
FIGURE 2.
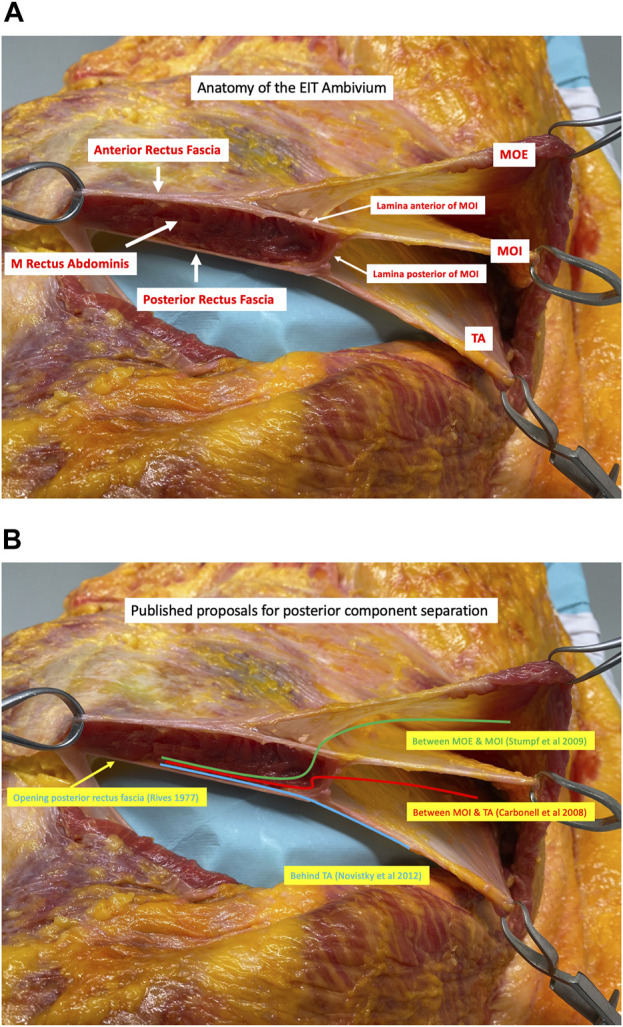
(A) Transverse dissection of the right side (viewed from a cranial perspective) of the anterior abdominal wall in the epigastric region showing the junction of the Musculus Obliquus Externus (MOE), the Musculus Obliquus Internus (MOI), and the Musculus Transversus Abdominis (TA). The lateral border of the rectus sheath is formed by the division of the MOI into an anterior and posterior lamina. These laminae then fuse with the aponeurosis of the MOE anteriorly and the musculoaponeurotic fibres of the TA posteriorly to form the anterior and posterior rectus sheath respectively. The acronym EIT Ambivium is proposed: MOE–MOI–TA, to designate the lateral border of the rectus sheath (Picture from a cadaveric dissection performed at the Anatomy lab of Professor Yohann Renard at the University of Reims, Champagne-Ardenne, France). (B) Each posterior component separation technique starts with a medial incision of the posterior rectus fascia next to the midline allowing for a dissection in the retrorectus plane, referred to as Rives-Stoppa dissection (1). The most superficial posterior component separation technique is performed by incising the lamina anterior of the MOI to enter the inter-oblique plane (2). A layer deeper, the lamina posterior of the MOI can be incised, accessing the plane between the MOI and the TA (3). The deepest posterior component separation technique, known as Transversus Abdominis Release (TAR), involves making an incision in the lamina posterior of the MOI approximately 1 cm medial to the course of the neurovascular bundles and about 1.5 cm medial to the junction. Subsequently, the contribution of the TA muscle to the posterior rectus fascia is incised, which is muscular in the upper part of the abdomen and aponeurotic in the lower part (4).