

Abstract
Introduction
It is unclear whether hydrodilatation is beneficial in the management of frozen shoulder compared with other common conservative management modalities. This systematic review evaluates the efficacy of hydrodilatation for the management of frozen shoulder.
Sources of data
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. An extensive search of PubMed, Embase, Scopus, Cochrane Central, Web of Science and CINAHL databases using multiple keyword combinations of ‘shoulder’, ‘rotator’, ‘adhesive capsulitis’, ‘hydrodilatat*’, ‘distension’ since inception of the databases to June 2023 was implemented.
Areas of agreement
Hydrodilatation leads to at least transient more marked improvements in shoulder disability and passive external rotation compared with intra-articular corticosteroid injections.
Areas of controversy
Hydrodilatation improves passive external rotation in the longer term. Moreover, hydrodilatation may be a preferable option over manipulation under anaesthesia, given its lower cost and better patient convenience.
Growing points
Intensive mobilization after hydrodilatation is a promising adjuvant treatment option for patients suffering from a frozen shoulder.
Areas timely for developing research
Although current evidence suggests that hydrodilatation provides a transient improvement in disability in patients with frozen shoulder, its clinical relevance remains unclear. Further research is necessary to establish its role in the management of the condition.
Keywords: frozen shoulder, hydrodilatation, corticosteroid injection
Introduction
Frozen shoulder, sometimes referred to as adhesive capsulitis, is an insidious musculoskeletal condition that affects the glenohumeral joint. It is characterized by the formation of scar tissue, adhesions and capsular thickening within the shoulder.1,2 Frozen shoulder has a reported prevalence of 2–5% in the general population, rising to 20% in individuals with diabetes mellitus.3 Typically, patients present with excruciating pain and reduced passive and active range of motion (ROM) of the glenohumeral joint. Symptoms generally last from 6 months to 2 years. Most patients demonstrate spontaneous resolution of symptoms, and thus conservative management is commonly advised.4
Currently, there exists a plethora of conservative management options for patients with frozen shoulder, including analgesia, corticosteroids (oral or intra-articular), physiotherapy, acupuncture, manipulation, suprascapular nerve blockade and hydrodilatation.5 First proposed in 1965 by Andren and Lundberg, intra-articular hydrodilatation attempts to expand the joint space through the sheer hydraulic pressure exerted by the injectate.6 However, given the marked disability caused by frozen shoulder, some patients may forgo the less invasive hydrodilatation and instead opt for more invasive surgery. This is a possible consequence of the perceived slow nature of symptom improvement with conservative approaches.7 Additionally, there remains ambiguity surrounding the effectiveness of hydrodilatation as a treatment method.8
Gam et al. compared hydrodilatation to corticosteroid injections alone and identified improvements in shoulder pain and ROM.9 However, the results of this study were limited given the high risk of bias. On the contrary, Corbiel et al. and Jacobs et al. found no significant differences when assessing the same treatment modalities.10,11 Furthermore, many studies have examined the efficacy of hydrodilatation amid other treatment options, and thus its specific effects have not always been assessed.12
The effectiveness of hydrodilatation may well be short-lived,10,11 as no large study has addressed this particular aspect of the intervention.10 Hydrodilatation may potentially lower the prevalence of long-term impairments; however, it remains challenging to determine the number of patients suffering from residual deficiencies.10 Most recently, Saltychev et al. demonstrated statistically significant symptomatic improvements with the use of hydrodilatation when assessing its effectiveness in the management of frozen shoulder. However, this effect was deemed not to be clinically relevant.5 Thus, amid the incongruent results in the literature, more research is warranted. Nonetheless, hydrodilatation is recommended as part of the patient care pathway co-produced by the British Elbow and Shoulder Society and British Orthopaedic Association.12
This review evaluates the current evidence on the efficacy of hydrodilatation for frozen shoulder. This study builds on the previous systematic review by Saltychev et al.,5 through the inclusion of recently published randomized controlled trials and prospective and retrospective studies.
Methods
Study design
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 were used to conduct and report this review.13 Our Population, Intervention, Comparison and Outcome framework was as follows:
Participants: adults, with frozen or painfully stiff shoulders, suffering from discomfort that limits both active and passive glenohumeral joint motions.
Intervention: glenohumeral joint hydrodilatation (hydrodistension and distension).
Comparison: intra-articular corticosteroid injections, a placebo, sham, other interventions or no therapy.
-
Outcome: all clinically relevant outcomes.
Primary: assessment of pain and function or disability.
Secondary: ROM, complications and any others.
Search strategy
Computer searches were conducted on PubMed, Embase, Scopus, Cochrane Central, Web of Science and CINAHL electronic databases from inception to June 18, 2023 for articles assessing hydrodilatation in patients with frozen shoulder. The goal was to increase the search strategy’s sensitivity to increase the likelihood that all relevant studies would be obtained.14,15
Our search clause for the PubMed search was ‘(shoulder OR rotator OR adhesive capsulitis) AND (hydrodilatat* OR distension).’ When conducting searches on the different databases, similar clauses were utilized. We adjusted the search strategy from a previous systematic review5 to accommodate our own needs. The search was restricted to humans only, and the reference management software EndNote was used to organize its results. The relevance of the cited studies’ references was also examined. A step-by-step process, which involved team meetings to improve the search strategy and settle disagreements, was utilized to ensure that the searches were producing relevant studies.16
Study screening
All references were downloaded from the Rayyan reference management software, and duplicates were removed before screening the title and abstract. The full texts of the remaining articles were examined after two authors (DP and RH) independently assessed the titles and abstracts. A consensus meeting between the two authors was organized to settle disputes that arose during research screening and selection. If no consensus could be reached, the senior author (NM) was contacted for a final decision.
Study selection
Only peer-reviewed journals were considered. There were limited restrictions on the study design within the selection criteria, which increased the likelihood of identifying pertinent studies. Thus, randomized controlled trials, prospective and retrospective comparative studies and case series were included. Level I–IV studies, according to the Oxford Centre for Evidence Based Medicine, were identified and included in our analysis. The hydrodilatation technique and follow-up period had to be well described in all included studies, which had to use at least one validated clinical outcome score or assess change in ROM. Studies needed to be published in English, and had to have recruited at least 10 adult participants. Exclusion criteria were reviews, case reports, experiments on animals, cadavers or in vitro and letters to editors. We also excluded articles with no information on hydrodilatation intervention, diagnosis, follow-up, clinical examination and statistical analysis.
To prevent bias, all authors read, evaluated and discussed the included and excluded studies and the relative list of references. The senior investigator (NM) made the final decision if there was a disagreement among the investigators on the inclusion and exclusion criteria.
Data extraction
Data extracted from each study included the following: author name, study year; study design (level of evidence); number of patients (shoulders); mean age (range) (years); diabetes mellitus diagnosis; Coleman Methodology Score (CMS); imaging assessment; duration of symptoms (average) (months); outcome measures (time intervals); regimen and modification of the distension arms; comparative intervention arm; hydrodilatation technique; and complications. Data were entered in a custom Excel spreadsheet by all the investigators independently. A standardized form, based on the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0, Chapter 7, was used for data extraction for the meta-analysis.17 Discussions with the senior author (NM) allowed the resolution of any discrepancies.
Quality assessment
The methodological quality was assessed according to the CMS.18 Modifications of the CMS were made to make it pertinent for the systematic review of frozen shoulder (Table 1). Each study was scored by two reviewers (DP and RH) independently and in duplicate for each of the criteria adopted to give a total CMS between 0 and 100. A study design that eliminates the impact of chance, bias and confounding variables would receive a score of 100. Disagreements were resolved by discussion. The CMS is divided into sections, each of which is based on a component of the CONSORT statement (for randomized controlled trials) with modifications to accommodate various study designs.
Table 1.
Modified Coleman Methodology Score
| Part A: Only one score to be given for each of the seven sections | ||
|---|---|---|
| Study—number of patients | < 30 | 0 |
| 30–50 | 4 | |
| 51–100 | 7 | |
| >100 | 10 | |
| Mean follow-up | < 6 months | 0 |
| 6–12 months | 4 | |
| 12–18 months | 7 | |
| >18 months | 10 | |
| Injection approach | Different approaches were used and outcomes were not reported separately | 0 |
| Different approaches were used and outcomes were reported separately | 7 | |
| Single approached | 10 | |
| Type of study | Retrospective cohort study | 0 |
| Prospective cohort study | 10 | |
| Randomized controlled trial | 15 | |
| Description of diagnosis | Described without % specified | 0 |
| Described with % specified | 5 | |
| Descriptions of injection technique | Inadequate (not stated, unclear) | 0 |
| Fair (technique only stated) | 5 | |
| Adequate (technique stated, details of surgical procedure given) | 10 | |
| Description of post-injection rehabilitation | Described | 5 |
| Not described | 0 | |
| Part B: Scores may be given for each option in each of the three sections if applicable | ||
| Outcome criteria | Outcome measures clearly defined | 2 |
| Timing of outcome assessment clearly stated | 2 | |
| Use of outcome criteria that have reported reliability | 3 | |
| General health measures included | 3 | |
| Procedure of assessing outcomes | Subjects recruited | 5 |
| Investigator independent of injection clinician | 4 | |
| Written assessment | 3 | |
| Completion of assessment by patients themselves with minimal investigator assistance | 3 | |
| Description of subject selection process | Selection criteria reported and unbiased | 5 |
| Recruitment rate reported | ||
| >90% | 5 | |
| <90% | 0 | |
Statistical analysis
The meta-analysis was performed using Review Manager, version 5.4 (The Cochrane Collaboration). The I2 statistic was used to test for statistical heterogeneity and was assessed as follows: 0% < I2 < 25%, low heterogeneity; 25% < I2 < 50%, moderate heterogeneity; and I2 > 50%, high heterogeneity.18 This effectively describes the percentage of variation across studies originating more from heterogeneity than from chance. We used the random-effects model because outcome measurements were taken at different time points, and the different phases of frozen shoulder increases the risk of heterogeneity. Data for quantitative analysis were extracted at two-time points: the first follow-up post-intervention and the last follow-up post-intervention. The Egger’s test and a funnel plot were used to evaluate the publication bias.
When just the interquartile range (IQR) was provided, IQR/1.35 was used to calculate the standard deviation (SD). According to the Cochrane Handbook for Systematic Review of Interventions Version 5.1.0, Chapter 7, the mean was presumed to be the same as the median when only the median was given.17 SD was computed as (max-min)/4 when only the range was given. Cohen’s d—a standardized mean difference (SMD) in variable change between groups—was used to calculate the effect sizes.
Variables were measured by the SMD with 95% confidence intervals (95% Cis). Data synthesis was initiated for each included study by combining pertinent reported outcomes stratified by pain, disability and ROM at pre-determined time points (earliest and latest follow-ups).
In all analyses, a P-value < 0.05 was considered statistically significant. Sensitivity analysis was conducted to evaluate the reliability of the effects. One study was eliminated at that time, and studies with very heterogeneous findings were also eliminated.
Results
Study identification and selection
Our initial search yielded 1234 articles, with a total of 452 left following the removal of duplicates. We then screened the titles and abstracts of the remaining articles and retained 54 articles for full-text evaluation, which resulted in 39 studies (Fig. 1).
Fig. 1.

Prisma flow diagram.
Demographics
A total of 2623 participants and 2632 shoulders were included. The number of participants recruited in each study varied from 22 to 250. Data on the incidence of diabetes were reported in 16 included studies. Of the 1187 patients, 224 (18%) were diabetic (Table 2).
Table 2.
Details of included articles
| Authors | Study design (level of evidence) | No. of patient (shoulders) | Mean age (range) (years) | Diabetes mellitus diagnosis | CMS |
|---|---|---|---|---|---|
| Dai et al. [2022]19 | Prospective randomized controlled trial (II) | 66 | ACR + HD group: 53.3 HD group: 52.8 |
77 | |
| Wang et al. [2022]20 | Prospective, double-blind, randomized controlled trial (I) | 84 | HD group 1: 54.3 (52.0–56.67) HD group 2: 55.1 (52.6–57.6) |
11 | 71 |
| Albana et al. [2022]21 | Retrospective cohort study (IV) | 31 | HD group: 55.9 HD + SSN group: 52.8 |
47 | |
| Debeer et al. [2021]22 | Prospective case series (IV) | 72 | 53 (38–70) | 9 | 63 |
| Saoji et al. [2021]23 | Prospective cohort study (IV) | 40 | 55 | ||
| Wang et al. [2021]24 | Prospective randomized control trial (II) | 64 | Posterior glenohumeral recess group: 54.0 (51.4–56.5) Rotator cuff interval group: 52.4 (50.1–54.7) |
12 | 76 |
| Makki et al. [2021]25 | Retrospective case series (IV) | 250 | 59 (21–73) | 27 | 36 |
| Paruthikunnan et al. [2020]26 | Prospective double-blinded randomized control trial (I) | 88 | Distension group: 56.5 (40–77) Non-distension group: 54.9 (39–68) | 46 | 78 |
| Rae et al. [2020]27 | Single-arm retrospective observational design (IV) | 90 | 58 | 56 | |
| Ainen et al. [2020]28 | Retrospective case series (IV) | 39 | 54.3 | 8 | 43 |
| Saoji et al. [2020]29 | Prospective cohort study (IV) | 40 | 58 | ||
| Baig et al. [2019]30 | Prospective case series (IV) | 150 | 43.0 (18–60) | 51 | |
| Kim et al. [2019]31 | Case Controlled, Retrospective, Comparative Study (IV) | 47 | Non-pumping group: 55.4 Pumping group: 56.5 |
56 | |
| Gallacher et al. [2018]32 | Randomized prospective controlled trial (II) | 50 | HD group: 55.2 (50.6–59.8) ACR group: 52.6 (48.7–56.5) |
8 | 79 |
| Haughton et al. [2018]33 | Retrospective case series (IV) | 76 | 55.5 (43–66) | 11 | 58 |
| Sinha et al. [2017]34 | Prospective case series (IV) | 118 | 52.6 (28–73) | 26 | 70 |
| Lee et al. [2016]35 | Prospective randomized controlled trial (II) | 64 | HD group: 55.9 IAS group: 53.8 |
70 | |
| Sharma et al. [2016]36 | Prospective randomized controlled trial (II) | 106 | HD group: 53 IAS group: 52 TAU group: 54 |
72 | |
| Yoon et al. [2016]37 | Prospective randomized controlled trial (I) | 86 | HD group: 54.0 IAS group: 53.0 SAI group: 57.0 |
12 | 77 |
| Yoong et al. (2015)38 | Prospective case series (IV) | 22 | 55.0 (32–71) | 3 | 52 |
| Afsar et al. (2015)39 | Prospective case series (IV) | 63 | 51.9 (44–73) | 63 | |
| Ahn et al. [2015]40 | Prospective cohort study (IV) | 121 | HD group: 54.6 IAS group: 55.2 |
57 | |
| Lee et al. [2015]41 | Prospective randomized controlled trial (I) | 64 | Hypertonic saline group: 56.5 Normal saline group: 53.7 |
60 | |
| Park et al. [2014]42 | Randomized controlled trial (II) | 53 | 56 | 47 | |
| Bae et al. [2014]43 | Randomized controlled trial (II) | 54 | Fluoroscopy-guided HD group: 53.3 Ultrasonography-guided HD group: 53.9 |
62 | |
| Clement et al. [2013]44 | Prospective cohort study (IV) | 51 (53) | 52 (34–75) | 12 | 77 |
| Park et al. [2013]45 | Prospective randomized controlled trial (II) | 90 | HD group: 55.2 IAS group: 56.3 |
79 | |
| Park et al. [2012]46 | Prospective randomized controlled trial (II) | 48 | Sono-guided HD group: 56.0 Fluoroscopically guided HD group: 56.4 |
66 | |
| Ng et al. [2012]47 | Prospective randomized trial (II) | 28 (30) | HD group: 53 (44–69) MUA group: 52 (44–61) |
9 | 63 |
| Trehan et al. [2010]48 | Prospective case series (IV) | 36 | 54.6 (26–74) | 74 | |
| Jacobs et al. [2009]49 | Prospective randomized controlled trial (I) | 53 | HD group: 57.0 MUA group: 56.5 |
71 | |
| Tveitå et al. [2008]50 | Randomized controlled trial (II) | 76 | 51.5 | 60 | |
| Quraishi et al. [2007]51 | Prospective randomized controlled trial (II) | 36 (38) | 55.2 (44–70) | 6 | 61 |
| Watson et al. [2007]52 | Prospective clinical series (IV) | 53 | 54.7 | 76 | |
| Buchbinder et al. [2004]53 | Double blind, randomized, placebo-controlled trial (I) | 48 | HD group: 57.2 Placebo group: 57.5 |
13 | 67 |
| Vad et al. [2003]54 | Prospective case series (IV) | 22 | 41.3 (29–54) | 76 | |
| Gam et al. [1998]9 | Randomized controlled trial (II) | 22 | 53 (40–65) | 66 | |
| Jacobs et al. [1991]55 | Prospective randomized controlled trial (II) | 47 (50) | HD group: 55 Distension only group: 53 IAS group: 52 |
52 | |
| Hsu et al. [1991]56 | Prospective cohort study (IV) | 75 | Women: 54 (41–73) Men: 49 (38–61) |
11 | 48 |
HD = hydrodilatation; SSN = supracapsular nerve block; ACR = arthroscopic capsular release; IAS = intra-articular steroid; SAI = subacromial injection; MUA = manipulation under anaesthesia; TAU = treatment as usual
Study identification and selection
A total of 20 studies (51.3%) used imaging, such as ultrasound or magnetic resonance imaging, to confirm the diagnosis of frozen shoulder. The hydrodilatation procedures were performed under ultrasound or fluoroscopic guidance. In 21 studies, the hydrodilatation was administered through the posterior approach, in 13 through the anterior approach, and in 1 using both anterior and posterior approaches. Inclusion and exclusion criteria were overall quite similar across most articles. The volume of mixture injected for hydrodilatation ranged from 9 to 100 mL. Typically, the hydrodilatation mixture consisted of corticosteroids, local anaesthetic and normal saline solution, and only one study used a combination of hyaluronic acid and lidocaine.45 Intra-articular corticosteroid injections were the most commonly utilized reference therapy. Arthroscopic capsular release (ACR), manipulation under anaesthesia (MUA), placebo (arthrogram), general physical therapy and treatment as usual (i.e. physical therapy and oral medication) were also used (Table 3).
Table 3.
Frozen shoulder management
| Authors | Imaging assessment | Duration of symptoms (average) (months) | Outcome measures (time intervals) | Regimen and modification of the distension arms | Comparative intervention arm | Hydrodilatation technique | Complications |
|---|---|---|---|---|---|---|---|
| Dai et al. [2022]19 | RX, MRI | ACR + HD group: 5.4 HD group: 4.5 | Passive ROM, VAS (baseline, 1, 4, 12, 24 weeks, 1 year) UCLA, DASH (baseline, 12 weeks, 24 weeks, 1 year) |
ACR + HD group: 50 mg triamcinolone acetonide, 100 mg ropivacaine with saline to a volume of 20 mL, plus ACR HD group: 50 mg Triamcinolone acetonide, 100 mg ropivacaine with saline to a volume of 20 mL |
Posterior approach with landmark guidance | There were no complications such as infection, nerve or vascular injury. | |
| Wang et al. [2022]20 | RX, ultrasound, MRI | HD group 1: 6.0 HD group 2: 5.6 | SPADI, VAS, ROM (baseline, 6, 12 weeks) |
HD group 1: 4 mL of 40 mg triamcinolone acetonide, 4 mL of 2% lidocaine, 12 mL of normal saline HD group 2: 1 mL of 10 mg triamcinolone acetonide, 4 mL of 2% lidocaine, 15 mL of normal saline |
Posterior approach with ultrasound guidance | No adverse events were reported in either group. | |
| Albana et al. [2022]21 | RX | VAS (intra-injection, 1, 6 months) ASES, DASH (1, 6 months) | HD group: 15–20 mL of saline, 40 mg of triamcinolone SSNB + HD group: 15–20 mL of saline, 40 mg of triamcinolone plus suprascapular nerve block | Posterior approach with ultrasound guidance | |||
| Debeer et al. [2021]22 | RX, ultrasound, MRI | 8 | SPADI, HADS, TSK-11, VAS (baseline, 3 months) Constant-Murley Score (baseline, immediately post-HD, 3 months) | HD group: 1 mL of 40 mg of methylprednisolonacetate, 15 mL of 0.5% marcaine, 20 mL of normal saline | Fluoroscopic guidance | ||
| Saoji et al. [2021]23 | RX, ultrasound | VAS (baseline, 3 weeks) |
HD with steroid group: Up to 16 mL of normal saline, 2 mL Bupivacaine hydrochloride, 2 mL of 80 mg Methylprednisolone HD without steroid group: 18 mL of sterile normal saline, 2 mL Bupivacaine hydrochloride (5 mg/ml) |
Fluoroscopic or ultrasound guidance | |||
| Wang et al. [2021]24 | RX, ultrasound | Posterior glenohumeral recess group: 6.7 Rotator cuff interval group: 6.1 | SPADI, VAS, ROM (baseline, 6, 12 weeks) |
Posterior glenohumeral recess group: 4 mL of 40 mg triamcinolone acetonide, 4 mL of 2% lidocaine, 12 mL of normal saline Rotator cuff interval group: 4 mL of 40 mg triamcinolone acetonide, 4 mL of 2% lidocaine, 12 mL of normal saline |
Posterior approach with ultrasound guidance | The procedure was well tolerated by the patients in both approaches, and no serious adverse events were observed. Two patients (one in each group) reported significant post-injection pain (VAS score > 4) on the first day after the intervention, which resolved spontaneously without the need for additional treatments. | |
| Makki et al. [2021]25 | ROM (baseline, 3 months, 12 months) Pain scores (baseline, 3 months) | HD group: 1 mL of 40 mg Kenalog, 10 mL of 0.25% levobupivacaine, 20 mL of 0.9% NaCl solution | Anterior approach with fluoroscopic guidance | ||||
| Paruthikunnan et al. [2020]26 | RX | Distension group: 5.0 Non-distension group: 5.1 | SPADI (baseline, 1.5, 3, 6 months) | IAS + HD (Distension) group: 12–18 mL of 0.25% bupivacaine, 2 mL of 80 mg methylprednisolone acetate | IAS (Non-distension) group: 2 mL of 0.25% bupivacaine, 2 mL (80 mg) of methylprednisolone acetate | Posterior approach with ultrasound guidance | Other than intra-procedural pain, there were no other significant complications. The average VAS pain score for the non-distension group was 7.4(SD: 1.1) while that in the distension group was significantly higher—8.6(SD:1.0); p < 0.001. 4 patients from the distension group and 3 from the non-distension group had very severe post-injection pain on the night following the intervention, which were controlled by analgesics. None of the patients had any features of septic arthritis post-intervention. |
| Rae et al. [2020]27 | RX | SPADI, UEFI, VAS, EQ-5D-5 L (baseline, 6, 12, 24 weeks) ROM (baseline, 24 hours post-HD) | HD group: 40 mg of triamcinolone acetonide, 4 mL of 1% lidocaine, 25 mL of 0.9% sodium chloride | Posterior approach with ultrasound guidance | None | ||
| Ainen et al. [2020]28 | Ultrasound | 10.2 | NRS, ROM (baseline, 6 weeks) | HD group: 40 mL of normal saline, 40 mg of kenalog, 2 mL of 0.25% marcaine | Posterior approach with ultrasound guidance | Procedure had to be abandoned in one case because of pain | |
| Saoji et al. [2020]29 | RX, ultrasound | SPADI (baseline, 3, 6, 12, 16 weeks) |
HD with steroid group: Up to 16 mL of sterile normal saline, 2 mL of Bupivacaine hydrochloride (5 mg/ml) and 2 mL Depomedrol (80 mg Methyl Prednisolone) HD without steroid group: 18 mL sterile normal saline, 2 mL of Bupivacaine hydrochloride (5 mg/ml) |
Anterior approach with either fluoroscopic or ultrasound guidance | |||
| Baig et al. [2019]30 | RX | VAS, OSS (baseline, 1 month) | HD group: 10 mL of 80 mg of triamcinolone, lidocaine 1%, 40 mL of warm saline | ||||
| Kim et al. [2019]31 | RX, ultrasound, MRI | Nonpumping group: 6.1 Pumping group: 5.6 | Passive ROM, VAS, SPADI (baseline, 3, 6 months) |
HD (Non-pumping) group: 1 mL of 40 mg Triamcinolone, 10 mL of 1% lidocaine, 19 mL of normal saline solution HD (Pumping) group: 1 mL of 40 mg Triamcinolone, 10 mL of 1% lidocaine, 19 mL of normal saline solution |
Posterior approach with ultrasound guidance | No serious complications such as loss of sensation, motor control in the affected arm, infection, or symptoms attributable to side effects of hydraulic distension. Some patients reported some side effects such as facial flushing (total n = 4: the pumping group, n = 2; the nonpumping group, n = 2), local depigmentation of the skin (the pumping group, n = 1) and disturbance of the menstrual pattern (total n = 5: the pumping group, n = 2; the nonpumping group, n = 3). | |
| Gallacher et al. [2018]32 | RX, ultrasound | OSS, EQ-5D VAS, Passive ROM (baseline, 6 weeks, 3 month, 6 months) | HD group: 1 mL of 80 mg Triamcinolone, 4 mL of 2% lidocaine, 40 mL of normal saline | ACR group: Arthroscopic capsular release through a rotator interval portal to the 5 o’clock position. | Anterior approach with fluoroscopic guidance | No complications were noted in either group. | |
| Haughton et al. [2018]33 | OSS (baseline, post-intervention) | HD group: 40 mg of Kenalog, 10 mL of 0.5% chirocaine, saline and contrast | Fluoroscopic guidance | There were no complications observed in any patient during the HD process. | |||
| Sinha et al. [2017]34 | RX, ultrasound | QDASH, OSS (4 weeks, 3, 6, 12 months) | HD group: 8–10 mL of 1% lignocaine, 1 mL of 80 mg triamcinolone, 15 mL of 0.25% bupivacaine, 40–60 mL of normal saline | Posterior approach with ultrasound guidance | The procedure was well tolerated by all patients. The patient group experienced few adverse events/complications of the procedure. One patient developed transient suprascapular nerve palsy because of leakage of anaesthetic into the supraglenoid notch region. Patients often feel some discomfort and sometimes feel dizzy in the first few minutes of/after the procedure. Patients were advised to be accompanied for the procedure and not to drive for the rest of the day. | ||
| Lee et al. [2016]35 | RX, ultrasound, MRI | HD group: 8.2 IAS group: 7.8 | SPADI, VAS, Passive ROM (baseline, 3, 6, 12 weeks) | HD group: Normal saline, 1 mL of 40 mg/mL triamcinolone acetonide, 6 mL of 1% lidocaine | IAS group: 1 mL of 40 mg/mL triamcinolone acetonide, 3 mL of 1% lidocaine | Posterior approach with ultrasound guidance | There were no serious complications (eg, infection) other than facial flushing on days 2 to 5 after injection (1 participant in the IACI group and 2 participants in the capsule-preserved hydrodilatation with corticosteroid group) and dizziness because of vasovagal reaction during the injection (3 participants in the capsule-preserved hydrodilatation with corticosteroid group). |
| Sharma et al. [2016]36 | HD group: 7.0 IAS group: 7.5 TAU group: 6.0 | SPADI (baseline, 4, 8 weeks, 1 year) NPRS, Passive ROM (baseline, 4, 8 weeks) | HD group: 1 mL of Triamcinolone 20 mg, 3 mL Lidocaine, 8 mL to 20 mL of sodium chloride | IAS group: 1 mL of 20 mg Triamcinolone, 3 mL of lidocaine TAU group: physiotherapy and oral pain medication | Posterior approach with landmark guidance | Six patients (17%) in the IS group and four (12%) patients in the ISD group experienced minor transitory side-effects such as flushing and after-pain. No incidences of other side effects were reported. | |
| Yoon et al. [2016]37 | RX, ultrasound | HD group: 9 IAS group: 9 SAI group: 9 | VAS, SST, Constant score, Passive ROM (baseline, 1, 3, 6 months) | HD group: 1 mL of 40 mg triamcinolone, 4 mL 2% lidocaine and 40 mL normal saline |
IAS group: 1 mL of 40 mg triamcinolone, 4 mL of 2% lidocaine and 5 mL of normal saline SAI group: 1 mL of 40 mg triamcinolone, 4 mL of 2% lidocaine and 5 mL of normal saline |
IAS & SAI group: Anterior approach with ultrasound guidance HD group: Anterior approach with fluoroscopic guidance |
Two patients in the IAI group and 1 patient in the SAI group compained of temporary mild dizziness and nausea after the injection. One patient in the HD group reported transient loss of sensation and motor control in the injected arm for a few hours after the injection, but these symptoms recovered with sequelae. One other patient in the HD group reported transient hypotensive syncope immediately after the injection, but the patient fully recovered after several minutes. |
| Yoong et al. (2015)38 | Ultrasound | VAS (baseline, immediately after injection, during the first 24 hrs, during second 24 hrs, 2 weeks) Symptom improvement (4 months) OSS (baseline, 4 months) | HD group: 20 mL of a mixture of 1% lidocaine and 0.5% bupivacaine (50:50 mixture) | Anterior approach with ultrasound guidance | Rotator interval hydrodilatation was well tolerated in all patients with no immediate complications | ||
| Afsar et al. (2015)39 | RX | Simple shoulder test, SST (baseline, 6 months) VAS (baseline, every 3 weeks for 6 months post injection) | HD group: 3 mL of 1% lidocaine and 40 mL of normal saline | Anterior approach | |||
| Ahn et al. [2015]40 | RX, ultrasound | HD group: 7.4 IAS group: 7.2 | SPADI, VNS, passive ROM (baseline, 1, 3, 6 months) | HD group: 19 ml of 0.5% lidocaine plus 1 mL of 30 mg ketorolac | IAS group: 4 mL of 0.5% lidocaine plus 1 mL of 40 mg triamcinolone | Posterior approach with ultrasound guidance | Two patients in US guided IA steroid injection group complained pain due to steroid-induced synovitis which resolved spontaneously within 1 week. Patients in US-guided IA ketorolac injection with capsular distension group reported two cases of dizziness, transient muscle weakness after injection. All reported symptoms had resolved at discharge after monitoring of the symptoms in the recovery room. There were no severe complications, such as septic arthritis, allergic reactions, dyspepsia, bleeding, gastric ulceration and renal dysfunction. |
| Lee et al. [2015]41 | RX, Ultrasound | HD (hypertonic saline) group: 4.8 HD (normal saline) group: 6.5 | SPADI, passive ROM (baseline, 2 weeks) |
HD (hypertonic saline) group: 4 mL of 1% lidocaine and 1 mL of 10 mg triamcinolone with 3% NaCl HD (normal saline) group: 4 mL of 1% lidocaine and 1 mL of 10 mg triamcinolone with 0.9% NaCl |
Posterior approach with ultrasound guidance | No side effects of hypertonic saline injection, including great soreness, pain and other severe conditions, were reported during the study. However, there was mild discomfort resulting from the needle injection and capsule distention in both groups. | |
| Park, et al. [2014]42 | VNS, SPADI, Constant score (baseline, 4 weeks after final treatment) |
HD + IM group: 1 mL of 40 mg of triamcinolone, 3 mL of 1% lidocaine and 10 mL of normal saline HD group: 1 mL of 40 mg of triamcinolone, 3 mL of 1% lidocaine and 10 mL of normal saline |
IM group: intensive mobilization without injection GPT group: general physical therapy without injection |
Anterior approach with fluoroscopic guidance | |||
| Bae et al. [2014]43 | Fluoroscopy-guided HD group: 7.2 Ultrasonography-guided HD group: 6.9 | SPADI, VNS, passive ROM, hand grip, pinch power (baseline, 1 week, 5 weeks, 9 weeks) |
HD (Fluoroscopy-guided) group: 2% lidocaine (5 mL), contrast dye (5 mL), triamcinolone (40 mg) and normal saline (9 mL), in a total fluid volume of 20 mL HD (Ultrasonography-guided) group: 2% lidocaine (5 mL), triamcinolone (40 mg) and normal saline (14 mL), for a total of 20 mL fluid volume |
Anterior approach with fluoroscopic guidance and posterior approach ultrasound guidance | |||
| Clement et al. [2013]44 | OSS, VAS (baseline, 2 days, 1 month, 14 months) ROM (baseline, 2 days, 1 month) | HD: 10 mL of 1% lidocaine and 40 mg (diabetic patients) or 80 mg (non-diabetic patients) of Kenalog (triamcinolone), up to 40 mL of warmed saline | Fluoroscopic guidance | One patient developed septic arthritis after the distension procedure. This required an emergent arthroscopic washout and an extended course of antibiotics. One distension procedure was aborted because the patient was unable to tolerate the procedure due to pain. Both patients were included in the final analysis. No other complications or adverse effects were reported. | |||
| Park et al. [2013]45 | RX, ultrasound | HD group: 5.3 IAS group: 5.3 | SPADI (baseline, 2 weeks, 6 weeks) VNS (baseline, 2 weeks and 12 weeks) Passive ROM (baseline, 2 weeks, 6 weeks) | HD group: 18 mL of 0.5% lidocaine plus 2 mL of sodium hyaluronate 20 mg plus capsular distension | IAS group: 4 mL of 0.5% lidocaine plus 1 mL of 40 mg triamcinolone | Posterior approach with ultrasound guidance | Two patients in group A and 1 patient in group B experienced pain because of needle contact to the labrum, and 12 patients in group B reported pain during capsular distension. No severe complications, such as vasovagal syncope, allergic reactions, steroid-associated infection, adipose tissue atrophy, or toxic reactions, including dizziness, were observed after injections. |
| Park et al. [2012]46 | RX, Ultrasound | Sono-guided HD group: 7.7 Fluoroscopically guided HD group: 7.4 | VNS, SPADI and ROM (baseline, 2 weeks and 6 weeks) | HD group: 10 cc non-ionic contrast media and 0.5% of lidocaine 10 cc containing 20 mg triamcinolone (total 20 cc) | Posterior approach with fluoroscopic and ultrasound guidance | Hot flush, as a side effect, was seen in 2 patients from each group, with no statistical differences between the two groups; no other side effects were reported. | |
| Ng et al. [2012]47 | RX | HD group: 17 MUA group: 17 | ROM, DASH, VAS (baseline, 6 weeks, 6 months) | HD group: 4 mL of 1% lidocaine, 4 mL of 0.5% bupivacaine, 80 mg of Depo-Medrone plus 20 mL of air | MUA group: Manipulation under anaesthesia followed by an intra-articular injection of 4 mL of 1% lidocaine, 4 mL of 0.5% bupivacaine and 2 mL of 80 mg Depo-Medrone | Anterior approach with fluoroscopic guidance | There were no complications encountered during either treatment in the trial. In particular, there were no neurovascular injuries, glenohumeral dislocations or fractures. Two patients who underwent capsular distension continued to have persistent pain and restricted ROM of their shoulders. They were offered MUA after the 6 months follow-up. |
| Trehan et al. [2010]48 | RX, MRI, Ultrasound | SDQ-UK, OSS | HD group: 10 mL of 0.5% bupivacaine, 2 mL of 80 mg triamcinolone and > 25 mL of normal saline | Posterior approach with fluoroscopic guidance | There were no reported adverse incidents reported. | ||
| Jacobs et al. [2009]49 | RX | Constant score, VAS score (baseline, 2, 6 and 12 weeks, and then at 6, 9, 12, 18 and 24 months) SF-36 (baseline, 24 months) | HD group: 1 mL of 40 mg triamcinolone, 5 mL of 2% lignocaine, 10 mL of 0.25% bupivacaine and 5 mL of air | MUA group: Manipulation under anaesthesia | Posterior approach | No systemic or local complications were noted from either treatment modality. | |
| Tveitå et al. [2008]50 | RX | HD group: 7 IAS group: 7 | SPADI, Active and Passive ROM (baseline, 6 weeks) | HD group: 4 mL contrast medium, 2 mL triamcinolone acetonide, 4 mL local anesthetic and 10 mL saline | IAS group: 3–4 mL contrast medium, 2 mL triamcinolone acetonide and 3–4 mL of bupivacaine hydrochloride | Anterior approach with fluoroscopic guidance | Patients recorded pain intensity related to the injection procedures. Most patients reported ‘no pain’ or ‘discomfort’ when describing the procedure. However, six patients in the INJ group and five patients in the DIL group felt that the injections were very painful. Other possible side effects were reported by 20 patients in the INJ group and 14 patients in the DIL group. These were usually mild and lasted only for a few days. Most frequent were complaints over flushing or disturbances in heat regulation (INJ group n = 13, DIL group n = 9). Two patients in each group reported a minor loss of sensation and motor control in their affected arm. Some patients complained over loss of sleep, nausea or dizziness. One patient in the DIL group developed a glenohumeral joint infection which was identified 5 days after the last injection. He immediately underwent arthroscopic surgery and was treated with infusions of cloxacillin for two weeks, with a good result. His baseline SPADI score was 38, and the score at follow-up was 50. One patient in the INJ group developed breast cancer during the study period. |
| Quraishi et al. [2007]51 | RX | HD group: 37.4 weeks MUA group: 39.8 weeks | VAS, Constant score, ROM (baseline, 2 months, 6 months) Satisfaction levels (final follow up) | HD group: 10-55 mL normal saline | MUA group: Manipulation under anaesthesia permitting restoration of shoulder movement | Anterior approach with fluoroscopic guidance | |
| Watson et al. [2007]52 | RX, ultrasound | Primary contracture group: 6.5 Secondary contracture group: 9 | SPADI, Shoulder Disability Index (SDI), self-rating of function, active ROM (baseline, 3 days, 1 week, 3 months, 1 year, 2 years) | HD group: 1 mL of triamcinolone acetonide, 10 mL bupivacaine 0.5%, sterile sodium chloride 0.9% | Anterior approach with fluoroscopic guidance | ||
| Buchbinder et al. [2004]53 | RX | HD group: 118 days Placebo group: 114 days | SPADI, Problem Elicitation Technique (PET), Pain vertical Likert scale, ROM (baseline, 3 weeks, 6 weeks, 12 weeks) | HD group: 1 mL of 40 mg methylprednisolone acetate and up to 82 mL normal saline (total 30–90 mL) | Placebo group: 6 mL of contrast media | Anterior approach with fluoroscopic guidance | No serious adverse effects were reported by participants in either group, but more participants in the active group had pain at the time of the procedure or lasting up to 48 hours than in the placebo group |
| Vad et al. [2003]54 | MRI | L’lnsalata Shoulder Rating Questionnaire—LSRQ (baseline, 3 weeks, minimum 1 year) Hannafin ROM protocol (baseline, immediately post-HD, 3 weeks, minimum 1 year) | HD group: 15 mL of 1% lidocaine with normal saline (range 40–100 mL) | Posterior approach with fluoroscopic guidance | |||
| Gam et al. [1998]9 | RX | HD group: 5 IAS group: 4.5 | Severity of disorder, passive ROM, VAS, daily usage of analgesia, type and number of side-effects (baseline, 3 weeks, 6 weeks, 12 weeks) | HD group: 20 mg of triamcinolonhexacetonid and 19 mL of 0.5% lidocaine | IAS group: 20 mg of triamcinolonhexacetonid | Posterior approach with ultrasound guidance | No other side-effects were reported except the two cases of unacceptabale pain after injection |
| Jacobs et al. [1991]55 | RX | HD group: 8 Distension only group: 6 IAS group: 6 | Analgesic use, severity of pain in relation to daily activities, severity of pain with resisted shoulder movement, active and passive ROM (baseline, 6, 12, 16 weeks) Shoulder dynanometry (2 week intervals for 16 weeks) | Distension only group: 6 mL of 0.25% bupivacaine and 3 mL air (total 9 mL) HD group: 1 mL of 40 mg triamcinolone acetonide, 6 mL of 0.25% bupivacaine and 3 mL air (total 10 mL) | IAS group: 1 mL of 40 mg triamcinolone acetonide (total 1 mL) | Posterior approach with landmark guidance | No patient developed intra-articular sepsis or a supra scapular nerve palsy after the intra-articular injections.Two patients, however, developed temporary (<24 hours) facial flushing after their steroid injection. |
| Hsu et al. [1991]56 | 7.6 | Percentage of pain relief, range of flexion and abduction, functional score, strength of abduction (baseline, 1, 2, 3, 5, 8, 12 weeks) | HD + physiotherapy group: normal saline 100-150 mL with standardized physiotherapy | MUA group: manipulation under anaesthesia and standard physiotherapy Physiotherapy group: standardized physiotherapy with short wave diathermy, interferential therapy and proprioceptive neuromuscular facilitation | Posterior approach | There were no significant complications. Superficial wound infection, which settled with eusol dressings, occurred in two cases in group D. |
Outcomes measurements
The included studies used several outcome measures. The visual analogue score (VAS) was used in 21 articles; the Shoulder and Pain Disability Index (SPADI) in 18 studies; the Oxford Shoulder Score (OSS) in seven studies; the Disabilities of the Arm, Shoulder and Hand (DASH) in three studies; and the Constant-Murley score in five studies.
Quality assessment
The average CMS score was 63, indicating that the overall quality of the included studies was fair. Table 2 provides the actual values of the CMS. Inter-rater reliability was calculated between the mean values of CMS calculated by two authors (DP and RH). Cohen’s kappa coefficient (k) was 0.779661, indicating substantial agreement for the first round of methodological quality assessment. The intra-rater reliability was k = 0.864111 and 0.915309 for DP and RH respectively, indicating almost perfect agreement.
Complications
The included studies reported transient complications such as flushing, local depigmentation of the skin, loss of sensory and motor control in the affected arm, loss of sleep, nausea, dizziness,31,35,36,40,50,55 hypotensive syncope37 and after-injection pain.9,24,26,34,36 In one patient, hydrodilatation was abandoned from unbearable pain during the procedure.28 Two studies reported one patient each with a glenohumeral joint infection.44,50
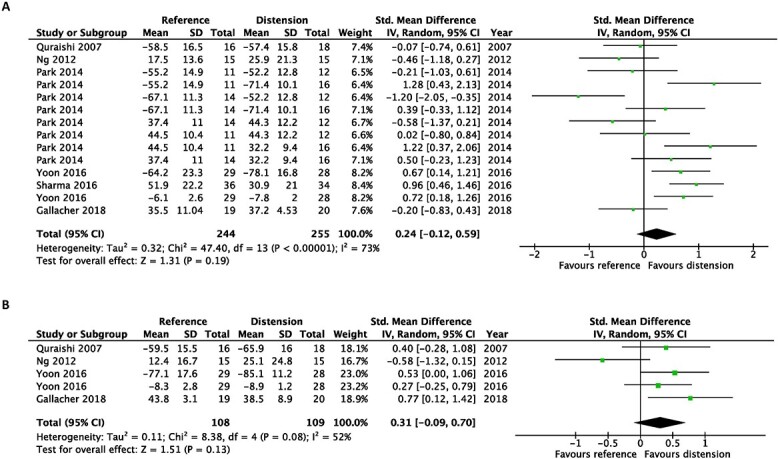
Meta-analysis of the studies evaluating the effect of capsular distension versus corticosteroid alone
There was no significant benefit of intra-articular corticosteroid injection alone compared with capsular distension at the first follow-up post-intervention (SMD, 0.09; 95% CI, −0.27 to 0.45) and at the last follow-up post-intervention (SMD, −0.02; 95% CI, −0.21 to 0.17) when pain scores were evaluated (Fig. 2).
Fig. 2.

Early after intervention (A) and at the end of the study (B). Forest plot of the standardized mean differences of pain improvement comparing hydrodilatation and intra-articular corticosteroid injection.
In terms of disability, hydrodilatation was favoured over intra-articular corticosteroid injection at first follow-up post-intervention (SMD, 0.24; 95% CI, 0.05–0.43). However, this was not observed at the last follow-up post-intervention (SMD, −0.01; 95% CI, −0.23 to 0.22) (Fig. 3).
Fig. 3.

Early after intervention (A) and at the end of the study (B). Forest plot of the standardized mean differences of disability improvement comparing hydrodilatation and intra-articular corticosteroid injection.
Regarding improvements in passive shoulder ROM, hydrodilatation prevailed over intra-articular corticosteroid injections when assessing passive external rotation at the earliest (SMD, 0.43; 95% CI 0.12–0.74) and at the latest follow-up post-intervention (SMD, 0.68; 95% CI, 0.21–1.16) (Fig. 4).
Fig. 4.

Early after intervention (A) and at the end of the study (B). Forest plot of the standardized mean differences of improvements in passive external rotation with the use of hydrodilatation or an intra-articular corticosteroid injection.
Moreover, there were no statistically significant differences in passive forward flexion, abduction or internal rotation at both time points (Figs 5–Fig. 7).
Fig. 5.

Early after intervention (A) and at the end of the study (B). Forest plot of standardized mean differences of improvements in passive forward flexion with the use of hydrodilatation or an intra-articular corticosteroid injection.
Fig. 7.

Early after intervention (A) and at the end of the study (B). Forest plot of the standardized mean differences of improvements in passive internal rotation with the use of hydrodilatation or an intra-articular corticosteroid injection.
Fig. 6.

Early after intervention (A) and at the end of the study (B). Forest plot of standardized mean differences of improvements in passive abduction with the use of hydrodilatation or an intra-articular corticosteroid injection.
The Cochrane Handbook Chapter 10 advises that tests for funnel plot asymmetry should only be used if a minimum of 10 studies are included in the meta-analysis. As this threshold was not reached, funnel plot asymmetry was not calculated.17
Quantitative analysis of the studies not included in the meta-analysis
The pooled effect sizes of studies not included in the meta-analysis where intra-articular corticosteroid was not used as a control are shown in forest plots (Figs 8–10). All comparisons were not statistically significant when evaluating the pooled effect size.
Fig. 8.

Early after the intervention (A) and at the end of the study (B). Forest plots of the standardized mean differences of improvements in pain with usage of hydrodilatation and/or different reference treatments.
Fig. 10.

Early after the intervention (A) and at the end of the study (B). Forest plots of standardized mean differences of improvements in external rotation with usage of hydrodilatation and/or different reference treatments.
Fig. 9.
Early after the intervention (A) and at the end of the study (B). Forest plots of the standardized mean differences of improvements in disability with usage of hydrodilatation and/or different reference treatments.
Park et al.42 showed large effect sizes at the outcome measurements for pain, disability and external rotation for the earliest follow-ups post-intervention. In that study, a combination of intensive mobilization after hydrodilatation was compared with general physiotherapy.
Discussion
The present systematic review investigated the effectiveness of hydrodilatation for frozen shoulder in terms of pain, shoulder disability and ROM, which were considered proxy indicators of therapeutic effects. Hydrodilatation demonstrated transient improvements in shoulder disability during the early follow-up periods. Additionally, significant improvements in passive external rotation were observed at the earliest and latest follow-ups. When comparing the pooled effects of hydrodilatation to other reference treatments, such as MUA, ACR and general physiotherapy, no significant differences were identified.
Contracture of the coracohumeral ligament is considered the predominant pathology in frozen shoulder. During image-guided hydrodilatation, leakage of contrast agents into the subscapularis bursa is often a sign of capsular rupture.11 This occurrence suggests that, in comparison with the posterior capsule, the anterior joint capsule is less resistant to the stretching forces of the injectate, which may account for the improvements in passive external rotation. However, more research is required to confirm this hypothesis. Various epidemiological studies have identified a link between diabetes mellitus and frozen shoulder.57–59 Indeed, this systematic review included a total of 224 individuals (18%) with diabetes mellitus.
In a previous Cochrane review, Buchbinder et al. identified one study comparing hydrodilatation versus placebo, and found improvements in shoulder pain and ROM. However, there was insufficient evidence to suggest that hydrodilatation prevailed over intra-articular corticosteroid injections, which are well reported for the treatment of a frozen shoulder.10 The combination of the two treatments may induce a synergistic effect, the former abating glenohumeral joint inflammation and the latter facilitating joint cavity expansion.11
Most of the evidence in the present systematic review is derived from comparisons between hydrodilatation versus intra-articular corticosteroid injections alone. The results of this review support previous studies, which also found statistically significant but transient improvements in shoulder disability and passive external rotation.11 Thus, clinicians must balance the immediate improvements in disability and external rotation with the possible negative consequences of hydrodilatation, such as the acute pain following joint capsular rupture. However, we did also identify improvements in passive external rotation at the latest follow-ups, contrary to the findings of previous studies.11
Furthermore, mixed results were evidenced when comparing the efficacy of hydrodilatation and MUA. Park et al. found statistically significant improvements in pain, disability and external rotation for MUA when compared with hydrodilatation.42 On the other hand, Quraishi et al. identified that hydrodilatation provided statistically significant improvements in pain compared with MUA in the earliest follow-up periods.51 However, there were no significant differences in pain scores at late follow-ups and in terms of disability outcome measures. Therefore, MUA should be considered secondary to hydrodilatation given its uncertainty regarding its superiority. Also, MUA is a relatively expensive inpatient procedure, whereas hydrodilatation is an outpatient treatment which does not require anaesthesia. Other recognized drawbacks of MUA include humeral fractures, isolated infraspinatus paralysis, brachial plexus traction injuries and rotator cuff tears.47,49,51
Limitations
This investigation presents several limitations. Firstly, as frozen shoulder of all durations was examined as a whole, we could not determine the best way to treat each of the stages of frozen shoulder. Secondly, both within and across trials, different volumes of hydrodilatation fluid were utilized. As a result, we were unable to assess the association between injectate volume and its clinical efficacy. Therefore, to standardize the delivery of hydrodilatation in future studies, researchers and clinicians should adhere to recently published guidelines.60 Thirdly, our secondary outcomes included several shoulder ROM components that might lead to erroneous positive results. As a result, any favourable secondary outcomes should be carefully assessed and supported by further research. Fifthly, publication bias was not assessed, as we had less than ten studies in the meta-analysis. Sixthly, our meta-analysis software (Review Manager 5.4) was not able to differentiate the specific outcomes measures and comparative treatments on the forest plots for the studies by Park (2014) and Yoon (2016) (Figs 8–10). This made it impossible to visually distinguish which comparative treatment demonstrated superior efficacy.
Furthermore, only a relatively few outcomes, namely changes in pain intensity, disability and improvements in ROM, were used to assess the efficacy of hydrodilatation. As a result, several potentially important outcomes were not considered, including patient satisfaction and incidence of complications. Also, the role of concurrent physiotherapy on the effects of hydrodilatation was not measured since patients’ post-intervention exercise routines differed among the included trials and were not described in sufficient detail. Therefore, future research should include standardized rehabilitation protocols, and ensure that the regimen is adequately described.61 Finally, doubts regarding the accuracy of injections should be considered as we did not differentiate the study’s results based on image- versus anatomical landmark-guided injections.
Conclusion
Hydrodilatation may provide early improvements of disability in addition to short- and long-term improvements in passive external rotation in frozen shoulder. However, there is comparable effectiveness of glenohumeral joint hydrodilatation and intra-articular corticosteroid injection when assessing most long-term outcomes. Hydrodilatation is a promising alternative treatment to the more expensive surgery. Clinicians must manage patient expectations appropriately given the wide number of reported complications. Finally, well-designed, appropriately powered RCTs, with a low risk of bias, are required to confirm the relevance and validity of hydrodilatation in the management of frozen shoulder.
Contributor Information
Daryl Poku, Faculty of Medicine, University of Southampton, Southampton, SO17 1TW, UK.
Rifat Hassan, Faculty of Medicine, University of Southampton, Southampton, SO17 1TW, UK.
Filippo Migliorini, Department of Orthopaedic, Trauma, and Reconstructive Surgery, RWTH University Hospital, Aachen 52074, Germany; Department of Orthopaedics and Trauma Surgery, Academic Hospital of Bolzano (SABES-ASDAA), Bolzano 39100, Italy.
Nicola Maffulli, Department of Medicine, Surgery and Dentistry, University of Salerno, Salerno 84084, Italy; Centre for Sports and Exercise Medicine, Barts and The London School of Medicine and Dentistry, Mile End Hospital, London E1 4DG, UK; School of Pharmacy and Biotechnology, Keele University School of Medicine, Thornburrow Drive, Stoke on Trent, Keele ST5 5BG, UK.
CRediT author statement
Daryl Poku (Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing—original draft), Rifat Hassan (Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing—original draft), Filippo Migliorini (Methodology, Software, Validation, Visualization), Nicola Maffulli (Methodology, Software, Validation, Visualization, Writing—review and editing).
Conflict of Interest Statement
The authors declare that they have no conflict of interest.
Funding
No external source of funding was used.
Data Availability
All the data underlying the submission in the manuscript has been reported.
References
- 1. Le HV, Lee SJ, Nazarian A, et al. Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments. Shoulder Elbow 2017;9:75–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Millar NL, Meakins A, Struyf F, et al. Frozen shoulder. Nat Rev Dis Primers 2022;8:59. [DOI] [PubMed] [Google Scholar]
- 3. Zreik NH, Malik RA, Charalambous CP. Adhesive capsulitis of the shoulder and diabetes: a meta-analysis of prevalence. Muscles Ligaments Tendons J 2016;6:26–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Eljabu W, Klinger HM, von Knoch M. Prognostic factors and therapeutic options for treatment of frozen shoulder: a systematic review. Arch Orthop Trauma Surg 2016;136:1–7. [DOI] [PubMed] [Google Scholar]
- 5. Saltychev M, Laimi K, Virolainen P, et al. Effectiveness of hydrodilatation in adhesive capsulitis of shoulder: a systematic review and meta-analysis. Scand J Surg 2018;107:285–93. [DOI] [PubMed] [Google Scholar]
- 6. Andrén L, Lundberg BJ. Treatment of rigid shoulders by joint distension during arthrography. Acta Orthop Scand 1965;36:45–53. [DOI] [PubMed] [Google Scholar]
- 7. Rex SS, Kottam L, McDaid C, et al. Effectiveness of interventions for the management of primary frozen shoulder. Bone Joint Open 2021;2:773–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Maund E, Craig D, Suekarran S, et al. Management of frozen shoulder: a systematic review and cost-effectiveness analysis. Health Technol Assess 2012;16:1–264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Gam AN, Schydlowsky P, Rossel I, Remvig L, Jensen EM. Treatment of 'Frozen Shoulder' with distension and glucorticoid compared with glucorticoid alone: a randomised controlled trial. Scand J Rheumatol 1998;27:425–30. [DOI] [PubMed] [Google Scholar]
- 10. Buchbinder R, Green S, Youd JM, et al. Arthrographic distension for adhesive capsulitis (frozen shoulder). Cochrane Database Syst Rev 2008;1:Cd007005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Wu W-T, Chang K-V, Han D-S, et al. Effectiveness of glenohumeral joint dilatation for treatment of frozen shoulder: a systematic review and meta-analysis of randomized controlled trials. Sci Rep 2017;7:10507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Rangan A, Goodchild L, Gibson J, et al. Frozen shoulder. Shoulder Elbow 2015;7:299–307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Haynes RB, Wilczynski N, McKibbon KA, et al. Developing optimal search strategies for detecting clinically sound studies in MEDLINE. J Am Med Inform Assoc 1994;1:447–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Wilczynski NL, Haynes RB. Optimal search strategies for detecting clinically sound prognostic studies in EMBASE: an analytic survey. J Am Med Inform Assoc 2005;12:481–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Tawfik GM, Dila KAS, Mohamed MYF, et al. A step by step guide for conducting a systematic review and meta-analysis with simulation data. Trop Med Health 2019;47:46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Higgins J, Green S. Cochrane handbook for systematic reviews of interventions (version 5.1.0). http://handbook-5-1.cochrane.org (6 May 2023, date last accessed).
- 18. Tallon C, Coleman BD, Khan KM, et al. Outcome of surgery for chronic Achilles tendinopathy. A critical review. Am J Sports Med 2001;29:315–20. [DOI] [PubMed] [Google Scholar]
- 19. Dai Z, Liu Q, Liu B, et al. Combined arthroscopic release with corticosteroid hydrodilatation versus corticosteroid hydrodilatation only in treating freezing-phase primary frozen shoulder: a randomized clinical trial. BMC Musculoskelet Disord 2022;23:1102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Wang JC, Hsu PC, Wang KA, et al. Comparative effectiveness of corticosteroid dosages for ultrasound-guided glenohumeral joint hydrodilatation in adhesive capsulitis: a randomized controlled trial. Arch Phys Med Rehabil 2023;104:745–52. [DOI] [PubMed] [Google Scholar]
- 21. Albana R, Prasetia R, Primadhi A, et al. The role of suprascapular nerve block in hydrodilatation for frozen shoulder. SICOT J 2022;8:25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Debeer P, Commeyne O, De Cupere I, et al. The outcome of hydrodilation in frozen shoulder patients and the relationship with kinesiophobia, depression, and anxiety. J Exp Orthop 2021;8:85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Saoji K, Gawande V, Sadavarte T, et al. A comparative study on assessment of pain as an outcome by vas score in patients of adhesive capsulitis treated by hydrodilatation with and without corticosteroids. Indian J Forensic Med Toxicol 2021;15:4460–5. [Google Scholar]
- 24. Wang JC, Tsai PY, Hsu PC, et al. Ultrasound-guided hydrodilatation with triamcinolone acetonide for adhesive capsulitis: a randomized controlled trial comparing the posterior glenohumeral recess and the rotator cuff interval approaches. Front Pharmacol 2021;12:686139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Makki D, Al-Yaseen M, Almari F, et al. Shoulder hydrodilatation for primary, post-traumatic and post-operative adhesive capsulitis. Shoulder Elbow 2021;13:649–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Paruthikunnan SM, Shastry PN, Kadavigere R, et al. Intra-articular steroid for adhesive capsulitis: does hydrodilatation give any additional benefit? A randomized control trial. Skeletal Radiol 2020;49:795–803. [DOI] [PubMed] [Google Scholar]
- 27. Rae GC, Clark J, Wright M, et al. The effectiveness of hydrodistension and physiotherapy following previously failed conservative management of frozen shoulder in a UK primary care centre. Musculoskeletal Care 2020;18:37–45. [DOI] [PubMed] [Google Scholar]
- 28. Ainen A, Sivan M. Ultrasound-guided hydrodilatation for adhesive capsulitis of the shoulder: a case series. J Orthop Trauma Rehabil 2020;0:2210491720963285. [Google Scholar]
- 29. Saoji K, Gawande V, Dulani R. A comparative study of disability and pain assessment by Shoulder Pain and Disability Index (SPADI) Score in patients of adhesive capsulitis treated by hydrodilatation with and without corticosteroids. Int J Curr Res Rev 2020;12:35–40. [Google Scholar]
- 30. Baig A, Rahim I, Farooq O, et al. Role of orthographic distension for treatment of frozen shoulder. Pak J Med Health Sci 2019;13:224–6. [Google Scholar]
- 31. Kim YW, Shin S, Chang WH, et al. Hydraulic distension with pumping technique for treating frozen shoulder: a case-controlled, retrospective, comparative study with 6-month follow-up. Pain Physician 2019;22:E563–e72. [PubMed] [Google Scholar]
- 32. Gallacher S, Beazley JC, Evans J, et al. A randomized controlled trial of arthroscopic capsular release versus hydrodilatation in the treatment of primary frozen shoulder. J Shoulder Elbow Surg 2018;27:1401–6. [DOI] [PubMed] [Google Scholar]
- 33. Haughton DN, Barton S, Meenan E, et al. Can we improve the outcome of hydrodilatation for adhesive capsulitis? Shoulder Elbow 2018;10:93–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Sinha R, Patel P, Rose N, et al. Analysis of hydrodilatation as part of a combined service for stiff shoulder. Shoulder Elbow 2017;9:169–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Lee DH, Yoon SH, Lee MY, et al. Capsule-preserving hydrodilatation with corticosteroid versus corticosteroid injection alone in refractory adhesive capsulitis of shoulder: a randomized controlled trial. Arch Phys Med Rehabil 2017;98:815–21. [DOI] [PubMed] [Google Scholar]
- 36. Sharma SP, Bærheim A, Moe-Nilssen R, et al. Adhesive capsulitis of the shoulder, treatment with corticosteroid, corticosteroid with distension or treatment-as-usual; a randomised controlled trial in primary care. BMC Musculoskelet Disord 2016;17:232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Yoon JP, Chung SW, Kim JE, et al. Intra-articular injection, subacromial injection, and hydrodilatation for primary frozen shoulder: a randomized clinical trial. J Shoulder Elbow Surg 2016;25:376–83. [DOI] [PubMed] [Google Scholar]
- 38. Yoong P, Duffy S, McKean D, et al. Targeted ultrasound-guided hydrodilatation via the rotator interval for adhesive capsulitis. Skeletal Radiol 2015;44:703–8. [DOI] [PubMed] [Google Scholar]
- 39. Afsar S, Ullah S, Idrees M. Results of hydraulic joint capsule distension in idiopathic adhesive capsulitis. Rawal Med J 2015;40:168–71. [Google Scholar]
- 40. Ahn JK, Kim J, Lee SJ, et al. Effects of ultrasound-guided intra-articular ketorolac injection with capsular distension. J Back Musculoskelet Rehabil 2015;28:497–503. [DOI] [PubMed] [Google Scholar]
- 41. Lee JH, Kim SB, Lee KW, et al. Effect of hypertonic saline in intra-articular hydraulic distension for adhesive capsulitis. PM&R 2015;7:721–6. [DOI] [PubMed] [Google Scholar]
- 42. Park SW, Lee HS, Kim JH. The effectiveness of intensive mobilization techniques combined with capsular distension for adhesive capsulitis of the shoulder. J Phys Ther Sci 2014;26:1767–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Bae JH, Park YS, Chang HJ, et al. Randomized controlled trial for efficacy of capsular distension for adhesive capsulitis: fluoroscopy-guided anterior versus ultrasonography-guided posterolateral approach. Ann Rehabil Med 2014;38:360–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Clement RG, Ray AG, Davidson C, et al. Frozen shoulder: long-term outcome following arthrographic distension. Acta Orthop Belg 2013;79:368–74. [PubMed] [Google Scholar]
- 45. Park KD, Nam H-S, Lee JK, et al. Treatment effects of ultrasound-guided capsular distension with hyaluronic acid in adhesive capsulitis of the shoulder. Arch Phys Med Rehabil 2013;94:264–70. [DOI] [PubMed] [Google Scholar]
- 46. Park KD, Nam HS, Kim TK, et al. Comparison of Sono-guided capsular distension with fluoroscopically capsular distension in adhesive capsulitis of shoulder. Ann Rehabil Med 2012;36:88–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Ng CY, Amin AK, McMullan L, et al. A prospective randomized trial comparing manipulation under anaesthesia and capsular distension for the treatment of adhesive capsulitis of the shoulder. Shoulder Elbow 2012;4:95–9. [Google Scholar]
- 48. Trehan RK, Patel S, Hill AM, et al. Is it worthwhile to offer repeat hydrodilatation for frozen shoulder after 6 weeks? Int J Clin Pract 2010;64:356–9. [DOI] [PubMed] [Google Scholar]
- 49. Jacobs LG, Smith MG, Khan SA, et al. Manipulation or intra-articular steroids in the management of adhesive capsulitis of the shoulder? A prospective randomized trial. J Shoulder Elbow Surg 2009;18:348–53. [DOI] [PubMed] [Google Scholar]
- 50. Tveitå EK, Tariq R, Sesseng S, et al. Hydrodilatation, corticosteroids and adhesive capsulitis: a randomized controlled trial. BMC Musculoskelet Disord 2008;9:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Quraishi NA, Johnston P, Bayer J, et al. Thawing the frozen shoulder. J Bone Joint Surg Br 2007;89-B:1197–200. [DOI] [PubMed] [Google Scholar]
- 52. Watson L, Bialocerkowski A, Dalziel R, et al. Hydrodilatation (distension arthrography): a long-term clinical outcome series. Br J Sports Med 2007;41:167–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Buchbinder R, Green S, Forbes A, et al. Arthrographic joint distension with saline and steroid improves function and reduces pain in patients with painful stiff shoulder: results of a randomised, double blind, placebo controlled trial. Ann Rheum Dis 2004;63:302–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Vad VB, Sakalkale D, Warren RF. The role of capsular distention in adhesive capsulitis. Arch Phys Med Rehabil 2003;84:1290–2. [DOI] [PubMed] [Google Scholar]
- 55. Jacobs LG, Barton MA, Wallace WA, et al. Intra-articular distension and steroids in the management of capsulitis of the shoulder. BMJ 1991;302:1498–501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Hsu SY, Chan KM. Arthroscopic distension in the management of frozen shoulder. Int Orthop 1991;15:79–83. [DOI] [PubMed] [Google Scholar]
- 57. Balci N, Balci MK, Tüzüner S. Shoulder adhesive capsulitis and shoulder range of motion in type II diabetes mellitus: association with diabetic complications. J Diabetes Complications 1999;13:135–40. [DOI] [PubMed] [Google Scholar]
- 58. Bridgman JF. Periarthritis of the shoulder and diabetes mellitus. Ann Rheum Dis 1972;31:69–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Huang Y-P, Fann C-Y, Chiu Y-H, et al. Association of diabetes mellitus with the risk of developing adhesive capsulitis of the shoulder: a longitudinal population-based followup study. Arthritis Care Res 2013;65:1197–202. [DOI] [PubMed] [Google Scholar]
- 60. Thompson H, Brealey S, Cook E, et al. Expert clinical consensus in the delivery of hydrodilatation for the management of patients with a primary frozen shoulder. Bone Joint Open 2022;3:701–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Hanchard NCA, Goodchild L, Brealey SD, et al. Physiotherapy for primary frozen shoulder in secondary care: developing and implementing stand-alone and post operative protocols for UK FROST and inferences for wider practice. Physiotherapy 2020;107:150–60. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All the data underlying the submission in the manuscript has been reported.