
Figure 7. ISHLT scores.
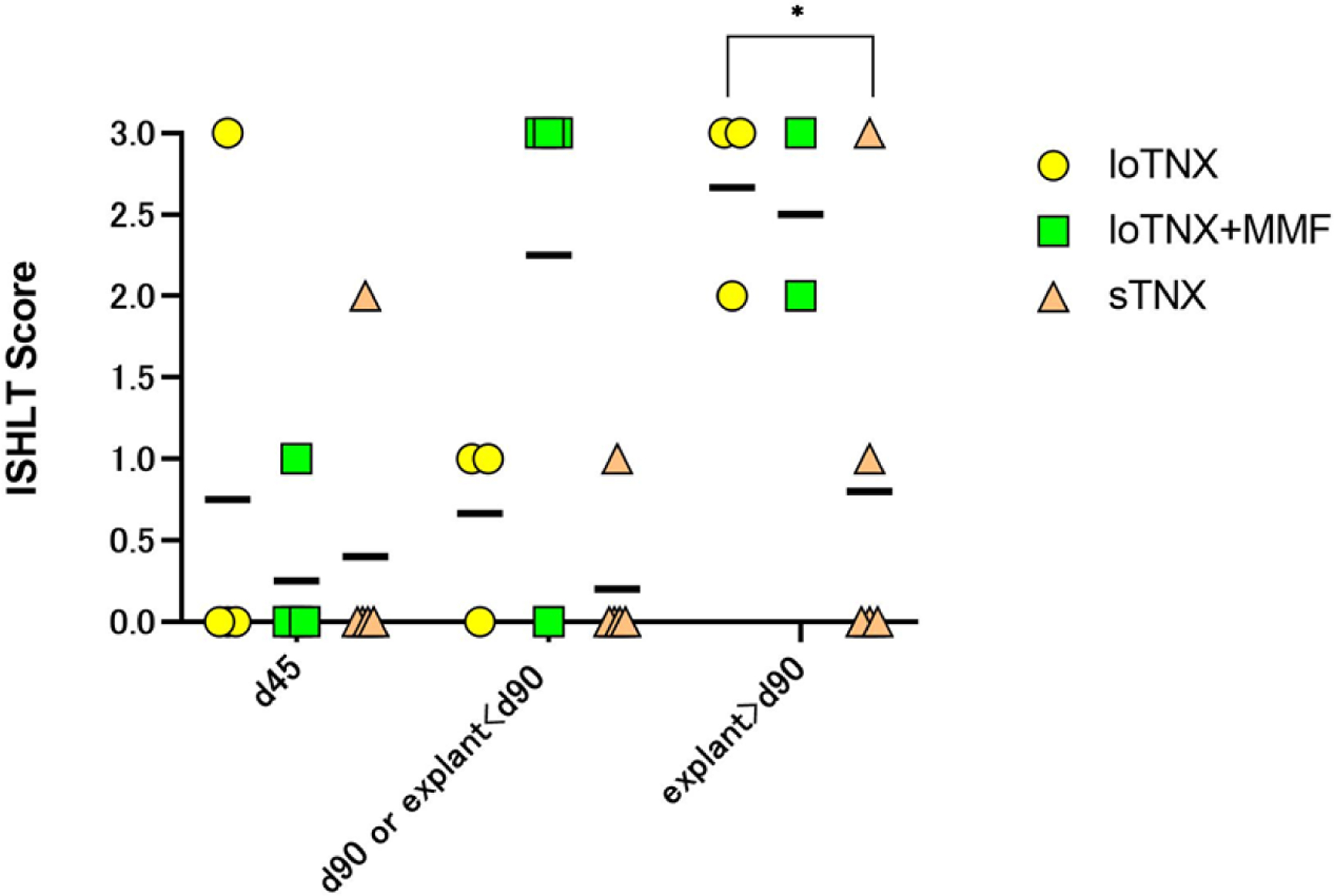
Individual animal and mean (black bars) ISHLT scores at the three protocol-defined time-point biopsies (d45, d90, d180 or earlier explant after day 90), or in for-cause biopsies or explanted failed grafts around those time points. Two grafts in loTNX (yellow symbols) failed with ACR3 at days 35 and 93; one was euthanized on d105 with a beating graft in which evidence of ACR3 was detected on terminal pathology, and the fourth beating graft (2R) was explanted by protocol at 180 days. In loTNX+MMF (green symbols), ACR was moderate (2R) or severe (3R) in the majority of biopsies of beating grafts or in explanted failed grafts after d45. sTNX (brown symbols) was associated with transient moderate rejection (2R resolving to 0R) at d45 in one recipient, and progressive ACR (1R progressing to 3R between day 90 and d116) in association with graft endocarditis and recurrent septicemia after antibiotic cessation at d90. With sTNX, one explanted allograft and 3 end-of-study biopsies around d180 showed absent (0R) or mild rejection (1R). LoTNX had significantly higher mean ISHLT score than sTNX-treated allografts at the time point of subsequent explant after d90 or end-of-study biopsy around d180 (2.7 vs 0.8; *p=0.033). When scores were occasionally discrepant, biopsies were reviewed in conference to discern the source of score variation and adjudicate an agreed score. TNX, TNX-1500, MMF, mycophenolate mofetil; d, post-transplant days; ACR, acute cellular rejection