

Abstract
Background
After the transfusion of RhD-positive red blood cell (RBC)-containing products to an RhD-negative woman of childbearing potential (WCP) during trauma resuscitation, there are several events that must occur for that WCP to have a future pregnancy affected by hemolytic disease of the fetus and newborn (HDFN). This study identified and quantitated the frequency of a novel event in the sequence from RhD-positive transfusion during trauma resuscitation to an HDFN outcome, that is, the development of a high titer anti-D among women who were D-alloimmunized.
Methods
The transfusion service records at one maternity hospital were searched to locate all anti-D titers that had been performed on pregnant women between 1996 and 2022. The highest titer score during each pregnancy was recorded for this study. The critical titer threshold at this institution was ≥16. Passive anti-D caused by Rh immunoglobulin were excluded from analysis.
Results
There were 97 pregnancies in 85 patients who had an immune-stimulated anti-D; in 60 of 97 (62%) pregnancies, the highest titer score was ≥16. There were 12 patients who had titers performed in two pregnancies during the study period; the correlation between the maximum titer in each pregnancy was not statistically significant (Spearman rank correlation r=0.42, p=0.17).
Conclusion
In this single center study, 62% of D-alloimmunized pregnant women had a high titer antibody. When considering all of the events that must occur for HDFN to happen, the rate of perinatal mortality was calculated to be 0.04% and the rate of perinatal death or serious adverse event from HDFN was 0.24%.
Keywords: transfusion, red blood cells, pregnancy
Introduction
The limited supply of RhD-negative red blood cell (RBC)-containing products in some regions has resulted in the transfusion RhD-positive units to injured RhD-negative women of childbearing potential (WCP) during emergent trauma resuscitation. The D-alloimmunization risk in this setting ranges from 7.8% to 42.7%.1 2 The main consequence from D-alloimmunization in this patient population is the risk (0.3% to 6% depending on the severity of HDFN outcome and the nature of the predictive model) of a future pregnancy being affected by hemolytic disease of the fetus and newborn (HDFN).3 4 However, D-alloimmunization is only one of myriad events that must occur for a future pregnancy to be affected by HDFN (figure 1).3 5 6 One novel factor that has to date not been considered when calculating the probability of HDFN developing after the transfusion of RhD-positive blood products to RhD-negative WCPs during trauma resuscitation is what proportion of pregnant, anti-D-alloimmunized WCPs will develop an antibody that has risen above a critical titer threshold, for example, ≥16, such that additional monitoring for HDFN would occur during her pregnancy. This study analyzed the frequency at which pregnant women with anti-D developed a high titer antibody at one large maternity hospital.
Figure 1.

Swiss cheese model demonstrating the events that must occur for hemolytic disease of the fetus and newborn (HDFN) to occur after the transfusion of RhD-positive red blood cell-containing blood products to an RhD-negative woman during trauma resuscitation and the probability of occurrence of each event. The light colored and textured Swiss cheese slice (Event 5) represents the novel contribution to the HDFN risk equation presented in this study. See text for explanation of the probabilities listed next to each event. Modified and reprinted from reference6 with the kind permission of John Wiley and Sons.
Methods
To estimate the frequency at which pregnant women with anti-D developed a high titer antibody, the transfusion service records at one maternity hospital were searched to locate all anti-D titers that had been performed on pregnant women between 1996 and 2022. Between 1996 and 2015, the titers were performed by doubling dilution in saline tube (1 hour incubation of patient plasma and RBCs at 37°C followed by testing with anti-human globulin (AHG) reagent) and since 2015, the titers have been performed by doubling dilution using column agglutination technology (15-min incubation of patient plasma and RBCs at 37°C followed by testing with AHG reagent impregnated card). Reagent R2R2 RBCs were used in both periods. The titer itself is unitless and is reported as the inverse of the highest dilution that produces macroscopic RBC agglutination; for example, if the 1:32 patient plasma dilution produces macroscopic RBC agglutination but the 1:64 dilution does not produce RBC macroscopic agglutination, the titer is reported as 32. By protocol, a plasma sample from the first titer performed in each pregnancy was frozen until a subsequent titer was ordered. Then, an aliquot of the first sample was thawed and tested in parallel with the new sample to standardize reporting. If there were multiple titers performed during the pregnancy, the highest titer score during each pregnancy was recorded for this study. The protocol for this study was approved by the Quality Improvement Review Committee, a division of the University of Pittsburgh’s Institutional Review Board.
The transfusion service at this hospital electronically documents the issue of Rh immunoglobulin (RhIg) and these records were compared with the dates on which titers were performed for all women whose highest anti-D titer score was ≤4 because 4 is the highest titer attributable to RhIg.7 An anti-D was attributed to RhIg if RhIg was administered at any time during the pregnancy or if it was administered in a subsequent pregnancy; this minimized the chance that a passive anti-D would be considered a low-titer immune-stimulated antibody. On several occasions an early-pregnancy antibody screen revealed what appeared to be anti-D but the titer was zero and these cases were not included in the analysis.
Results
At this hospital there were 112 patients who had an anti-D titer measured during the study period (figure 2). There were 97 pregnancies in 85 patients who had an immune-stimulated anti-D, that is, anti-D not passively acquired through RhIg administration, with a maximum titer >0; in 60 of 97 (62%) pregnancies, the highest titer score was ≥16, defined at this institute as the critical titer threshold.8 There were 12 patients who had titers performed in two pregnancies during the study period and each of the pregnancies in these 12 women were counted individually when analyzing if a high titer anti-D had occurred; the correlation between the maximum titer in each pregnancy was not statistically significant (Spearman rank correlation r=0.42, p=0.17). In one patient’s first pregnancy the anti-D was attributable to RhIg and in the second pregnancy the titer was 8 so the second anti-D was considered an immune-stimulated antibody; it is not clear why she developed an immune antibody after receipt of RhIg during her first pregnancy, perhaps this represented a failure of the RhIg to prevent alloimmunization as has been previously described.9 10
Figure 2.
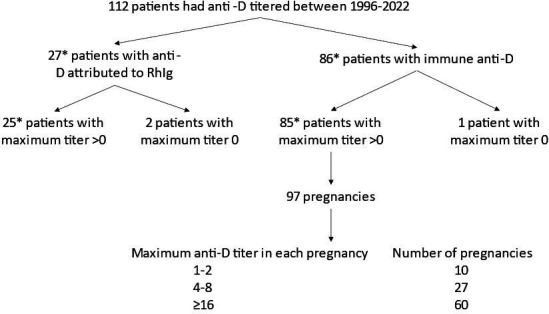
Stratification of the patients included in this study. *One patient had one pregnancy with an anti-D attributable to Rh immunoglobulin (RhIg) and a second pregnancy with an immune anti-D, hence she is counted twice.
Discussion
After the transfusion of RhD-positive RBC-containing products such as low titer group O whole blood (LTOWB) and RBC units to an injured RhD-negative WCP, there are several events that all must occur for her to have a future pregnancy affected by HDFN (figure 1). This study identified and quantitated the frequency of a novel event in the sequence from RhD-positive transfusion during trauma resuscitation to an HDFN outcome, that is, the development of a high titer anti-D among women who were D-alloimmunized. In this single center study, 62% of the pregnant women who were D-alloimmunized developed an antibody with a titer ≥16, which is the titer threshold at this institution for initiating closer monitoring of the pregnancy for HDFN. The corollary of this finding is that approximately 38% of women who are D-alloimmunized do not produce an antibody of a sufficiently high titer to routinely warrant closer monitoring for HDFN thereby lowering the probability that HDFN will occur among these women.
The sole intention of this pragmatic study was to determine the proportion of alloimmunized women who produced a high titer antibody that would prompt closer scrutiny of the pregnancy. To that end, this study did not evaluate whether HDFN occurred in the D-alloimmunized pregnancies or if the severity of HDFN correlated with the anti-D titer because it is known that anti-D can cause HDFN and that higher titer antibodies tend to cause worse disease.11–13 Furthermore, the mechanistic explanation of why some women develop high titer antibodies remains elusive and warrants further investigation in larger multicenter studies.
With the new data from this study on the frequency of developing a high titer anti-D, as well as the inclusion of several relevant events that were not considered when the original HDFN risk calculations were published,3 it is possible to more accurately estimate how frequently perinatal death or perinatal death and other severe outcomes of HDFN will occur after the transfusion of RhD-positive blood products to women during their resuscitation (figure 1). First, the woman must be of childbearing age and, according to 2021 US population census data,14 approximately 54% of the women who were 15 years of age or older in 2021 were between 15 and 49 years old. However, a broader view of the childbearing years would also account for the girls who were younger than 15 years old because, if they survive their trauma, they could become pregnant in the future. In 2021, 62% of all women and girls in the USA were between the ages of 0 and 49 years old and this higher percentage will be used in the overall HDFN risk calculation.14 In the USA, 15% of women will be RhD-negative and thus at risk of HDFN.15 The Pragmatic, Randomized Optimal Platelet and Plasma Ratios (PROPPR) study found that approximately 76% of patients with trauma survived for at least 30-days.16 If she survives the trauma then she must become pregnant, which happens at least once in 86% of American women aged 40–44 years old.17 Next, the woman must become D-alloimmunized. The range of D-alloimmunization rates that have been reported among hospitalized RhD-negative recipients of RhD-positive blood products such as RBCs and/or LTOWB during their resuscitation is between 7.8% to 42.7% and for this calculation, the highest reported rate will be used.1 2 As the current study found, 62% of pregnant, D-alloimmunized women produce an anti-D with a titer ≥16 thereby putting that pregnancy at higher risk of HDFN. Approximately 60% of fetuses will be RhD-positive and thus susceptible to HDFN.15 Finally, 4% of pregnancies affected by HDFN will result in perinatal death,18 whereas 25% of affected pregnancies will result in perinatal death or another serious adverse effect such as requiring an intrauterine transfusion or neonatal exchange transfusion.19 Multiplying all these frequencies together gives a calculated risk of perinatal death from HDFN of 0.04% and of perinatal death or other serious adverse effects of 0.24%. These risks of perinatal adverse outcomes must be weighed against the benefits of prehospital and early in-hospital transfusions, which in many cases might be RhD-postive due to the scarcity of RhD-negative units.
This study has several limitations. It was not possible to determine the source of the anti-D alloimmunization event for these women, although a recent study demonstrated that the stimulating event of antibodies that cause HDFN is predominantly from previous pregnancies.20 Furthermore, it is not known if antibodies stimulated by transfusion are more or less likely to become high titer than those stimulated by a previous pregnancy. In any case, it is unlikely that a woman’s pregnancy with a high titer anti-D would be managed differently based on the cause of the alloimmunization. It is also unknown if the women were re-exposed to RhD-positive RBCs via fetal–maternal hemorrhage during their second pregnancy. In addition, it is possible that some women had anti-D titers performed outside of this hospital’s network, which would not have been available for analysis. It is also important to consider that although titer testing is limited by high intra-laboratory and inter-laboratory scoring variation,21 the titer data used in this study are those that were used by the patients’ obstetricians for clinical decision-making and so they reflect this hospital’s laboratory and clinical practice. Both the American College of Obstetricians and Gynecologists (ACOG)22 and the AABB (Association for the Advancement of Blood and Biotherapies, formerly known as the American Association of Blood Banks)15 recommend a critical anti-D titer threshold of between 8 and 32 when determining which pregnancies require more intensive monitoring for HDFN. A lower titer threshold would be more sensitive for detecting affected pregnancies but would result in more women with unaffected pregnancies undergoing what would ultimately be unnecessary HDFN screening.23 24 At this hospital, women with anti-D that titers to <16 are followed by repeat titer testing every month, however, additional testing such as non-stress tests, growth ultrasounds, or fetal biophysical profiles are not performed because the anti-D titer has not crossed the critical threshold. Thus, the focus of this study was on women with a titer ≥16 because at this center, those women are especially likely to be routinely offered extra monitoring for HDFN during their pregnancy. Although unlikely, it is possible that RhIg could produce an anti-D titer >4, which would have led to the patient’s erroneous inclusion in this study. However, the published literature, and the experience at this hospital’s RBC immunohematology reference laboratory, all suggest that anti-D titers ≥8 are not caused by RhIg administration. Lastly, this study was performed at one center, thereby potentially limiting its generalizability to other centers and a multicenter trial is required to definitively determine the rate at which D-alloimmunized women develop a high titer antibody.
These data suggest that 62% of the D-alloimmunized WCPs might produce an anti-D that rises to a titer that would typically lead to more extensive HDFN monitoring at this institution. These data allow for a more comprehensive calculation of the perinatal HDFN risk after the transfusion of RhD-positive RBCs and LTOWB during a woman’s resuscitation. Including the 62% risk of developing a high titer (≥16) anti-D, the risk of perinatal death was calculated to be 0.04% and the risk of perinatal death or experiencing a severe adverse HDFN event was calculated to be 0.24%.
Footnotes
Correction notice: This article has been corrected since it published Online to include the updated figure 1.
Contributors: MHY: Designed and performed the research, analyzed the data, wrote the manuscript. PS, SPE, CL, DJT: Contributed to study design, critically revised the manuscript, approved final version of manuscript.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: PS consults for Hemanext, Cerus, CSL Behring, is on the scientific advisory board for Haima and Octapharma and is a co-founder and chief medical officer for Kalocyte. DJT is on the scientific advisory board for Fresenius Kabi. MHY is on the scientific advisory board for Hemanext and has given paid lectures for Terumo BCT, Grifols. SPE and CL do not have any conflicts of interest to disclose.
Provenance and peer review: Not commissioned; externally peer reviewed.
Ethics statements
Patient consent for publication
Not applicable.
References
- 1.Raval JS, Madden KM, Neal MD, Moore SA. Anti-D alloimmunization in Rh(D) negative adults with severe traumatic injury. Transfusion 2021;61 Suppl 1:S144–9. 10.1111/trf.16493 [DOI] [PubMed] [Google Scholar]
- 2.Yazer M, Triulzi D, Sperry J, Corcos A, Seheult J. Rate of RHD-alloimmunization after the transfusion of RHD-positive red blood cell containing products among injured patients of childbearing age: single center experience and narrative literature review. Hematology 2021;26:321–7. 10.1080/16078454.2021.1905395 [DOI] [PubMed] [Google Scholar]
- 3.Yazer MH, Delaney M, Doughty H, Dunbar NM, Al-Riyami AZ, Triulzi DJ, Watchko JF, Wood EM, Yahalom V, Emery SP. It is time to reconsider the risks of transfusing RHD negative females of childbearing potential with RHD positive red blood cells in bleeding emergencies. Transfusion 2019;59:3794–9. 10.1111/trf.15569 [DOI] [PubMed] [Google Scholar]
- 4.Yazer MH, Spinella PC, Seheult JN. Risk of future haemolytic disease of the fetus and newborn following the transfusion of Rh(D)-Positive blood products to Rh(D)-Negative children. Vox Sang 2022;117:291–2. 10.1111/vox.13169 [DOI] [PubMed] [Google Scholar]
- 5.Seheult JN, Stram MN, Pearce T, Bub CB, Emery SP, Kutner J, Watanabe-Okochi N, Sperry JL, Takanashi M, Triulzi DJ, et al. The risk to future pregnancies of transfusing Rh(D)-Negative females of childbearing potential with Rh(D)-Positive red blood cells during trauma resuscitation is dependent on their age at transfusion. Vox Sang 2021;116:831–40. 10.1111/vox.13065 [DOI] [PubMed] [Google Scholar]
- 6.Yazer MH, Díaz-Valdés JR, Triulzi DJ, et al. Considering equality in transfusion medicine practice. Br J Haematol 2023;201:1245–7. 10.1111/bjh.18830 [DOI] [PubMed] [Google Scholar]
- 7.Cacciatore A, Rapiti S, Carrara S, Cavaliere A, Ermito S, Dinatale A, Imbruglia L, Recupero S, La Galia T, Pappalardo EM, et al. Obstetric management in Rh alloimmunizated pregnancy. J Prenat Med 2009;3:25–7. [PMC free article] [PubMed] [Google Scholar]
- 8.Bowman JM, ed. Hemolytic disease (Erythroblastosis Fetalis) 3rd ed. W.B. Saunders Company, 1994. [Google Scholar]
- 9.Bowman JM, Pollock JM. Failures of intravenous Rh immune globulin prophylaxis: an analysis of the reasons for such failures. Transfus Med Rev 1987;1:101–12. 10.1016/s0887-7963(87)70010-8 [DOI] [PubMed] [Google Scholar]
- 10.Badami KG, Parker J, Kenny A, Warrington S. Incidence of maternal sensitisation to Rh(D) in Christchurch, New Zealand and reasons for prophylaxis failures. N Z Med J 2014;127:40–6. [PubMed] [Google Scholar]
- 11.Lieberman L, Callum J, Cohen R, Cserti-Gazdewich C, Ladhani NNN, Buckstein J, Pendergrast J, Lin Y. Impact of red blood cell alloimmunization on fetal and neonatal outcomes: a single center cohort study. Transfusion 2020;60:2537–46. 10.1111/trf.16061 [DOI] [PubMed] [Google Scholar]
- 12.Liu S, Ajne G, Wikman A, Lindqvist C, Reilly M, Tiblad E. Management and clinical consequences of red blood cell antibodies in pregnancy: a population-based cohort study. Acta Obstet Gynecol Scand 2021;100:2216–25. 10.1111/aogs.14261 [DOI] [PubMed] [Google Scholar]
- 13.Rahimi-Levene N, Chezar J, Yahalom V, Israeli HSGI. Red blood cell alloimmunization prevalence and hemolytic disease of the fetus and newborn in Israel: A retrospective study. Transfusion 2020;60:2684–90. 10.1111/trf.15987 [DOI] [PubMed] [Google Scholar]
- 14.United States Census Bureau . Population by age and sex: 2021. Available: https://www.census.gov/data/tables/2021/demo/age-and-sex/2021-age-sex-composition.html [Accessed 5 Oct 2023].
- 15.Cohen C, Delaney M, Johnson S, et al. Technical manual. 20th edn. Bethesda, MD: AABB press, 2020. [Google Scholar]
- 16.Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA 2015;313:471–82. 10.1001/jama.2015.12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pew Research Center . They’re waiting longer, but US women today more likely to have children than a decade ago, Available: https://www.pewsocialtrends.org/2018/01/18/theyre-waiting-longer-but-u-s-women-today-morelikely-to-have-children-than-a-decade-ago/ [Accessed 14 Jul 2019].
- 18.Zwiers C, Oepkes D, Lopriore E, Klumper FJ, de Haas M, van Kamp IL. The near disappearance of fetal hydrops in relation to current state-of-the-art management of red cell Alloimmunization. Prenat Diagn 2018;38:943–50. 10.1002/pd.5355 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Koelewijn JM, de Haas M, Vrijkotte TGM, Bonsel GJ, van der Schoot CE. One single dose of 200 microg of antenatal rhig halves the risk of anti-D immunization and hemolytic disease of the fetus and newborn in the next pregnancy. Transfusion 2008;48:1721–9. 10.1111/j.1537-2995.2008.01742.x [DOI] [PubMed] [Google Scholar]
- 20.Delaney M, Wikman A, van de Watering L, Schonewille H, Verdoes JP, Emery SP, Murphy MF, Staves J, Flach S, Arnold DM, et al. Blood group antigen matching influence on gestational outcomes (AMIGO) study. Transfusion 2017;57:525–32. 10.1111/trf.13977 [DOI] [PubMed] [Google Scholar]
- 21.Karafin MS, DeSimone RA, Dvorak J, Metcalf RA, Pagano MB, Park YA, Schwartz J, Souers RJ, Szczepiorkowski ZM, Uhl L, et al. Antibody titers in transfusion medicine: a critical reevaluation of testing accuracy, reliability, and clinical use. Arch Pathol Lab Med February 2, 2023. 10.5858/arpa.2022-0248-CP [DOI] [PubMed] [Google Scholar]
- 22.The American College of Obstetricians and Gynecologists (ACOG) . ACOG practice bulletin number 192 March 2018. management of Alloimmunizationn during pregnancy. [Google Scholar]
- 23.Singh B, Chaudhary R, Katharia R. Reassessment of critical anti-D antibody titer in RHD alloimmunized antenatal women. Lab Med 2023;54:429–33. 10.1093/labmed/lmac149 [DOI] [PubMed] [Google Scholar]
- 24.Walsh CA, Doyle B, Quigley J, McAuliffe FM, Fitzgerald J, Mahony R, Higgins S, Carroll S, McParland P. Reassessing critical maternal antibody threshold in RHD alloimmunization: a 16-year retrospective cohort study. Ultrasound Obstet Gynecol 2014;44:669–73. 10.1002/uog.13383 [DOI] [PubMed] [Google Scholar]