

Abstract
Background Metachromatic leukodystrophy (MLD) is a lysosomal enzyme deficiency disorder leading to progressive demyelination and, consecutively, to cognitive and motor decline. Brain magnetic resonance imaging (MRI) can detect affected white matter as T2 hyperintense areas but cannot quantify the gradual microstructural process of demyelination more accurately. Our study aimed to investigate the value of routine MR diffusion tensor imaging in assessing disease progression.
Methods MR diffusion parameters (apparent diffusion coefficient [ADC] and fractional anisotropy [FA]) were in the frontal white matter, central region (CR), and posterior limb of the internal capsule in 111 MR datasets from a natural history study of 83 patients (age: 0.5–39.9 years; 35 late-infantile, 45 juvenile, 3 adult, with clinical diffusion sequences of different scanner manufacturers) as well as 120 controls. Results were correlated with clinical parameters reflecting motor and cognitive function.
Results ADC values increase and FA values decrease depending on disease stage/severity. They show region-specific correlations with clinical parameters of motor and cognitive symptoms, respectively. Higher ADC levels in CR at diagnosis predicted a disease course with more rapid motor deterioration in juvenile MLD patients. In highly organized tissues such as the corticospinal tract, in particular, diffusion MR parameters were highly sensitive to MLD-associated changes and did not correlate with the visual quantification of T2 hyperintensities.
Conclusion Our results show that diffusion MRI can deliver valuable, robust, clinically meaningful, and easily obtainable/accessible/available parameters in the assessment of prognosis and progression of MLD. Therefore, it provides additional quantifiable information to established methods such as T2 hyperintensity.
Keywords: metachromatic leukodystrophy, DTI, ADC, FA, diffusion
Introduction
Metachromatic leukodystrophy (MLD) is a lysosomal storage disorder and results in progressive sulfatide deposition in cells due to a deficiency of the sulfatide-degrading enzyme arylsulfatase A (ASA). The increasing sulfatide load causes cellular dysfunction and leads to progressive demyelination in the central and peripheral nervous system, with negative consequences for motor and cognitive skills of the patients. 1 2 As a reflection of demyelination, brain magnetic resonance imaging (MRI) shows confluent periventricular T2 hyperintensities, whose extension correlates to a certain extent with the clinical course. 3 Cognitive involvement has been shown to be primarily associated with T2 hyperintensities in the frontal white matter (FWM), while motor deficits are associated with signal abnormalities in the central region (CR). 4 5 Yet more detailed microstructural tissue changes might be revealed even in areas of normal-appearing white matter using newer MR sequences (including diffusion-weighted imaging [DWI], MR spectroscopy, magnetization transfer imaging, or myelin water imaging). 6 7 8 9 Furthermore, pseudonormalization of T2 hyperintensities may occur in the late stage of the late-infantile form, 6 so there is a discrepancy between the visual assessment of the extent of T2 signal changes and the clinical symptoms in early as well as late stages of the disease. Juvenile MLD, in particular, is characterized by a heterogeneous clinical course and T2 hyperintensities are observed already before clinical symptoms, 3 underlining the need for more quantifiable and more closely correlated MR parameters.
DWI allows assessing white matter microstructure by quantification of the molecular movement of water 10 and might therefore be well suited to detect even subtle changes in the degradation of white matter and, hence, in the clinical course of MLD. The parameters apparent diffusion coefficient (ADC) and fractional anisotropy (FA) have been investigated in several other demyelinating diseases 11 and are often acquired as part of routine clinical MRI exam. In MLD, changes in these values have already been demonstrated in affected patients. 6 8 12 13 14 However, their potential to reflect the clinical condition of the patient or their prognostic value remains to be elucidated.
To gain further insights, we performed this study with the following objectives:
Examine the extent to which DWI parameters ADC and FA reflect the clinical course in MLD patients with regard to motor (gross motor function measure) and cognitive (intelligence quotient [IQ] values) characteristics.
Evaluate ADC and FA as possible prognostic markers for the individual disease course.
Compare the performance of DWI parameters with the established MLD MR severity score, 15 which is based on quantification of T2 hyperintensities and brain atrophy. 16
We pursued these objectives using MR data from different MR scanners. In natural history studies of rare diseases, it is inherently very difficult to form larger monocentric patient cohorts that allow the identification of group effects such as clinical correlations with imaging parameters or prognostic statements. However, the DWI parameters ADC and FA in particular have been shown to be relatively robust and comparable between different field strengths and MR scanners in studies. 17 18
We chose a region of interest (ROI)–based evaluation in three different ROIs (FWM, CR, and posterior limb of the internal capsule [PLIC]) to capture changes in anatomically and functionally distinct areas that differ in thickness of their myelin sheaths and the presence of crossing or parallel fiber organization 19 and might therefore be differently affected by a primarily demyelinating pathology as MLD.
Methods
Patients
Clinical and MRI data of patients with MLD were collected within the German leukodystrophy network LEUKONET starting in 2006 and at the Amsterdam Leukodystrophy Center. 2 MLD was diagnosed as deficiency of ASA supported by an increase in urinary sulfatide level along with typical clinical features, often confirmed by genetic analysis.
The study cohort consisted of 83 MLD patients (median: 6.5 years; range: 0.5–39.9 years; 42 female). The patients were examined during the natural course of the disease with a total of 111 MRI scans. Thirty-five patients (42 scans, 19 female) were classified as late-infantile, 45 patients (66 scans, 20 female) as juvenile, and 3 patients (3 scans, 1 female) as adult MLD. The median time between onset of symptoms and date of scan was 4.4 years (range: 3.8–30.6 years).
To quantify the extent of MLD-associated diffusion changes compared with normal, we used a control group of 120 healthy children (range: 0.1–18.9 years; mean age: 8.0 years) with 188 MRI scans that originated from the National Institutes of Health (NIH)–funded Cincinnati MR Imaging of Neurodevelopment (C-MIND) study available at https://nda.nih.gov/edit_collection.html?id=2329 (dataset identifier DOI 10.15154/1528588). As the total patient cohort exceeded the upper age of the control cohort, an age-matched subcohort of 77 patients with a total of 100 MRI scans was extracted from the total cohort to meet the age range of the controls for analyses with direct comparisons. From this group, 35 patients (42 scans) were classified as late-infantile and 39 patients (55 scans) as juvenile MLD (median: 5.4 years; range: 0.5–18.3 years; 39 female).
Motor function was assessed via the Gross Motor Function Classification in MLD (GMFC-MLD) score 20 from 0 to 6 (0 = walking without support with quality of performance normal for age; 1 = walking without support but with reduced quality of performance; 2 = walking with support; 3 = Sitting without support and locomotion such as crawling or rolling; 4 = sitting without support but no locomotion or sitting without support not possible, but locomotion still possible; 5 = no locomotion nor sitting without support, head control is possible; 6 = no locomotion possible, loss of head control), which was documented for 99 datasets (0 = 25 patients; 1 = 27 patients; 2 = 8 patients; 3 = 7 patients; 4 = 7 patients; 5 = 6 patients; 6 = 19 patients; mean: 2.4). The IQ, which was collected using the Wechsler Intelligence Scale for Children (WISC), the Wechsler Adult Intelligence Scale (WAIS), and the Kaufmann Assessment Battery for Children (KABC II), was available for 21 scans (mean IQ: 77; range: 47–114).
Written informed consent was given by at least one caregiver. The study was approved by the local ethics committee (401/2005).
MRI Acquisition
The patients were examined on different 1.5T and 3T MR scanners. Seventy-six datasets were examined with a 1.5T scanner (Vision, Sonata, Avanto Fit, Aera, Espree, Symphony, Essenza from Siemens Healthineers; Signa from GE Healthcare; Titan from Toshiba; Achieva and Intera from Philips Healthcare) and 35 datasets with a 3T scanner (Skyra, Prisma fit, Trio, and Verio from Siemens Healthineers; Signa MR 750 from GE Healthcare). Data were collected at 38 different sites. The acquisition protocol included T1-weighted and axial T2-weighted sequences, which were used to precisely define the anatomical regions examined as described later and to derive the MLD MRI severity score. Due to the different sites and scanners, different DWI sequences were used. As ADC values correlate with the b -value applied, 21 22 23 only diffusion sequences with relatively low b-value ≤ 1,000 s/mm 2 (mean b -value in patients: 895 s/mm 2 ; range, 700–1,000 s/mm 2 ) were used to derive ADC values. Spatial resolution varied between the sequences (median slice thickness: 5 mm; range: 2–7.2 mm).
Controls were all scanned with the same diffusion sequence (3T MR scanner; b -value: 1,000 s/mm 2 ; voxel size: 2 × 2 × 2 mm).
Image Processing
DWI data were corrected for motion artifacts, eddy current, and echo planar imaging distortions (when b 0 -image with reversed phase-encoding direction was available) using FSL (version 5.0.9). 24 Maps of ADC and FA were calculated using the standard log-linear least squares fit of the tensor model. 25 All datasets underwent a visual quality check for motion artifacts or postprocessing issues.
The DWI data were then linearly coregistered with the anatomical sequences (T1 and T2/T2 fluid-attenuated inversion recovery [FLAIR]) using FSL (version 5.0.9) 26 27 to correctly target three defined ROIs in the DWI data in each left hemisphere based on the following anatomical landmarks (see also Fig. 1 ):
Fig. 1.
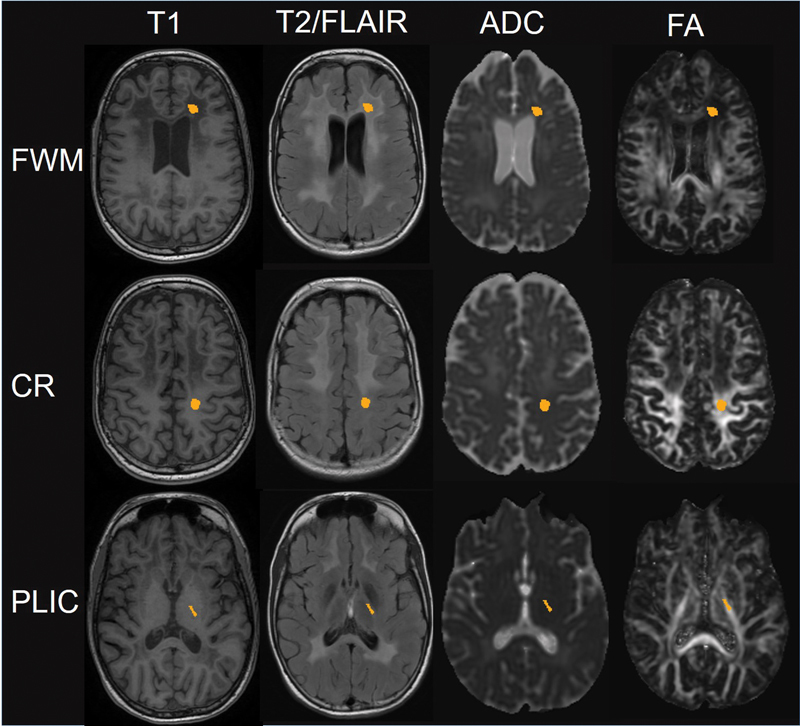
Exemplary illustration of the location of the regions of interest (ROIs) in the frontal white matter (FWM), the central region (CR), and the posterior limb of the internal capsule. Rows from left to right show the positioning of the ROIs in the anatomical images T1 and T2/FLAIR—these ROIs were transferred to co-registered DWI maps ADC and FA to derive the values within each ROI as mean of all marked voxels.
FWM, in the area of the deep white matter lateral to the anterior horn of the ventricles, sagittally at the level of the genu of the corpus callosum. The median volume of the ROI was 380 mm 3 (range: 168–808 mm 3 ). ADC values of FWM could be analyzed in all 111 and FA in 50 datasets.
CR, identified with the help of the central sulcus, the hand knob in the precentral gyrus, and the fissura longitudinalis cerebri. The median volume of the ROI was 364 mm 3 (range: 136–632 mm 3 ). ADC values of CR could be analyzed in all 111 and FA in 50 datasets.
PLIC, at the level of the third ventricle. The median size of this ROI was 125 mm 3 (range: 80–296 mm 3 ). In some patients, it was difficult delineating the PLIC due to atrophy; therefore, ADC values could be analyzed in this ROI in 100 and FA in 39 datasets.
Our ROI selection method was adopted from a previous study, 19 where it was applied in a group of healthy adolescents to examine microstructural differences in these ROIs. Variations arise in the number of voxels included, which were naturally less in younger children than in older ones. Labeling of each ROI was done on T1 anatomical images using MRtrix (version 0.3.12, www.github.com/MRtrix3/mrtrix3 28 ) to avoid selection bias, and is easy to perform even in infants. MRtrix was used likewise to calculate the mean ADC and FA values within the marked ROIs.
The MLD MR severity score 15 is a measure to quantify the extent of changes in conventional MR images in the course of MLD via a scoring system from 0 (no visible alterations) to 34 (maximum lesion load), taking into account T2 hyperintensities (graded as not visible = 0, faint = 1, and dense = 2) in different brain regions (among those, the central FWM, the central parieto-occipital white matter, and the PLIC) as well as atrophy. It was shown to correlate well with disease severity in MLD. 29 30 The total MLD MR severity score was determined for all patients to compare its correlation with motor and cognitive symptoms with the diffusion data performance in this cohort. Furthermore, we correlated ADC and FA values of the three ROIs with the corresponding regions of the MLD MR severity scores (ROI FWM with the central FWM, ROI CR with the central parieto-occipital white matter, and ROI PLIC with the PLIC) to evaluate to which extent the structural changes visible as T2 hyperintensities correlate with changes in diffusion measures.
Statistical Analysis
ADC and FA values were compared between healthy controls and MLD patients of the same age range for differences between groups (healthy controls, late-infantile patients, juvenile patients). Analysis of variance tests were performed with post hoc analysis using Tukey test to adjust for multiple comparisons.
ADC and FA values were correlated with clinical parameters (GMFC-MLD and IQ). Categorical parameters (GMFC-MLD) were analyzed using Spearman's rank correlation coefficient ( r s ), while for continuous variables (IQ) we applied Pearson's correlation coefficient ( r ).
ADC and FA values were used for prediction of disease course in juvenile patients. We retrospectively categorized the disease course of patients with a clinical follow-up of at least 2 years using the time interval between disease onset, that is, first clinical signs (whether motor or cognitive/behavioral), and entering GMFC-MLD level 2 (loss of independent walking). According to the median of progression in a large natural history cohort, 31 a rapidly progressive course was defined as reaching GMFC-MLD level 2 within less than 27 months after the onset of first symptoms (GMFC-MLD level 1), while a slowly progressive course was defined as a period of more than 27 months.
ADC and FA values were correlated with the MLD MR severity score and the amount of T2 hyperintensity (0–2) in ROI-correlating areas, using Spearman's rank correlation coefficient ( r s ).
In all tests, the significance level was defined as p < 0.05 and regarded as descriptive in this explorative analysis.
Results
ADC and FA Values of Healthy Control Subjects and MLD Patients over Age
Healthy controls showed higher values for FA and lower values for ADC with higher age, in accordance with the physiologically progressing myelination of the brain ( Fig. 2 ). ADC (FWM r = −0.64, CR r s = −0.61, PLIC r s = −0.36; each p < 0.001) and FA (FWM r = 0.41, p < 0.001; CR r = 0.62, p < 0.001; PLIC r = −0.22, p = 0.003) values correlated with age in every ROI.
Fig. 2.
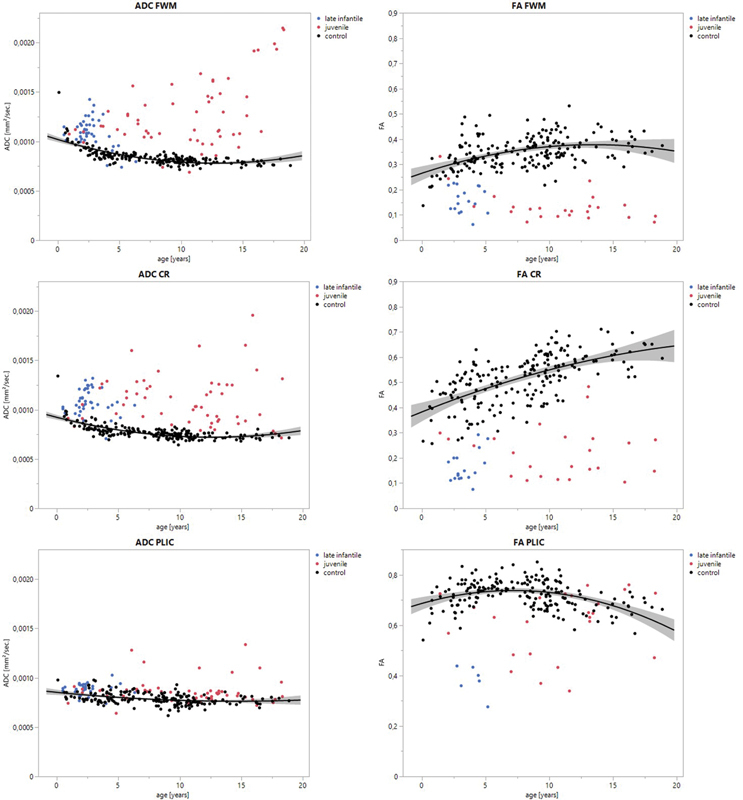
Correlation of ADC and FA values in three different regions of interest (FWM = frontal white matter, CR = central region, PLIC = posterior limb of the internal capsule) is shown in correlation to age at scan. Healthy controls ( black ) present with decreasing ADC and increasing FA values as an expression of the physiological myelination process during brain development. MLD patients either show an opposite development or their values are in a range that deviates significantly from the norm. The graphic shows the polynomial regression curve and confidence interval for controls.
For MLD patients, these age-related physiological changes in FA and ADC were either abolished or diminished ( Fig. 2 ). Instead, both ADC and FA values showed on average clearly abnormal values throughout the entire age range. On the group level, the age-matched MLD cohort differed significantly from healthy controls across all regions for ADC and FA ( p < 0.001). Late-infantile patients (age: 0–6.6 years) also differed from an age-matched control group (age: 0–6.6 years) in all ROIs as well as juvenile patients (age: 0–18.3 years) did for the total control group in every ROI for ADC and FA values ( p < 0.001). The group of late-infantile patients differed significantly from the juvenile group in the FWM for ADC values ( p = 0.01) and in the PLIC for ADC and FA values ( p = 0.02).
ADC and FA Correlated with Gross Motor Function
Across the cohort of 99 datasets with available GMFC-MLD score, there was a significant correlation of ADC and FA values in CR as well as PLIC with increasing motor impairment ( Fig. 3 ). ADC values had a positive correlation in the CR ( r s = 0.25, p = 0.014) as well as in the PLIC ( r s = 0.45, p < 0.001). FA values showed a negative correlation with increasing GMFC-MLD in the CR ( r s = −0.65, p < 0.001) as well as in the PLIC ( r s = −0.71, p < 0.001). For the FWM, there was no significant correlation with GMFC-MLD for either ADC or FA.
Fig. 3.
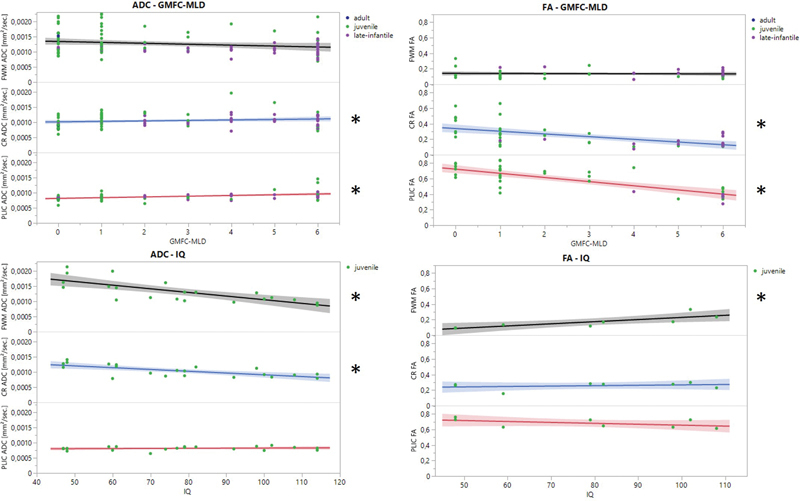
Motor symptoms are positively correlated with ADC along the corticospinal tract (CR, PLIC) and negatively correlated with FA in the respective regions. IQ showed a significant correlation with cortical ROIs (FWM, CR) for ADC and FWM only for FA. Significant correlations are indexed with an asterisk.
ADC and FA Correlated with IQ
Based on the available absolute IQ values for 21 juvenile scans, there was a significantly negative correlation of IQ value with ADC value in FWM ( r = −0.74, p < 0.001) and in CR ( r = −0.73, p < 0.001). For FA, FWM achieved a significantly positive correlation ( r = 0.81, p = 0.014). For the PLIC region, there was no significant correlation for either parameter, nor for FA in CR.
Prediction of Disease Progression in Juvenile MLD Patients Based on ADC
For 19 patients with juvenile MLD, MR scans were available at the time of diagnosis with no or only few motor symptoms (GMFC-MLD score of 0 or 1 at the time of MRI examination). For these patients, enough clinical follow-up information was available to divide them into patients with fast or slow disease progression. Five patients deteriorated from GMFC-MLD stage 1 to 2 within 27 months and thus were defined as “rapid disease progression,” while 14 patients were categorized as “slow disease progression.” As FA values at the time of diagnosis were only available from one patient with enough clinical follow-up information, the assessment was based solely on ADC values. The two groups of different disease progression did not differ with regard to age at MRI exam ( p > 0.7).
The fast and slow progression groups were found to differ significantly based on their ADC scores in CR at the time of diagnosis ( p < 0.014), with higher ADC values in the rapid progression group. The group values partially overlapped, but ADC values above 0.001 mm 2 /s in CR indicated a rapidly progressive course with an odds ratio of 14.4 ( p = 0.038; see Fig. 4 ).
Fig. 4.
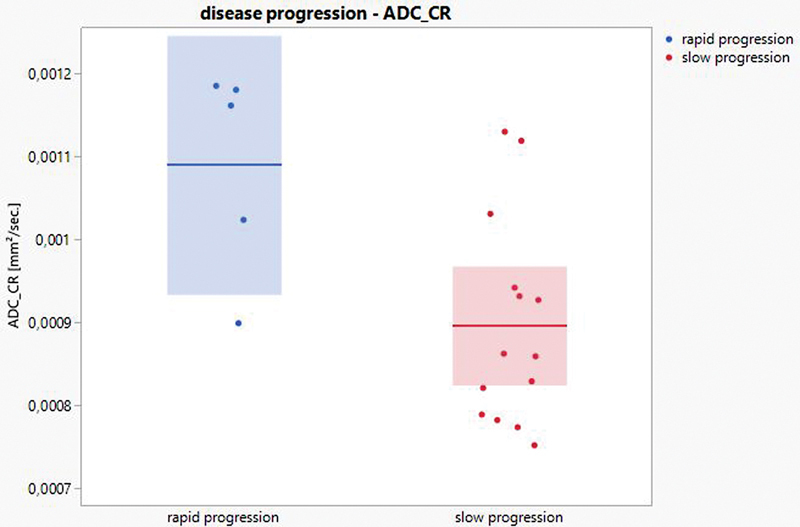
Disease progression with deterioration of motor symptoms from GMFC-MLD stage 1 to 2 in less (= rapid) or more (= slow) than 27 months was predicted with an odds ratio of 14.4 for values of ADC in the central region (CR) higher than 1.0*10e −3 mm 2 /s.
Correlation of ADC and FA with MLD MR Severity Subscores
The total MR severity score showed a significant correlation with GMFC-MLD ( r s = 0.21, p = 0.03) and IQ ( r = −0.8, p < 0.001).
T2 hyperintensity in the central FWM (corresponding to ROI FWM), the central parieto-occipital white matter (corresponding to ROI CR), and the PLIC (corresponding to ROI PLIC) showed no significant correlation to the GMFC-MLD score. Yet, for IQ, there was a significant negative correlation in each region (central FWM: r s = −0.63, p = 0.003; central parieto-occipital white matter: r = −0.52, p = 0.02; PLIC: r s = −0.52, p = 0.02). ADC and FA values in the FWM correlated significantly to their corresponding region of the MR severity score in the central FWM ( r s = 0.36 and r s = − 0.48, respectively; with each p < 0.001) and for ADC in CR with the subscore derived from the central parieto-occipital white matter ( r s = 0.3; p = 0.02), but not in CR for FA or PLIC for both parameters.
Discussion
In this study, we performed a multicenter study to investigate the clinical significance of the DWI parameters ADC and FA with respect to (1) their correlation with motor and cognitive impairment of late-infantile, juvenile and adult MLD patients, (2) their potential to give prognostic hints about the course of the disease, and (3) the performance of DWI parameters in comparison with the visual MLD MR severity score.
Healthy controls showed asymptotic changes in ADC and FA with age (except for FA in CR, where there is a maximum before the age of 10), reflecting progressing myelination and fiber organization during brain development in line with previous literature. 32 33 In contrast to this, the DWI parameters were significantly abnormal in all ROIs investigated (FWM, CR, PLIC) in patients with MLD, whereby the degree of organization seems to be related to the degree of deviation from the normal. Thus, the deviations in the FWM are clearly more pronounced than in the highly organized corticospinal tract in the PLIC. Patients with more severely impaired IQ show stronger changes in the FWM than less cognitively affected patients, while motor deterioration was associated with DWI changes especially in areas of the corticospinal tract in the CR and PLIC. In juvenile patients at the time of diagnosis, ADC values in the CR predicted an either slow or fast progression of motor symptoms in early stages of the disease, in that higher ADC values were associated with more rapid motor deterioration. ADC and FA showed a moderate correlation with the visually scored MLD MR severity score in the FWM, but not along the corticospinal tract. This indicates that T2 hyperintensities are not closely associated with microstructural changes and therefore each modality conveys different and possibly complementary information. The results are consistent with already published data available for DWI in children with MLD, 8 where a clinical correlation was yet missing.
From a histological perspective, the observed changes in DWI parameters might be explained by the histopathologically well-described process of demyelination and a reduction of fiber density and tissue organization. 34 35 It seems plausible to assume that, in the highly structured corticospinal tract, ADC and FA reflect changes in clinical symptoms more closely than methods only relying on T2 hyperintensities (such as the MLD MR severity score), and more than in the FWM where the degree of organization is not as high and crossing fibers influence FA values in particular. 19 36 Therefore, ADC and FA, having the advantage of giving quantitative information about gradual tissue changes, seem to provide additional information especially in areas with highly parallel fiber organization and may thus yield valuable information not only reflecting the current motor status, but also prognosis. Normal-appearing white matter in T2-weighted sequences may already show microstructural damage detectable by DWI, suggesting that the latter may be a more sensitive tool than assessing T2 signal alone. Further, more gradual changes or response to treatment could be captured more sensitively by the quantifiable ADC and FA values.
The MLD MR severity score was previously reported to correlate strongly with the IQ in 15 MLD patients ( r s = −0.87). 29 This result could be reproduced in our sample with a correlation of −0.8, which is in turn comparable to FA values in FWM with up to 0.81. The single subscore “central FWM” yielded significant correlations for IQ, yet to a lesser extent than the global score so that FA turned out to be superior on the single ROI level.
The correlation of GMFC-MLD with the MLD MR severity score showed a weaker correlation with r = 0.21, which was clearly inferior to the results of FA along the corticospinal tract (CR: r = −0.65; PLIC: r = −0.71).
Our results suggest that DWI parameters provide additional information above and beyond the T2 hyperintensities obtained by visual inspection. They can support the clinician in making decisions about therapy and counselling patients and their parents. The DWI parameters ADC and FA can be obtained by diffusion imaging using standard MRI protocols. Routine collection of DWI data, especially in the early course of the disease, is therefore possible and, in our opinion, recommended based upon the data presented. Radial diffusivity is another DWI parameter that needs to be considered for assessing pathological changes in MLD, as demyelination can be more specifically assessed using radial diffusivity—at least in inflammatory demyelinating disorders. 37 At the same time, this makes only sense in fiber populations with single fiber direction 38 39 and not in crossing fiber regions. Unfortunately, the only singe fiber population ROI in our data is in the PLIC, where we had less data. For future studies, the unique capability of DWI parameters to quantify microstructural tissue properties on a micrometer level should be used more broadly, potentially applying other advanced DWI parameters, such as radial diffusivity in tensor-based approaches, or even multishell parameters (such as fiber density or Neurite Orientation Dispersion and Density Imaging (NODDI) parameters, among others 6 19 ).
Naturally, there are several limitations to this study. Different centers were involved to recruit such a large number of patients affected by this rare disease. MR scanner type, field strength, and sequence parameters varied, and not all patients were examined with the full protocol including FA maps. Although this is a real-world scenario and has the advantage of making our results applicable to different MR scanners and sequences, it led to the limitation of increased data variation. It is therefore possible that these effects influence the results of this study; however, an increase in variation must only be expected to decrease sensitivity. Hence, our results must be seen to underestimate rather than overestimate the “true” differences. Further, the large differences in ADC and FA values between MLD patients and the healthy cohorts as well as the reproduced results for correlation with motor and cognitive symptoms in a subcohort (scanned at the same scanner with the same protocol; see Supplementary Material , available in the online version only) suggest that the effect of the pathology far exceeds that of scanner variability. In the available literature, ADC and FA are described as robust to different magnetic field strengths with mean concordance coefficients of 0.96 for FA and 0.86 for ADC or coefficient of variation ranging between 1 and 7.4% (mean: 2.6%), demonstrating that although the impact of different scanners is present, there is high concordance and robustness of ADC and FA across scanners. 17 18 Harmonization of DWI data of different sites and scanners by means of postprocessing algorithms 40 would likely reduce data variation, but would significantly limit the transferability of the results. Needless to say, it would be ideal to measure all controls and patients with the same imaging protocol in the same scanner, yet again this is challenging due to the low incidence of MLD. Based on the results obtained here, we consider it possible to use different DWI sequences and different MR scanners to investigate pathological changes in patients with rare diseases where the effect size of the pathology is as pronounced as in MLD.
Summary
In summary, the easily acquired DWI parameters ADC and FA can be used to derive relevant diagnostic and prognostic information on the clinical course of motor function and cognition in MLD. The microstructural damage elucidated in this way provides additional information above and beyond that obtained from classical T2 signal changes, underlining the added value of DWI values in quantifying disease progression in the brain in MLD.
Funding Statement
Funding The work was supported by an institutional research grant from Takeda Pharma AG (IIR-DEU-002540) and the German Research Foundation (GR 4688/2–1).
Conflict of Interest S.G. received institutional research support from Shire/Takeda, outside of the submitted work. He is an advisor and co-investigator for trials in Metachromatic Leukodystrophy (Shire/Takeda, Orchard, Bioclinica), but receives no personal payment related to this role. N.W. is advisor and/or co-investigator for trials in Metachromatic Leukodystrophy and other leukodystrophies (Shire/Takeda, Orchard, Ionis, PassageBio, Vigil Neuro), but receives no personal payment related to this role. P.M. has received honorary as an advisory board member from Biogen.
The other authors declare that they have no conflict of interest.
Note
S.G., I.K.-M., and N.W. are members of the ERN-RND, project ID 739510.
MRI data used in the preparation of this manuscript were obtained from the National Institute of Mental Health (NIMH) Data Archive (NDA). NDA is a collaborative informatics system created by the NIH to provide a national resource to support and accelerate research in mental health. Dataset identifier(s): DOI 10.15154/1528588. This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH or of the Submitters submitting original data to NDA.
Ethics Approval
The study was approved by the local ethics committees of the University of Tuebingen, Germany, and VU University Medical Center, Amsterdam, the Netherlands (401/2005 and 2018.300). Written informed consent was given by the parents of the patients or the patients themselves as appropriate.
Supplementary Material
References
- 1.Gieselmann V, Krägeloh-Mann I.Metachromatic leukodystrophy McGraw-Hill; 2014:chapter 148 [Google Scholar]
- 2.Kehrer C, Elgün S, Raabe C. Association of age at onset and first symptoms with disease progression in patients with metachromatic leukodystrophy. Neurology. 2021;96(02):e255–e266. doi: 10.1212/WNL.0000000000011047. [DOI] [PubMed] [Google Scholar]
- 3.Groeschel S, Kehrer C, Engel C. Metachromatic leukodystrophy: natural course of cerebral MRI changes in relation to clinical course. J Inherit Metab Dis. 2011;34(05):1095–1102. doi: 10.1007/s10545-011-9361-1. [DOI] [PubMed] [Google Scholar]
- 4.Groeschel S, Clas P. Cerebral gray and white matter changes and clinical course in metachromatic leukodystrophy. Neurology. 2012;79(16):1662–1670. doi: 10.1212/WNL.0b013e31826e9ad2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Strölin M, Krägeloh-Mann I, Kehrer C, Wilke M, Groeschel S. Demyelination load as predictor for disease progression in juvenile metachromatic leukodystrophy. Ann Clin Transl Neurol. 2017;4(06):403–410. doi: 10.1002/acn3.420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Martin P, Hagberg G E, Schultz T. T2-pseudonormalization and microstructural characterization in advanced stages of late-infantile metachromatic leukodystrophy. Clin Neuroradiol. 2021;31(04):969–980. doi: 10.1007/s00062-020-00975-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.van Rappard D F, Klauser A, Steenweg M E. Quantitative MR spectroscopic imaging in metachromatic leukodystrophy: value for prognosis and treatment. J Neurol Neurosurg Psychiatry. 2018;89(01):105–111. doi: 10.1136/jnnp-2017-316364. [DOI] [PubMed] [Google Scholar]
- 8.van Rappard D F, Königs M, Steenweg M E. Diffusion tensor imaging in metachromatic leukodystrophy. J Neurol. 2018;265(03):659–668. doi: 10.1007/s00415-018-8765-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Feldmann J, Martin P, Bender B. MR-spectroscopy in metachromatic leukodystrophy: a model free approach and clinical correlation. Neuroimage Clin. 2023;37:103296. doi: 10.1016/j.nicl.2022.103296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sullivan E V, Adalsteinsson E, Pfefferbaum A. Selective age-related degradation of anterior callosal fiber bundles quantified in vivo with fiber tracking. Cereb Cortex. 2006;16(07):1030–1039. doi: 10.1093/cercor/bhj045. [DOI] [PubMed] [Google Scholar]
- 11.Rueda-Lopes F C, Hygino da Cruz L C, Jr, Doring T M, Gasparetto E L. Diffusion-weighted imaging and demyelinating diseases: new aspects of an old advanced sequence. AJR Am J Roentgenol. 2014;202(01):W34-42. doi: 10.2214/AJR.13.11400. [DOI] [PubMed] [Google Scholar]
- 12.Singh P, Kaur R. Diffusion-weighted magnetic resonance imaging findings in a case of metachromatic leukodystrophy. J Pediatr Neurosci. 2016;11(02):131–133. doi: 10.4103/1817-1745.187640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Martin A, Sevin C, Lazarus C, Bellesme C, Aubourg P, Adamsbaum C. Toward a better understanding of brain lesions during metachromatic leukodystrophy evolution. AJNR Am J Neuroradiol. 2012;33(09):1731–1739. doi: 10.3174/ajnr.A3038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Patay Z. Diffusion-weighted MR imaging in leukodystrophies. Eur Radiol. 2005;15(11):2284–2303. doi: 10.1007/s00330-005-2846-2. [DOI] [PubMed] [Google Scholar]
- 15.Eichler F, Grodd W, Grant E. Metachromatic leukodystrophy: a scoring system for brain MR imaging observations. AJNR Am J Neuroradiol. 2009;30(10):1893–1897. doi: 10.3174/ajnr.A1739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Clas P, Groeschel S, Wilke M. A semi-automatic algorithm for determining the demyelination load in metachromatic leukodystrophy. Acad Radiol. 2012;19(01):26–34. doi: 10.1016/j.acra.2011.09.008. [DOI] [PubMed] [Google Scholar]
- 17.Grech-Sollars M, Hales P W, Miyazaki K. Multi-centre reproducibility of diffusion MRI parameters for clinical sequences in the brain. NMR Biomed. 2015;28(04):468–485. doi: 10.1002/nbm.3269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fox R J, Sakaie K, Lee J C. A validation study of multicenter diffusion tensor imaging: reliability of fractional anisotropy and diffusivity values. AJNR Am J Neuroradiol. 2012;33(04):695–700. doi: 10.3174/ajnr.A2844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Groeschel S, Hagberg G E, Schultz T. Assessing white matter microstructure in brain regions with different myelin architecture using MRI. PLoS One. 2016;11(11):e0167274. doi: 10.1371/journal.pone.0167274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kehrer C, Blumenstock G, Raabe C, Krägeloh-Mann I. Development and reliability of a classification system for gross motor function in children with metachromatic leucodystrophy. Dev Med Child Neurol. 2011;53(02):156–160. doi: 10.1111/j.1469-8749.2010.03821.x. [DOI] [PubMed] [Google Scholar]
- 21.DeLano M C, Cooper T G, Siebert J E, Potchen M J, Kuppusamy K. High-b-value diffusion-weighted MR imaging of adult brain: image contrast and apparent diffusion coefficient map features. AJNR Am J Neuroradiol. 2000;21(10):1830–1836. [PMC free article] [PubMed] [Google Scholar]
- 22.García Santos J M, Ordóñez C, Torres del Río S. ADC measurements at low and high b values: insight into normal brain structure with clinical DWI. Magn Reson Imaging. 2008;26(01):35–44. doi: 10.1016/j.mri.2007.04.004. [DOI] [PubMed] [Google Scholar]
- 23.Hui E S, Cheung M M, Chan K C, Wu E X. B-value dependence of DTI quantitation and sensitivity in detecting neural tissue changes. Neuroimage. 2010;49(03):2366–2374. doi: 10.1016/j.neuroimage.2009.10.022. [DOI] [PubMed] [Google Scholar]
- 24.Andersson J LR, Sotiropoulos S N. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage. 2016;125:1063–1078. doi: 10.1016/j.neuroimage.2015.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Basser P J, Mattiello J, LeBihan D. Estimation of the effective self-diffusion tensor from the NMR spin echo. J Magn Reson B. 1994;103(03):247–254. doi: 10.1006/jmrb.1994.1037. [DOI] [PubMed] [Google Scholar]
- 26.Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage. 2002;17(02):825–841. doi: 10.1016/s1053-8119(02)91132-8. [DOI] [PubMed] [Google Scholar]
- 27.Greve D N, Fischl B. Accurate and robust brain image alignment using boundary-based registration. Neuroimage. 2009;48(01):63–72. doi: 10.1016/j.neuroimage.2009.06.060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tournier J D, Calamante F, Connelly A. MRtrix: diffusion tractography in crossing fiber regions. Int J Imaging Syst Technol. 2012;22(01):53–66. [Google Scholar]
- 29.Tillema J M, Derks M G, Pouwels P J. Volumetric MRI data correlate to disease severity in metachromatic leukodystrophy. Ann Clin Transl Neurol. 2015;2(09):932–940. doi: 10.1002/acn3.232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schoenmakers D H, Beerepoot S, Krägeloh-Mann I. Recognizing early MRI signs (or their absence) is crucial in diagnosing metachromatic leukodystrophy. Ann Clin Transl Neurol. 2022;9(12):1999–2009. doi: 10.1002/acn3.51692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.GERMAN LEUKONET . Kehrer C, Blumenstock G, Gieselmann V, Krägeloh-Mann I. The natural course of gross motor deterioration in metachromatic leukodystrophy. Dev Med Child Neurol. 2011;53(09):850–855. doi: 10.1111/j.1469-8749.2011.04028.x. [DOI] [PubMed] [Google Scholar]
- 32.Reynolds J E, Grohs M N, Dewey D, Lebel C. Global and regional white matter development in early childhood. Neuroimage. 2019;196:49–58. doi: 10.1016/j.neuroimage.2019.04.004. [DOI] [PubMed] [Google Scholar]
- 33.Clayden J D, Jentschke S, Muñoz M. Normative development of white matter tracts: similarities and differences in relation to age, gender, and intelligence. Cereb Cortex. 2012;22(08):1738–1747. doi: 10.1093/cercor/bhr243. [DOI] [PubMed] [Google Scholar]
- 34.Aung W Y, Mar S, Benzinger T L. Diffusion tensor MRI as a biomarker in axonal and myelin damage. Imaging Med. 2013;5(05):427–440. doi: 10.2217/iim.13.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Suzuki K. London, UK: Hodder Arnold Publishers; 2007. Lysosomal diseases; pp. 515–599. [Google Scholar]
- 36.De Santis S, Drakesmith M, Bells S, Assaf Y, Jones D K. Why diffusion tensor MRI does well only some of the time: variance and covariance of white matter tissue microstructure attributes in the living human brain. Neuroimage. 2014;89(100):35–44. doi: 10.1016/j.neuroimage.2013.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Winklewski P J, Sabisz A, Naumczyk P, Jodzio K, Szurowska E, Szarmach A. Understanding the physiopathology behind axial and radial diffusivity changes-what do we know? Front Neurol. 2018;9:92. doi: 10.3389/fneur.2018.00092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Groeschel S, Tournier J D, Northam G B. Identification andbib interpretation of microstructural abnormalities in motor pathways in adolescents born preterm. Neuroimage. 2014;87:209–219. doi: 10.1016/j.neuroimage.2013.10.034. [DOI] [PubMed] [Google Scholar]
- 39.Wheeler-Kingshott C A, Cercignani M. About “axial” and “radial” diffusivities. Magn Reson Med. 2009;61(05):1255–1260. doi: 10.1002/mrm.21965. [DOI] [PubMed] [Google Scholar]
- 40.Mirzaalian H, de Pierrefeu A, Savadjiev P. Harmonizing diffusion MRI data across multiple sites and scanners. Med Image Comput Comput Assist Interv. 2015;9349:12–19. doi: 10.1007/978-3-319-24553-9_2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.