

Abstract
Two recent large trials showed the potential of single pill combinations (SPCs) with ≥3 low-dose components among people with hypertension who were untreated or receiving monotherapy. In both trials, these ‘hypertension polypills’ were superior to usual care, achieving >80% BP control without increasing withdrawal due to side effects. However, there are no such products available for prescribers. To address this unmet need, George Medicines developed GMRx2 with telmisartan/amlodipine/indapamide in three strengths (mg): 10/1.25/0.625, 20/2.5/1.25; 40/5/2.5. Two pivotal trials are ongoing to support FDA submission for the treatment of hypertension, including initial treatment. These assess efficacy and safety of GMRx2 compared to: placebo, and each of the three possible dual combinations. Regulatory submissions are planned for 2024, with the aim of providing access to GMRx2 in developed and developing regions. Wider implementation of GMRx2-based treatment strategies will be guided by further research to inform access and appropriate scale up.
Keywords: hypertension, polypill, blood pressure, single pill combination, fixed dose
Burden of Hypertension and Current Treatment Gaps
High blood pressure (BP) is a leading cause of the global disease burden and less than 1 in 4 treated individuals achieve recommended BP goals [1,2,3,4]. Globally, most treated patients only receive monotherapy, despite broad consensus that the large majority of patients require multiple antihypertensive drugs [3,4,5,6]. In the United States of America (USA), about 40% of treated patients receive monotherapy, and this has not changed substantially in recent decades [7]. Given the recommendations in recent guidelines for lower BP targets for many patients, the need for effective, tolerable and affordable therapy is even more imperative for the initial treatment of hypertension.
Potential Role of Single Pill Combinations, Including Low-Dose Options
Recent hypertension guidelines, including the 2018 European Society of Cardiology/European Society of Hypertension (ESC/ESH) Guideline, [4] the 2017 American College of Cardiology/American Heart Association (ACC/AHA) Guideline, [3] the 2020 International Society of Hypertension Guideline [8] and the 2021 WHO Hypertension Guideline [9] now suggest combination blood pressure (BP)-lowering of two drugs as initial treatment for many or most patients. These recommendations were based on evidence that dual combinations compared to monotherapy achieve better BP control, improve adherence and reduce therapeutic inertia, without important increases in adverse effects [10,11,12,13]. In recent years there has been interest in low-dose combination therapy with three or more drugs, with evidence indicating that low-dose treatment of multiple drug classes may achieve greater BP control without increasing adverse effects:
Much of the BP-lowering efficacy of any drug in monotherapy is achieved at low doses and efficacy dose-response curves are typically shallow above one quarter of the standard dose [14,15].
At low doses there are few or no adverse effects, but for many classes adverse effects rise steeply and steadily as the dose increases [14,15].
The incidence of idiosyncratic reactions (such as anaphylaxis) to BP-lowering drugs is so low that the risks for a patient simultaneously taking three drugs is acceptably low [15].
There is additivity of effects across drug classes that target different pathophysiological pathways [10,14,15].
There is clear evidence of greater reduction in cardiovascular events with greater BP reduction [16,17].
Large and tolerable reductions in BP have been demonstrated in four short-term (4–12 weeks) trials of triple or quadruple low-dose SPC therapy (Table 1) [18,19,20,21]. These trials provided the rationale for the triple pill vs usual care management for patients with mild-to-moderate hypertension (TRIUMPH) [20] and the quadruple ultralow dose treatment for hypertension (QUARTET) [22] trials among patients with hypertension, who were either untreated or managed with monotherapy. TRIUMPH was a six-month open label randomized controlled trial (RCT) conducted in Sri Lanka that compared initial or early low-dose triple single pill combination (SPC) (telmisartan 20 mg, amlodipine 2.5 mg, chlorthalidone 12.5 mg) with usual care in adults with uncontrolled hypertension [20]. The QUARTET was a 12-week double blinded RCT in 591 Australian adults with uncontrolled hypertension that compared treatment starting with an ultra-low-dose combination (containing irbesartan 37.5 mg, amlodipine 1.25 mg, indapamide 0.625 mg, and bisoprolol 2.5 mg) to guideline-recommended treatment starting with standard dose monotherapy (irbesartan 150 mg). As shown in Figure 1, both trials showed large improvement in BP control achieved quickly and sustained over 6–12 months without usual care group ‘catch-up’ despite considerably higher rates of add-on BP treatment in the usual care group. Furthermore, the usual care groups had superior levels of care, with lower treatment inertia rates and higher BP control rates than are generally seen in normal clinical practice.
Table 1.
Short-term RCTs of triple or quadruple low-dose combination therapy.
|
| |||
|---|---|---|---|
| TRIAL | COMPARISON | BP REDUCTION | TOLERABILITY |
|
| |||
| Mahmud et al 2007 [18] | 4 × ¼ dose (amlodipine 1.25 mg, atenolol 12.5 mg, bendroflumethiazide 0.625 mg, captopril 25 mg, n = 22) vs each at standard dose (n = 86) | 13/8 mmHg (p < 0.001) | No SAEs or treatment withdrawals |
|
| |||
| Wald et al 2012 [19] | 3 × ½ dose (amlodipine 2.5 mg, losartan 25 mg, hydrochlorothiazide 12.5 mg) vs. placebo (n = 86 crossover) | 18/10 mmHg (P < 0.001) | No SAEs or treatment withdrawals |
|
| |||
| Chow et al 2017 [21] | 4 × ¼ dose (irbesartan 37.5 mg, amlodipine 1.25 mg, HCTZ 6.25 mg and atenolol 12.5 mg) vs. placebo (n = 21 crossover) | 22/13 mmHg p < 0.001 | No SAEs or treatment withdrawals |
|
| |||
| Hong et al 2020 [54] | amlodipine, losartan and chlorthalidone at 3 × ½ dose, 3 × ⅓ dose and 3 × ¼ dose (n = 107) vs. placebo (n = 36) for 8 weeks | 17/9, 20/10 and 14/8 mmHg, respectively (all p < 0.01) | No SAEs, 1 treatment-related withdrawal |
|
| |||
Figure 1.
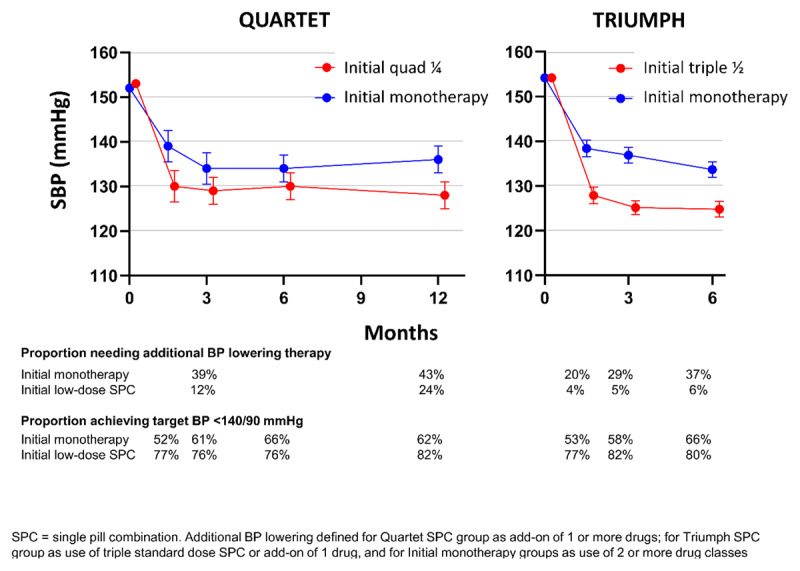
Summary of the QUARTET [22] and TRIUMPH [20] trials of low-dose combination vs usual care for initial/early treatment of hypertension.
Rationale for a New Triple Single Pill Combination
Currently available triple SPCs are only indicated for substitution among patients already taking all the three-component drugs, or as an add-on/switch therapy among patients not adequately controlled on two of the component drugs [23,24,25]. None of the available triple SPCs are available in low-dose strengths, nor indicated for initial treatment. Furthermore, there are no existing SPC products on the market with low-doses of an angiotensin receptor blocker (ARB), calcium channel blocker (CCB) and a thiazide-like diuretic. To address this unmet need, George Medicines (GM) developed a new SPC containing telmisartan, amlodipine and indapamide, named GMRx2, in three strengths (Table 2).
Table 2.
GMRx2 strengths.
|
| ||
|---|---|---|
| GMRx2 DOSE VERSION | STANDARD DOSES OF COMPONENT DRUGS | TELMISARTAN/AMLODIPINE/INDAPAMIDE DOSES (MG) |
|
| ||
| 1 | ¼ | 10/1.25/0.625 |
|
| ||
| 2 | ½ | 20/2.5/1.25 |
|
| ||
| 3 | 1 | 40/5/2.5 |
|
| ||
The rationale for the choice of the individual drug components of GMRx2 is based on several considerations [26]. Hypertension guidelines recommend use of drugs from the four following antihypertensive drug classes: ACEI, ARB, CCB, or thiazide/like diuretics for first-line therapy of adults with hypertension. ARBs are better tolerated than ACEIs and are less likely to cause angioedema among black patients [27], with direct randomized comparisons suggesting comparable efficacy in reducing CV events [28,29,30]. Telmisartan has the longest half-life (~24 hours) of all ARBs [31]. Among CCBs, amlodipine has been used most commonly in CV outcome trials, has little potential for drug interactions and has a long half-life (30–50 hours) [17,32]. Low-doses of the thiazide-like indapamide provide good BP reduction with low side effect profiles [15,33,34,35,36], has a half-life of 16 to 18 hours [37], and is widely available internationally.
The systolic BP (SBP)-lowering efficacy of GMRx2 strengths 1, 2 and 3 (Table 2) from a baseline SBP of 150 mmHg are expected to be approximately 13 mmHg, 18 mmHg and 25 mmHg, respectively [38]. This represents a much greater and clinically important BP reduction in comparison to standard-dose monotherapy, which reduces SBP compared with placebo by only 8–9 mmHg on average, with each doubling of dose conferring only a 1–2 mmHg incremental SBP reduction [10,15]. Dual combinations typically show only a 1–2 mmHg difference between neighboring drug doses and an SBP reduction of around 20 mmHg at maximal dose [10,15,38]. The rationale for developing GMRx2 is, therefore, in line with USA Food & Drug Administration (FDA) observations:
‘Over the last decade, the Agency has actively discouraged antihypertensive monotherapy and combination doses with effects that were very close together, considering them a nuisance to physicians seeking to get patients to goal [39]’
Summary of the GMRx2 Trial Program
The main design features of the two phase III trials for FDA approval of GMRx2 are outlined in Table 3, with further details reported on clinicaltrials.gov [40,41]. Both trials are expected to be completed in 2023. The overall clinical program is directed by an independent steering committee of international experts (Table 4) and an independent data and safety monitoring board (Table 5).
Table 3.
Summary of characteristics of the phase III efficacy and safety trials of GRMx2.
|
| |||||||||
|---|---|---|---|---|---|---|---|---|---|
| TRIAL | DESIGN | PARTICIPANT KEY ELIGIBILITY FOR RANDOMIZATION | KEY EXCLUSION CRITERIA | RANDOMIZED ALLOCATION | INTERVENTION, COMPARATOR | DURATION OF RANDOMIZED TREATMENT AND FOLLOW UP | PRIMARY OUTCOME | PRIMARY SAFETY OUTCOME | SAMPLE SIZE, POWER |
|
| |||||||||
| GMRx2 ACT | Randomized, double-blind, active-controlled, parallel-group, international multi-center | Adults on ≤3 BP-lowering drugs, adhering to and tolerating GMRx2 dose 2 run-in and post run-in home SBP 110-154 mmHg | Receiving 4 or more BP-lowering drugs. Contraindication to the individual components of the GMRx2 |
2:1:1:1 ratio to GMRx2 or one of the three comparators of dual combinations | Intervention: GMRx2 dose 2 Comparators: telmisartan 20 + amlodipine 2.5, Or telmisartan 20 + indapamide 1.25, Or amlodipine 2.5 + indapamide 1.25 for 6 weeks, forced uptitration to double dose for 6 weeks |
12 weeks + 4 weeks safety follow up | Difference in change in home mean SBP from randomization to week 12 | Adverse events (AEs) leading to discontinuation of trial medication from baseline to week 12 | 1500, ≥95% for each of the three comparisons |
|
| |||||||||
| GMRx2 PCT | Randomized, double-blind, placebo-controlled, parallel-group, international multi-center | Adults on ≤2 BP-lowering drugs, adhering to and tolerating placebo run-in and post run-in home SBP 130-154 mmHg | Receiving 2 or more BP-lowering drugs. Contraindication to placebo run-in or any of the randomized medications |
2:2:1 ratio to GMRx2 dose 1, GMRx2 dose 2 or placebo | Intervention 1: GMRx2 dose 1 for 4 weeks Intervention 2: GMRx2 dose 2 for 4 weeks Comparator: Placebo for 4 weeks |
4 weeks + 4 weeks safety follow up | Difference in change in home mean SBP from randomization to week 4 | AEs leading to discontinuation of trial medication from baseline to week 4 | 250, >90% for GMRx2 vs placebo, and >80% for GMRx2 dose 1 vs GMRx2 dose2 |
|
| |||||||||
Table 4.
GMRx2 Program Steering Committee.
|
| ||
|---|---|---|
| NAME | AFFILIATION | ROLE |
|
| ||
| Professor Paul Whelton | Tulane University, New Orleans, USA | Steering Committee Member (Chair) |
|
| ||
| Professor William Cushman | University of Tennessee Health Science Center, USA | Steering Committee Member |
|
| ||
| Professor Asita de Silva | University of Kelaniya, Sri Lanka | Steering Committee Member |
|
| ||
| Professor Diederick Grobbee | University Medical Center Utrecht, Utrecht University, The Netherlands | Steering Committee Member |
|
| ||
| Professor Krzysztof Narkiewicz | Medical University of Gdańsk, Poland | Steering Committee Member |
|
| ||
| A/Professor Dike Ojji | University of Abuja, Nigeria | Steering Committee Member |
|
| ||
| Professor Suzanne Oparil | University of Alabama at Birmingham, USA | Steering Committee Member |
|
| ||
| Professor Neil Poulter | Imperial College, London, UK | Steering Committee Member |
|
| ||
| Professor Markus Schlaich | The University of Western Australia, Australia | Steering Committee Member |
|
| ||
| A/Professor Wilko Spiering | University Medical Center Utrecht, Utrecht University, The Netherlands | Steering Committee Member |
|
| ||
| Professor Bryan Williams | University College, London, UK | Steering Committee Member |
|
| ||
| Professor Jackson T Wright Jr | University Hospitals Cleveland Medical Center, Case Western Reserve University, USA | Steering Committee Member |
|
| ||
| Professor Anthony Rodgers* | The George Institute for Global Health, University of New South Wales, Australia | Steering Committee Member, Academic Coordinating Center |
|
| ||
| Dr Abdul Salam* | The George Institute for Global Health, University of New South Wales, India | Steering Committee Member, Academic Coordinating Center |
|
| ||
| Professor Aletta E Schutte* | The George Institute for Global Health, University of New South Wales, Australia | Steering Committee Member, Academic Coordinating Center |
|
| ||
| Professor Gian Luca Di Tanna* | The George Institute for Global Health, University of New South Wales, Australia | Academic Coordinating Center |
|
| ||
* Non-voting members.
Table 5.
GMRx2 Data and Safety Monitoring Board.
|
| ||
|---|---|---|
| NAME | AFFILIATION | ROLE |
|
| ||
| Professor Lawrence Appel | Johns Hopkins University, Bal, USA | Chair |
|
| ||
| Professor Mark Espeland | Wake Forest University, NC, USA | Member |
|
| ||
| Professor Michael Weber | State University of New York, NY, USA | Member |
|
| ||
| Professor Gian Luca Di Tanna | University of Applied Sciences and Arts of Southern Switzerland, Lugano, Switzerland | Blinded statistician |
|
| ||
| Chris Gianacas | The George Institute for Global Health, Sydney, Australia | Blinded statistician |
|
| ||
| Xiaoqiu (Julia) Liu | The George Institute for Global Health, Sydney, Australia | Unblinded statistician |
|
| ||
| Michelle Leroux | Toronto, Canada | Executive Secretary |
|
| ||
Active-controlled trial
The main objective of this trial is to assess the contribution of each GMRx2 component drug to its overall effects, by assessing the efficacy and safety of GMRx2 compared to each of the three possible dual combinations of the component drugs. The key eligibility criteria are individuals with hypertension currently receiving 0–3 medications, for whom there is uncertainty about treatment with GMRx2 vs dual combinations. The design is summarized in Figure 2. The run-in period will assess participant adherence to trial medication and trial procedures, hence maximizing the likelihood of participant follow-up and complete data collection. The double-blind period will assess the efficacy and safety of GMRx2 dose versions 2 and 3, sequentially, compared to the corresponding three possible dual combinations of the component drugs. The duration of six weeks for each treatment period will allow comparison of the maximal effects of treatment. The safety follow-up period will assess safety over 4 weeks following switching from randomized trial medication to open label usual care treatment.
Figure 2.
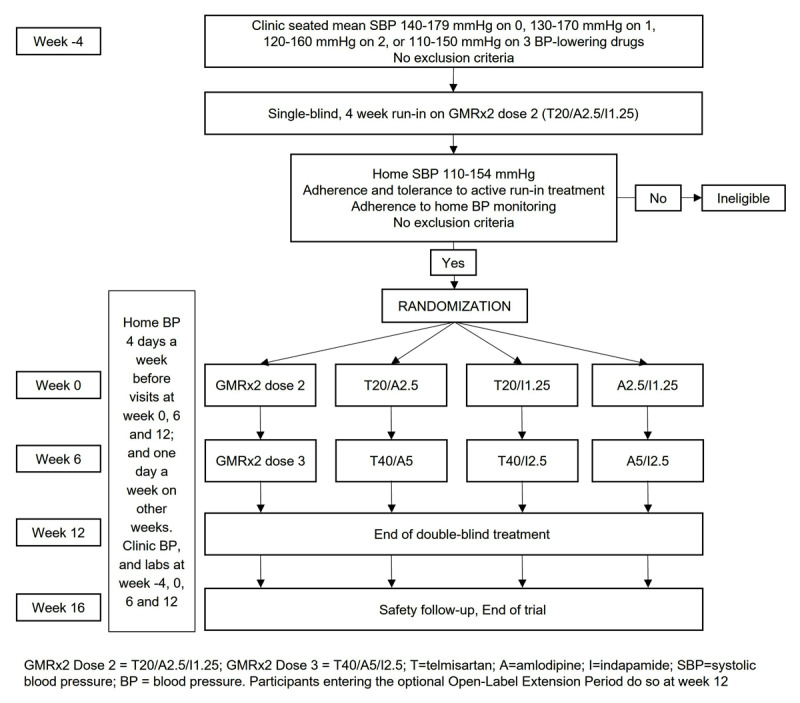
Schema for trial comparing GMRx2 with each dual combination (GMRx2 ACT).
Participants who adhere to GMRx2 dose 2 during the run-in period and have an average home SBP 110–154 mmHg at the end of run-in period. Participants are being recruited from Australia, the Czech Republic, New Zealand, Poland, Sri Lanka, the United Kingdom and the USA. The primary outcome is the difference in change of home SBP from randomization to week 12 (averaged over the preceding week). Randomization was completed with 1385 participants in May 2023, which was >90% of the original 1500 planned, with the steering committee recommending a reduced sample size, without any reference to unblinded data, given the likelihood of adequate power and unexpected problems with drug supply due to pandemic-related supply chain issues. This sample size will provide over 97% power to detect a minimum clinically significant difference of 3 mmHg in mean home seated level of SBP for each of the three comparisons of GMRx2 vs dual therapy, assuming a common standard deviation in SBP of 11 mmHg and a correlation coefficient of 0.4. The overall power for all three comparisons will therefore be > 90%. Previous trials have demonstrated an additional reduction in office SBP of approximately 5 mmHg [42].
Placebo-controlled trial
The main objective of this trial is to investigate the efficacy and safety of GMRx2 compared to placebo. Placebo controlled trials provide important evidence on the full effects of treatment, including both efficacy and safety. Without such evidence it would be difficult to assess the full degree of efficacy, or to reliably attribute the causality of any adverse effects observed. The key eligibility criteria are individuals with hypertension currently receiving 0–1 medications and low estimated cardiovascular risk (e.g., Pooled Cohorts Equation <10% ten-year risk), for whom there is uncertainty about treatment with GMRx2 vs. placebo. The design is summarized in Figure 3. The placebo run-in period will assess each participant’s adherence to trial procedures and allow confirmation of untreated mean BP levels, hence enhancing the power of the trial to detect a difference between GMRx2 and placebo. The double-blind period will assess the efficacy and safety of GMRx2 dose 1 and GMRx2 dose 2 compared to placebo. The safety follow-up period will assess safety over four weeks following switching from randomized trial medication to open label usual care treatment.
Figure 3.
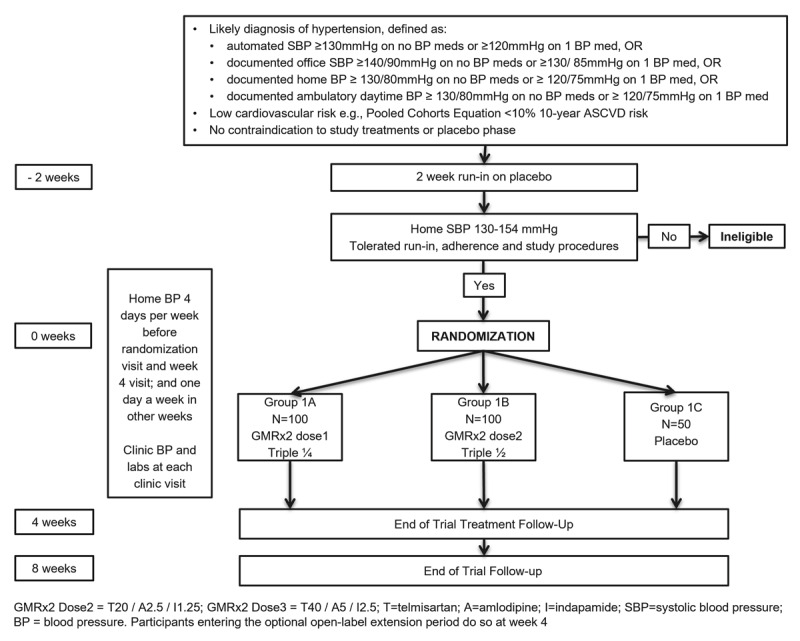
Schema for trial comparing GMRx2 with placebo (GMRx2 PCT).
Participants who tolerate placebo and whose average home SBP is between 130–154 mmHg after a two-week run-in period on placebo are eligible for randomization. Participants were recruited from Australia, Nigeria, Sri Lanka and the USA. The primary outcome is difference in change in home SBP from randomization to week 4 (averaged over the week preceding the final clinic visit). The trial sample size of 250 randomized participants (100 each to GMRx2 strength 1 and 2, and 50 to placebo) is expected to provide 90% power to detect a difference of at least 9 mmHg in mean home SBP for each of the active drug comparisons vs placebo, assuming a common standard deviation of 11 mmHg.
Open-label extension of active and placebo-controlled trial
An open-label extension period of the above two trials will be conducted in some sites, to assess the efficacy and safety of GMRx2 over a one-year period. Willing participants on ≤3 BP-lowering drugs, being adherent to the trial procedures will be consented to be switched at the end of the double-blind period to open label GMRx2. Follow-up visits for the open-label extension study will be scheduled at weeks 2 and 4, given the evidence that almost all the BP-lowering effects of treatment will accrue within two weeks [43], hence providing an opportunity for the study to assess the effects of an evidence-based, accelerated titration schedule. Subsequent follow-up visits will be conducted at week 12, 28, and 40. Participants will continue to monitor home BP, with uptitration for those with home BP > 130/80 mmHg: GMRx2 strength 1 à GMRx2 strength 2 → GMRx2 strength 3 → GMRx2 strength 3 plus telmisartan 40 mg/amlodipine five mg → GMRx2 strength 3 plus telmisartan 40 mg/amlodipine 5 mg plus spironolactone 25 mg. Each titration step was chosen to provide an estimated additional SBP reduction of at least 5 mmHg, in keeping with the strategy of avoiding titration steps that only confer additional average SBP reductions of 1–3 mmHg, such as doubling the dose of a single drug [10,15,42].
Other studies
Pharmacokinetic studies
The GMRx2 development program also includes pharmacokinetic studies [44,45]. The first trial aimed to evaluate pharmacokinetic drug interactions between telmisartan, amlodipine and indapamide and GMRx2. The trial design was a single center, open, randomized, single-dose, two-period, four-treatment, two-sequence, crossover study with a washout period between doses of at least 14 days for Cohort 1 (telmisartan) and Cohort 3 (indapamide), and 28 days for Cohort 2 (amlodipine). In total, 122 healthy volunteers were enrolled and randomized. The second trial aims to evaluate the effect of food on bioavailability (AUC and Cmax) of GMRx2. It is a single center, open, randomized, single-dose, two-period, two-treatment (fed vs. fasting), two-sequence, crossover study with a washout period between doses of at least 28 days. Performed where?
The delivery of optimal blood pressure control in Africa (VERONICA) – Nigeria trial
VERONICA-Nigeria is an investigator-initiated trial being conducted in Black Africans that is comparing a triple therapy SPC-based treatment protocol with treatment based on the Nigeria hypertension guidelines to determine the effectiveness, safety, and feasibility of the SPC for control of high BP in Nigeria. Eligibility is restricted to Black African adults who are untreated or on one BP-lowering medication for ≥2 weeks with clinic BP 140–179 mmHg and/or DBP 90–109 mmHg. The trial compares treatment with an accelerated, simplified, GMRx2-based regimen to the Nigeria hypertension treatment protocol, and the primary outcome is difference in change in home SBP from randomization to month 6. A total of 300 participants are planned, with outcomes expected in late 2023.
Triple therapy prevention of recurrent intracerebral disease events trial (TRIDENT)
TRIDENT is an investigator initiated and conducted, multicenter, international, double-blinded, placebo-controlled, parallel-group, randomized trial designed to determine the efficacy of more intensive BP control with a low-dose SPC (GMRx2 dose 2) strategy in addition to standard of care, on stroke recurrence in patients with a history of acute stroke due to intracerebral hemorrhage [46]. Eligible participants are adults with a history primary intracerebral hemorrhage, SBP of 130–160 mmHg, and no contraindication to the randomization of GMRx2-dose version 2 or placebo in addition to any existing BP lowering regimen. The primary outcome is time to first occurrence of recurrent stroke. A total of 1500 randomized participants are planned with a mean duration of 3 years follow-up.
Discussion
Low-dose triple SPCs have the potential to significantly improve BP control by providing improved efficacy and adherence, and reduced therapeutic inertia with fewer adverse effects compared to current approaches. However, to date there is limited clinical research in this area, and no low-dose triple SPCs on the market globally. The GMRx2 clinical development aims to address these gaps, assessing efficacy and tolerability, with two pivotal regulatory approval trials, and a series of investigator-initiated studies.
The phase III and pharmacokinetics trial program described in this manuscript has been approved by the FDA to potentially support an indication for the treatment of hypertension, including initial treatment. Regulatory approval will also be sought in other markets globally, including importantly low- and middle- income countries (LMICs). Globally there is a dearth in availability and affordability of SPCs in LMICs, where more effective treatment is most needed [47,48]. For example, BP levels are now among the highest globally in Sub-Saharan Africa, where over 200 million people are projected to have hypertension by 2030. Furthermore, hypertension is the leading cause of the rapidly increasing burden of noncommunicable diseases, and less than one in seven with hypertension achieve adequate control [2,49,50]. Market access is also planned in high income settings outside of the USA, but this may be delayed in Europe, given the current requirements for additional studies [51]. The majority of SPC products in Europe are approved only on the basis of bioequivalence studies, and such approvals lead to a ‘straight substitution’ indication (i.e., for use only in people already stabilized on the same drugs at the same doses). This is not possible or appropriate for novel low-dose combinations, developed to help address poor adherence and treatment inertia.
Following regulatory approval of GMRx2, additional studies and implementation research will be required to further delineate the role and cost-effectiveness of GMRx2 compared to current usual care modalities in different patient populations and geographies. Further indications will also be explored such as the prevention of stroke in people with intracerebral hemorrhage [46] and the prevention of dementia [52]. A key issue will be reimbursement in HIC markets, availability and affordability. Most importantly research will be conducted to inform access and appropriate scale-up in disadvantaged populations, where the burden of high BP is highest, and reliable access to affordable, effective therapies is lowest [53].
Funding Statement
The GMRx2 program is funded by George Medicines Pty Ltd (GM), which is partly owned by George Health Enterprises (GHE), the social enterprise arm of The George Institute for Global Health (TGI). GM has received investment from GHE, Brandon Capital, Bupa, and Federation Asset Management.
Abbreviations
ACEI: Angiotensin converting enzyme inhibitor
ARB: angiotensin receptor blocker
BP: blood pressure
CCB: calcium channel blocker
FDA: United States Food and Drug Administration
LMIC: low- and middle- income country
RCT: randomized controlled trial
SPC: single pill combination
SBP: systolic blood pressure
USA: United States of America
Funding Information
The GMRx2 program is funded by George Medicines Pty Ltd (GM), which is partly owned by George Health Enterprises (GHE), the social enterprise arm of The George Institute for Global Health (TGI). GM has received investment from GHE, Brandon Capital, Bupa, and Federation Asset Management.
Competing Interests
Authors Anthony Rodgers, Abdul Salam, Sonali Gnanenthiran and Aletta E Schutte are employed at TGI, which holds an interest in GMRx2 via its ownership of George Health Enterprises. None of the TGI staff have a personal financial interest in GM. Professor Rodgers is seconded part-time to GM. TGI holds patents for ultra-low-dose fixed-dose combination products for the treatment of hypertension and diabetes, and Professor Rodgers is listed as one of the inventors (Granted: US 10,369,15; US 10,799,487; US 10,322,117; US 11,033,544; US 11,478,462; Pending: US 17/932,982; US 18/446,268; US 17/598,122; US 17/317,614; US 17/527,084; US 17/527,085; US 17/527,087). Professor Rodgers does not have a financial interest in these patents. None of the other authors have a financial interest in GM or have received funding for their independent contribution to the GMRx2 program.
Aletta E Schutte has received consulting fees and/or speaker honoraria from Omron Healthcare, Aktiia, Medtronic, Servier, Abbott, Sanofi, Sun Pharmaceuticals, Novartis. She is supported by a Fellowship of the National Health and Medical Research Council of Australia (ID 2017504).
Dike B. Ojji has received speaker honoraria from Novartis, AstraZeneca, Servier, Swipha and Boehringer for speaking at educational meetings.
Krzysztof Narkiewicz has received speaker and consulting honoraria from Bausch Health, Berlin-Chemie/Menarini, Egis, Idorsia, Gedeon Richter, Gilead, Krka, Novo Nordisk, Polpharma, Recordati, Sandoz and Servier.
Markus Schlaich has received consulting fees, and/or travel and research support from Medtronic, Abbott, ReCor, Novartis, Servier, Pfizer, and Boehringer-Ingelheim. He is the current president of Hypertension Australia and Treasurer of the World Hypertension League.
Author Contributions
AR and AS developed the first draft of the manuscript. All the other authors contributed substantially to the conception or design, and in editing and revising this manuscript critically for important intellectual content and provided final approval for its publication.
References
- 1.Murray CJL, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. 2020; 396(10258): 1223–49. DOI: 10.1016/S0140-6736(20)30752-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Campbell NRC, Schutte AE, Varghese CV, Ordunez P, Zhang X, Khan T, et al. São Paulo call to action for the prevention and control of high blood pressure: 2020. The Journal of Clinical Hypertension. 2019; 21(12): 1744–52. DOI: 10.1111/jch.13741 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018; 71(6): e13–e115. DOI: 10.1161/HYP.0000000000000065 [DOI] [PubMed] [Google Scholar]
- 4.Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. European Heart Journal. 2018; 39(33): 3021–104. DOI: 10.1093/eurheartj/ehy339 [DOI] [PubMed] [Google Scholar]
- 5.Chow CK, Teo KK, Rangarajan S, Islam S, Gupta R, Avezum A, et al. Prevalence, Awareness, Treatment, and Control of Hypertension in Rural and Urban Communities in High-, Middle-, and Low-Income Countries. JAMA. 2013; 310(9): 959–68. DOI: 10.1001/jama.2013.184182 [DOI] [PubMed] [Google Scholar]
- 6.Benjamin IJ, Kreutz R, Olsen MH, Schutte AE, Lopez-Jaramillo P, Frieden TR, et al. Fixed-dose combination antihypertensive medications. The Lancet. 2019; 394(10199): 637–8. DOI: 10.1016/S0140-6736(19)31629-0 [DOI] [PubMed] [Google Scholar]
- 7.Derington CG, King JB, Herrick JS, Shimbo D, Kronish IM, Saseen JJ, et al. Trends in Antihypertensive Medication Monotherapy and Combination Use Among US Adults, National Health and Nutrition Examination Survey 2005–2016. Hypertension. 2020; 75(4): 973–81. DOI: 10.1161/HYPERTENSIONAHA.119.14360 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of Hypertension global hypertension practice guidelines. Journal of Hypertension. 2020; 38(6): 982–1004. DOI: 10.1097/HJH.0000000000002453 [DOI] [PubMed] [Google Scholar]
- 9.World Health Organization. Guideline for the pharmacological treatment of hypertension in adults. https://iris.who.int/bitstream/handle/10665/344424/9789240033986-eng.pdf?sequence=1 (accessed 31 January 2024). [PubMed]
- 10.Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination Therapy Versus Monotherapy in Reducing Blood Pressure: Meta-analysis on 11,000 Participants from 42 Trials. The American Journal of Medicine. 2009; 122(3): 290–300. DOI: 10.1016/j.amjmed.2008.09.038 [DOI] [PubMed] [Google Scholar]
- 11.Salam A, Kanukula R, Atkins E, Wang X, Islam S, Kishore SP, et al. Efficacy and safety of dual combination therapy of blood pressure-lowering drugs as initial treatment for hypertension. Journal of Hypertension. 2019; 37(9): 1768–74. DOI: 10.1097/HJH.0000000000002096 [DOI] [PubMed] [Google Scholar]
- 12.Feldman RD, Zou GY, Vandervoort MK, Wong CJ, Nelson SAE, Feagan BG. A Simplified Approach to the Treatment of Uncomplicated Hypertension. Hypertension. 2009; 53(4): 646–53. DOI: 10.1161/HYPERTENSIONAHA.108.123455 [DOI] [PubMed] [Google Scholar]
- 13.Mourad JJ, Waeber B, Zannad F, Laville M, Duru G, Andrejak M. Comparison of different therapeutic strategies in hypertension. Journal of Hypertension. 2004; 22(12): 2379–86. DOI: 10.1097/00004872-200412000-00021 [DOI] [PubMed] [Google Scholar]
- 14.Bennett A, Chow CK, Chou M, Dehbi HM, Webster R, Salam A, et al. Efficacy and Safety of Quarter-Dose Blood Pressure–Lowering Agents. Hypertension. 2017; 70(1): 85–93. DOI: 10.1161/HYPERTENSIONAHA.117.09202 [DOI] [PubMed] [Google Scholar]
- 15.Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003; 326(7404): 1427. DOI: 10.1136/bmj.326.7404.1427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bundy JD, Li C, Stuchlik P, Bu X, Kelly TN, Mills KT, et al. Systolic Blood Pressure Reduction and Risk of Cardiovascular Disease and Mortality. JAMA Cardiology. 2017; 2(7): 775–81. DOI: 10.1001/jamacardio.2017.1421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rahimi K, Bidel Z, Nazarzadeh M, Copland E, Canoy D, Ramakrishnan R, et al. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. The Lancet. 2021; 397(10285): 1625–36. DOI: 10.1016/S0140-6736(21)00590-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mahmud A, Feely J. Low-Dose Quadruple Antihypertensive Combination. Hypertension. 2007; 49(2): 272–5. DOI: 10.1161/01.HYP.0000254479.66645.a3 [DOI] [PubMed] [Google Scholar]
- 19.Wald DS, Morris JK, Wald NJ. Randomized polypill crossover trial in people aged 50 and over. PLoS ONE. 2012; 7(7): e41297. DOI: 10.1371/journal.pone.0041297 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Webster R, Salam A, de Silva HA, Selak V, Stepien S, Rajapakse S, et al. Fixed Low-Dose Triple Combination Antihypertensive Medication vs Usual Care for Blood Pressure Control in Patients With Mild to Moderate Hypertension in Sri Lanka. JAMA. 2018; 320(6): 566–579. DOI: 10.1001/jama.2018.10359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chow CK, Thakkar J, Bennett A, Hillis G, Burke M, Usherwood T, et al. Quarter-dose quadruple combination therapy for initial treatment of hypertension: placebo-controlled, crossover, randomised trial and systematic review. The Lancet. 2017; 389(10073): 1035–42. DOI: 10.1016/S0140-6736(17)30260-X [DOI] [PubMed] [Google Scholar]
- 22.Chow CK, Atkins ER, Hillis GS, Nelson MR, Reid CM, Schlaich MP, et al. Initial treatment with a single pill containing quadruple combination of quarter doses of blood pressure medicines versus standard dose monotherapy in patients with hypertension (QUARTET): a phase 3, randomised, double-blind, active-controlled trial. The Lancet. 2021; 398(10305): 1043–52. DOI: 10.1016/S0140-6736(21)01922-X [DOI] [PubMed] [Google Scholar]
- 23.Calhoun DA, Lacourcière Y, Chiang YT, Glazer RD. Triple Antihypertensive Therapy With Amlodipine, Valsartan, and Hydrochlorothiazide. Hypertension. 2009; 54(1): 32–9. DOI: 10.1161/HYPERTENSIONAHA.109.131300 [DOI] [PubMed] [Google Scholar]
- 24.Chrysant SG, Izzo JL, Kereiakes DJ, Littlejohn T, Oparil S, Melino M, et al. Efficacy and safety of triple-combination therapy with olmesartan, amlodipine, and hydrochlorothiazide in study participants with hypertension and diabetes: a subpopulation analysis of the TRINITY study. Journal of the American Society of Hypertension. 2012; 6(2): 132–41. DOI: 10.1016/j.jash.2011.09.003 [DOI] [PubMed] [Google Scholar]
- 25.Mourad JJ, Amodeo C, de Champvallins M, Brzozowska-Villatte R, Asmar R. Blood pressure-lowering efficacy and safety of perindopril/indapamide/amlodipine single-pill combination in patients with uncontrolled essential hypertension. Journal of Hypertension. 2017; 35(7): 1481–95. DOI: 10.1097/HJH.0000000000001359 [DOI] [PubMed] [Google Scholar]
- 26.Neutel JM, Smith DHG. Hypertension management: rationale for triple therapy based on mechanisms of action. Cardiovascular Therapeutics. 2013; 31(5): 251–8. DOI: 10.1111/1755-5922.12015 [DOI] [PubMed] [Google Scholar]
- 27.Kostis JB, Kim HJ, Rusnak J, Casale T, Kaplan A, Corren J, et al. Incidence and Characteristics of Angioedema Associated With Enalapril. Archives of Internal Medicine. 2005; 165(14): 1637–42. DOI: 10.1001/archinte.165.14.1637 [DOI] [PubMed] [Google Scholar]
- 28.ACE-inhibitors versus angiotensin receptor blockers for prevention of events in cardiovascular patients without heart failure — A network meta-analysis. International Journal of Cardiology. 2016; 217: 128–34. DOI: 10.1016/j.ijcard.2016.04.132 [DOI] [PubMed] [Google Scholar]
- 29.Li EC, Heran BS, Wright JM. Angiotensin converting enzyme (ACE) inhibitors versus angiotensin receptor blockers for primary hypertension. Cochrane Database of Systematic Reviews. 2014; 8: CD009096. DOI: 10.1002/14651858.CD009096.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bangalore S, Fakheri R, Toklu B, Ogedegbe G, Weintraub H, Messerli FH. Angiotensin-Converting Enzyme Inhibitors or Angiotensin Receptor Blockers in Patients Without Heart Failure? Insights From 254,301 Patients From Randomized Trials. Mayo Clinic Proceedings. 2016; 91(1): 51–60. DOI: 10.1016/j.mayocp.2015.10.019 [DOI] [PubMed] [Google Scholar]
- 31.Israili Z. Clinical pharmacokinetics of angiotensin II (AT1) receptor blockers in hypertension. Journal of Human Hypertension. 2000; 14(S1): S73–86. DOI: 10.1038/sj.jhh.1000991 [DOI] [PubMed] [Google Scholar]
- 32.Sica DA. Calcium Channel Blocker Class Heterogeneity: Select Aspects of Pharmacokinetics and Pharmacodynamics. The Journal of Clinical Hypertension. 2005; 7: 21–6. DOI: 10.1111/j.1524-6175.2006.04482.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Liang W, Ma H, Cao L, Yan W, Yang J. Comparison of thiazide-like diuretics versus thiazide-type diuretics: a meta-analysis. Journal of Cellular and Molecular Medicine. 2017; 21(11): 2634–42. DOI: 10.1111/jcmm.13205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Roush GC, Ernst ME, Kostis JB, Tandon S, Sica DA. Head-to-head comparisons of hydrochlorothiazide with indapamide and chlorthalidone: antihypertensive and metabolic effects. Hypertension. 2015; 65(5): 1041–6. DOI: 10.1161/HYPERTENSIONAHA.114.05021 [DOI] [PubMed] [Google Scholar]
- 35.Olde Engberink RHG, Frenkel WJ, van den Bogaard B, Brewster LM, Vogt L, van den Born BJH. Effects of Thiazide-Type and Thiazide-Like Diuretics on Cardiovascular Events and Mortality. Hypertension. 2015; 65(5): 1033–40. DOI: 10.1161/HYPERTENSIONAHA.114.05122 [DOI] [PubMed] [Google Scholar]
- 36.Roush GC, Holford TR, Guddati AK. Chlorthalidone Compared With Hydrochlorothiazide in Reducing Cardiovascular Events. Hypertension. 2012; 59(6): 1110–7. DOI: 10.1161/HYPERTENSIONAHA.112.191106 [DOI] [PubMed] [Google Scholar]
- 37.Thomas J. A review of 10 years of experience with indapamide as an antihypertensive agent. Journal of Hypertension. 1985; 7(6 pt 2): II152. DOI: 10.1161/01.HYP.7.6_Pt_2.II152 [DOI] [PubMed] [Google Scholar]
- 38.Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ. 2009; 338: b1665. DOI: 10.1136/bmj.b1665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Khin MU. FDA Briefing Document. Cardiovascular and Renal Drugs Advisory Committee Meeting September 10, 2014 To discuss the potential clinical utility of fixed combination prescription drugs composed of an antihypertensive drug, aspirin, and a statin administered to reduce the risk of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke in patients with a history of cardiovascular disease. 2014. [Google Scholar]
- 40.ClinicalTrials.gov. Efficacy and Safety of GMRx2 Compared to Placebo for the Treatment of Hypertension (GMRx2_PCT). https://classic.clinicaltrials.gov/ct2/show/NCT04518306?term=gmrx2&cond=gmrx2&draw=2&rank=1 (accessed 31 January 2024).
- 41.ClinicalTrials.gov. Efficacy and Safety of GMRx2 Compared to Dual Combinations for the Treatment of Hypertension (GMRx2_ACT). https://clinicaltrials.gov/study/NCT04518293?tab=results (accessed 31 January 2024).
- 42.Salam A, Atkins ER, Hsu B, Webster R, Patel A, Rodgers A. Efficacy and safety of triple versus dual combination blood pressure-lowering drug therapy. Journal of Hypertension. 2019; 37(8): 1567–73. DOI: 10.1097/HJH.0000000000002089 [DOI] [PubMed] [Google Scholar]
- 43.Lasserson DS, Buclin T, Glasziou PJH. How quickly should we titrate antihypertensive medication? Systematic review modelling blood pressure response from trial data. Heart. 2011; 97(21): 1771–5. DOI: 10.1136/hrt.2010.221473 [DOI] [PubMed] [Google Scholar]
- 44.Evaluation of pharmacokinetic drug interaction between telmisartan, amlodipine and indapamide when administered together as a fixed-dose combination in GMRx2. Available from: EudraCT No.: 2020-000648-68. Sponsor’s Study No.: GMRX2_Interaction CPA 527-20. [Google Scholar]
- 45.Effect of food on pharmacokinetics of telmisartan, amlodipine, and indapamide fixed-dose combination (GMRx2). Available from: EudraCT No.: 2021-002863-23. Sponsor’s Study No.: GMRX2_Food effect_01 CPA 533-21. [Google Scholar]
- 46.Anderson CS, Rodgers A, de Silva HA, Martins SO, Klijn CJ, Senanayake B, et al. Triple Therapy Prevention of Recurrent Intracerebral Disease Events Trial: Rationale, design and progress. International Journal of Stroke. 2022; 17(10): 1156–1162. DOI: 10.1177/17474930211068671 [DOI] [PubMed] [Google Scholar]
- 47.Salam A, Huffman MD, Kanukula R, Hari Prasad E, Sharma A, Heller DJ, et al. Two-drug fixed-dose combinations of blood pressure-lowering drugs as WHO essential medicines: An overview of efficacy, safety, and cost. The Journal of Clinical Hypertension. 2020; 22(10): 1769–1779. DOI: 10.1111/jch.14009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Khatib R, McKee M, Shannon H, Chow C, Rangarajan S, Teo K, et al. Availability and affordability of cardiovascular disease medicines and their effect on use in high-income, middle-income, and low-income countries: an analysis of the PURE study data. The Lancet. 2016; 387(10013): 61–9. DOI: 10.1016/S0140-6736(15)00469-9 [DOI] [PubMed] [Google Scholar]
- 49.Adeloye D, Basquill C. Estimating the Prevalence and Awareness Rates of Hypertension in Africa: A Systematic Analysis. PLoS ONE. 2014; 9(8): e104300. DOI: 10.1371/journal.pone.0104300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Dzudie A, Rayner B, Ojji D, Schutte AE, Twagirumukiza M, Damasceno A, et al. Roadmap to achieve 25% hypertension control in Africa by 2025. Cardiovascular Journal of Africa. 2017; 28(4): 262–272. DOI: 10.5830/CVJA-2017-040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Committee for Medicinal Products for Human Use (CHMP). Guideline on clinical investigation of medicinal products in the treatment of hypertension. EMA/CHMP/29947/2013/Rev. 4. 23 June 2016; 2016. [Google Scholar]
- 52.Peters R, Xu Y, Fitzgerald O, Aung HL, Beckett N, Bulpitt C, et al. Blood pressure lowering and prevention of dementia: an individual patient data meta-analysis. European Heart Journal. 2022; 43(48): 4980–90. DOI: 10.1093/eurheartj/ehac584 [DOI] [PubMed] [Google Scholar]
- 53.World Health Organization. Global report on hypertension: the race against a silent killer. https://www.who.int/publications/i/item/9789240081062 (accessed 31 January 2024).
- 54.Hong SJ, Sung KC, Lim SW, Kim SY, Kim W, et al. Low-Dose Triple Antihypertensive Combination Therapy in Patients with Hypertension: A Randomized, Double-Blind, Phase II Study. Drug Design, Development and Therapy. 2020; 14: 5735–5746. DOI: 10.2147/DDDT.S286586 [DOI] [PMC free article] [PubMed] [Google Scholar]