

Abstract
A 50-year-old man who had undergone endovascular therapy 70 days previously was referred to us for the sudden onset of cyanosis with rest pain in the bilateral lower limbs. The patient was diagnosed with blue toe syndrome. Although computed tomography angiography showed irregular aortic wall thickness, preoperative aortic angioscopy detected a remarkable number of spontaneously ruptured aortic plaques, such as puff-chandelier ruptures, predominantly in the abdominal aorta. Continuous embolization of a large quantity of cholesterol crystals from puff-chandelier ruptures subsequently might be responsible for cholesterol embolization syndrome.
Learning objective
A patient presenting with cholesterol embolization syndrome had undergone a non-obstructive general angioscopy. We highlight the numerous spontaneously ruptured aortic plaques demonstrated by non-obstructive general angioscopy.
Keywords: Puff-chandelier rupture, Aorta, Angioscopy, Cholesterol crystal
Introduction
Cholesterol embolization syndrome (CES) refers to the embolization of the contents of an atherosclerotic plaque from a proximal large-caliber artery to distal small to medium arteries causing end-organ damage by mechanical ischemia and inflammatory response [1]. CES may affect multi-organs and might be fatal. Blue toe syndrome is a peripheral manifestation of CES. The risk factors for CES are related to atherosclerosis [2]. The severity of atherosclerosis is directly associated with the chance of developing CES [3]. To find the mechanism of CES, demonstrating each step, continuous plaque scattering that is prone to CES, flowing in the aorta, and reaching end-organs are essential. The last step, embolization in the skin and kidney, is well-known [1,3]. We developed a method to observe spontaneously ruptured aortic plaques (SRAPs) using non-obstructive general angioscopy [4,5]. Debris that causes CES is thought to be atheroma with cholesterol crystals (CCs) [5]. Among SRAPs, puff-chandelier rupture is caused by puff-like materials easily blown out spontaneously that glisten against the light from the tip of the angioscopic fiber. Puff-chandelier rupture contains CCs. CCs were shown to be the main trigger of interleukin (IL)-6 production through innate inflammatory response in human SRAPs in situ [6]. We report the non-obstructive general angioscopy (NOGA) observation of a patient with blue toe syndrome three months after percutaneous transluminal intervention.
Case report
A 50-year-old man with hypertension and dyslipidemia was referred to us for the sudden onset of cyanosis with rest pain for bilateral lower limbs for one week (Fig. 1, Fig. 2A). He had a history of percutaneous coronary intervention for angina pectoris 92 days previously and endovascular therapy for bilateral common iliac stenoses 70 days previously. (Fig. 2B). He underwent successful endovascular therapies (EVT) for the lesions by femoral artery approaches (Fig. 2C). No slow flow was found during and after EVT, and he was free of embolic limb symptoms such as cyanosis for at least five days and a 4-times regular visit to the hospital until the seven days before the onset. The right and left ankle-brachial indexes improved from 0.79 and 0.79 to 1.14 and 1.10, respectively. On admission, the right and left ankle-brachial indices were 1.17 and 1.01, respectively. Magnetic resonance angiography of the lower limbs did not reveal significant stenosis or occlusion in the arteries of the lower extremities. He was diagnosed with blue toe syndrome. Low-density lipoprotein cholesterol decreased from 217 mg/dL to 77 mg/dL by 10 mg rosuvastatin and 10 mg ezetimibe (Fig. 1). Preoperative computed tomography and NOGA for aortic atherosclerosis [4] (Fig. 1) were reviewed. Angioscopic images were obtained with a VISIBLE Fiber (FT-203F, Fiber Tech Co. Ltd., Tokyo, Japan), a fiber imaging system, and a console (Intertec Medicals Co. Ltd., Osaka, Japan). Computed tomography angiography showed irregular wall thickness before diagnostic catheterization without remarkable calcification, protruding, or floating plaques in the thoracic and abdominal aorta (Video 1), while NOGA detected 23 SRAPs in the aorta (Fig. 3A and Video 1). Five SRAPs were distributed circumferentially (Fig. 3B and C). The puff-chandelier rupture was dominantly distributed in the abdominal aorta (Fig. 3C), and histopathological examination of sampling materials from the puff-chandelier rupture demonstrated CCs and atheromatous materials (Fig. 3D and E). Sampling from 5 out of 13 puff-chandelier ruptures was performed using the NOGA system. CCs were found in 3 of 5 samples, and the number of CCs averaged 6455/10 mL of CCs. Low-density lipoprotein cholesterol decreased to 4 mg/dL by additional subcutaneous injection with 140 mg evolocumab. (Fig. 1). He recovered from blue toe syndrome after two months through steroid pulse therapy.
Fig. 1.

The clinical course of the patient.
Fig. 2.
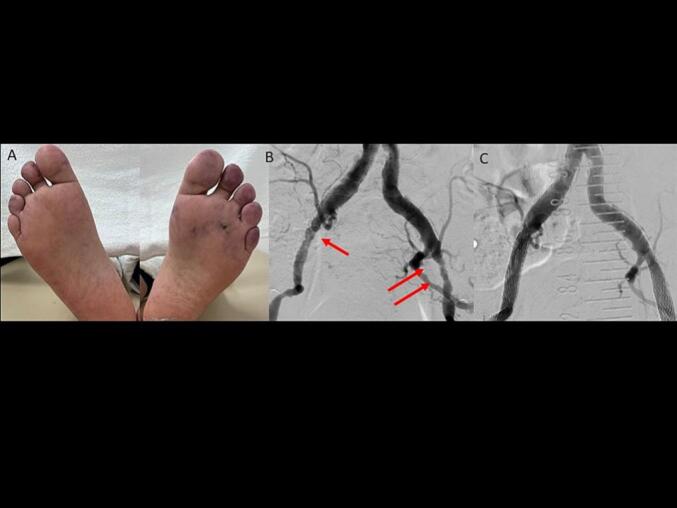
A. A gross image of lower limbs on admission.
B. Angiography of common iliac arteries with significant stenoses (arrows).
C. Angiography of common iliac arteries after stenting.
Fig. 3.

A. A representative image of puff-chandelier rupture in the abdominal aorta demonstrated by non-obstructive general angioscopy.
B. A schematic image of spontaneous ruptured aortic plaques detected by non-obstructive general angioscopy in the thoracic aorta.
C. A schematic image of spontaneous ruptured aortic plaques detected by non-obstructive general angioscopy in the abdominal aorta.
D. A polarized light microscopic image of cholesterol crystals sampled from puff-chandelier rupture. Bar: 20 μm
E. Histopathological image of the puff-chandelier plaque stained with hematoxylin-eosin showing atheromatous materials. Bar: 50 μm.
P, puff rupture; PC, puff-chandelier rupture; E, erosion; FB, fissure bleeding; SB, subintimal bleeding.
Discussion
Predisposing risk factors for cholesterol embolism include male gender, hypertension, hyperlipidemia, diabetes mellitus, peripheral vascular disease, atherosclerosis of the ascending aorta, renal failure, and advanced age [2]. These risk factors are related to atherosclerosis. Identifying SRAPs, including CCs, might lead to preventing CES. Notably, remarkable atherosclerosis is due to CES; however, scattering or protruding aortic plaques are hard to detect by conventional modalities. NOGA can demonstrate SRAPs, including scattering or protruding plaques safely [4]. SRAPs are identified in 80.8 % of patients with or suspected coronary artery disease [5]. However, patients having SRAPs rarely advance to CES. Atheromatous materials and CCs from SRAPs scatter for years [7]. We previously reported that free CCs were obtained from the femoral artery next day after onset in a patient with spontaneous CES [8]. Thus, the continuous scattering of many SRAPs, including CCs, may cause CES. NOGA showed 23 SRAPs (Fig. 3B and C). According to the registry of NOGA in patients with or suspected coronary artery disease, the median number of SRAPs is one [9]. Recently, we reported that CCs were detected in 94 of 260 SRAPs (36 %), and the count of CCs was 11,590 [2386, 30, 113] per 10 mL (median, interquartile range) in CC-positive SRAP samples [6]. The amount of 6455/10 mL of CCs was between 25 percentiles to the median; however, the patient had five puff-chandelier ruptures, and the area of puff-chandelier rupture was wide. CCs were detected in 3 of 5 SRAPs (60 %). This might be a high risk for CES. Our report demonstrated aortic plaques with computed tomography and NOGA. Computed tomography showed remarkable atherosclerosis; however, it did not show scattering plaques.
CCs may play a pivotal role in activating innate inflammation, including nucleotide-binding oligomerization domain-like receptor, pyrin domain-containing (NLRP)3 inflammasomes, which regulate caspase-1 activation and the subsequent processing of inflammatory cytokines in atherosclerotic lesions. CCs were shown to be the main trigger of IL-6 production through innate inflammatory response in human SRAPs in situ [7]. CCs and CCs-induced NLRP3 inflammasome/inflammatory cytokines were expected to be scattered from SRAPs and might cause inflammation in his limbs, as shown previously [10]. CCs risk stratification according to SRAPs and CCs detected by NOGA may be the next issue. Finally, this patient also had many risk factors for CES, so it cannot be denied that iatrogenicity due to these procedures played a role in the onset of CES. We always need to consider the benefits and drawbacks of interventions carefully.
The following is the supplementary data related to this article.
A series of computed tomography, computed tomography angiography, and angioscopic video. Puff-chandelier rupture with a flap-like lesion is observed.
Patient permission/consent statement
The study was approved by the local ethics committee of Osaka Gyoumeikan Hospital, and the patient provided written consent.
Funding
None
Funding support and author disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
References
- 1.Kronzon I., Saric M. Cholesterol embolization syndrome. Circulation. 2010;122:631–641. doi: 10.1161/CIRCULATIONAHA.109.886465. [DOI] [PubMed] [Google Scholar]
- 2.Ghanem F., Vodnala D., Kalavakunta J.K., Durga S., Thormeier N., Subramaniyam P., et al. Cholesterol crystal embolization following plaque rupture: a systemic disease with unusual features. J Biomed Res. 2017;31:82–94. doi: 10.7555/JBR.31.20160100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ozkok A. Cholesterol-embolization syndrome: current perspectives. Vasc Health Risk Manag. 2019;15:209–220. doi: 10.2147/VHRM.S175150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Komatsu S., Ohara T., Takahashi S., Takewa M., Minamiguchi H., Imai A., et al. Early detection of vulnerable atherosclerotic plaque for risk reduction of acute aortic rupture and thromboemboli and atheroemboli using non-obstructive angioscopy. Circ J. 2015;79:742–750. doi: 10.1253/circj.CJ-15-0126. [DOI] [PubMed] [Google Scholar]
- 5.Komatsu S., Yutani C., Ohara T., Takahashi S., Takewa M., Hirayama A., et al. Angioscopic evaluation of spontaneously ruptured aortic plaques. J Am Coll Cardiol. 2018;71:2893–2902. doi: 10.1016/j.jacc.2018.03.539. [DOI] [PubMed] [Google Scholar]
- 6.Komatsu S., Yutani C., Takahashi S., Takewa M., Iwa N., Ohara T., et al. Cholesterol crystals as the main trigger of interleukin-6 production through innate inflammatory response in human spontaneously ruptured aortic plaques. J Atheroscler Thromb. 2023 doi: 10.5551/jat.64098. Apr 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Takahashi S., Komatsu S., Yutani C., Takewa M., Ohara T., Kodama K. Serial observation of aortic puff-chandelier rupture for 2 years by non-obstructive general angioscopy. Circ J. 2022;86:476. doi: 10.1253/circj.CJ-21-0767. [DOI] [PubMed] [Google Scholar]
- 8.Komatsu S., Yutani C., Takewa M., Takahashi S., Kodama K. Detecting free cholesterol crystals in a patient with spontaneous cholesterol embolization syndrome. JACC Case Rep. 2020;2:615–618. doi: 10.1016/j.jaccas.2019.12.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kojima K., Komatsu S., Kakuta T., Fukamachi D., Kimura S., Fujii H., et al. Aortic plaque burden predicts vascular events in patients with cardiovascular disease: the EAST-NOGA study. J Cardiol. 2022;79:144–152. doi: 10.1016/j.jjcc.2021.08.028. [DOI] [PubMed] [Google Scholar]
- 10.Komatsu S., Yutani C., Takahashi S., Takewa M., Ohara T., Hirayama A., et al. Debris collected in-situ from spontaneously ruptured atherosclerotic plaque invariably contains large cholesterol crystals and evidence of activation of innate inflammation: insights from non-obstructive general angioscopy. Atherosclerosis. 2022;352:96–102. doi: 10.1016/j.atherosclerosis.2022.03.010. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
A series of computed tomography, computed tomography angiography, and angioscopic video. Puff-chandelier rupture with a flap-like lesion is observed.