanyl-first approach.7
There is evidence that opioid-first administration yields a substantial reduction in the amount of additional sedative needed to achieve similar degrees of moderate sedation, which was observed in this evaluation.7,9 The fentanyl-first approach is reported to reduce the clearance and prolong the duration of action of midazolam, likely as a result of competitive inhibition of CYP3A (cytochrome P4503A) activity.10 This could increase clinical treatment time but may require longer post-operative monitoring by an escort. Compared to single-drug techniques, there is increased unpredictability and a reduced margin of safety, potentially increasing the risk of adverse events.4 Although the risks of apnoea, chest wall rigidity and vocal cord closure11,12 associated with rapid administration of high doses of fentanyl is low in the dental setting due to the small doses used, the risk of respiratory depression associated with concomitant use of fentanyl with central nervous system depressants, such as benzodiazepines, is higher.13,14 The incidence of respiratory depression in this evaluation (8.2%) was slightly higher than Saiso's study,15 which reported six incidents of desaturation (5.6%); however, in the latter, patients received supplemental oxygen at 3 L/min immediately after establishment of intravenous access throughout the procedure, which could mask the incidence of respiratory depression. Furthermore, desaturation requiring intervention was defined as oxygen saturation of below 95%, which is higher than the standard 90% level in our service. Figures from studies focused on medical procedures using fentanyl and midazolam sedation show mortality rates of 1:2000 for upper gastrointestinal endoscopy and 1:1500 for colonoscopy,16 but the small data set in our evaluation limits any evaluation of the safety profile of combining fentanyl with midazolam for sedation in dentistry.
The incidence of vomiting with this technique is about 30% according to Craig and Boyle,17 hence fasting before sedation and antiemetics may be considered, though this was not seen in our service evaluation. If a decision is made to prescribe fentanyl with benzodiazepine, the lowest effective dose should be used, the duration of treatment should be as short as possible, and the patient's vital signs should be monitored closely throughout and after sedation.
There is also the risk of administrating the wrong drug during multi-drug sedation. To mitigate this, midazolam and fentanyl should be kept in separate trays away from each other with the syringes clearly labelled. Fentanyl is usually drawn up in a 1 ml syringe due to the small quantity required and midazolam in a 5 ml syringe (one way of distinguishing between the two drugs). The vial of the drug should also be crosschecked with a second person before drawing up to ensure the drugs are drawn up as intended and in-date. There was no reported complication of over-sedation or wrong drug administration in this evaluation.
The retrospective data collection relied on the record-keeping diligence of clinicians and missing/improbable data could not be followed-up. Most of the missing documentation in the excluded sample were of Ellis grade and midazolam dose without fentanyl - the reason being that previous unsuccessful midazolam-only sedation was carried out elsewhere and our service had no access to that information. Patients' self-reported outcome measures, such as patient satisfaction, anxiety and pain, were not investigated as part of this retrospective evaluation, hence it was not possible to compare patient perspectives of this technique compared to the midazolam-only technique. Patients were not considered the statistical unit of analysis, so the possible clustering effect for repeated sedation episodes of the same patients was not considered.
As the majority of patients in the sample were of ASA I and II (91.7%), the patient demographic within the evaluation could be representative of the primary dental care patient population in general. Older and medically complex patients (ASA III and above) should be approached with caution in a specialist centre and this group is rarely considered for multi-drug sedation within our service.
Regulation
Fentanyl-midazolam conscious sedation is considered an advanced technique. The IACSD guidance states that this opioid-midazolam combination is 'suitable for the operator-sedationist working in a primary care setting on condition that the dentist and second appropriate person have successfully completed recognised training programmes, have an appropriate level of experience, and that only ASA grade I and II adults (over 16 years of age) are treated'.4 In Wales, the Service standards for conscious sedation in a dental care setting18 advises that multi-drug techniques including the use of fentanyl should take place only within an acute or dental teaching hospital setting.
Recent NHS commissioning guide released in January 2023 states that primary care dental sedation services commissioned by the NHS only, are now advised to refer patients to a secondary care setting for advanced sedation techniques.19
Dentists, sedationists and nurses involved in the administration of this technique require additional theory and a minimum of 20 supervised cases to demonstrate competency for independent safe practice. This would be an extended competency developed by sedation practitioners who are trained and experienced in carrying out single-drug sedation using midazolam (documented experience of at least 100 cases over last two years).20
Similar to basic sedation techniques, team members involved in fentanyl and midazolam sedation must be trained in intermediate life support. Due to the mutual potentiation between opioids and benzodiazepines, the sedation team must be fully equipped to manage deep sedation and associated risks (respiratory depression/apnoea, airway obstruction, vomiting and prolonged recovery). Airway assessment is crucial to pre-empt ease of managing airway complications during sedation and availability of personnel with 'deployable' airway competencies (including basic airway manoeuvres, the use of airway adjuncts and the ability to administer positive pressure ventilation) is mandatory according to the IACSD and Resuscitation Council UK. Capnography may be useful in multi-drug sedation due to the increased risk of hypoxaemia and apnoea. Detection of early deterioration is especially important to help monitor respiratory status in patients with complex medical needs. When fentanyl is used, the reversal agent naloxone must be readily accessible, but for this multi-drug sedation technique, flumazenil should be used in the first instance to reverse the cardiorespiratory depressant effect of midazolam.
Conclusion
The fentanyl-midazolam multi-drug advanced sedation technique is a useful one to have in the armamentarium of sedation techniques offered when single-drug sedation has failed or where additional pain relief is deemed beneficial for surgical procedures. The COVID-19 pandemic exacerbated the pressures of access to general anaesthetic theatre lists, hence fentanyl use in this service evaluation could offer an alternative means for managing uncooperative patients. However, it is not without risk. The therapeutic benefits of adding fentanyl should therefore be weighed against the increased risks of cardiorespiratory depression and morbidity and should only be administered by those trained to do so. This service evaluation provided an encouraging snapshot of the potential safety profile and effectiveness of fentanyl in dental sedation; however, its small sample size undermines its internal and external validity. Further validation with larger-scale and longer-term studies in different settings across dentistry are necessary to provide the evidence base needed to support rigorous sedation regulations aimed at safeguarding sedation practice.
Acknowledgements
The authors would like to thank the dental core trainees who were involved in the data collection for this project (Lucinda Simpson, Balpreet Sambi, Chloe Bass).
Author contributions
Xin Hui Yeo: study design, data collection, data analysis, interpretation of results and manuscript preparation. Zahra Shehabi: study proposal and design, supervision of data collection, review of results and data analysis and manuscript preparation. The final manuscript was reviewed and finalised by both authors.
Ethics declaration
The authors declare no conflicts of interest.
Ethical approval was not required based on the Medical Research Council HRA toolkit: this is a retrospective service evaluation where the findings were not expected to be generalisable or comparable without a control group, the participants were not randomised and there was no change to usual clinical practice.
References
- 1.Arrowsmith J B, Gerstman B B, Fleischer D E, Benjamin S B. Results from the American Society for Gastrointestinal Endoscopy/U.S. Food and Drug Administration collaborative study on complication rates and drug use during gastrointestinal endoscopy. Gastrointest Endosc 1991; 37: 421-427. [DOI] [PubMed]
- 2.Daneshmend T K, Bell G D, Logan R F. Sedation for upper gastrointestinal endoscopy: results of a nationwide survey. Gut 1991; 32: 12-15. [DOI] [PMC free article] [PubMed]
- 3.NHS Digital. Adult Dental Health Survey 2009. 2011. Available at https://digital.nhs.uk/data-and-information/publications/statistical/adult-dental-health-survey/adult-dental-health-survey-2009-summary-report-and-thematic-series (accessed March 2022).
- 4.Royal College of Surgeons of England. Standards for Conscious Sedation in the Provision of Dental Care: Report of the Intercollegiate Advisory Committee for Sedation in Dentistry. 2015. Available at https://www.rcseng.ac.uk/dental-faculties/fds/publications-guidelines/standards-for-conscious-sedation-in-the-provision-of-dental-care-and-accreditation/ (accessed December 2021).
- 5.Ellis S. Response to intravenous midazolam sedation in general dental practice. Br Dent J 1996; 180: 417-420. [DOI] [PubMed]
- 6.Ben-Shlomo I, Abd-el-Khalim H, Ezry J, Zohar S, Tverskoy M. Midazolam acts synergistically with fentanyl for induction of anaesthesia. Br J Anaesth 1990; 64: 45-47. [DOI] [PubMed]
- 7.Moore P A, Finder R L, Jackson D L. Multidrug intravenous sedation: determinants of the sedative dose of midazolam. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997; 84: 5-10. [DOI] [PubMed]
- 8.Stander M, Wallis L A. Procedural sedation in the emergency centre. S Afr Med J 2011; 101: 195-201. [DOI] [PubMed]
- 9.Lobb D, Clarke A, Lai H. Administration order of midazolam/fentanyl for moderate dental sedation. J Dent Anesth Pain Med 2018; 18: 47-56. [DOI] [PMC free article] [PubMed]
- 10.Hase I, Oda Y, Tanaka K, Mizutani K, Nakamoto T, Asada A. IV fentanyl decreases the clearance of midazolam. Br J Anaesth 1997; 79: 740-743. [DOI] [PubMed]
- 11.Ouchi K. Intravenous sedation accompanied with fentanyl is effective for intramaxillary fixation in trauma patients. Glob Anesth Perioper Med 2016; DOI: 10.15761/GAPM.1000144.
- 12.Bennett J A, Abrams J T, Van Riper D F, Horrow J C. Difficult or impossible ventilation after sufentanil-induced anaesthesia is caused primarily by vocal cord closure. Anesthesiology 1997; 87: 1070-1074. [DOI] [PubMed]
- 13.Dionne R A, Yagiela J A, Moore P A, Gonty A, Zuniga J, Beirne O R. Comparing efficacy and safety of four intravenous sedation regimens in dental outpatients. J Am Dent Assoc 2001; 132: 740-751. [DOI] [PubMed]
- 14.Bailey P L, Pace N L, Ashburn M A, Moll J W, East K A, Stanley T H. Frequent hypoxaemia and apnea after sedation with midazolam and fentanyl. Anesthesiology 1990; 73: 826-830. [DOI] [PubMed]
- 15.Saiso K, Adnonla P, Munsil J, Apipan B, Rummasak D, Wongsirichat N. Complications associated with intravenous midazolam and fentanyl sedation in patients undergoing minor oral surgery. J Dent Anesth Pain Med 2017; 17: 199-204. [DOI] [PMC free article] [PubMed]
- 16.Lord D A, Bell G D, Grey A et al. Sedation for Gastrointestinal Endoscopic Procedures in the Elderly: Getting Safer but Still Not Nearly Safe Enough. Br Soc Gastroenterol 2006.
- 17.Craig D, Boyle C A. Practical Conscious Sedation. London: Quintessence Publishing, 2017.
- 18.Welsh Government. Service Standards for Conscious Sedation in a dental care setting. 2018. Available at https://www.gov.wales/sites/default/files/publications/2019-03/service-standards-for-conscious-sedation-in-a-dental-care-setting.pdf (accessed May 2023).
- 19.NHS England. Clinical guide for dental anxiety management. 2023. Available at: https://www.england.nhs.uk/long-read/clinical-guide-for-dental-anxiety-management/ (accessed May 2023)
- 20.Scottish Dental Clinical Effectiveness Programme. Conscious Sedation in Dentistry: Guidance Development Methodology. 2017. Available at https://www.sdcep.org.uk/media/oxtb4tut/sdcep-conscious-sedation-methodology.pdf (accessed December 2022).