

Abstract
Background:
Yoga therapy (YT) as an adjunct treatment has reportedly been demonstrated to offer clinical benefits in major depressive disorder (MDD). Although a few biological pathways are suggested to mediate the effects of yoga, the precise mechanistic basis remains unknown. Oxidative stress pathway activation has consistently been linked to the pathobiology of MDD. Whether YT has a modulatory effect on the oxidative stress pathway in MDD is not adequately understood.
Aim and Objectives:
In this study, we examined the impact of a course (3 months) of yoga as an add on therapy on the markers of the oxidative stress pathway in MDD patients.
Methods:
Thirty-three MDD patients were randomized to the YT (n = 16) and waitlist control (WC) (n = 17) groups. Colorimetric estimation of the plasma malondialdehyde (MDA) and total antioxidant (AO) levels was performed in all the study participants using commercially available kits at the baseline and after 3 months.
Results:
A significant reduction of plasma MDA levels was observed in MDD patients of YT group (P = 0.05) after 3 months of YT. Notably, the plasma MDA levels also decreased in MDD patients of WC group (P = 0.015) after the trial period. In addition, levels of total AO showed a trend toward significance only in MDD patients after 3 months of YT (P = 0.07). Conclusion: The current study suggests that the benefits of YT might be mediated through its modulatory role on the oxidative stress pathway in MDD.
Keywords: Antioxidants, major depressive disorder, oxidative stress, yoga therapy
Introduction
Major depressive disorder (MDD), a complex and highly relapsing-remitting illness, is associated with considerable functional impairment. Although antidepressants improve the symptoms in the majority of patients, their use is associated with a number of adverse effects, and >50% patients either do not respond or respond partially to the medications.[1] This has necessitated the exploration of alternative treatment modalities that may help achieve better remission in patients with MDD.
Yoga therapy (YT) has reportedly shown overwhelming clinical benefits as an adjunct treatment for depression.[2,3] Further support for the beneficial effects of YT on MDD was provided by empirical studies on the levels of neurotransmitters like gamma aminobutyric acid as well as neurotrophins like brain-derived neurotrophic factor.[4,5] One of the widely recognized etiopathological pathways of MDD is oxidative dysregulation. Multiple studies, including meta-analyses, suggested increased oxidative stress and decreased antioxidant (AO) defenses in MDD.[6,7] It is not adequately known whether the clinical benefits of YT in MDD is mediated through the downregulation of the oxidative stress pathway. In a recent study, yoga and meditation-based lifestyle intervention were shown to reduce the severity of depression and this was accompanied by decreased levels of reactive oxygen species (ROS) and 8-hydroxy-2-deoxyguanosine, as well as increased total AO levels in patients with MDD.[8] However, the impact of YT on lipid peroxidation, a potential indicator of ROS-induced damage to cell membranes, has not been examined so far in MDD. Malondialdehyde (MDA) is an end product of polyunsaturated fatty acid peroxidation and is commonly used to assess oxidative stress. Thiobarbituric acid reactive substance (TBARS) method is used to measure the levels of MDA. Herein, in this study, we examined the impact of 3-months YT on the levels of MDA and total AO in MDD patients using a validated MDD-specific yoga module to understand the modulatory role of yoga on the oxidative stress pathway in MDD.
Study Participants and Methods
This randomized controlled trial was conducted to examine the impact of 3-month therapy, adjunct to antidepressant treatment on the plasma profile of MDA and total AO in MDD patients at NIMHANS, Bengaluru, India. Screening of all the participants was carried out using Mini International Neuropsychiatric Interview. Thirty-six MDD patients (male [n = 16]; female [n = 20] and mean age: 32.5 ± 8.5 years) with a Hamilton Depression Rating Scale (HAMD) score ≥18 were recruited and randomized to YT and waitlist control (WC) groups. However, only those patients who completed the 12-weeks trial period and with analyzable plasma samples were considered for the analysis. The final analysis was carried out on the data obtained from 16 MDD patients of YT group and 17 MDD patients of WC group. This study was initiated after obtaining the institute ethics committee’s approval (No: NIMHANS/IEC [BS and NS DIV.]) 5th Meeting/2017, dated-March 22, 2017] as well as written informed consent from all the participants. The study was registered in the Clinical Trials Registry India (No.CTRI/2017/07/009070). The HAMD, Clinical Global Impression (CGI), and Montgomery-Asberg Depression Rating Scale (MADRS) were used for clinical assessments at baseline as well as at the end of the 1st, 2nd, and 3rd months by trained clinicians.
Intervention
Patients with MDD in the YT group underwent YT for 12 weeks using a generic yoga module, validated for depression and the duration of each yoga session was 52 min [Table 1].[9] The patients were taught yoga steps by a trained yoga teacher for twelve sessions in the 1st 4 weeks in the NIMHANS Integrated Centre for Yoga (NICY), NIMHANS, Bengaluru, followed by home-based yoga practice for at least 4 days a week for the remaining 2 months. Two booster sessions were given in the 2nd and 3rd months at the NICY. Overall, the patients performed 48–72 sessions of yoga (4–6 per week for 12-weeks), of which 16 sessions were completed under the direct supervision of the yoga instructor. The patients in the WC group received antidepressants as per the guidelines followed for routine clinical treatment of MDD and no changes in medications were made during the entire study period. The recruited patients were stabilized on antidepressants for a minimum duration of 2 weeks. All the patients were on selective serotonin reuptake inhibitors, in the standard therapeutic doses, and were on the same dose throughout the study period. The patients were on either T. Escitalopram (15–20 mg) or T. Fluoxetine (20–40 mg) or T. Sertraline (50–150 mg). A psychiatrist regularly monitored the clinical improvement in these patients. If any of the patients needed treatment changes, the required changes were made and they were dropped out from the study. Study participants in the WC group were offered the same yoga module after the trial period of 12 weeks. The study design is depicted in Figure 1.
Table 1.
Yoga module for depression
| Steps | Practices | Description | Duration (min) |
|---|---|---|---|
| 1 | Preparatory practices Sukshma and sthula vyayama Suryanamaskara (3 rounds) | Loosening exercises | 15 |
| 2 | Shavasana | 2 | |
| 3 | Asanas and mudra | ||
| Standing posture | Ardha chakrasana | 2 | |
| Sitting postures | Ushtrasana Paschimottanasana | 4 | |
| Prone posture | Bhujangasana | 2 | |
| Shavasana | 2 | ||
| Supine postures | Pavanamukthasana Viparithakarani mudra Sethubandasana | 6 | |
| 4 | Shavasana (QRT) | 4 | |
| 5 | Kriya | Kapalabhati | 2 |
| 6 | Pranayama | Suryanulomaviloma Ujjayi Bhastrika | 10 |
| 7 | Pranava Japa | AUM chanting | 3 |
QRT: Quick relaxation technique
Figure 1.
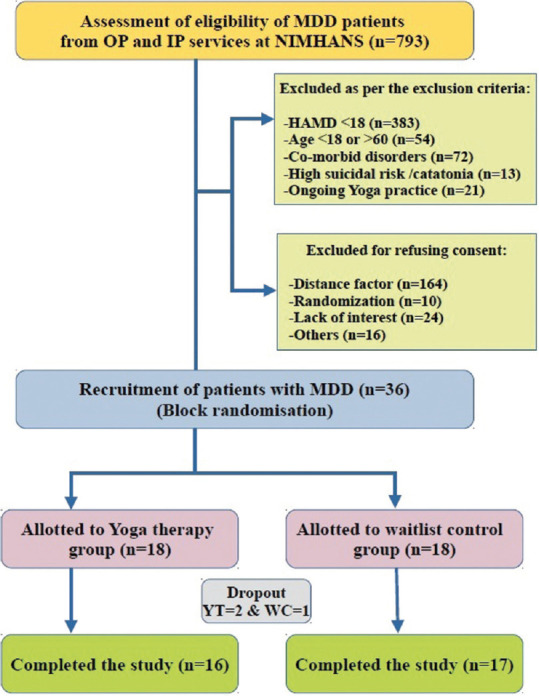
Study outline. MDD: Major depressive disorder, HAMD: Hamilton Depression Rating Scale, YT: Yoga therapy, WC: Waitlist control
Blood sample collection
Peripheral blood (approximately 10 mL) was collected by venepuncture into ethylenediaminetetraacetic acid-coated vacutainers from all the participants at two time points, i.e., at baseline and after the trial period. The clinical assessments were done at four time points, i.e., at the baseline and at the end of 1st, 2nd, and 3rd months. Plasma samples were collected by centrifugation of the blood samples at 4°C for 10 min at 4000 RPM in a refrigerated centrifuge (Make: Eppendorf, Model No.:5430R). The separated plasma samples were aliquoted and stored in −80°C deep freezer.
Measurement of levels of malondialdehyde and total antioxidant in plasma samples
The levels of the marke of oxidative stress were measured by determining MDA, which is one of the end products of lipid peroxidation. The MDA level was quantified colorimetrically in the plasma samples using a commercially available TBARS Assay Kit (Cat No. 100009055, Cayman Chemicals, USA) following the manufacturer’s guidelines in all the study participants at baseline and after 3 months. The dynamic range of the kit was 0–50 μM. In 7 mL glass tubes, plasma sample (100 μL) and serially diluted MDA standards were taken separately, followed by the addition of 100 uL of sodium dodecyl sulfate solution and these were mixed by swirling. 4 mL of the color reagent, prepared by adding TBA to a mixture of sodium hydroxide and acetic acid, was added. The glass tubes were kept in a boiling water bath at 100° C for 1 h. The glass tubes were then placed in ice for 10 min to stop the reaction, followed by centrifugation at 1600 × g for 10 min at 4°C. 150 μL of reaction mixture from each glass tube was loaded into a clear 96-well plate and the absorbance was measured at 530–540 nM in a plate reader (Multiskan Go, Thermo Scientific, USA). The standard curve was plotted using the absorbance measured for the standards and the MDA levels in the plasma samples were calculated using the linear regression equation obtained from the standard curve. The assays were performed in duplicate.
The total AO in the plasma samples of all the study participants were assayed colorimetrically using a commercially available AO Assay Kit (Cat No. 709001, Cayman Chemicals, USA) following the manufacturer’s guidelines at baseline and after 3 months. The dynamic range of the kit was 0.068–0.495 mM. Plasma samples were diluted 1:20 using the assay buffer provided in the kit. Trolox standards were prepared by serial dilution. Into each well of a 96-well plate, 10 μL of the standards and diluted plasma sample were added. In addition, 10 μL of metmyoglobin along with 150 μL of chromogen was added to each well of the plate. The reaction was initiated by quickly adding 40 μL of hydrogen peroxide. The plate was then incubated for 5 min on a shaker at room temperature and the absorbance was measured at 750 nM in a plate reader (Multiskan Go, Thermo Scientific, USA). The standard curve plotted using the Trolox standards was used to generate the equation for the slope (linear regression). The AO concentration of the samples was calculated by substituting the absorbance value in the slope equation. All samples were analyzed in duplicate.
Statistical analysis
All the statistical analyses were carried out by using Statistical Package for the Social Sciences (version-16) IBM SPSS Statistics for Windows, Version 16.0. Armonk, NY: IBM Corp. The levels of MDA and AO followed normal distribution. Therefore, parametric paired sample t-test was applied. The significance was set at P < 0.05 (two-tailed).
Results
There were no differences in the age and gender between MDD patients of YT and WC groups (P > 0.9). The patients of both the groups also did not differ significantly on the clinical parameters such as age at onset, illness duration, number of past episodes, CGI, MADRS score, and HAMD score (all P > 0.06) at baseline. Lower mean HAMD scores were seen in MDD patients of the YT group in comparison to the patients of the WC group at the end of the trial period (mean ± standard deviation [SD], YT = 4.13 ± 2.63; WC = 6.94 ± 4.94; P = 0.05). More number of MDD patients of the YT group achieved complete remission (HAMD <7) compared to WC (YT = 81% and WC = 53%) at the end of the trial. Similarly, the MADRS scores when compared between the groups, the patients in YT group scored lower than the WC (Mean ± SD, YT = 4.69 ± 3.02; WC = 9.00 ± 7.22; P = 0.03). The patients in the YT group also had lower CGI scores than patients in WC (mean ± SD, YT = 1.56 ± 0.62; WC = 2.29 ± 1.35; P = 0.06). The lower scores in HAMD, CGI, and MADRS scales indicate improvement of the symptoms of depression. Notably, MDD patients in the YT group showed significantly better improvement, indexed by HAMD and MADRS scores.
Significant differences were observed for the markers of oxidative stress pathway in MDD patients of both the YT and WC groups between baseline and at the end of the trial period. Significant reduction in the plasma levels of MDA was observed in MDD patients of both the YT (P = 0.05) and WC (P = 0.015) groups after the trial period [Table 2]. The plasma total AO levels showed a trend toward significance in MDD patients of YT group after 3 months of YT (P = 0.07). The levels of MDA and total AO did not correlate with the clinical rating scales and phenotypes. Paired t-test was performed to assess the differences in plasma levels of MDA and total AO between MDD patients of YT and WC groups at baseline as well as after the trial period. The levels of MDA and total AO did not differ between YT and WC groups at baseline; however, MDA levels were significantly higher in the WC group compared to the YT group after the trial period [Table 3].
Table 2.
Plasma levels of malondialdehyde and total antioxidant in the major depressive disorder patients of yoga therapy and waitlist control groups at baseline and after the trial period
| Oxidative stress markers | MDD patients in YT, mean±SD | t # | P | |
|---|---|---|---|---|
|
| ||||
| At baseline (n=16) | Post yoga (n=16) | |||
| MDA | 9.2±4.7 | 6.5±0.99 | 2.101 | 0.05 |
| Total antioxidant content | 7.29±3.5 | 7.84±2.9 | −1.926 | 0.07 |
|
| ||||
| Oxidative stress markers | MDD patients in the WC group, mean±SD | t # | P | |
|
| ||||
| At baseline (n=17) | After the trial period (n=17) | |||
|
| ||||
| MDA | 9.3±3.0 | 7.5±2.0 | 2.785 | 0.015 |
| Total antioxidant content | 8.32±3.26 | 7.9±3.26 | 0.720 | 0.48 |
#Paired sample t-test. The significance was set at P<0.05 (two-tailed). SD: Standard deviation, MDA: Malondialdehyde, MDD: Major depressive disorder, WC: Waitlist control, YT: Yoga therapy
Table 3.
Intergroup comparison of plasma levels of malondialdehyde and total antioxidant in major depressive disorder patients at baseline and after the trial period
| Oxidative stress markers | Baseline analysis, mean±SD | t # | P | |
|---|---|---|---|---|
|
| ||||
| Yoga group (n=16) | Waitlist group (n=17) | |||
| MDA | 9.2±4.7 | 9.3±3.0 | −0.77 | 0.24 |
| Total antioxidant content | 7.29±3.5 | 8.32±3.26 | −0.87 | 0.38 |
|
| ||||
| Oxidative stress markers | Analysis after 12 weeks of trial period, mean±SD | t # | P | |
|
| ||||
| Yoga group (n=16) | Waitlist group (n=17) | |||
|
| ||||
| MDA | 6.5±0.99 | 7.5±2.0 | −0.173 | 0.03 |
| Total antioxidant content | 7.84±2.9 | 7.9±3.26 | −0.101 | 0.26 |
#Independent sample t-test, The significance was set at P<0.05 (two-tailed). SD: Standard deviation, MDA: Malondialdehyde
Discussion
YT is increasingly being considered a valuable nonpharmacological treatment modality for MDD.[10,11] In the current study, 12-week add-on YT was found beneficial in improving symptoms of MDD, especially by lowering the HAMD scores and increasing remission rates. In addition, 12-week add-on YT was found to significantly reduce the levels of MDA and also increase the total AO levels in MDD patients. These findings appear important given the fact that the oxidative stress pathway contributes to the risk and progression of MDD by altering multiple pathways/systems including microvascular dysfunction and neuroprogression.[12,13] Notably, increased lipid peroxidation, measured by TBARS, was reported in treatment-resistant depression and was suggested as a trait marker of depression.[14] Thus, YT offering clinical benefits by modulating a trait marker of MDD adds more dimension to the biological mode of action and the usefulness of yoga.
The oxidative stress pathway has reciprocal functional interactions with other pathways such as the immune-inflammatory pathway.[15] Converging evidence indicates a predominant role of the immune-inflammatory pathway in MDD.[16] In our recent study, YT resulted in the reduction of the levels of complement proteins such as complement component 1q (C1q), Factor H, and properdin in the plasma of MDD patients, implying its modulatory effects also on inflammatory pathway.[17] It is noteworthy that a combined immune-inflammatory and oxidative as well as nitrosative stress (IO and NS) pathway has emerged as a predominant underlying mechanism and target for the treatment of MDD.[14,18,19] Therefore, an intervention targeting the IO and NS pathway will offer greater clinical benefits in MDD. The present study suggests a role of YT on oxidant-AO balance, while the previous study[17] indicated an immunomodulatory effect of YT in MDD. Based on the findings of both the studies, YT seems to have the potential to emerge as an important intervention having modulatory effects on IO and NS pathway in MDD.
Conclusion
Proven clinical benefits of YT in MDD are evident in multiple clinical studies. However, there exists a considerable lack of understanding whether yoga offers clinical benefits by modulating the activities of a pathway that has pathobiological relevance in MDD. The modulatory effect of YT on oxidative stress pathway observed in this study provides empirical evidence toward biological mode of action of YT in MDD. Additional studies, comprising a large cohort of MDD patients as well as other markers of oxidative and nitrosative stress pathway, will be useful in validating the importance of these preliminary findings.
Author contributions
Talukdar PM: Data curation. Reddy VR: Data curation, data analysis and interpretation, and drafting of the tables and figures. Bhargav PR: Data curation. Subbanna M: Data curation and analysis. Karmani S: Data curation and fund acquisition. Arasappa R: Data curation and analysis and revision to the manuscript. Venkatasubramanian G: Data interpretation and revision to the manuscript and fund acquisition. Muralidharan K: Conception and design of the study, data curation and interpretation, revision to the manuscript, and fund acquisition. Debnath M: Conception and design of the study, data curation and interpretation, drafting of the article, and fund acquisition.
Financial support and sponsorship
This study was supported financially by a grant from the Department of Science and Technology, Government of India (Grant No: SR/SATYAM/351/2015), under Science and Technology of Yoga and Meditation and the NIMHANS Centre for Integrative Medicine (NICY), NIMHANS, Bengaluru, India.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A star*d report. Am J Psychiatry. 2006;163:1905–17. doi: 10.1176/ajp.2006.163.11.1905. [DOI] [PubMed] [Google Scholar]
- 2.Prathikanti S, Rivera R, Cochran A, Tungol JG, Fayazmanesh N, Weinmann E. Treating major depression with yoga: A prospective, randomized, controlled pilot trial. PLoS One. 2017;12:e0173869. doi: 10.1371/journal.pone.0173869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gangadhar BN, Naveen GH, Rao MG, Thirthalli J, Varambally S. Positive antidepressant effects of generic yoga in depressive out-patients: A comparative study. Indian J Psychiatry. 2013;55:S369–7. doi: 10.4103/0019-5545.116312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Streeter CC, Gerbarg PL, Brown RP, Scott TM, Nielsen GH, Owen L, et al. Thalamic gamma aminobutyric acid level changes in major depressive disorder after a 12-week Iyengar yoga and coherent breathing intervention. J Altern Complement Med. 2020;26:190–7. doi: 10.1089/acm.2019.0234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Aditi Devi N, Phillip M, Varambally S, Christopher R, Gangadhar BN. Yoga as a monotherapy alters proBDNF –Mature BDNF ratio in patients with major depressive disorder. Asian J Psychiatr. 2023;81:103429. doi: 10.1016/j.ajp.2022.103429. [DOI] [PubMed] [Google Scholar]
- 6.Jiménez-Fernández S, Gurpegui M, Díaz-Atienza F, Pérez-Costillas L, Gerstenberg M, Correll CU. Oxidative stress and antioxidant parameters in patients with major depressive disorder compared to healthy controls before and after antidepressant treatment: Results from a meta-analysis. J Clin Psychiatry. 2015;76:1658–67. doi: 10.4088/JCP.14r09179. [DOI] [PubMed] [Google Scholar]
- 7.Black CN, Bot M, Scheffer PG, Cuijpers P, Penninx BW. Is depression associated with increased oxidative stress?A systematic review and meta-analysis. Psychoneuroendocrinology. 2015;51:164–75. doi: 10.1016/j.psyneuen.2014.09.025. [DOI] [PubMed] [Google Scholar]
- 8.Tolahunase MR, Sagar R, Faiq M, Dada R. Yoga- and meditation-based lifestyle intervention increases neuroplasticity and reduces severity of major depressive disorder: A randomized controlled trial. Restor Neurol Neurosci. 2018;36:423–42. doi: 10.3233/RNN-170810. [DOI] [PubMed] [Google Scholar]
- 9.Naveen GH, Rao MG, Vishal V, Thirthalli J, Varambally S, Gangadhar BN. Development and feasibility of yoga therapy module for out-patients with depression in India. Indian J Psychiatry. 2013;55:S350–6. doi: 10.4103/0019-5545.116305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wu Y, Yan D, Yang J. Effectiveness of yoga for major depressive disorder: A systematic review and meta-analysis. Front Psychiatry. 2023;14:1138205. doi: 10.3389/fpsyt.2023.1138205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bridges L, Sharma M. The efficacy of yoga as a form of treatment for depression. J Evid Based Complementary Altern Med. 2017;22:1017–28. doi: 10.1177/2156587217715927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Greaney JL, Saunders EF, Santhanam L, Alexander LM. Oxidative stress contributes to microvascular endothelial dysfunction in men and women with major depressive disorder. Circ Res. 2019;124:564–74. doi: 10.1161/CIRCRESAHA.118.313764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Vaváková M, Ďuračková Z, Trebatická J. Markers of oxidative stress and neuroprogression in depression disorder. Oxid Med Cell Longev. 2015;2015:898393. doi: 10.1155/2015/898393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sowa-Kućma M, Styczeń K, Siwek M, Misztak P, Nowak RJ, Dudek D, et al. Lipid peroxidation and immune biomarkers are associated with major depression and its phenotypes, including treatment-resistant depression and melancholia. Neurotox Res. 2018;33:448–60. doi: 10.1007/s12640-017-9835-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Morgan MJ, Liu ZG. Crosstalk of reactive oxygen species and NF-kB signaling. Cell Res. 2011;21:103–15. doi: 10.1038/cr.2010.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Miller AH, Raison CL. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat Rev Immunol. 2016;16:22–34. doi: 10.1038/nri.2015.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Subbanna M, Talukdar PM, Abdul F, Debnath M, Reddy PV, Arasappa R, et al. Long-term add-on yoga therapy offers clinical benefits in major depressive disorder by modulating the complement pathway: A randomized controlled trial. Asian J Psychiatr. 2021;66:102876. doi: 10.1016/j.ajp.2021.102876. [DOI] [PubMed] [Google Scholar]
- 18.Lindqvist D, Dhabhar FS, James SJ, Hough CM, Jain FA, Bersani FS, et al. Oxidative stress, inflammation and treatment response in major depression. Psychoneuroendocrinology. 2017;76:197–205. doi: 10.1016/j.psyneuen.2016.11.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Maes M. The cytokine hypothesis of depression: Inflammation, oxidative and nitrosative stress (IO and NS) and leaky gut as new targets for adjunctive treatments in depression. Neuro Endocrinol Lett. 2008;29:287–91. [PubMed] [Google Scholar]