
FIGURE 2.
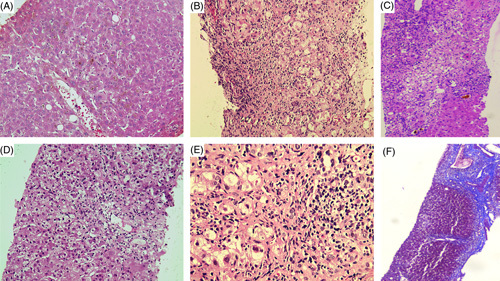
Representative liver histology of patients with ashwagandha-induced liver injury. Severe hepatocellular cholestasis (hematoxylin and eosin stain, ×40) (A); lymphocyte and eosinophil predominant portal inflammation (hematoxylin and eosin stain, ×20) (B); bridging necrosis and canalicular cholestasis in the presence of mild to moderate mixed inflammation consisting of lymphocytes, eosinophils, few plasma cells, and neutrophils (hematoxylin and eosin stain, ×20) (C); centrizonal and focal necrosis with minimal inflammation (hematoxylin and eosin stain, ×20) (D); mild to moderate interface hepatitis with lymphocyte predominant and few macrophage-based portal inflammation (E) and in the patient (shown in C) with bridging necrosis and cholestasis, repeat liver biopsy revealed progression to chronic herb-induced liver injury with the formation of vague/incomplete hepatocyte nodules and thick bridging fibrosis (Masson-trichrome stain, ×10) (F).