
Figure 1. Clinical Manifestations of Disabling Pansclerotic Morphea (DPM).
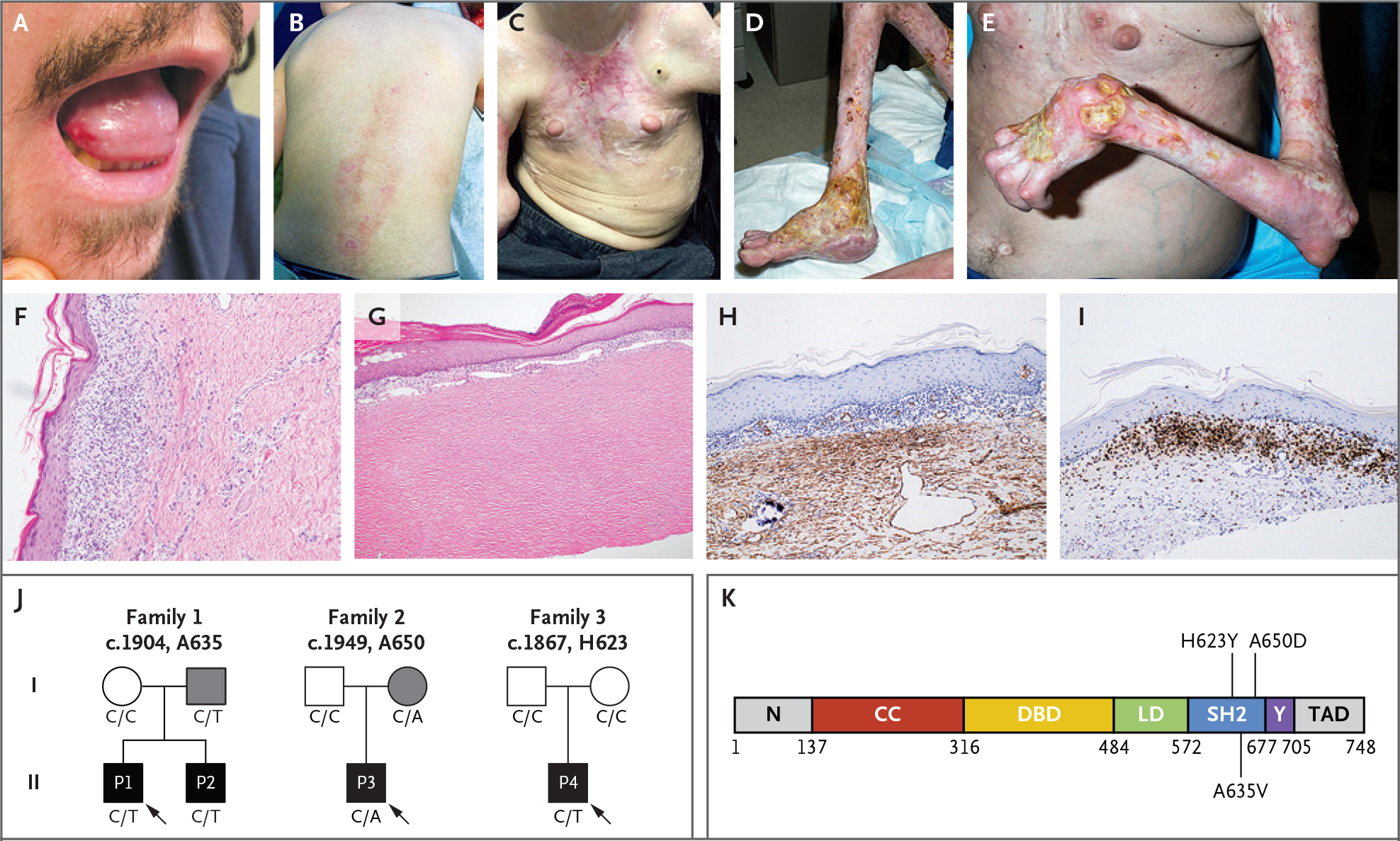
Clinical images show oral ulceration and limitation in tongue protrusion (Panel A); spreading waxy, hypopigmented lesions on the back and waxy hypopigmented “tank top” sign on the chest (Panels B and C); and ulcerations with articular ankylosis of the legs and arms (Panels D and E). Histologic sections of skin-biopsy samples show prominent inflammation (Panel F) and dermal thickening and hyalinization of morphea (Panel G). Images are shown of immunohistochemical staining for smooth-muscle action (Panel H) and CD3 (Panel I) in skin-biopsy samples before use of ruxolitinib. Family pedigrees (Panel J) are shown, with probands indicated by arrows. Circles represent female family members, squares male family members, and solid symbols persons who have received a diagnosis of DPM. Grey shading indicates persons with the STAT4 variants but with milder symptoms. The genotype at the specified locus is indicated under each person. A linear protein model (Panel K) shows the approximate locations of the identified variants in the SRC homology 2 (SH2) domain. CC denotes coiled-coil domain, DBD DNA-binding domain, LD linker domain, N the N-terminal domain, TAD transactivation domain, and Y the phosphotyrosyl-tail segment.