
Figure 1.
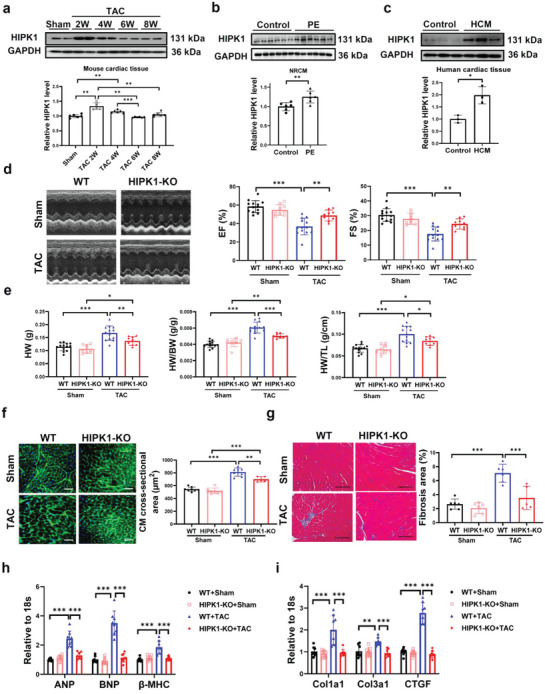
Genetic ablation of HIPK1 prevents TAC‐induced pathological cardiac hypertrophy. a) Western blot for HIPK1 in heart tissues from sham‐operated mice or mice at 2, 4, 6, and 8 weeks post TAC surgery (n = 6). b) Western blot for HIPK1 in NRCMs treated with PE or control vehicle (n = 6). c) Western blot for HIPK1 in human cardiac tissues from patients with hypertrophic cardiomyopathy and control samples (n = 3). d) Echocardiography for LV ejection fraction (EF) and fractional shortening (FS) at 8 weeks post TAC surgery (n = 13 for WT mice, n = 9 for HIPK1 KO mice). e) Heart weight (HW), heart weight/body weight (HW/BW) ratio, and heart weight/tibia length (HW/TL) ratio of mice (n = 9–13). f) Wheat germ agglutinin (WGA) staining for cardiomyocyte (CM) cross‐sectional area (n = 8,8,8,5). Scale bar = 50 µm. g) Masson staining for cardiac fibrosis area (n = 5–6). Scale bar = 100 µm. h,i) qRT‐PCR for h) ANP, BNP, and β‐MHC and i) Col1a1, Col3a1, and CTGF in mice heart tissues after sham or TAC surgery (n = 8). Data between two groups were compared by independent‐sample two‐tailed Student's t‐test. Data among four groups were compared by one‐way ANOVA test or two‐way ANOVA test followed by Tukey post hoc test. *, p < 0.05; **, p < 0.01; ***, p < 0.001.