
Fig. 1 .
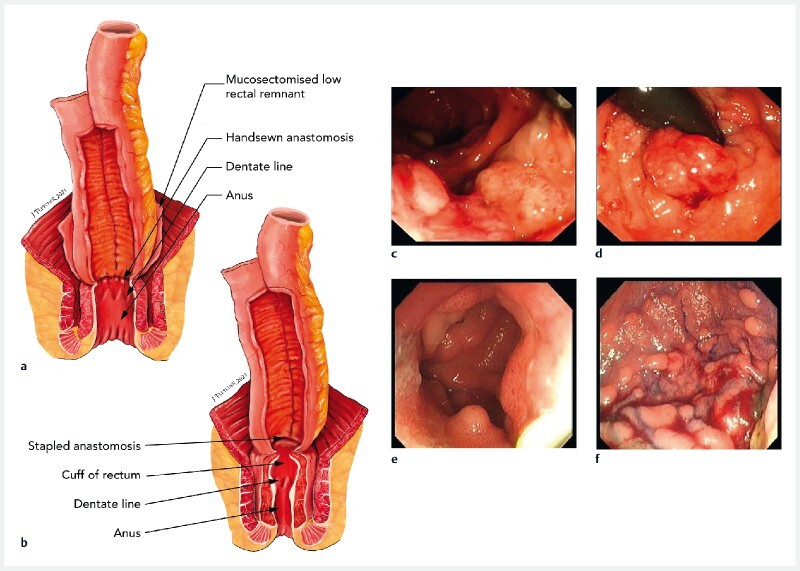
Types of anastomoses used and the adenomas that develop in pouches in familial adenomatous polyposis. a, b Illustrations of the anastomoses showing: a a handsewn anastomosis, in which there remains a hidden risk of adenoma development from residual rectal cuff mucosal islands – the ileal pouch has been advanced into a 2-cm rectal cuff following mucosectomy, and is handsewn at the dentate line, meaning islands of mucosal cells can remain behind that may develop into adenomas that cannot be visualized on direct endoscopy, and therefore require expert digital examination; b a stapled anastomosis, in which ~1–2 cm of rectal cuff remains in-situ and is proximally stapled to the ileoanal pouch with a circular stapling device, with this technique enabling direct visualization of any adenomas at pouchoscopy. c–f Endoscopic images of example pouch adenomas showing: c cancer in a cuff; d high grade dysplasia in a cuff lesion visualized on retroflexion; e adenomas in the pouch body; f diffuse polyposis within the pouch body.