
Fig. 8—
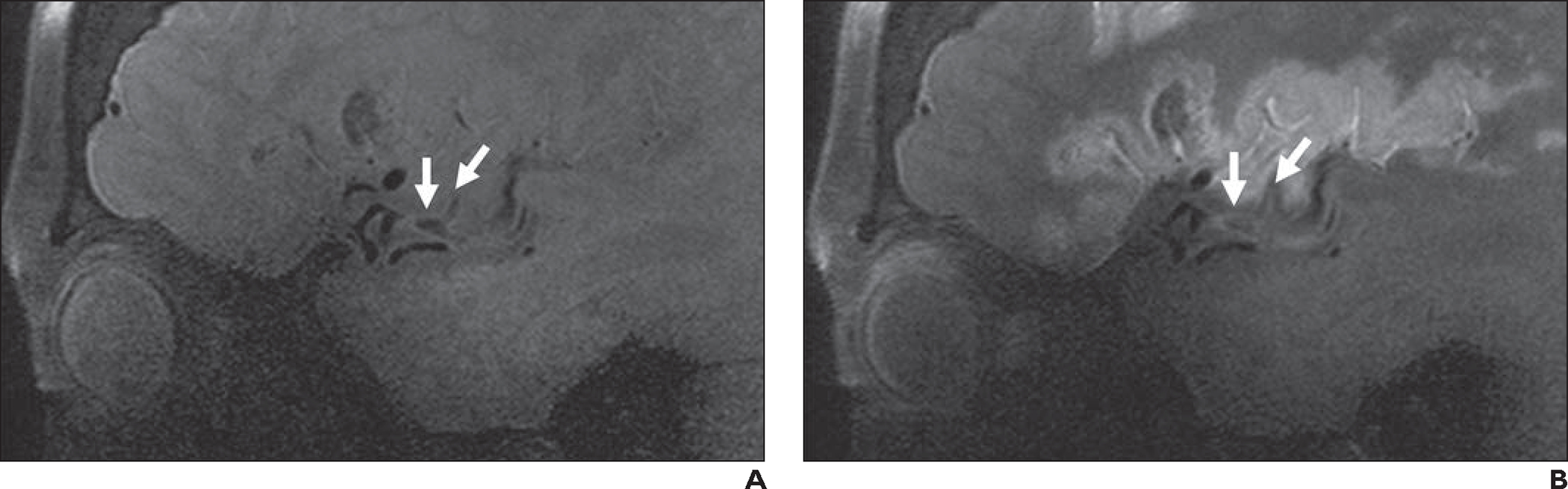
62-year-old woman with left middle cerebral artery infarct (same patient as in Fig. 1). MRI at 7 T with vessel wall imaging was performed to exclude intracranial atherosclerosis and vasculitis. Evaluation was performed with sagittal 3D fat-saturated T1-weighted black-blood SPACE sequence (slice thickness, 0.5 mm; matrix, 272 × 272; FOV, 136 mm; interslice distance, 0%; voxel size, 0.3 × 0.3 × 0.5 mm; acquisition time, 5 minutes 6 seconds; TR/TE, 1100/23; acceleration factor, controlled aliasing in parallel imaging results in higher acceleration 3 [CAIPIRINHA 3]; interpolation on).
A and B, Precontrast image (A) and postcontrast image obtained with half dose of contrast medium (B) show no vasculitis or inflamed plaque. Presumed embolic thrombus is present at M2-M3 junction (Y-shaped structure [arrows]) and exhibits subtle signal, in contrast to low signal intensity in patent vasculature. Adjacent vessel wall exhibits accompanying mild thickening. Expected enhancing cortical laminar necrosis is also present in B.