
Figure 2. ALK aberrations are common in congenital and pediatric GBMs.
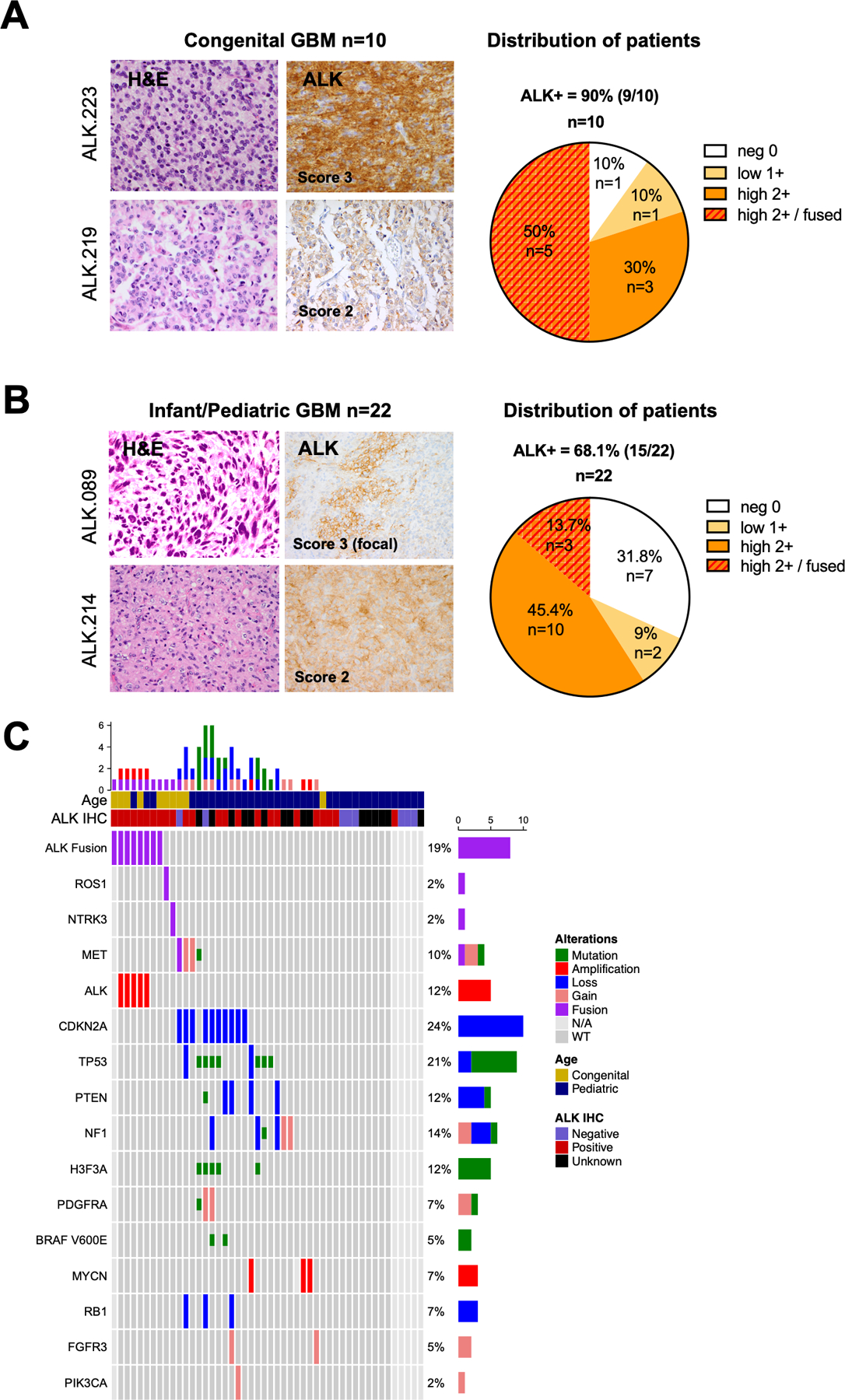
A. H&E staining showing glioma features. ALK immunohistochemistry (IHC) showing typical 3+ (left top) and 2+ (left bottom) staining appearance; pie chart demonstrating the distribution of ALK IHC scores in the congenital GBM cohort (n = 10). See methods for detail scoring schema.
B. H&E staining and ALK IHC of two illustrative pediatric GBMs scored as focally IHC 3+ (left top) and 2+ (left bottom); pie chart demonstrating the distribution of ALK IHC scores in the infant/pediatric GBM cohort (n = 22).
C. Oncoprint of sequenced GBMs illustrating ALK fusion/amplification is the sole candidate driver alteration in pediatric GBMs. The second lane showed the ALK-positive samples by IHC. Genomic aberrations including fusions (red), focal amplifications (>log 2.0, >10Mb), deletions or mutations (green). The tumors ALK.219, ALK.227 and ALK.228 harbored NTRK3, MET and ROS1 fusions respectively but were negative for ALK fusion.