
Fig. 5—
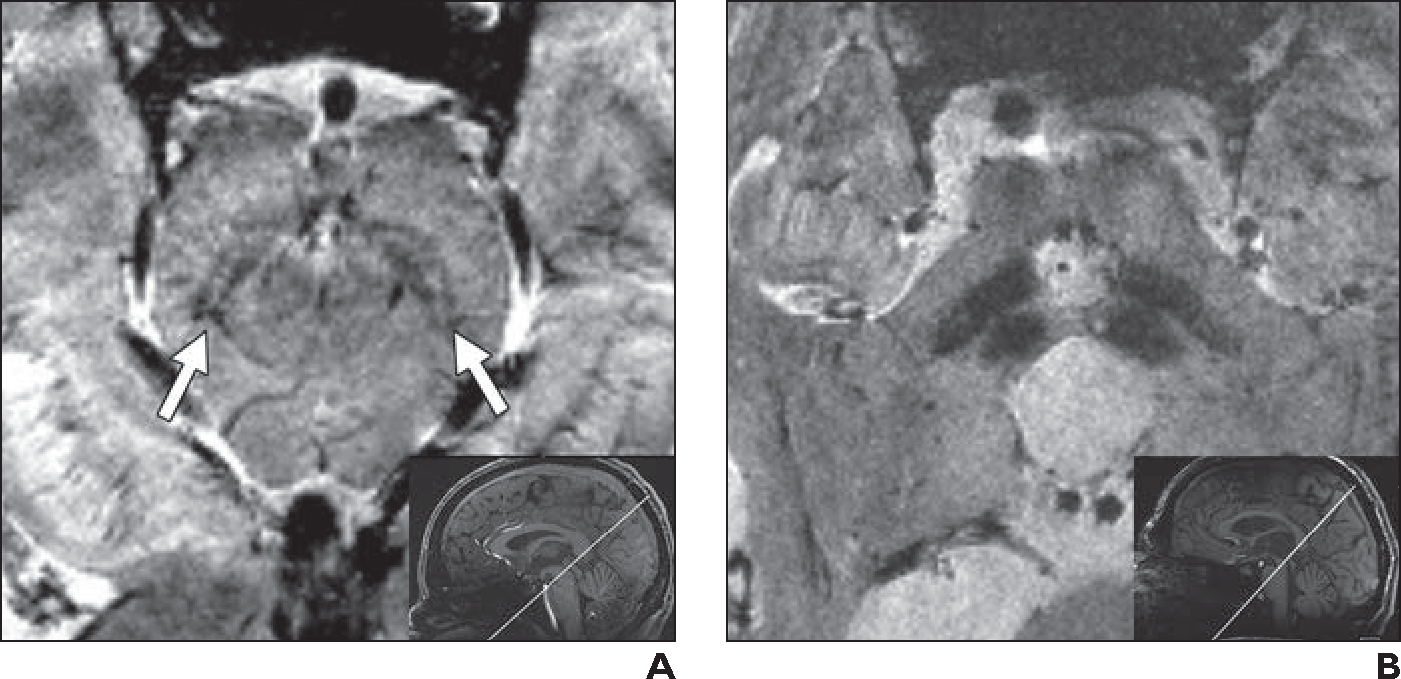
“Loss of swallowtail” sign.
A, 32-year-old healthy man who volunteered to undergo 7-T brain MRI. Oblique axial 7-T T2*-weighted image (limited anatomic coverage; 42 slices of midbrain; slice thickness, 1 mm; matrix, 448 × 448; acquisition time, 4.34 minutes; FOV, 180 mm; voxel size, 0.4 × 0.4 × 1.0 mm; TR/TE, 1140/20; acceleration factor, GRAPPA 2; interpolation off) obtained perpendicular to axis of mesencephalon (inset) clearly shows bilateral swallowtail sign (normal hyperintensity within inner inferior and posterolateral part of substantial nigra) (arrows).
B, 61-year-old man with typical ocular findings of mild-to-moderate progressive supranuclear palsy, including frequent square wave jerks, decreased blinking rate, slowed saccades (vertical more than horizontal), and moderate vertical supranuclear palsy. Oblique axial 7-T T2*-weighted image obtained with same anatomic coverage, orientation (inset), and parameters as in A shows bilateral loss of swallowtail sign, consistent with diagnosis of progressive supranuclear palsy. Examination additionally revealed “hummingbird” sign (< 0.52 ratio of anterior-posterior diameter on midsagittal T1-weighted image of midbrain to pons [not shown]), also consistent with progressive supranuclear palsy. Dopamine transporter scan was also suggestive of progressive supranuclear palsy (not shown).