
Central Illustration 1.
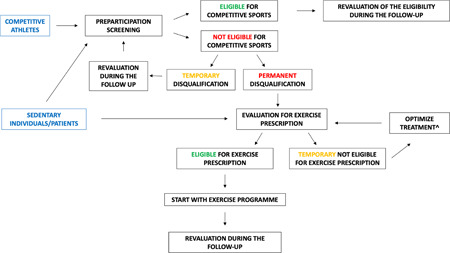
Competitive athletes should undergo comprehensive preparticipation screening, including a 12‐lead resting electrocardiogram. In case of a permanent disqualification, it is of paramount importance to evaluate the subject for a tailored exercise prescription. The prescription should include a comprehensive clinical evaluation, culminating in a personalized prescription with a specific target heart rate for aerobic exercise and detailed information about the intensity, type, volume, and frequency of exercise per week, including resistance conditioning (with a personalized intensity). In case of a clinical risk deemed to be excessively high and the impossibility to temporarily practice exercise, the patient should be reevaluated for an exercise program after the implementation of the medical therapy (e.g., after reducing a significant left ventricular outflow tract obstruction in patients with hypertrophic cardiomyopathy). The exercise program should start gradually, and a routine revaluation after the first months of exercise is essential to evaluate the adaptation to the exercise program, reevaluate the aerobic and anaerobic thresholds, and objectively and subjectively assess the program results. Exercise prescription should also be considered in sedentary individuals who do not want to practice competitive sports but are interested in a personalized training program for primary or secondary prevention. ^e.g., reduction of left ventricular outflow tract obstruction in patients with hypertrophic cardiomyopathy.