
Figure 3.
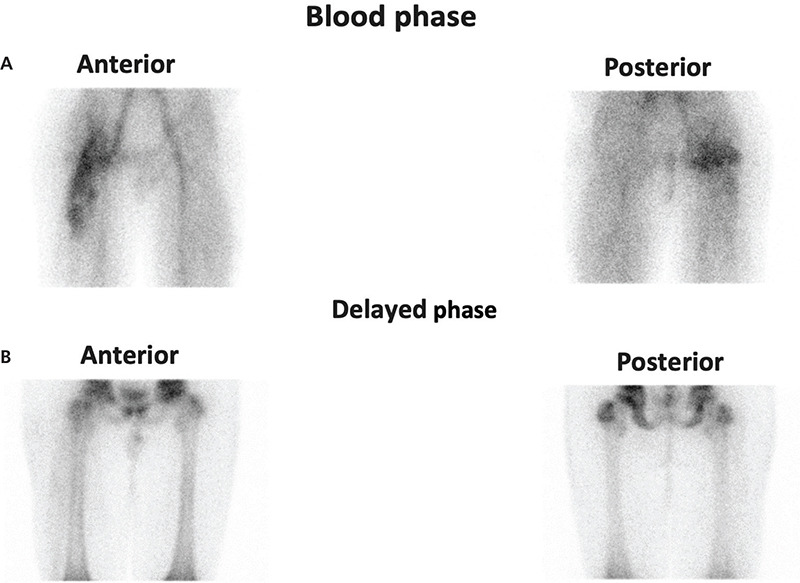
Triphasic Tc-99m-methylene diphosphonate bone scan of the upper part of lower extremities demonstrated heterogeneously increased vascularity and perfusion of the right proximal half of the femur and the right acetabular region (A). A minimal reduction in activity accumulation was observed in the right hip epiphyseal line compared to the contralateral side. However, there was no increased activity accumulation at nearby pelvic bones and the right femur on delayed images (B). An excisional biopsy was performed for the mass measuring 35x25x10 mm with a soft consistency, creamy white and brown in places. The diagnosis of inflammatory myofibroblastic tumors (IMT) was confirmed histopathologically with a large number of lymphoplasmacytic cells, destroying muscle structure. No significant mitotic activity and necrosis were observed. Ki-67 positive tumor cells accounted for approximately 5-6%. IMT is a neoplasm of intermediate biological potential with partial local invasion and recurrence, but they rarely metastasize (1). IMTs can occur in various systems including central nervous system, internal organs, and extremities (2,3). Older children can sometimes be affected by this disease, and it has also been reported as a very rare condition (4). The specific pathogenesis of IMT is unknown, while various infections, inflammatory and autoimmune diseases, and trauma are among the most commonly suspected etiologies of the disease. The clinical presentation of IMT varies depending on the anatomical location and it sometimes mimics lymphoma (5). Patients generally present with general inflammatory symptoms such as fever, weight loss, pain, and malaise which may also raise suspicion of lymphoproliferative malignancies. CT and MR are the most commonly used imaging modalities when evaluating of IMTs. In most cases, a histological examination must be carried out for a reliable diagnosis. 18F-FDG PET/CT scan is useful for detection of primary tumor, local recurrence, treatment response, and distant metastasis (6,7). Histopathologically our case showed low mitotic activity and indicates the uptake of 18F-FDG, mainly related to high glucose utilization of the inflammatory cells contained in the tumor. PET/CT helps in delineating the tumor burden to guide surgery and thus prevents the damage to normal anatomical structures. The best treatment strategy for this type of tumor is complete resection if achieved surgically. Due to the high 18F-FDG avidity of the tumor, the PET/CT scan is also useful to identify local recurrence after resection of the primary tumor.