
Figure 2.
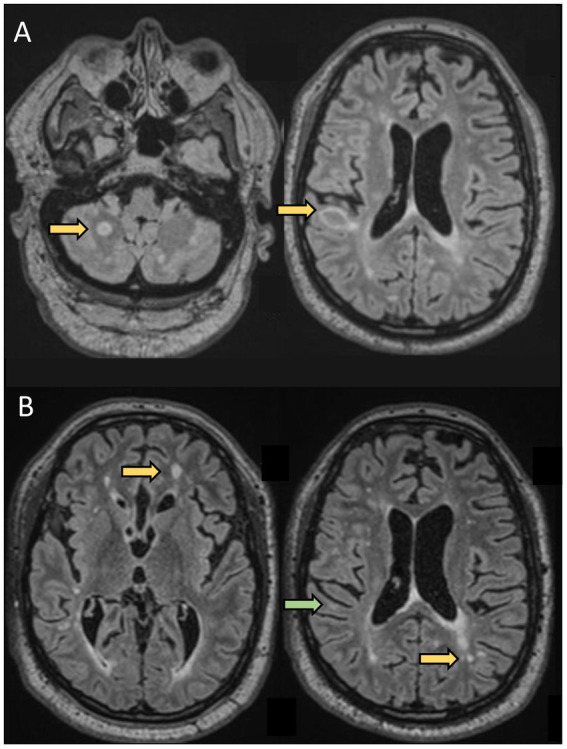
A 61-year-old man was evaluated for new neurological symptoms suggestive of a relapse. He was diagnosed with RRMS in 1998 after two episodes compatible with sub-acute sensory myelitis in 1994 and 1998. He did not receive any treatment for his MS between 1998 and 2019. Between 2000 and 2008, he had a couple of episodes suggestive of mild relapses. He had also noticed some progressively worsening gait instability and cognitive difficulties over the past few years, In April 2019 (at the age of 57), he experienced transient tingling followed by mild weakness and ataxia of the left upper extremity which resolved spontaneously over 5 weeks. Brain MRI showed 2 new lesions, one in the right juxtacortical posterior frontal lobe in the precentral gyrus explaining his symptoms. He was started on dimethyl fumarate 240 mg BID. He was doing well until August 2020 (at the age of 58 years), when he experienced tingling in the RUE associated with worsening cognitive difficulties. Repeat MRI showed 2 new lesions in the supratentorial regions. He was switched to oral cladribine without new clinical events or new radiological activity. This case highlights that although rare, some patients have continued disease activity despite an older age and longer disease duration.(A) Axial FLAIR sequences of brain MRI in April 2019 showing 2 new lesions (arrows) compared to prior MRI in 2017, and concomitant with a relapse (weakness and proprioceptive ataxia of the left upper extremity). (B) Axial FLAIR sequences of brain MRI in August 2020, 13 months after starting dimethyl fumarate, showing 2 new lesions (yellow arrows) compared to MRI in April 2019, with a decrease in size of the right posterior frontal lesion seen on prior MRI (green arrow) concomitant to a relapse: weakness of LUE and LLE.