

Abstract
Background
Treatments currently available for ceruminous gland tumors include surgery and radiation therapy, which come with high financial costs and frequent complication and recurrence rates.
Hypothesis
To evaluate the treatment, response, complication, and recurrence of ceruminous gland tumors confirmed with biopsy and ablated using CO2 laser.
Methods
Retrospective review of medical records from Iowa State University and the University of Illinois between January 1, 2016 and December 31, 2021. Electronic medical records were evaluated for a histopathologically confirmed ceruminous gland tumor via video‐otoscopic aided biopsy and subsequent CO2 laser ablation. Signalment, tumor type, size, location within the ear canal, length of time tumor was present before presentation, advanced imaging, and follow‐up including recurrence were assessed.
Results
Fourteen ceruminous gland adenomas (4 dogs, 10 cats) and 12 ceruminous gland adenocarcinomas (7 dogs, 5 cats) were identified. Bacterial otitis externa was present in 4/26 (15%) animals. Recurrence was identified in 1/14 (7%) ceruminous gland adenomas and 1/12 (8%) ceruminous gland adenocarcinomas.
Conclusions and Clinical Importance
Video‐otoscopic aided biopsy and CO2 laser ablation of ceruminous gland tumors in dogs and cats is a viable treatment option with low recurrence and complication rates with CO2 laser ablation.
Keywords: ceruminous adenocarcinoma, ceruminous adenoma, CO2 laser, ear tumor
Abbreviations
- CT
computed tomography
- TECABO
total ear canal ablation and bulla osteotomy
1. INTRODUCTION
Ceruminous gland tumors are the most common tumors identified in the external ear canal of dogs and cats. The most common malignant ear tumor in dogs and cats is ceruminous gland adenocarcinoma, while ceruminous gland adenoma is a frequent benign tumor of the ear. 1 , 2 Malignant tumors of the external ear canal are locally invasive in up to 67% of dogs and 88% of cats. 1 While ceruminous gland adenocarcinoma is usually locally invasive, it can metastasize to regional lymph nodes, lung, liver, and kidneys in rare cases. 3 Typical treatment options for these tumors are surgical removal of the ear canal or radiation therapy. Surgery has a recurrence rate for ceruminous gland adenocarcinoma of 25% with a total ear canal ablation and bulla osteotomy (TECABO) and 67% with lateral ear canal resection in cats. 4 Radiation therapy has a recurrence rate of 36%. 5 Complications associated with surgery can be mild, such as wound healing impairments, or more severe with Horner syndrome, facial nerve paralysis, and head tilt being encountered. These complications can vary from temporary to permanent, and range in occurrence from 5% to 56% of cases. 4 , 6 , 7 , 8 , 9
Both surgery and radiation therapy can be cost prohibitive. Additionally, because of the potential complications and recurrence rate, some owners decline these treatment options and elect palliative care. Without therapy for the purpose of intent to cure, the inevitable reality is local invasion or metastasis. Surgery is normally recommended for treatment of ceruminous gland tumors. The preferred surgery is a TECABO and this results in the majority of animals having partial hearing or complete deafness in the affected ear because of the entire external ear canal being removed. 7 Animals with tumors and otitis externa will clinically have decreased hearing ability in the affected ear(s) on presentation. The loss of the external ear canal and permanent deafness can be concerning for owners and is the reason some owners decline surgery. Therefore, an alternative option, which can be of lower cost and retain the full function of the ear canal is ideal.
CO2 laser ablation has been attempted in some ear tumors as an alternative therapy with the intent to preserve the external ear canal. This study aimed to evaluate cases that have been treated with this therapy for ceruminous gland tumors and analyze complication and recurrence rates. Evaluation of other factors, which could have altered the success or failure of therapy, were also investigated. It was hypothesized that if the tumor was determined to be within the external ear canal via computed tomography (CT) that biopsy of the tumor followed by video‐otoscopic aided CO2 laser ablation of the remnant tissue would provide an acceptable treatment outcome.
2. MATERIALS AND METHODS
2.1. Study design
This was a retrospective review of electronic medical records performed at 2 veterinary teaching hospitals in central United States. Electronic medical records were searched at Iowa State University and the University of Illinois between January 1, 2016 and December 31, 2021 for dogs and cats diagnosed with ceruminous gland adenoma and ceruminous gland adenocarcinoma on histopathology. Medical records were searched for the terms ceruminous tumor, ceruminous gland tumor, ceruminous adenoma, and ceruminous adenocarcinoma. Additional inclusion criteria included video‐otoscopic evaluation of the external ear canal with biopsy for histopathology, video‐otoscopic aided CO2 laser ablation of remnant tissue, and follow‐up evaluation of at least 3 months to monitor for secondary complications and recurrence.
2.2. Review of medical records
The age and sex of the animal along with tumor type, size of the tumor submitted for histopathology, location within the ear canal, length of time mass was noted before to presentation, advanced imaging, and follow‐up including recurrence were assessed based on medical records. Any additional underlying disease or factors were also recorded. Follow‐up evaluations for regrowth or post‐operative complications were performed by the investigators or by the referring veterinarian.
2.3. Procedure
The procedure included video otoscopic evaluation of the external ear to identify the location and extent of the tumor. All tumors were then grasped at the base of the tumor with Storz biopsy forceps through the working channel of the video otoscope and submitted for histopathology. After the biopsy of the tissue was performed, remnants of the tumor were present in all cases along the wall of the ear canal. An Aesculight CO2 laser set to a range of 10 to 20 Watts in the continuous wave mode was then used to ablate the remnant tissue through the working channel of the video otoscope, as seen in Figure S1. Two CO2 laser tips were used including the 40 mm hollow semi‐rigid metal tip with a 0.8 mm diameter (Figure S1A,B) or a 175 mm long fiber optic tip with a 0.8 mm diameter (Figure S1C). Either the MedRx video otoscope (Figure S1A) or the Storz HD video otoscope (Figure S1B,C) were used to fully visualize the tissue that was being ablated with the CO2 laser during the procedure. CO2 laser ablation was performed until all remnant tissue was removed or until the cartilage was reached. The cumulative amount of CO2 laser time varied from 30 seconds to 3 minutes depending on the settings of the CO2 laser, amount of remnant tissue left, and size of the tumor. Intermittent flushing of the external ear canal with saline or wiping of the tissue with a saline‐soaked cotton‐tipped applicator was performed to clean the tissue and remove any char.
2.4. Statistical analysis
The following data was evaluated statistically: species; age of animal; type of ceruminous gland tumor; size of the tumor; length of time tumor was present before presentation; location of tumor; recurrence of tumor; follow‐up time in months; post‐procedure infection; and whether a CT was performed before procedure.
All continuous data was evaluated for normality with the Shapiro‐Wilk test. Continuous data included age in years, size in mm, time present in months, and follow‐up in months. If normally distributed, variables were reported with mean ± SD, and non‐normally distributed continuous variables were reported as median (range). The continuous data was evaluated with either independent samples T test, if normally distributed, or Wilcoxon Signed Rank Test, if non‐normally distributed. Nominal data included species, type of ceruminous gland tumor, location, CT performed, and recurrence. The nominal data was evaluated with Chi‐square test or Fisher exact test, if any variable was less than 5. Statistical significance was noted with P < .05. IBM SPSS Statistics version 27 (Armonk, NY: IBM Corp) was used for all statistical evaluation.
2.5. Ethical statement
This was a retrospective review of medical records using hospital data from 2 veterinary teaching hospitals. Client consent was obtained upon presentation to either institution to use clinical data and medical records for research purposes.
3. RESULTS
3.1. Signalment
A total of 26 medical records were identified, including 11 dogs and 15 cats, from January 1, 2016 to December 31, 2021. The dogs were comprised of 5 neutered males and 6 spayed females, while the cats encompassed 8 neutered males and 7 spayed females. The age for all animals was 9.69 years ±3.0, with dogs being 9.55 years ±3.3, and cats being 9.8 years ±3.0. Dog breeds included 3 mixed breed dogs, 2 Cocker spaniels, 2 Shih Tzu's, and 1 each of French bulldog, English mastiff, beagle, and English springer spaniel. Cat breeds included 12 domestic short hair cats and 1 each of domestic medium hair, domestic long hair, and Siamese.
3.2. Tumors
There was a total of 14 ceruminous adenomas (4 dogs, 10 cats) and 12 ceruminous adenocarcinomas (7 dogs, 5 cats) with no statistical difference between species and type of ceruminous gland tumor (P = .13). Evaluating the age and type of ceruminous gland tumor revealed no statistical significance (P = .77) with the data shown in Table 1. Tumors were noted before presentation for a mean amount of time of 4 months (range 1‐24 months; Table 1). No statistical difference was detected when evaluating the type of ceruminous gland tumor and the amount of time the tumor was noted before the presentation (P = .08). Size of the tumors was determined on histopathology after removal of the mass. The median size was 6.25 mm (range 2‐25 mm). No statistical significance was detected when evaluating the size of the tumor and type of ceruminous tumor (P = .052) with the sizes for each tumor type noted in Table 1. Ceruminous gland tumors were located throughout the external ear canal, but statistical significance was identified when comparing the type of ceruminous gland tumor with the location (P = .04). Locations are shown in Table 2 with a higher incidence of ceruminous gland adenomas located in the horizontal ear canal compared with a higher incidence of ceruminous gland adenocarcinomas being noted at the entrance of the external ear canal.
TABLE 1.
Data for age, time present before presentation, size, follow up, and recurrence for all ceruminous gland tumors, ceruminous gland adenomas, and ceruminous gland adenocarcinomas.
| Age | Tumor before presentation | Size | Follow up | Recurrence | |
|---|---|---|---|---|---|
| All ceruminous gland tumors | 9.69 ± 3.0 years | 4 months (1‐24 months) | 6.25 mm (2‐25 mm) | 16.5 months (3‐50 months) | 2/26 = 8% |
| Ceruminous gland adenomas only | 9.78 ± 2.3 years | 3.9 months (1‐8 months) | 4 mm (2‐20 mm) | 19 months (3‐50 months) | 1/14 = 7% |
| Ceruminous gland adenocarcinomas only | 10.78 ± 3.3 years | 11.2 months (1‐24 months) | 10 mm (2‐25 mm) | 22 months (10‐40 months) | 1/12 = 8% |
TABLE 2.
Location within the ear canal for ceruminous gland adenomas and ceruminous gland adenocarcinomas.
| Entrance of external ear canal | Vertical ear canal | Transition from vertical to horizontal | Horizontal ear canal | |
|---|---|---|---|---|
| Ceruminous gland adenoma | 2/14 | 3/14 | 2/14 | 7/14 |
| Ceruminous gland adenocarcinoma | 6/12 | 1/12 | 3/12 | 2/12 |
3.3. Advanced imaging
Most of the cases, 18/26, were evaluated via a CT scan with contrast to assess for invasion and local metastasis of the tumor. None of the cases had metastasis noted and all tumors that underwent a CT were found to be contained within the ear canal with no invasion through the cartilage identified.
3.4. Post‐operative therapy
There were a variety of post‐operative therapies used. The most common therapy was topical antimicrobials to treat concurrent bacterial infections in 22/26 cases. Silver sulfadiazine containing products were used in 9/26 cases. Topical or systemic glucocorticoids for inflammation and pruritus were used in 13/26 cases.
3.5. Follow‐up and complications
The median follow‐up time was 16.5 months (range 3‐50 months). Post‐operative complications were limited; 4 dogs developed otitis externa in the 30 days after the procedure (4/26, 15%; P = .02).
3.6. Recurrence
There was recurrence in 2 of the cases. One of the cases was a ceruminous adenocarcinoma, which did not have a CT performed before the procedure to evaluate for invasion. Roughly 7 months post‐operative, a mass was noted caudal to the left ear. Fine needle aspiration was consistent with ceruminous gland adenocarcinoma, and it was presumed to be local extension of the mass that was previously ablated with CO2 laser.
The other case was a ceruminous adenoma that was removed by another veterinarian. When it presented 2 weeks after removal for video‐otoscopic aided CO2 laser ablation to prevent regrowth, it was difficult to determine where the base of the mass was previously positioned. The ceruminous adenoma recurred about 2 months later. An additional CO2 laser ablation of the ceruminous adenoma was performed after a CT, and no recurrence was noted through the follow‐up time. In total, there was a recurrence rate of ceruminous gland adenoma of 7% (1/14) compared with ceruminous gland adenocarcinoma of 8% (1/12) with no statistically significant difference (P = .72).
4. DISCUSSION
This study showed that biopsy for histopathological confirmation followed by video‐otoscopic aided CO2 laser ablation can be used as a successful treatment option for dogs and cats with ceruminous gland tumors, no matter the location in the external ear canal. When comparing ceruminous gland adenomas and ceruminous gland adenocarcinomas, there was no difference in recurrence rates. When CT scan preceded surgery, all of the cases had tumors contained within the external ear canal previous to video‐otoscopic aided CO2 laser ablation. The ceruminous gland adenocarcinoma case, which recurred, did not have advanced imaging performed. It was assumed to be locally invasive, with a new lesion noted 7 months later, caudal to the ear. If a CT was completed before the CO2 laser ablation, the local invasion through the cartilage of the external ear canal could have been noted. The chance of success with CO2 laser ablation would have been low in this case. Surgery or radiation therapy would have been a better option for this cat because of the invasiveness and extension of the tumor. The recorded size of this recurrent tumor at the time of initial removal was 10 mm in size, which is the median for ceruminous gland adenocarcinomas. Additionally, the ceruminous gland adenoma that recurred was only 6 mm in size, which is also close to the median size (4 mm) for ceruminous gland adenomas. Therefore, the size of the tumor is not considered a factor for recurrence. Infiltration through the cartilage in this case was suspected, which led to recurrence. It is the authors' opinion that if the base of the mass is attached to less than 1/3 of the circumference of the wall of the ear canal, it is a good candidate for CO2 laser ablation. Performing CO2 laser ablation to tissue larger than 1/3 of the ear canal circumference will likely heal in with strictures, so surgery would be the recommended treatment in those cases.
This study showed that recurrence of ceruminous gland adenocarcinomas was low at 8% when combining biopsy and CO2 laser ablation, which is lower than reported with surgery (in cats) of 25% to 50% and radiation therapy (in dogs and cats) of 36%. 4 , 5 , 9 While biopsy was performed to obtain a diagnosis with histopathology and remove a larger piece of the tumor, CO2 laser ablation was believed to be the most important part of the procedure to remove residual microscopic neoplastic cells. Post‐operative complications were minimal with this approach, with only 4 dogs (15%) developing otitis externa in the immediate follow‐up period and they all resolved with treatment. Most of these cases received topical antimicrobials post‐operatively, which likely reduced the incidence of post‐operative otitis externa. At the same time, 3/4 dogs that developed otitis externa post‐operatively had underlying atopic dermatitis, making them more susceptible to otitis externa in general. The chance of otitis externa is presumed to be higher with no post‐operative intervention and a greater risk with CO2 laser compared with TECABO. Traditional surgical complications are reported to range from mild wound healing issues, to more severe, with Horner syndrome and facial nerve paralysis. Most of these surgical complications were reported to be temporary in 42% to 82% of cases, but there is a chance of permanent damage described in 8% to 28% of cases. 7 , 8 , 9 The reason for low recurrence and low complication rates in this study, could be because of case selection criteria for video‐otoscopic aided CO2 laser ablation. All cases with advanced imaging were reviewed to see whether biopsy and CO2 laser ablation was an option, or if surgical removal of the ear canal and tumor were indicated. Surgery and radiation therapy are preferred treatments for more severe and locally aggressive tumors of the ear canal which infiltrate through the cartilage of the ear canal. This case selection could inherently increase the risk of recurrence and complications with surgery and radiation therapy.
CO2 laser is a prevailing surgical method for treating cutaneous lesions throughout the body, but a minimal amount of literature is available regarding ear diseases. Ceruminous cystomatosis has been reported to be treated with CO2 laser, but these lesions are usually at the entrance of the external ear canal or on the pinnae. 10 Another condition where CO2 laser ablation was recently described as a treatment option was chronic proliferative otitis externa. However, this condition was again confined to the entrance of the external ear canal. 11 Because of the location of these types of lesions, they are easy to access with a CO2 laser by itself. There is no literature available detailing treatment within the external ear canal utilizing video‐otoscopic aided CO2 laser ablation. It is important to use the highest quality video otoscope possible, as there is a disparity in image quality between devices as shown in Figures 1 and 2. Another alternative that has been attempted to remove ceruminous adenomas is the diode laser through a video otoscope. Unfortunately, diode lasers cause excessive thermal injury, resulting in extreme tissue trauma and a higher likelihood of stricture formation. 12
FIGURE 1.
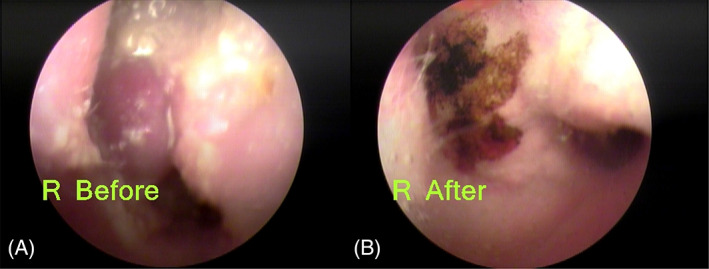
Images after traction removal of the ceruminous gland adenocarcinoma and (A) before and (B) after treatment with the semi‐rigid metal laser tip through the MedRx video otoscope.
FIGURE 2.
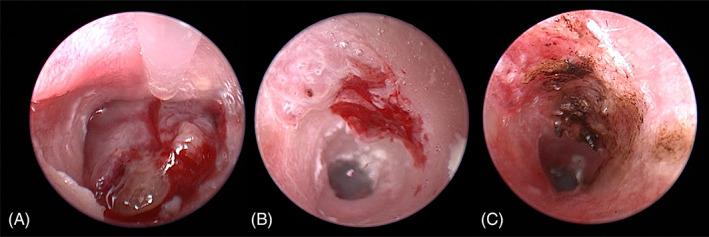
Images of the ceruminous gland adenocarcinoma (A) before traction removal, (B) after traction removal with remnants of tissue left, and (C) after treatment with fiber optic laser tip through the HD Storz video otoscope.
Limitations of this study are inherent to the retrospective nature of the investigation. Limitations include a small sample size, slight variation in technique, and non‐standardized post‐operative management since 3 investigators performed these procedures. This variability prevented further evaluation of the impact of topical or systemic post‐operative therapies. Additionally, some procedures were performed with different video otoscopes and different CO2 laser equipment as seen in Figure S1.
This study describes a viable alternative for the management of ceruminous tumors that is less invasive with lower complication rates post‐operatively than traditional modalities. Performing a CT to determine the invasiveness of the tumor is recommended for planning purposes. If the tumor is confined to the ear canal with no infiltration through the cartilage and not attached to greater than 1/3 of the ear canal circumference, CO2 laser ablation is a viable treatment option. When infiltration and extension through the cartilage are noted, then surgery or radiation therapy is the recommended treatment option. In the future, a prospective study with a larger sample size would be ideal.
CONFLICT OF INTEREST DECLARATION
Dr. Pieper has received speaker honoraria from Aesculight/VetScalpel. No other authors declare a conflict of interest.
OFF‐LABEL ANTIMICROBIAL DECLARATION
Authors declare no off‐label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
Authors declare no IACUC or other approval was needed.
HUMAN ETHICS APPROVAL DECLARATION
Authors declare human ethics approval was not needed for this study.
Supporting information
Figure S1. A variety of devices with the CO2 laser and video otoscope. (A) MedRx video otoscope with a semi‐rigid metal laser tip inserted through the working channel. (B) HD Storz video otoscope with semi‐rigid metal laser tip inserted through the working channel. (C) HD Storz video otoscope with fiber optic laser tip inserted through the working channel.
ACKNOWLEDGMENT
Open access funding provided by the Iowa State University Library.
Pieper JB, Noxon JO, Berger DJ. Retrospective evaluation of ceruminous gland tumors confined to the external ear canal of dogs and cats treated with biopsy and CO2 laser ablation. J Vet Intern Med. 2023;37(6):2385‐2390. doi: 10.1111/jvim.16873
REFERENCES
- 1. London C, Dubilzeig R, Vail D, et al. Evaluation of dogs and cats with tumors of the ear canal: 145 cases (1978‐1992). J Am Vet Med Assoc. 1996;208:1413‐1418. [PubMed] [Google Scholar]
- 2. Moisan P, Watson G. Ceruminous gland tumors in dogs and cats: a review of 124 cases. J Am Anim Hosp Assoc. 1996;32:448‐452. [DOI] [PubMed] [Google Scholar]
- 3. Cotchin E. Skin Tumours of cats. Res Vet Sci. 1961;2:353‐364. [Google Scholar]
- 4. Marino D, MacDonald J, Matthiesen D, et al. Results of surgery in cats with ceruminous gland adenocarcinoma. J Am Anim Hosp Assoc. 1994;30:54‐58. [Google Scholar]
- 5. Théon AP, Barthez PY, Madewell BR, Griffey SM. Radiation therapy of ceruminous gland carcinomas in dogs and cats. J Am Vet Med Assoc. 1994;205:566‐569. [PubMed] [Google Scholar]
- 6. Marino D, MacDonald J, Matthiesen D, et al. Results of surgery and long‐term follow‐up in dogs with ceruminous gland adenocarcinoma. J Am Anim Hosp Assoc. 1993;29:560‐563. [Google Scholar]
- 7. Spivack R, Elkins A, Moore G, et al. Postoperative complications following TECA‐LBO in the dog and cat. J Am Anim Hosp Assoc. 2013;49:160‐168. [DOI] [PubMed] [Google Scholar]
- 8. Smeak D, Dehoff W. Total ear canal ablation – clinical‐results in the dog and cat. Vet Surg. 1986;15:161‐170. [Google Scholar]
- 9. Bacon N, Gilbert R, Bostock D, et al. Total ear canal ablation in the cat: indications, morbidity and long‐term survival. J Small Anim Pract. 2003;44:430‐434. [DOI] [PubMed] [Google Scholar]
- 10. Corriveau LA. Use of a carbon dioxide laser to treat ceruminous gland hyperplasia in a cat. J Feline Med Surg. 2012;14:413‐416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Aslan J, Shipstone M, Mackie J. Carbon dioxide laser surgery for chronic proliferative and obstructive otitis externa in 26 dogs. Vet Dermatol. 2021;32:262‐272. [DOI] [PubMed] [Google Scholar]
- 12. Usui R, Okada Y, Fukui E, et al. A canine case of otitis media examined and cured using a video otoscope. J Vet Med Sci. 2015;77:237‐239. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. A variety of devices with the CO2 laser and video otoscope. (A) MedRx video otoscope with a semi‐rigid metal laser tip inserted through the working channel. (B) HD Storz video otoscope with semi‐rigid metal laser tip inserted through the working channel. (C) HD Storz video otoscope with fiber optic laser tip inserted through the working channel.