
Figure 9.
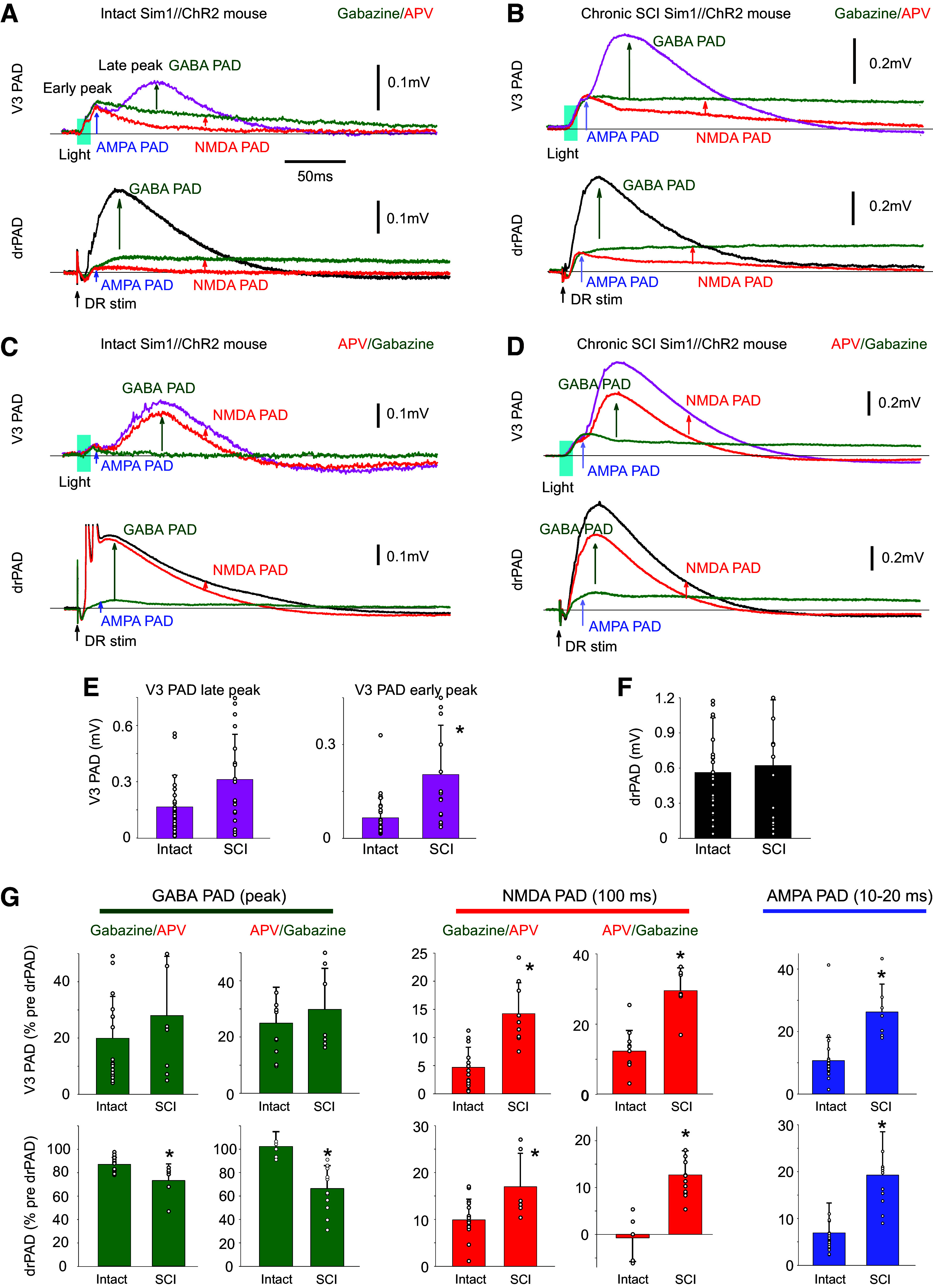
Chronic spinal cord injury (SCI) increases NMDA and AMPA PAD while reducing GABA PAD. A: changes in V3 PAD and drPAD recorded in S3 DR (as detailed in Fig. 6, B and D) with sequential application of gabazine and APV in Sim1//ChR2 mouse (50 µM each). GABA and NMDA PAD measured by drug-induced reductions, and AMPA PAD measured as remaining PAD in both drugs. V3 PAD and drPAD evoked by a brief light or DR stimulation, respectively (as detailed in Fig. 6, B and D). B: same as A, but in Sim1//ChR2 mouse with an S2 spinal transection 1 mo previously (chronic SCI). C and D: same as A and B, but with APV added before gabazine to estimated resting state NMDA PAD. E and F: group averages of changes in PAD with SCI, with significant change (*) in early peak of V3 PAD, but not the late peak of V3 PAD or drPAD, P < 0.05, n = 31 and 15 from 6 control and 6 SCI mice. G: group averages of changes in GABA PAD (at peak), NMDA PAD (recorded at 100 ms latency), and AMPA PAD (recorded at peak between 10 and 20 ms) with SCI, *significant change, P < 0.05, n = 20 and 6–9 roots tested with gabazine given first, without and with SCI, respectively, and n = 12 and 6–9 roots with APV given first, without and with SCI, respectively; from 4–6 mice each condition. All changes with drugs normalized by predrug drPAD peak. NMDA, N-methyl-d-aspartate; PAD, primary afferent depolarization.