

Abstract
Ventricular fibrillation (VF) is a cardiovascular disease that is one of the major causes of mortality worldwide, according to the World Health Organization. Heart rate variability (HRV) is a biomarker that is used for detecting and predicting life-threatening arrhythmias. Predicting the occurrence of VF in advance is important for saving patients from sudden death. We extracted features from seven HRV data lengths to predict the onset of VF before nine different forecast times and observed the prediction accuracies. By using only five features, an artificial neural network classifier was trained and validated based on 10-fold cross-validation. Maximum prediction accuracies of 88.18% and 88.64% were observed at HRV data lengths of 10 and 20 s, respectively, at a forecast time of 0 s. The worst prediction accuracy was recorded at an HRV data length of 70 s and a forecast time of 80 s. Our results showed that features extracted from HRV signals near the VF onset could yield relatively high VF prediction accuracies.
1. Introduction
Cardiovascular disease (CVD) is the leading cause of death in many developed countries [1] and accounts for an estimated 31% of all global deaths according to the World Health Organization, making it the primary cause of mortality worldwide. CVD includes abnormal heart rhythms, called ventricular tachyarrhythmias (VTAs), which comprise ventricular fibrillation (VF) and ventricular tachycardia (VT). VTA is one of the factors causing a fast heart rate and mortality in the absence of immediate medical treatment [2]. Therefore, early prediction of VTA is important to save patients from sudden death. The development of early preventive interventions could reduce the risk of an imminent VTA event.
Heart rate variability (HRV) indices have been used as noninvasive biomarkers to predict life-threatening VTAs such as VF [3]. These indices provide features useful for distinguishing arrhythmia from normal HRV [4]. HRV signifies the time variation of the R-peaks between two successive QRS complexes. The maximum upward deflection of a normal QRS complex is the R-peak, and the duration between two consecutive R-peaks is called the RR interval [5]. Previous studies have analyzed HRV by quantifying its features using three analysis methods: time-domain, frequency-domain, and Poincare nonlinear analyses [2, 6, 7].
Several studies have used the above three HRV analysis methods to analyze short-term (~5 min) and ultra-short-term (<5 min) HRV data. Short-term analysis has been widely considered to be methodologically reliable for analyzing HRV data [8] and for extracting features to investigate the occurrence of VF. Joo et al. applied an artificial neural network (ANN) to predict VTAs (both VT and VF) 10 s before their occurrence, using short-term HRV data [6]. Recently, Lee et al. attempted to predict the occurrence of VT using HRV features extracted from short-term HRV data [2]. Although short-term HRV data showed promising performance in predicting VTAs, ultra-short-term HRV data were found to be adequate for personal health devices with limited performance and memory capacity [9]. Therefore, recent studies have focused on ultra-short-term HRV analysis for applications in ambulatory heart rate devices [9]. Ebrahimzadeh et al. used the time-frequency and Poincare nonlinear analyses to extract HRV features from ultra-short-term HRV data. They extracted features from different segments of the HRV signals at successive 1 min ultra-short-term HRV intervals (i.e., at the first, second, third, and fourth minute before the event). They used the multilayer perceptron and K-nearest neighbor algorithms to classify healthy subjects and patients with VTA [10]. Finally, they compared the accuracies for predicting the occurrence of VTA by employing various time-series forecasting models with a fixed data length (1 min).
Although several studies have attempted to use ultra-short-term HRV data, the optimal data length and forecast time period have yet to be determined. Therefore, in this study, multiple combinations of different HRV data lengths and forecast time periods were investigated to obtain the optimal HRV data and forecast time interval for our data set. The objective of this study was to investigate the optimal HRV data lengths and forecast time periods for VF prediction, by comparing the performance in VF prediction of various HRV data lengths and forecast time periods. We evaluated nine different forecast times (from 0 to 80 s at 10 s intervals) and seven different HRV data lengths (from 10 to 70 s at 10 s intervals). All combinations of different HRV data lengths and forecast time periods were assessed based on the prediction accuracies obtained using the ANN algorithm.
2. Materials and Methods
2.1. Database
We used the following databases from PhysioNet [11]: Creighton University VTA database (CUDB) [12], spontaneous VTA database (MVTDB) [13], normal data sets from the paroxysmal atrial fibrillation prediction challenge database (PAFDB) [14], and the Massachusetts Institute of Technology-Beth Israel Hospital normal sinus rhythm database (NSRDB) [11]. We selected 29 VF subjects from CUDB, 29 VF and 30 control subjects from MVTDB, and 30 control subjects from PAFDB and NSRDB (12 and 18 subjects, respectively), resulting in a total of 58 VF subjects and 60 control subjects. The sampling rates were 250 Hz for CUDB, 1000 Hz for MVTDB, and 128 Hz for the other two data sets.
2.2. Preprocessing
RR intervals were collected from the PhysioBank Automated Teller Machine, a web service that contains waveforms annotated by cardiologists, for the data used in this study. Figure 1 shows the procedure used to organize the data sets using different data lengths and forecast time periods. Based on the 150 s HRV signal before the occurrence of VF, we considered nine different forecast time periods ranging from 0 to 80 s at intervals of 10 s. Each forecast time contains seven different HRV data lengths from 10 to 70 s at intervals of 10 s, resulting in 63 combinations. The HRV data length represents the time period used for feature extraction, shown as a gray line in Figure 1. The forecast time is the time period before the VF onset (Figure 1).
Figure 1.
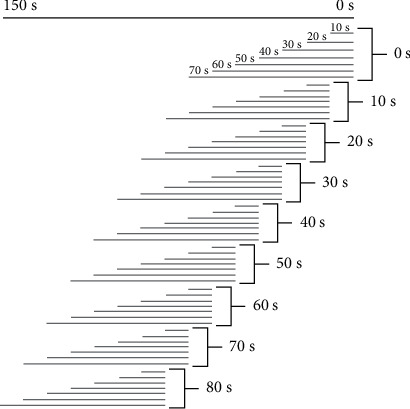
Representation of the seven data lengths from 10 s to 70 s in an interval of 10 s and nine forecast time periods from 0 s to 80 s in an interval of 10 s selected from the total period 150 s.
2.3. Feature Extraction
The features listed in Table 1 were calculated for each HRV data length denoted by the gray segments in Figure 1. These features consist of five HRV features (two features in the time-domain analysis and three features obtained using Poincare nonlinear analysis), which were extracted from each of the 58 VF and 60 control data sets. All HRV features were computed from successive RR intervals.
Table 1.
Features extracted from the HRV, the QRS complex singed area, and the R-peak amplitude.
| Component | Analysis | Feature | Unit | Description |
|---|---|---|---|---|
| HRV | Time-domain analysis | Mean NN | ms | Mean of normal R-peak to normal R-peak (NN) interval |
| RMSSD | ms | Square root of the mean squared differences of successive NN intervals | ||
| Poincare nonlinear analysis | SD1 | ms | Standard deviation of points perpendicular to the axis of the line of identity | |
| SD2 | ms | Standard deviation of points along the axis of the line of identity, | ||
| SD1/SD2 | Ratio of SD1 over SD2 |
2.3.1. Time-Domain Features
The time-domain features can be characterized by (1) the mean RR intervals (mean NN [RR]) and (2) the square root of the mean squared difference of the successive NN (RR) interval (RMSSD), which can be defined as follows:
| (1) |
| (2) |
2.3.2. Poincare Nonlinear Features
The features were a dispersion of the points perpendicular to and along the axis of the identity. Here, SD1, which represents the standard deviation of the points perpendicular to the axis of the line of identity, and SD2, which represents the standard deviation of the points along the axis of identity, were both calculated using Equations (3) and (4). The ratio of SD1 to SD2 was also calculated.
| (3) |
| (4) |
2.4. Proposed Methods
We implemented a fully connected ANN with three layers: an input layer containing input features to the network, a hidden layer capturing the nonlinearity of the data, and an output layer representing the dependent variable (Figure 2) [15, 16]. Rectified linear unit [17] activation functions were used in the input and hidden layers, and a sigmoid activation function [18] was used in the output layer. Through trial and error, six neurons were selected for the hidden layer. All features in the frequency-domain analysis and a few features in the time-domain analysis require a longer recording period to be considered reliable features [8]. Thus, we considered only five such features in this study. The input features were standardized and shuffled before they were used in the ANN. We used a 10-fold cross-validation to avoid overfitting of the classification. The data set was randomly divided into approximately 10 groups: 1 group was used as the testing data set and the remaining 9 groups were used as the training data set. The cross-validation was repeated 10 times to obtain unbiased prediction accuracy. Thus, the final prediction accuracies were determined by estimating the mean and standard deviation of the 10 × 10-fold cross-validation results.
Figure 2.
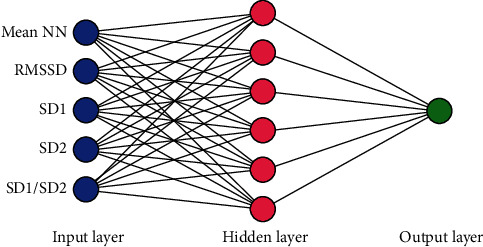
The architecture of our artificial neural network (ANN). The input features to the ANN are as follows: mean NN: mean normal R-peak to normal R-peak interval; SDNN: standard deviation of NN; RMSSD: square root of the mean squared difference of successive NN; pNN50: proportion of the interval differences of successive NN intervals greater than 50 ms; VLF: very low frequency; LF: low frequency; HF: high frequency; SD1: standard deviation of the points perpendicular to the axis of the line of identity; SD2: standard deviation of the points along the axis of identity.
3. Results
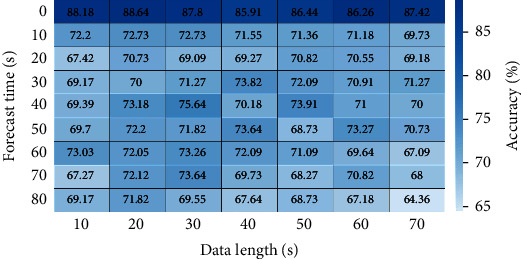
Figure 3 presents the prediction accuracies of all combinations of data length and forecast time. All data lengths with a 0 s forecast time have relatively higher prediction accuracies, indicating that the features extracted from the vicinity of VF onset could well distinguish VF from the control. Furthermore, maximum prediction accuracies of 88.18% and 88.64% were obtained with data lengths of 10 and 20 s, respectively, at a forecast time of 0 s, whereas a minimum prediction accuracy of 64.36% was obtained with a data length of 70 s at a forecast time of 80 s.
Figure 3.
Average accuracies obtained when using the same forecast times over different data lengths. The asterisk (∗) indicates a statistically significant difference between the corresponding groups.
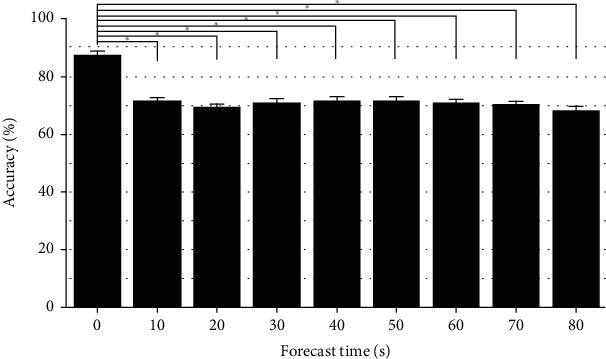
Figure 4 shows the mean prediction accuracies with their standard deviations in terms of the forecast time. The highest mean accuracy of 88.75% was obtained when using a 0 s forecast time, which was statistically higher than the accuracies of the other forecast times (analysis of variance [ANOVA] Tukey statistical test, F[8, 54] = 68.61, p < 0.001), whereas no significant difference was found between the mean prediction accuracies of the other forecast times (p > 0.05).
Figure 4.
Prediction accuracies of all combinations of the data length and forecast time (63 cases).
Figure 5 presents the mean prediction accuracies with their standard deviations in terms of the data length. The ANOVA Tukey statistical test yielded no statistical differences among the mean accuracies for different data lengths.
Figure 5.
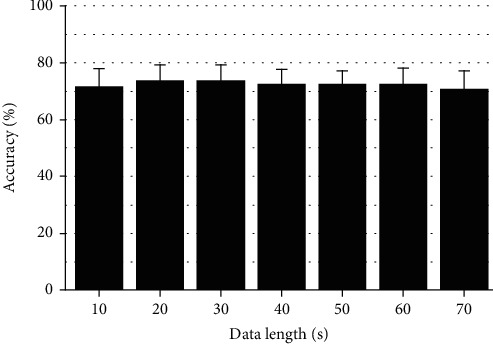
Average accuracies obtained when using the same data lengths over different forecast times.
4. Discussion
Advanced technologies have enabled the real-time monitoring of various health conditions by exchanging information between patients and common practitioners. These technologies have inherently low memory and capacity. Therefore, the application of ultra-short-term HRV is inevitably important to analyze HRV in appliances and devices with low memory and capacity [8]. Several studies have investigated ultra-short-term HRV recordings ranging from 10 s to 2 min to determine the reliability of the computed HRV parameters [8, 19]. Although ultra-short-term HRV data are not always reliable for analysis, previous studies have strongly suggested that researchers should consider statistical methods to compensate for the considerable measurement errors caused by the very short HRV segments [19]. Therefore, in this study, we investigated several combinations of data lengths and forecast time periods. Features were extracted from seven different HRV data lengths, each with nine different forecast times, to predict the occurrence of VF in 63 cases. We trained an ANN using these features, and high prediction accuracies were obtained using a forecast time of 0 s. However, the forecast time period of 80 s yielded low prediction accuracies, as shown in Figure 4. The overall results highlighted that features extracted from HRV signals near the VF onset have a higher probability of predicting the occurrence of VF.
We extracted five features using two analysis methods, namely, the time-domain and Poincare nonlinear analysis techniques. However, the frequency-domain features were not considered in this study, as their reliability depends on the length of the HRV signals they are extracted from. All features in the frequency-domain analysis and two features (SDNN and pNN50) in the time-domain analysis require a longer recording period to be considered reliable [8]. Thus, we considered only five features in this study, namely, mean NN, RMSSD, SD1, SD2, and SD1/SD2.
A limitation of this study was that only a few data sets (119 recordings in each case) were used to train our ANN. The ANN model must be trained using more data sets to achieve clinical validation. Further studies involving larger data sets should be conducted to investigate different clinical applications. Finally, the results of this study could be used with a patient's implantable cardiac defibrillator for real-time VF predictions, thus providing additional functionality for VF detection. Predicting the occurrence of VF hours in advance would be particularly useful; however, the data sets used in this study were limited to the 120 s data window and predicted VF 30 s before its occurrence.
5. Conclusions
In this study, we trained an ANN to predict VF using features extracted from 63 HRV segments with variable combinations of forecast time periods and data lengths. Subsequently, we determined the optimal data lengths to be 10 and 20 s with a forecast time period of 0 s, which were used to predict the occurrence of VF with relatively high prediction accuracies of 88.18% and 88.64%, respectively. This study could improve the prediction of imminent VF using very short HRV signals.
Acknowledgments
This research was partially supported by the National Research Foundation (NRF) of Korea under the basic engineering research project (2016R1D1A1B0101440) and the EDISON (NRF-2011-0020576) Programs and the Grand Information Technology Research Center Program through the Institute of Information & Communications Technology and Planning & Evaluation (IITP) funded by the Ministry of Science and ICT (MSIT), Korea (IITP-2021-2020-0-01612).
Data Availability
The method and result data used to support the findings of this study are included in the article.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Supplementary Materials
The supplementary materials for this article can be found here: Supplementary Table S1 and Table S2 show the summary of the ANN model according to the data length with 0 s of forecast time. Supplementary figures show the features that were used in this study, as the form of heat map graph.
References
- 1.Mathers C. D., Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Medicine . 2006;3(11):2011–2030. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lee H., Shin S. Y., Seo M., Nam G. B., Joo S. Prediction of ventricular tachycardia one hour before occurrence using artificial neural networks. Scientific Reports . 2016;6, article 32390 doi: 10.1038/srep32390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kleiger R. E., Miller J. P., Bigger J. T., Moss A. J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. The American Journal of Cardiology . 1987;59(4):256–262. doi: 10.1016/0002-9149(87)90795-8. [DOI] [PubMed] [Google Scholar]
- 4.Melillo P., Izzo R., Orrico A., et al. Automatic prediction of cardiovascular and cerebrovascular events using heart rate variability analysis. PLoS One . 2015;10(3):1–14. doi: 10.1371/journal.pone.0118504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Reed M. J., Robertson C. E., Addison P. S. Heart rate variability measurements and the prediction of ventricular arrhythmias. QJM: An International Journal of Medicine . 2005;98(2):87–95. doi: 10.1093/qjmed/hci018. [DOI] [PubMed] [Google Scholar]
- 6.Joo S., Choi K. J., Huh S. J. Prediction of spontaneous ventricular tachyarrhythmia by an artificial neural network using parameters gleaned from short-term heart rate variability. Expert Systems with Applications . 2012;39(3):3862–3866. doi: 10.1016/j.eswa.2011.09.097. [DOI] [Google Scholar]
- 7.Bilgin S., Çolak O. H., Polat O., Koklukaya E. Estimation and evaluation of sub-bands on LF and HF base-bands in HRV for ventricular tachyarrhythmia patients. Expert Systems with Applications . 2009;36(6):10078–10084. doi: 10.1016/j.eswa.2009.01.014. [DOI] [Google Scholar]
- 8.Nussinovitch U., Elishkevitz K. P., Katz K., et al. Reliability of ultra-short ECG indices for heart rate variability. Annals of Noninvasive Electrocardiology . 2011;16(2):117–122. doi: 10.1111/j.1542-474X.2011.00417.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Baek H. J., Cho C. H., Cho J., Woo J. M. Reliability of ultra-short-term analysis as a surrogate of standard 5-min analysis of heart rate variability. Telemedicine and e-Health . 2015;21(5):404–414. doi: 10.1089/tmj.2014.0104. [DOI] [PubMed] [Google Scholar]
- 10.Ebrahimzadeh E., Pooyan M., Bijar A. A novel approach to predict sudden cardiac death (SCD) using nonlinear and time-frequency analyses from HRV signals. PLoS One . 2014;9(2):1–14. doi: 10.1371/journal.pone.0081896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Goldberger A. L., Amaral L. A. N., Glass L., et al. PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation . 2000;101(23):e215–e220. doi: 10.1161/01.cir.101.23.e215. [DOI] [PubMed] [Google Scholar]
- 12.Nolle F. M., Badura F. K., Catlett J. M., Bowser R. W., Sketch M. H. CREI-GARD, a new concept in computerized arrhythmia monitoring systems. Computers in Cardiology . 1986;13:515–518. [Google Scholar]
- 13.Goldberger A., Amaral L., Glass L., et al. Spontaneous Ventricular Tachyarrhythmia Database, PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation [Online] . 2000;101(23) doi: 10.1161/01.cir.101.23.e215. [DOI] [PubMed] [Google Scholar]
- 14.Moody G., Goldberger A., McClenne S., Swiryn S. Predicting the onset of paroxysmal atrial fibrillation: the computers in cardiology challenge 2001. Computers in Cardiology . 2001;28:113–116. doi: 10.1109/cic.2001.977604. [DOI] [Google Scholar]
- 15.Basheer I. A., Hajmeer M. Artificial neural networks: fundamentals, computing, design, and application. Journal of Microbiological Methods . 2000;43(1):3–31. doi: 10.1016/S0167-7012(00)00201-3. [DOI] [PubMed] [Google Scholar]
- 16.Lippmann R. P. Pattern classification using neural networks. IEEE Communications Magazine . 1989;27(11):47–50. doi: 10.1109/35.41401. [DOI] [Google Scholar]
- 17.Xavier G., Antoine B., Yoshua B. Deep sparse rectifier neural networks. International Conference on Artificial Intelligence and statistics (AISTATS) . 2011;15:315–323. [Google Scholar]
- 18.Narayan S. The generalized sigmoid activation function: competitive supervised learning. Information Sciences . 1997;99(1–2):69–82. doi: 10.1016/S0020-0255(96)00200-9. [DOI] [Google Scholar]
- 19.Schroeder E. B., Whitsel E. A., Evans G. W., Prineas R. J., Chambless L. E., Heiss G. Repeatability of heart rate variability measures. Journal of Electrocardiology . 2004;37(3):163–172. doi: 10.1016/j.jelectrocard.2004.04.004. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The supplementary materials for this article can be found here: Supplementary Table S1 and Table S2 show the summary of the ANN model according to the data length with 0 s of forecast time. Supplementary figures show the features that were used in this study, as the form of heat map graph.
Data Availability Statement
The method and result data used to support the findings of this study are included in the article.