
Fig. 1. Intracranial neurosurgery.
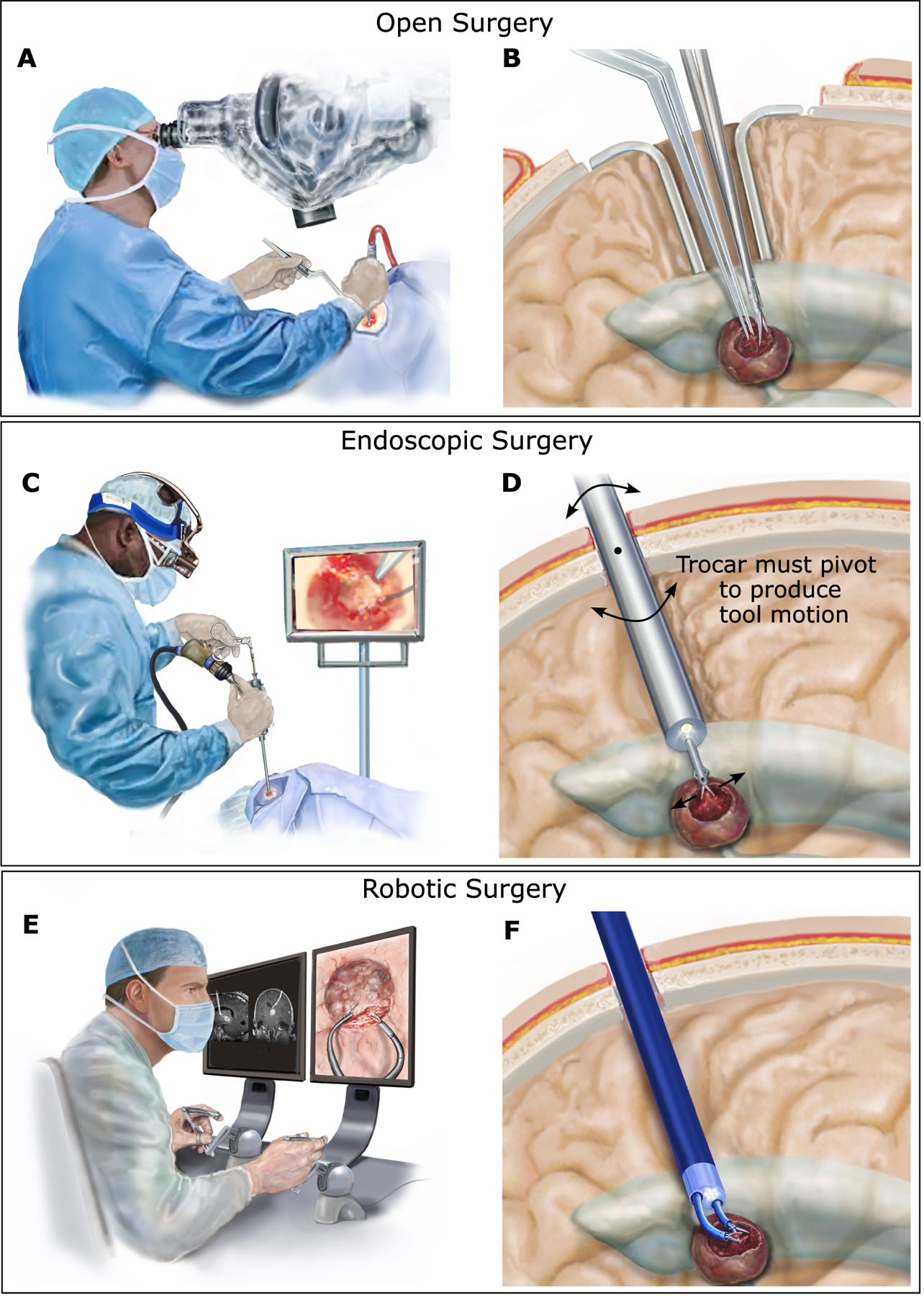
(A) In open surgery, the surgeon views the brain through a microscope and uses both hands to manipulate tools inside the brain. (B) A portion of the skull is removed, and retractors are used to hold back healthy brain tissue to create a corridor through the brain to reach the tumor (shown in dark red) and to enable manipulation of the tools. (C) In endoscopic surgery, the surgeon inserts an endoscope trocar through the brain tissue to reach tumors adjacent to the fluid-filled ventricles. In most cases, only a single straight tool can be deployed through the trocar. (D) Endoscope insertion requires only a small burr hole in the skull and minimal disruption of brain tissue for insertion. To produce lateral motion of the tool, however, the endoscope trocar must be pivoted about the burr hole in the skull, causing potentially dangerous compression or disruption of the adjacent brain tissue. (E) Robotic endoscopic surgery enables the surgeon to sit comfortably while viewing the endoscopic video on a large screen and controlling the motions of two tools using joysticks. (F) As in standard endoscopy, the robotic trocar is inserted through a burr hole in the skull. Two tip-mounted steerable arms enable the surgeon to perform bimanual surgical tasks and to do so without pivoting the trocar against the surrounding brain tissue.