

Key Points
-
•
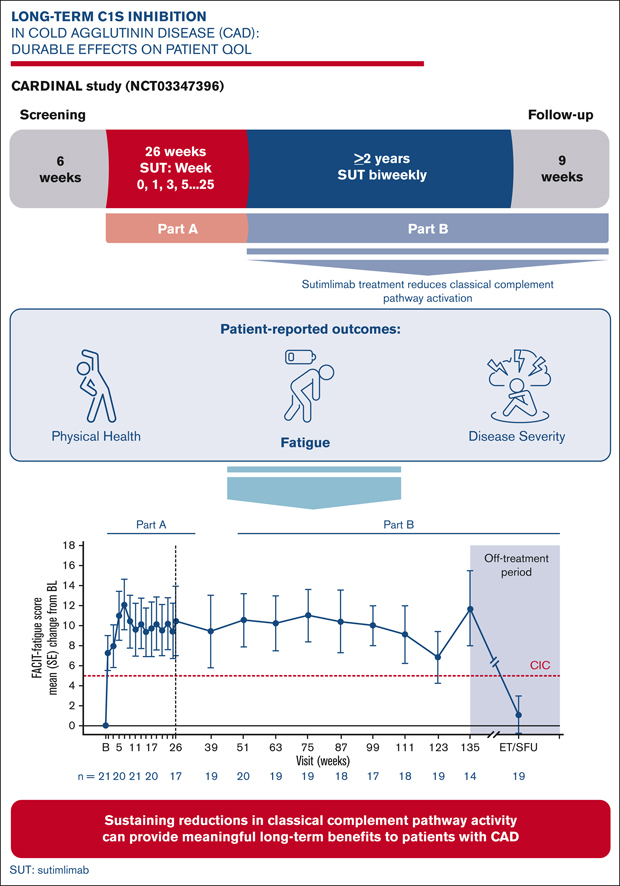
In CARDINAL part B, upstream inhibition of the classical complement pathway in CAD maintained improved patient-reported outcomes at 2 years.
-
•
Sutimlimab provides sustained benefits in chronic CAD, including a continued meaningful impact on patient quality of life.
Visual Abstract
Abstract
Cold agglutinin disease (CAD) is a rare form of autoimmune hemolytic anemia with a substantial burden on patient’s quality of life. CARDINAL was a 2-part, open-label, single-arm, multicenter phase 3 study evaluating the C1s inhibitor, sutimlimab, for treatment of CAD. Part A consisted of the pivotal study phase, with the part B extension phase assessing long-term safety and durability of response including patient-reported outcomes, which is the focus of this report. Altogether, 22 patients continued from part A to part B, majority female (68.2%) with a median age of 71.5 years (range, 55-85). Throughout treatment, score improvement on the Functional Assessment of Chronic Illness Therapy (FACIT)–Fatigue scale exceeded a predefined, group-level clinically important change of ≥5 points vs baseline, with a mean (standard error [SE]) change of 11.7 (3.7) points at week 135. The 12-Item Short Form Health Survey physical and mental component scores remained above baseline, with week 123 mean change (SE) exceeding clinically important changes of 3.9 for physical and 2.8 for mental component scores at 4.7 (2.8) and 3.8 (5.7) points, respectively. EuroQol Visual Analogue Scale, scoring patients’ self-rated health, also remained above baseline with a change of 17.1 (5.6) points at week 135. Patient Global Impression of (fatigue) Severity improved vs baseline, corroborating FACIT-Fatigue scores. Patient Global Impression of Change indicated a reduction in perceived disease burden. Data from CARDINAL part B support sustained alleviation of CAD disease burden after long-term treatment with sutimlimab over 2 years, returning toward baseline upon treatment cessation. This trial was registered at www.clinicaltrials.gov as #NCT03347396.
Introduction
Cold agglutinin disease (CAD) is a rare but serious type of autoimmune hemolytic anemia, characterized by chronic hemolysis mediated by cold agglutinins, primarily monoclonal immunoglobulin M antibodies, which bind to erythrocytes and initiate activation of the classical complement pathway.1,2 This disease accounts for 15% to 25% of autoimmune hemolytic anemia, with a reported prevalence of 16 per million people in Northern Europe, and an incidence rate of 1 per million per year, primarily in the older adult population.1 Patients with CAD can experience deleterious, complement-mediated symptoms, including chronic hemolysis, anemia, fatigue, and hemoglobinuria, as well as transient, cold-induced agglutination–mediated circulatory symptoms, such as acrocyanosis and Raynaud's phenomenon.3,4 These symptoms impose a severe burden on quality of life (QoL), in addition to an increased risk of thromboembolism and early mortality.4, 5, 6 In particular, fatigue has been found to affect 90% of patients with CAD, and patients report a negative effect on their daily activities, physical well-being, emotional well-being, social life, and household finances.7
Sutimlimab is a first-in-class, humanized, monoclonal antibody designed to selectively target C1s, a serine protease of the C1-complex responsible for activating the classical complement pathway of the immune system.8,9 By selectively inhibiting the classical complement pathway at C1s, sutimlimab leaves the immune functions of the lectin and alternative complement pathways intact.8, 9, 10, 11, 12 CARDINAL (NCT03347396) was a prospective, open-label, single-arm, 2-part, multicenter phase 3 study evaluating the efficacy, durability of effect, safety, and tolerability of sutimlimab in patients with primary CAD and a recent history of transfusion. After completion of the 26-week pivotal phase of the study (part A) in 2019, the 1-year interim in 2020 and the 2-year, long-term extension phase (part B) in 2021, sutimlimab was found to be an effective and well-tolerated therapy.9,13,14
The criteria of the composite primary end point (increase in hemoglobin [Hb] level ≥2 g/dL from baseline or reaching a Hb level ≥12 g/dL at the treatment assessment time point [mean of weeks 23, 25, and 26]; absence of transfusions from weeks 5 to 26; no use of protocol-prohibited medications) were met by 54% of patients in CARDINAL part A.9 Sutimlimab treatment had a rapid and sustained effect on Hb levels and hemolytic markers, as well as yielded a clinically meaningful reduction in fatigue (secondary end point), with only mild-to-moderate adverse events assessed as treatment-related.9,13,14
To date, the number of publications describing long-term patient-reported outcome (PRO) data in patients receiving treatment for CAD is limited. In CARDINAL, treatment with sutimlimab demonstrated improvement across a range of PROs, assessed by the Functional Assessment of Chronic Illness Therapy (FACIT)–Fatigue scale and exploratory end point measures consisting of the 12-Item Short Form Health Survey (SF-12), the EuroQol Visual Analogue Scale (EQ-VAS), and the Patient Global Impression of (fatigue) Severity (PGIS) and Patient Global Impression of Change (PGIC) questionnaires.15
Part B of the CARDINAL study constituted a 2-year extension period to evaluate the long-term safety, tolerability, and durability of sutimlimab treatment response beyond 26 weeks. Although the long-term safety and efficacy data are reported in a separate manuscript,14 in this study we present the PRO data demonstrating the durable impact on QoL achieved with long-term management of CAD with sutimlimab.
Methods
Study design, dosing, and patient population
The CARDINAL study (#NCT03347396) was a 2-part, open-label, single-arm, multicenter study evaluating the safety and efficacy of IV administered sutimlimab as a treatment for patients with primary CAD. A full description of the study design was published with the pivotal trial results in 2021.9 In brief, eligible patients were aged ≥18 years with a body weight of ≥39 kg, a Hb level of ≤10 g/dL, evidence of active hemolysis (total bilirubin above normal), a recent history of transfusion (within 6 months), and the presence of ≥1 CAD-related symptom at screening. Sutimlimab was administered by IV infusion at fixed doses of 6.5 g for patients weighing <75 kg and 7.5 g for patients weighing ≥75 kg. Initial doses were administered at day 0 and day 7, followed by maintenance dosing every 14 days thereafter. All patients who completed part A (22/24), including those who received transfusions, were eligible and were rolled over to part B and continued their same biweekly dose treatment for up to 2 years after the last patient finished part A. A missing dose (ie, outside the dosing window or >17 days since the last dose) was reconciled with an additional loading dose 1-week before the next scheduled dose, after which biweekly dosing visits resumed.
All ongoing patients receiving treatment in part B were evaluated in a follow-up end-of-study visit 9 weeks after their last dose. As previously described, part A and part B were conducted in accordance with consensus ethics principles derived from international ethics guidelines, and patients gave written informed consent for their participation. The protocol and any amendments and country-specific amendments was/were submitted to independent ethics committees and/or institutional review boards for review and written approval.
QoL outcome measures
QoL and PROs were assessed by FACIT-Fatigue score, SF-12 score, EuroQol five-dimension five-level questionnaire (EQ-5D-5L) index score, EQ-VAS, PGIS score, and PGIC score. In part B, assessments were conducted every 12 weeks at scheduled visits both before and throughout the treatment period, and at the 9-week follow-up visit. Data in this manuscript are reported up to week 135, the assessment time point closest to 2 years, and for the follow-up visit, 9 weeks after the last dose of sutimlimab. For all PROs, mean change from baseline is reported.
FACIT-Fatigue
The 13-item FACIT-Fatigue scale was used to rate the extent of fatigue on a 5-point scale ranging from 0 (not at all) to 4 (very much so) over the past 7 days. A patient’s total score could range from 0 (worst fatigue) to 52 (no fatigue), with a change of ≥5 points considered a clinically important change (CIC) in CAD.16,17
Short Form Health Survey (SF-12)
The 12-item, 8-domain SF-12 survey was used to assess physical component scores (PCS, such as general health, physical functioning, role physical, and body pain) and mental component scores (MCS, such as vitality, social functioning, role emotional, and mental health) over the past 4 weeks. A patient’s total score could range from 0 (worst health) to 100 (best health), with changes ≥3.9 and 2.8 being considered as CICs in CAD for PCS and MCS, respectively.18, 19, 20
EQ-5D-5L and EQ-VAS
The 5-domain EQ-5D-5L instrument was used to assess general health consisting of the following domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. To assess each domain, patients chose from a 5-level response scale corresponding from minimal problems to extreme problems for the current day, which were then translated into index scores. EQ-5D-5L health states can be represented by a single number given as the summary index value, which considers the values (weights) of each health state within a socioeconomic region. In addition, patients rated their current day’s health on a scale ranging from 0 (worst health) to 100 (best health) using the EQ-VAS.21,22
PGIS and PGIC questionnaires
The single-item PGIS questionnaire was used to assess fatigue severity (over the past week) on a 5-point Likert scale ranging from “no fatigue” to “very severe fatigue” at baseline and at week 135.23 The single-item PGIC questionnaire was used to assess change in symptom severity since the beginning of the study on a 7-point Likert scale ranging from 1 (very much improved) to 7 (very much worse) at week 135.23
Statistical analysis
Because part B of this study was an open-label extension that included patients from part A, no calculation for sample size was performed. Data were summarized for the full analysis set using standard summary statistics for continuous and categorical data. The full analysis set was defined as all patients who enrolled in part B and received ≥1 dose of study drug, synonymous with an intent-to-treat study population. Because the duration of treatment period varied in part B, PRO end points by visit were summarized through week 135. If a patient had missing data in a PRO questionnaire at a visit, the prorated score was calculated if >50% of the items (eg, a minimum of 7 out of 13 items for FACIT-Fatigue) were available.
Results
Baseline demographics
All the 22 patients who completed part A, were enrolled in part B (supplemental Figure 1). A total of 16 patients were among the 6.5 g-cohort and 6 were among the 7.5 g-cohort. The majority of patients were female (68.2%), with a median age of 71.5 years (range, 55-85) (Table 1). Baseline assessment of PROs included a mean (standard deviation) FACIT-Fatigue score of 32.4 (10.9; n = 21); mean SF-12 PCS and MCS scores of 39.5 (8.2; n = 20) and 50.4 (8.1; n = 20), respectively; a mean EQ-5D-5L index score of 0.74 (0.18; n = 21); and EQ-VAS of 63.3 (12.8; n = 21). Moderate or severe fatigue was reported by 66.6% of patients completing the PGIS at baseline (n = 6).
Table 1.
Patient demographics and disease characteristics at baseline
| Total | |
|---|---|
| Patients, n | 22 |
| Age, y | |
| Mean (SD) | 71.7 (7.9) |
| Median (range) | 71.5 (55-85) |
| Female, n (%) | 15 (68.2) |
| Geographic location, n (%) | |
| Europe | 15 (68.2) |
| North America | 3 (13.6) |
| Asia | 3 (13.6) |
| Australia | 1 (4.5) |
| Baseline FACIT-Fatigue∗, (n = 21) | |
| Mean (SD) | 32.4 (10.9) |
| Median (range) | 38 (14-47) |
| Baseline SF-12 (PCS)†, (n = 20) | |
| Mean (SD) | 39.5 (8.2) |
| Median (range) | 40.6 (19.9-52.2) |
| Baseline SF-12 (MCS)†, (n = 20) | |
| Mean (SD) | 50.4 (8.1) |
| Median (range) | 50.1 (33.8-63.2) |
| Baseline EQ-5D-5L Index Score‡, (n = 21) | |
| Mean (SD) | 0.74 (0.18) |
| Median (range) | 0.79 (0.34-1.0) |
| Baseline EQ-VAS§, (n = 21) | |
| Mean (SD) | 63.3 (12.8) |
| Median (range) | 60 (40-80) |
SD, standard deviation.
Scores on the FACIT-Fatigue Scale range from 0 to 52, with higher scores indicating less fatigue.
Scores range from 0 to 100, with higher scores indicating better physical and mental health functioning.
EQ-5D-5L index scores range from 0 (the value of a health state equivalent to dead) to 1 (the value of full health).
The EQ-VAS is a vertical visual analog scale that takes values between 100 (best imaginable health) and 0 (worst imaginable health).
FACIT-Fatigue score
Mean FACIT-Fatigue score improvement was sustained throughout part B, with the mean change from baseline remaining above the empirically determined CIC of 5 points from weeks 1 to 135 (Figure 1). The maximum mean (standard error [SE]) change was 12.1 (2.5) points at week 7 and the minimum was 6.8 (2.6) points at week 123. The mean (SE) change from baseline at week 135, ∼2 years from the end of part A, was 11.7 (3.7) points. The mean (SE) change from baseline remained above CIC at the last available on-treatment visit, in which it was 8.3 (2.8) points. At the early termination or safety follow-up (ET/SFU) visit 9 weeks after cessation of sutimlimab, the mean (SE) change compared with baseline was 1.1 (1.9) points, falling below the CIC (Figure 1). Over parts A and B of the study, patients received sutimlimab for a median of 144 weeks (range 54-177).
Figure 1.

Mean (SE) change from baseline in FACIT-Fatigue score throughout pivotal (part A) and 2-year extension (part B) phases of CARDINAL, and at the ET/SFU follow-up visit, 9 weeks after cessation of sutimlimab treatment. BL, baseline.
SF-12 PCS and MCS
Mean SF-12 score improvement for both PCS and MCS remained above their respective CICs of 3.9 and 2.8 points until week 51. Thereafter, although the mean change in PCS score remained above CIC throughout until week 123, the mean MCS score fluctuated above and below the CIC of 2.8 but consistently remained above baseline value until week 123 (Figure 2). The maximum mean (SE) change in PCS score was 12.0 (1.4) at week 111, and the minimum was 4.7 (2.8) points at week 123. The maximum mean (SE) change in MCS score was 5.9 (2.6) points at week 39, and the minimum was 1.6 (2.4) points at week 87. At week 123, both PCS and MCS scores were above their respective CICs (3.9 and 2.8), with mean (SE) change from baseline of 4.7 (2.8) and 3.8 (5.7) points, respectively. A meaningful assessment at the week 135 visit was not possible owing to a protocol change that resulted in a low number of respondents among the patients who initiated the study before 2019 (n = 1 for week 135). Similarly, SF-12 was only assessed in 1 patient at the 9-week follow-up visit.
Figure 2.

Change from baseline in SF-12 physical and mental component scores. Mean (SE) change from baseline in Short Form Health Survey (SF-12) PCS (A) and MCS (B) throughout the 2-year extension (part B) phase of CARDINAL. Note: SF-12 data not presented at week 135 owing to low patient numbers. BL, baseline.
EQ-5D-5L index and VAS score
Mean EQ-5D-5L index score improvement remained above mean baseline levels throughout part B. The mean (SE) index score was 0.81 (0.06; n = 15) at week 135 and 0.74 (0.04; n = 20) at ET/SFU (supplemental Table 2).
Mean EQ-VAS score improvement remained above baseline levels throughout part B (Figure 3). The maximum mean (SE) change from baseline was 18.9 (3.6) points at week 111, and the minimum was 8.8 (4.3) points at week 123. Mean (SE) change from baseline in EQ-VAS score was 17.1 (5.6; n = 15) points ∼2 years after completion of part A at week 135 and 1.3 (4.4; n = 19) at ET/SFU.
Figure 3.

Mean (SE) change from baseline in EQ-VAS scores throughout the 2-year extension (part B) phase of CARDINAL, and at the ET/SFU follow-up visit, 9 weeks after cessation of sutimlimab treatment. BL, baseline.
PGIC and PGIS
The majority of PGIS responses (66.6%; 4/6) reported fatigue severity ranging from “moderate” (33.3%) to “severe” (33.3%) at baseline. At week 135, the proportion of patients reporting fatigue severity as “none” or “mild” was 80% (12/15) (Figure 4A). At ET/SFU, 50% (10/20) of patients rated their fatigue as “none” or “mild,” with 25% reporting “severe” and 5% reporting “very severe” fatigue.
Figure 4.

Change from baseline in PGIS and PGIC questionnaires at week 135 and ET/SFU of CARDINAL. (A) Proportion of responders (%) reporting no, mild, moderate, severe or very severe fatigue at baseline, week 135 and ET/SFU. (B) Proportion of responders (%) reporting degrees of improvement from baseline, from very much improved to very much worse, at week 135 and ET/SFU.
The majority of PGIC responses (86.7%; 13/15) reported an improvement in disease burden including “minimally improved” (13.3%), “much improved” (40%), or “very much improved” (33.3%), at week 135 (Figure 4B). At the ET/SFU follow-up visit, more than half of the patients still reported “much improved” (40%) or “very much improved” (15%) status, but the proportion of patients reporting improvements in disease burden compared with baseline was reduced to 65%. In contrast, 15% (3/20) of patients reported a worse disease burden compared with baseline.
Discussion
CAD is a chronic, severe disease leading to symptoms with deleterious effects on patients’ QoL, negatively affecting their ability to carry out daily activities and restricting their social and professional lives.1,2,7 This is reflected in the baseline PRO values in the CARDINAL study, including a mean FACIT-Fatigue score of 32.4 which is comparable to the levels of fatigue seen in other serious chronic diseases, including rheumatoid arthritis and cancer-related anemia.24, 25, 26, 27 A survey of patients with CAD found that 44% of patients experience this fatigue on a daily basis.7 The baseline values for SF-12 and EQ-VAS were similarly comparable to or more severe than values reported for patients with rheumatoid arthritis.28 In addition, medically attended anxiety and depression have been found to manifest at a higher rate in CAD patients than in a matched non-CAD cohort.29 Because CAD is a condition that occurs most commonly in older patients, it is likely to exacerbate the impact of aging in patients, and these data indicate a substantial burden on patient QoL.
Data from the hematologic results of the CARDINAL study part B, reported in another manuscript,14 demonstrated that long-term inhibition of C1s with sutimlimab yields sustained improvements in hemolysis and anemia in a treatment-dependent manner, with these parameters improving rapidly on treatment initiation and declining after discontinuation. In this report, PROs including FACIT-Fatigue, SF-12, EQ-VAS, PGIC, and PGIS also showed rapid improvements compared with baseline after treatment with sutimlimab. The beneficial effects of sustained treatment with sutimlimab on FACIT-Fatigue and other PROs were similarly maintained throughout the treatment period and declined after discontinuation. In part B, FACIT-Fatigue scores maintained a consistent elevation above baseline values that was maintained for over 2 years and until the last available treatment score. Improvements in FACIT-Fatigue and both components of SF-12 exceeded their respective CIC values, representing meaningful treatment benefits for individual patients’ QoL.17,20 Both the PCS and MCS components of SF-12 showed benefits throughout the extension period, though the PCS showed greater improvement. Although the MCS was above baseline throughout part B, unlike PCS it did not remain consistently above the CIC. The mental component of the SF-12 might be affected by social or personal factors unrelated to the disease state which are not within the scope of this study and which may have affected the data owing to the small sample size. PGIS and PGIC both indicated an improvement in fatigue severity and overall health from baseline at week 135, with no patients reporting severe fatigue, and 86.7% of evaluable patients experienced an improved overall disease state. Taken together, these data indicate that long-term upstream inhibition of complement pathway activation is an effective therapy for the relief of fatigue and the overall disease burden associated with CAD.
Our observations on the effects on PROs after discontinuation of sutimlimab are in line with previous reports on Hb levels and hemolysis.14,30,31 In CARDINAL part B, data from the 9-week follow-up period after cessation of sutimlimab included 20 of the 22 patients who entered part B and suggested that as complement inhibition was reversed upon discontinuation, treatment effect on hemolytic anemia declined.14 In a phase 1b trial, Jäger et al30 reported that 7 of 10 patients with CAD responded to treatment with sutimlimab, but hemolytic anemia recurred when the drug was cleared from circulation, from 3 to 4 weeks after the last dose. An observational study by Gelbenegger et al31 reported on 3 patients with CAD who had responded to sutimlimab in a named patient program and open-label extension. After discontinuation of sutimlimab, 1 of the 3 patients relapsed after 7 weeks. Interestingly, the 2 other patients displayed sustained hematologic remission 12 months after discontinuation, indicating that few patients can maintain near on-treatment Hb levels without overt signs of hemolysis after discontinuation of sutimlimab. Overall, current evidence supports an association between complement inhibition and reduction in hemolysis and provides a rationale for the use of sutimlimab in long-term treatment for patients with CAD. To our knowledge, CARDINAL is the first study to report on PROs after cessation of sutimlimab. We previously showed that similar to Hb levels, mean FACIT-Fatigue scores approached presutimlimab values after discontinuation.14 Similar effects were seen for the additional PROs described in this study. EQ-VAS and PGIS scores declined 9 weeks after the last sutimlimab dose in this study, and EQ-5D index scores were slightly lower than baseline. Interestingly, the proportion of patients at the study follow-up visit self-reporting an improved health status on the PGIC form compared with baseline remained high.
Overall, C1s inhibition had a positive impact on patient well-being as recorded by PROs, and this effect followed the major shifts observed in hematologic parameters assessing anemia and hemolysis in this study, declining after discontinuation of treatment. This impact on patient experience is an important factor for clinical decision-making while treating a disease with a heavy burden on patient QoL. The novel findings on PRO improvements in the long-term and the effect of treatment discontinuation reported in this study will therefore be of significant interest to clinicians treating patients with CAD, favoring the recommendation that patients should remain on treatment. The contribution of individual hematologic parameters to this subjective benefit remains an interesting question, and further studies with larger patient cohorts and more granular sampling are needed to assess the correlation between these parameters and identify any existing functional relationships.
Limitations include the single-arm study design and the low patient numbers owing to the rarity of the disease. With the exception of the FACIT-Fatigue assessment, the PROs were exploratory end points in CARDINAL.
The results of CARDINAL part B show that continued upstream inhibition of the classical complement pathway with sutimlimab provides sustained and durable treatment benefits in chronic CAD, including a continued meaningful impact on patient QoL in the long term.
Conflict-of-interest disclosure: A.R. has received research support from Roche, and received honoraria and provided consultancy to Alexion Pharmaceuticals Inc, Amgen, Apellis Pharmaceuticals, Biocryst, Grifols, Kira, Novartis, Roche, Bioverativ (a Sanofi company), Sanofi, and Sobi. C.M.B. has received honoraria and/or research funding from Alexion Pharmaceuticals, Bioverativ, Cellphire, Incyte, Rigel, and Sanofi Genzyme. W.B. has received research support from Alexion Pharmaceuticals and Novartis; participated in advisory boards for Agios, Alexion Pharmaceuticals Inc, Bioverativ, and Incyte; and has been an invited speaker for Alexion Pharmaceuticals Inc, and Novartis. T.H.A.T. has participated in advisory boards for Janssen, Novartis, and Sobi. S.D. has received grant funding, honoraria, and/or speaker’s fees from Janssen, BeiGene, and Sanofi. D.C. is President of FACIT.org, which distributes the FACIT-Fatigue Questionnaire. S.B., D.J., R.Y., F.S., and M.W. are employees of Sanofi and may hold shares and/or stock options in the company. The remaining authors declare no competing financial interests.
Acknowledgments
The authors thank the investigators, health care providers, research staff, and patients and their families who participated in the CARDINAL study. The authors also thank Florence Joly, Jennifer Wang, Erika von Grote, and Timothee Sourdille for their contributions to the development of this manuscript. Medical writing and editing support were provided by David Campbell of Lucid Group Communications Ltd.
This study was funded by Sanofi (Waltham, MA).
Authorship
Contribution: All authors had access to primary clinical trial data, had full editorial control of the manuscript, and provided final approval of all content.
Footnotes
Presented at the European Hematology Association annual meeting, 9-12 June 2022.
Qualified researchers may request access to patient-level data and related study documents, such as the clinical study report, study protocol (with amendments), statistical analysis plan, and data set specifications. Notably, patient-level data will be anonymized, and study documents will be redacted to protect the privacy of trial participants. Further information related to Sanofi’s data-sharing criteria, eligible studies, and process for requesting access can be found at: https://www.vivli.org/.
The full-text version of this article contains a data supplement.
Supplementary Material
References
- 1.Berentsen S, Ulvestad E, Langholm R, et al. Primary chronic cold agglutinin disease: a population based clinical study of 86 patients. Haematologica. 2006;91(4):460–466. [PubMed] [Google Scholar]
- 2.Berentsen S. Complement activation and inhibition in autoimmune hemolytic anemia: focus on cold agglutinin disease. Semin Hematol. 2018;55(3):141–149. doi: 10.1053/j.seminhematol.2018.04.002. [DOI] [PubMed] [Google Scholar]
- 3.Berentsen S. Cold agglutinin disease. Hematology Am Soc Hematol Educ Program. 2016;2016(1):226–231. doi: 10.1182/asheducation-2016.1.226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mullins M, Jiang X, Bylsma LC, et al. Cold agglutinin disease burden: a longitudinal analysis of anemia, medications, transfusions, and health care utilization. Blood Adv. 2017;1(13):839–848. doi: 10.1182/bloodadvances.2017004390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Broome CM, Cunningham JM, Mullins M, et al. Increased risk of thrombotic events in cold agglutinin disease: a 10-year retrospective analysis. Res Pract Thromb Haemost. 2020;4(4):628–635. doi: 10.1002/rth2.12333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bylsma LC, Gulbech Ording A, Rosenthal A, et al. Occurrence, thromboembolic risk, and mortality in Danish patients with cold agglutinin disease. Blood Adv. 2019;3(20):2980–2985. doi: 10.1182/bloodadvances.2019000476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Joly F, Schmitt LA, Watson PAM, Pain E, Testa D. The burden of cold agglutinin disease on patients' daily life: web-based cross-sectional survey of 50 American patients. JMIR Form Res. 2022;6(7):e34248. doi: 10.2196/34248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bartko J, Schoergenhofer C, Schwameis M, et al. A randomized, first-in-human, healthy volunteer trial of sutimlimab, a humanized antibody for the specific inhibition of the classical complement pathway. Clin Pharmacol Ther. 2018;104(4):655–663. doi: 10.1002/cpt.1111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Röth A, Barcellini W, D'Sa S, et al. Sutimlimab in cold agglutinin disease. N Engl J Med. 2021;384(14):1323–1334. doi: 10.1056/NEJMoa2027760. [DOI] [PubMed] [Google Scholar]
- 10.Shi J, Rose EL, Singh A, et al. TNT003, an inhibitor of the serine protease C1s, prevents complement activation induced by cold agglutinins. Blood. 2014;123(26):4015–4022. doi: 10.1182/blood-2014-02-556027. [DOI] [PubMed] [Google Scholar]
- 11.Colonna L, Parry GC, Panicker S, Elkon KB. Uncoupling complement C1s activation from C1q binding in apoptotic cell phagocytosis and immunosuppressive capacity. Clin Immunol. 2016;163:84–90. doi: 10.1016/j.clim.2015.12.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lewis LA, Panicker S, DeOliveira RB, Parry GC, Ram S. Effect of a C1s inhibitor on the efficacy of anti-capsular antibodies against Neisseria meningitidis and Streptococcus pneumoniae. Immunohorizons. 2019;3(11):519–530. doi: 10.4049/immunohorizons.1900031. [DOI] [PubMed] [Google Scholar]
- 13.Röth A, Barcellini W, D’Sa S, et al. Complement C1s inhibition with sutimlimab results in durable response in cold agglutinin disease: CARDINAL study 1-year interim follow-up results. Haematologica. 2022;107(7):1698–1702. doi: 10.3324/haematol.2021.279812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Röth A, Barcellini W, D'Sa S, et al. Sustained inhibition of complement C1s with sutimlimab over 2 years in patients with cold agglutinin disease. Am J Hematol. 2023;98(8):1246–1253. doi: 10.1002/ajh.26965. [DOI] [PubMed] [Google Scholar]
- 15.Röth A, Barcellini W, Tvedt THA, et al. Sutimlimab improves quality of life in patients with cold agglutinin disease: results of patient-reported outcomes from the CARDINAL study. Ann Hematol. 2022;101(10):2169–2177. doi: 10.1007/s00277-022-04948-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Acaster S, Dickerhoof R, DeBusk K, Bernard K, Strauss W, Allen LF. Qualitative and quantitative validation of the FACIT-fatigue scale in iron deficiency anemia. Health Qual Life Outcomes. 2015;13:60. doi: 10.1186/s12955-015-0257-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hill QA, Röth A, Jilma B, et al. 2021. Clinically important change in FACIT-Fatigue score for patients with cold agglutinin disease: an analysis using the phase 3 CARDINAL and CADENZA studies. European Hematology Association Virtual Congress. [Google Scholar]
- 18.Bhandari NR, Kathe N, Hayes C, Payakachat N. Reliability and validity of SF-12v2 among adults with self-reported cancer. Res Social Adm Pharm. 2018;14(11):1080–1084. doi: 10.1016/j.sapharm.2018.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Huo T, Guo Y, Shenkman E, Muller K. Assessing the reliability of the short form 12 (SF-12) health survey in adults with mental health conditions: a report from the wellness incentive and navigation (WIN) study. Health Qual Life Outcomes. 2018;16(1):34. doi: 10.1186/s12955-018-0858-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Joly F, Kosinski M, Shafer F, Wardecki M, Karaouni A, Hill Q. Clinically important change in SF-12v2 physical (PCS) and mental (MCS) component summary scores for patients with cold agglutinin disease: an analysis using the phase 3 CARDINAL and CADENZA studies. Blood. 2021;138(suppl 1) [Google Scholar]
- 21.Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–343. doi: 10.3109/07853890109002087. [DOI] [PubMed] [Google Scholar]
- 22.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L) Qual Life Res. 2011;20(10):1727–1736. doi: 10.1007/s11136-011-9903-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Eremenco S, Chen WH, Blum SI, et al. Comparing patient global impression of severity and patient global impression of change to evaluate test-retest reliability of depression, non-small cell lung cancer, and asthma measures. Qual Life Res. 2022;31(12):3501–3512. doi: 10.1007/s11136-022-03180-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cella D, Eton DT, Lai JS, Peterman AH, Merkel DE. Combining anchor and distribution-based methods to derive minimal clinically important differences on the Functional Assessment of Cancer Therapy (FACT) anemia and Fatigue scales. J Pain Symptom Manage. 2002;24(6):547–561. doi: 10.1016/s0885-3924(02)00529-8. [DOI] [PubMed] [Google Scholar]
- 25.Cella D, Yount S, Sorensen M, Chartash E, Sengupta N, Grober J. Validation of the Functional Assessment of Chronic Illness Therapy Fatigue Scale relative to other instrumentation in patients with rheumatoid arthritis. J Rheumatol. 2005;32(5):811–819. [PubMed] [Google Scholar]
- 26.Escalante CP, Chisolm S, Song J, et al. Fatigue, symptom burden, and health-related quality of life in patients with myelodysplastic syndrome, aplastic anemia, and paroxysmal nocturnal hemoglobinuria. Cancer Med. 2019;8(2):543–553. doi: 10.1002/cam4.1953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schrezenmeier H, Röth A, Araten DJ, et al. Baseline clinical characteristics and disease burden in patients with paroxysmal nocturnal hemoglobinuria (PNH): updated analysis from the International PNH Registry. Ann Hematol. 2020;99(7):1505–1514. doi: 10.1007/s00277-020-04052-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dritsaki M, Petrou S, Williams M, Lamb SE. An empirical evaluation of the SF-12, SF-6D, EQ-5D and Michigan Hand Outcome Questionnaire in patients with rheumatoid arthritis of the hand. Health Qual Life Outcomes. 2017;15(1):20. doi: 10.1186/s12955-016-0584-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Broome CM, Hooda N, Su J, et al. Medically-attended anxiety and depression is increased among newly diagnosed patients with cold agglutinin disease: analysis of an integrated claim-clinical cohort in the United States. PLoS One. 2022;17(12):e0276617. doi: 10.1371/journal.pone.0276617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jäger U, D'Sa S, Schörgenhofer C, et al. Inhibition of complement C1s improves severe hemolytic anemia in cold agglutinin disease: a first-in-human trial. Blood. 2019;133(9):893–901. doi: 10.1182/blood-2018-06-856930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Gelbenegger G, Jäger U, Fillitz M, Schoergenhofer C, Sillaber C, Jilma B. Sustained hematologic remission after discontinuation of sutimlimab treatment in patients with cold agglutinin disease. Blood Adv. 2022;7(10):1987–1990. doi: 10.1182/bloodadvances.2022008574. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.