
Figure 2:
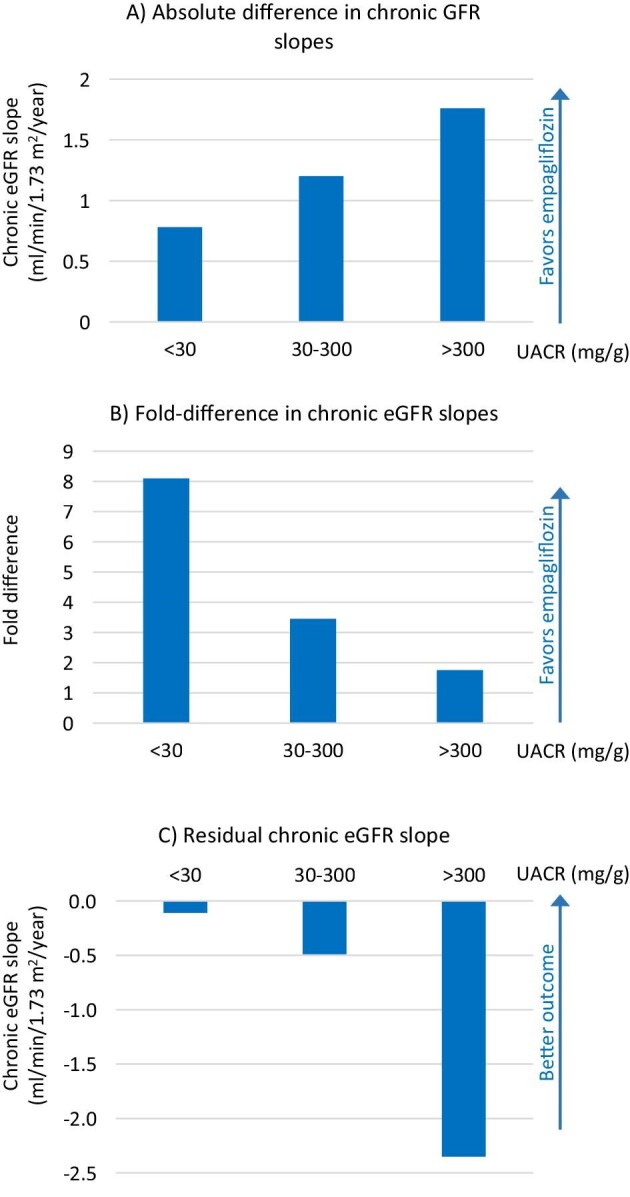
Chronic eGFR slopes according to baseline UACR category in EMPA-KIDNEY. (A) Absolute difference in chronic GFR slopes for albuminuria categories A1, A2 and A3 between the placebo and empagliflozin arms. Note that the largest difference is observed for participants with UACR >300 mg/g, i.e. in absolute terms, these participants obtained the largest preservation of chronic eGFR slope on empagliflozin vs placebo. (B) Fold-difference in chronic eGFR slopes for albuminuria categories A1, A2 and A3 between the placebo and empagliflozin arms. Note that in relative terms, the largest improvement in chronic eGFR slopes was observed for participants with UACR <30 mg/g. (C) On-treatment chronic eGFR slope. Note that the best outcome (i.e. the slowest eGFR slope) was observed in participants randomized to empagliflozin that had UACR <30 mg/g. These figures were generated using data from [9].