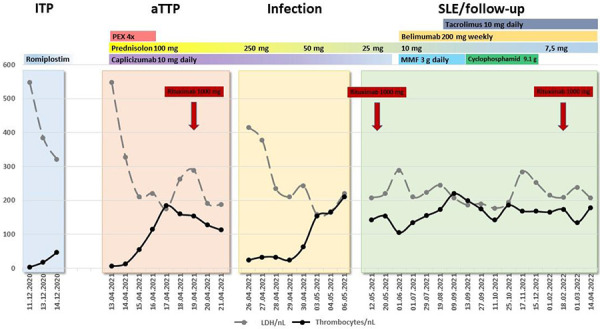
Figure 2. Clinical course demonstrating four different phases of thrombocytopenia, underlying etiologies and chosen therapies. The clinical course of the patient could be grouped into four different phases dominated by thrombocytopenia: The first phase (light blue) represented her last idiopathic immune thrombocytopenia (ITP) flare in December 2020, resulting in romiplostim therapy due to refractory disease. At that timepoint, autoimmune hemolytic anemia (AIHA) as well as microangiopathic hemolytic anemia (MAHA) were not known to exist, but increased lactate dehydrogenase levels may point towards a missed hemolysis. The second phase started in April 2021 (orange) and was dominated by the newly diagnosed acquired thrombotic thrombocytopenic purpura (aTTP), introducing plasma exchange and caplacizumab as well as rituximab in the patients’ therapeutic regimen. The third thrombocytopenic phase (yellow) superimposed aTTP and was due to overt upper respiratory tract infection with blastic cells in peripheral blood smears. It was mainly resolved by antibiotic treatment and increased doses of prednisolone. The fourth phase (light green) reflected the phase of SLE diagnosis and treatment as well as aTTP follow-up with stable thrombocyte counts and resolved ITP, AIHA, and MAHA.