
Fig. 3.
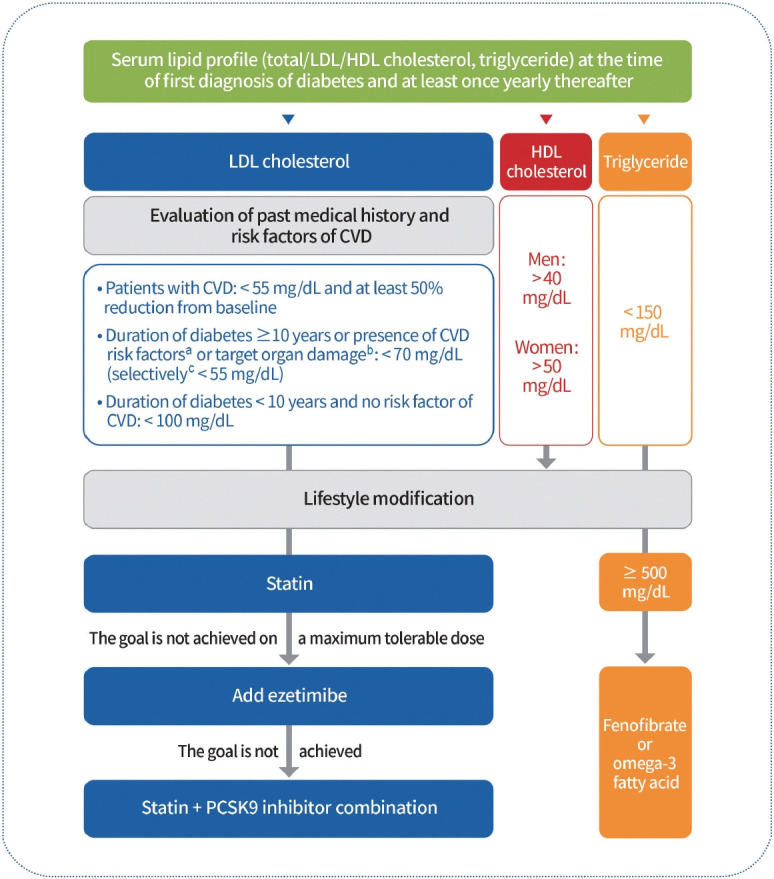
Lipid management in patients with diabetes. Serum lipid profiles should be obtained at the time of the first diagnosis of diabetes and at least once a year thereafter. Past history of cardiovascular disease (CVD) and target organ damage (albuminuria, estimated glomerular filtration rate <60 mL/min/1.73 m2, retinopathy, and left ventricular hypertrophy), the major risk factors for CVD (age, family history of early-onset coronary artery disease, hypertension, smoking, and high-density lipoprotein cholesterol [HDL-C] <40 mg/dL) and duration of diabetes should be investigated to determine the low-density lipoprotein cholesterol (LDLC) goal. Education on active lifestyle modifications should also be provided. Pharmacological therapy should be implemented if LDL-C goals are not achieved. Statins should be used as first-line therapy. Ezetimibe should be added if the goal is not achieved with the maximum tolerable dose of statin therapy. If diabetic patients with CVD do not achieve this goal even after treatment with a statin plus ezetimibe, combination therapy with a statin and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors should be considered. Adults with severe hypertriglyceridemia (triglyceride levels ≥500 mg/dL) were treated with fenofibrate or omega-3 fatty acids. aAge (men ≥45 years, women ≥55 years), family history of early-onset coronary heart disease, hypertension, smoking, HDL-C <40 mg/dL, bAlbuminuria, estimated glomerular filtration rate <60 mL/min/1.73 m2, retinopathy, and left ventricular hypertrophy, cTarget organ damage or three or more major risk factors for CVD.