
Figure 5.
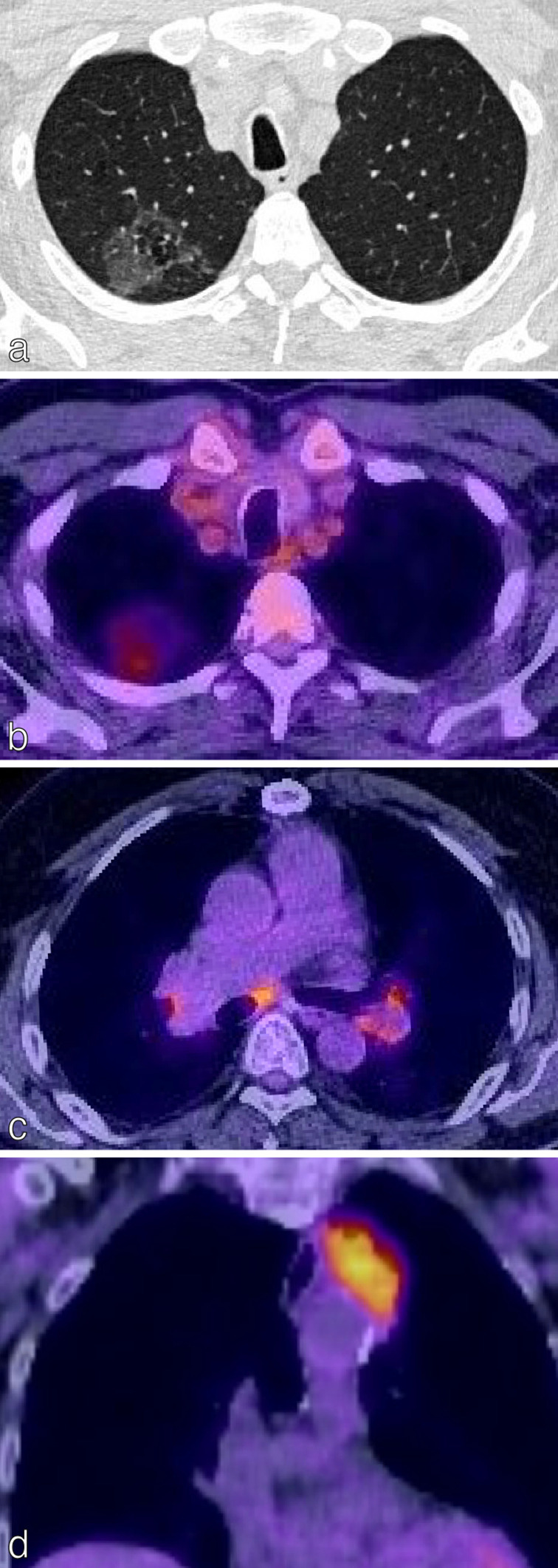
False negatives and false positives on 18F-FDG PET/CT. (a) Axial CT chest of a 72-year-old patient with confirmed adenocarcinoma in situ demonstrates a right upper lobe ground-glass opacity. (b) There was faint FDG uptake in the opacity (SUVmax less than the mediastinal blood pool); resulting in a low HERDER score. This is solely because of the ground-glass composition and emphasises the importance of interpreting FDG avidity carefully in each clinical context. (c) Axial 18F-FDG PET/CT in a patient with a T1c primary NSCLC demonstrates FDG-avidity in bilateral hilar lymph nodes and a subcarinal node; suspected N3 disease. EBUS confirmed granulomatous cells and no malignancy, thereby a false-positive study. (d) Coronal 18F-FDG PET/CT images of the thorax in an 88-year-old female presenting with trauma. The left upper lobe mass adjacent to the mediastinum is highly FDG-avid. CT-guided biopsy confirmed necrotising granulomatous disease with no malignant cells; thus a false positive. 18F-FDG PET, 18-fludeoxyglucose positron emission tomography; EBUS, endobronchial ultrasound; NSCLC, non-small cell lung cancer; SUVmax, maximum standardized uptake value.