
Figure 3.
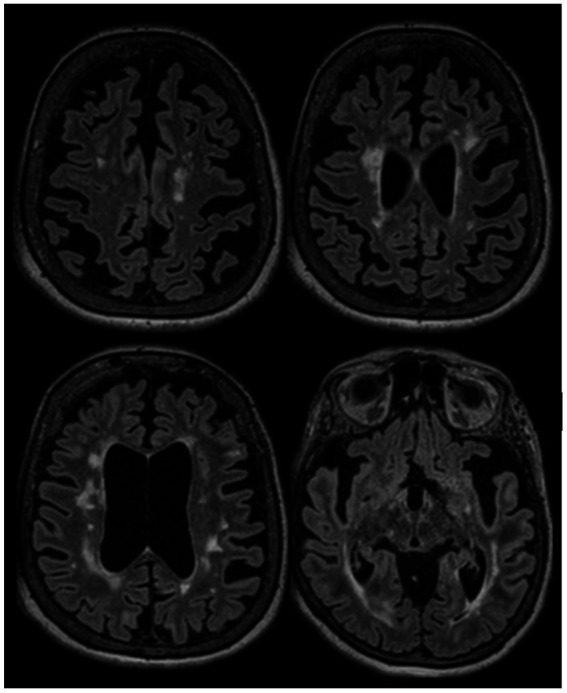
A 66-year-old woman was evaluated to establish care in our clinic. She was diagnosed with RRMS in 2002 after an episode compatible with sub-acute sensory myelitis. She was a participant in a Natalizumab trial, and was treated with this drug between 2003 and 2006. She experienced a relapse in 2007 after Natalizumab discontinuation, and was started on interferon beta1-a IM once a week between 2007 and 2015. She had a pseudo-relapse in 2014 in the context of acute illness. She did not report subacute symptoms since 2014, however she has noticed progressively worsening gait difficulties over the past few years, which she attributes to invalidating mechanical lower back pain related to severe spinal stenosis and degenerative disk disease. She continues to have flu-like symptoms after each interferon injection which last 12 to 24 hours. Her brain MRI in 2022 (at the age of 65) is stable compared to her MRIs between 2015 and 2019, except for a mild worsening of whole brain atrophy. After explaining the risks and benefits of treatment discontinuation, we decided to discontinue her interferon treatment. She has been clinically stable since. This case highlights that treatment discontinuation is a reasonable option in older patients with long standing disease duration and no clinical/radiological activity. Axial FLAIR sequences of brain MRI in July 2022 showing extensive lesions in the supratentorial regions which were stable in number and size compared to prior MRI in 2017, associated with diffuse brain atrophy.