
FIGURE 2.
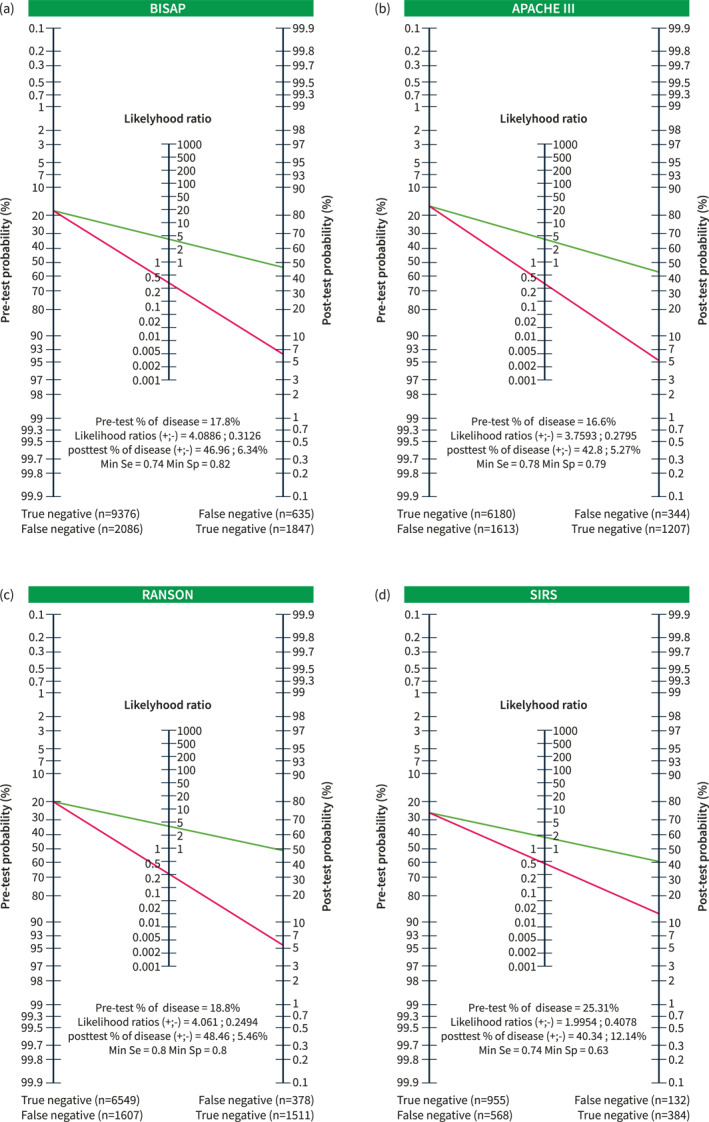
Panel (a) performance of the Bedside Index for Severity in Acute Pancreatitis (BISAP) score in 42 studies with a pre‐test probability of 17.8% and positive and negative likelihood ratios of 4.09 and 0.31, respectively, and the post‐test probability of severe acute pancreatitis (SAP) is 47% when BISAP is positive and 6% when it is negative. With this performance, only 1847 of the 2482 patients who eventually developed SAP would have been correctly identified as true positives, with 635 false negatives; only 9376 of the 11,462 patients experiencing non‐severe AP would have been correctly classified, with 2086 having a false positive prediction of SAP. Panel (b) performance of the Acute Physiology and Chronic Health Examination (APACHE)‐II score in 30 studies with a pre‐test probability of 16.6% and positive and negative likelihood ratios of 3.76 and 0.28, respectively, and the post‐test probability of SAP is 43% when APACHE is positive and 5% when it is negative. With this performance, only 1207 of the 1551 patients who eventually developed SAP would have been correctly identified as true positives, with 344 false negatives, and only 6180 of the 7793 patients experiencing non‐severe AP would have been correctly classified, with 1613 having a false positive prediction of SAP. Panel (c) performance of the Ranson score in 27 studies with a pre‐test probability of 18.8% and positive and negative likelihood ratios of 4.06 and 0.25, respectively. The post‐test probability of SAP is 48% when Ranson is positive and 5% when it is negative. With this performance, only 1511 of the 1889 patients who eventually developed SAP would have been correctly identified as true positives, with 378 false negatives; only 6549 of the 8156 patients experiencing non‐severe AP would have been correctly classified, with 1607 having a false positive prediction of SAP. Panel (d) performance of the Systemic Inflammatory Response Syndrome (SIRS) score in eight studies with a pre‐test probability of 25.3% and positive and negative likelihood ratios of 1.99 and 0.41, respectively, with a post‐test probability of SAP of 40% when SISR was positive and 12% when it was negative. With this performance, only 384 of the 516 patients who eventually developed SAP would have been correctly identified as true positives, with 132 false negatives, and only 955 of the 1523 patients with non‐severe AP would have been correctly classified, with 568 having a false positive prediction of SAP.