

Abstract
Purpose:
The aim of this study was to analyze current radiology practice types, specific subspecialty needs, employment trends, and retirement trends.
Methods:
ACR members, nonmembers, and Radiology Business Management Association members were surveyed using predominantly structured closed-ended questions about a variety of current and recent radiology practice characteristics. Responses were group practice deduplicated and weighted.
Results:
Of 1,702 survey respondents, 64% were men, with a median age of 51 years. In 2021, 62% of responding practices hired radiologists, with the average practice hiring 2 radiologists and academic practices on average hiring the most (3.5). Most radiologists (87%) were hired for full-time positions, with independent practices hiring the largest proportion of part-time positions. Body and breast imagers represented the largest numbers of hired radiologists (17% each). Practices anticipated similar hiring patterns in 2022, prioritizing breast (37%) and body (35%) imaging. Of all practice types, academic groups were least likely to prioritize general radiologist hiring. A large majority (82%) of radiology practices permit remote work (teleradiology), more common at academic than other practices. Of currently employed radiologists, 16% plan to seek new employment in the next year; early-career radiologists indicated the highest likelihood (92%) and academic radiologists the lowest (66%) of remaining in the same practice for at least 5 years. A large majority of practices (80%) reported no radiologist retirements in 2021. Of those retiring, the average age was 75 years, and 66% worked full-time until retirement.
Conclusions:
Radiologist recruiting remains robust. Current information on practice characteristics may help inform radiology practice leaders seeking to right-size their groups.
Keywords: Human resources, workforce, hiring, recruitment, practice management
Graphical Abstract
INTRODUCTION
Given an expected shortage of between 37,800 and 124,00 physicians by 2034 as the US population ages [1], and the increasing need for medical care supported by radiologic services [2], ongoing radiologist workforce information is necessary to optimize patient access to imaging. In addition, the radiologist workforce has become increasingly mobile [3], which necessitates a more sophisticated understanding of practice hiring and staffing patterns. Imaging volumes continue to increase over time, and physician burnout is higher among radiologists than other physicians [4,5], potentially contributing to early retirement and radiologist attrition [6,7] and further exacerbating a critical workforce shortage. Finally, radiology groups report difficulty not only hiring radiologists in general but also hiring radiologists with appropriate subspecialty skills to meet their specific practice and broader population needs [8].
From 2012 [9] to 2019 [10], the ACR Commission on Human Resources (HR Commission) conducted an annual workforce survey deployed to radiology practice managers and leaders within the United States to assess the employment and hiring patterns of radiology professionals for market research purposes. The ACR Practice of Radiology Environment Database nationwide was used to identify practice leaders, who were asked to complete an electronic survey internally developed by the HR Commission with the support of an outside consultant [9,10].
Because of the coronavirus disease 2019 pandemic in 2020, the HR Commission did not conduct a survey and instead updated the annual workforce questions with revised survey methodology for 2021. This new survey was conducted as a partnership between the Radiology Business Management Association (RBMA) and the ACR’s HR Commission. The aim of the study was to understand radiology practice types, specific subspecialty needs, employment trends, and retirement trends. Such information could inform predictions about future shortages and oversupplies of radiologists and thus help optimize future patient care. We anticipate that the results of this survey will also serve as a baseline comparison for future planned annual workforce surveys by the ACR’s HR Commission.
METHODS
Sample Sources
The sample was multisourced and drew from the ACR member database (n = 30,440), nonmembers in the ACR member database (n = 13,015) and RBMA members (n = 1,736). These sample sources were compared, and duplicate records occurring in both the ACR and RBMA were removed.
Questionnaire Construction
The 2021 ACR Workforce Survey questionnaire was constructed using predominantly structured, closed-ended questions, with some questions requiring limited numeric entry (Appendix 1). Study questions were tailored to three types of respondents: fully qualified, partially qualified, and retired.
Respondent Categorization
Fully qualified respondents were defined as employed either part-time or full-time or were residents or fellows and self-reported that they had at least some input into hiring decisions made at the practice level. Fully qualified respondents answered all questions asked of partially qualified respondents and provided practice-level counts of physicians and nonphysicians across dimensions of demography, subspecialty of radiology, full-time and part-time work dynamics, hiring, prospective hiring, and retirements. Fully qualified respondents were specifically asked to focus on the radiology practice and, in cases in which their employers served other functions, to base their answers on knowledge of the radiology function only.
Partially qualified respondents were defined as employed radiologists or residents or fellows who self-reported that they had no input into decision making at the practice level. Partially qualified respondents answered questions regarding demography, practice type, clinical time spent in subspecialty work, telework, tenure, likelihood of seeking new employment, and preference.
Retired respondents indicated their status at screening and were branched to unique questions regarding retirement status.
“Disqualified” respondents included radiologists who self-reported that they were furloughed or otherwise not working, locum tenens physicians, and interns (vs residents or fellows; see Appendix 1), all of whom answered only demographic questions.
Early-career radiologists were defined as radiologists within the first 8 years of practice after residency and fellowship training.
Sample Development and Weighting Protocol
The invitation to participate was sent to the full member databases of both the ACR and the RBMA with the intention to weight the data in accordance with respondent type populations, thereby producing a stratified, representative sample of this population. Weighting ensures that the ending sample accurately reflects the population of which it is a subset. Demographic markers used to develop the appropriate proportional weights included data collected in the previous ACR member tracker, including age, gender, region, and specialty (eg, diagnostic radiology, interventional radiology).
The proportions of demographic groups were determined using the 2021 ACR membership tracker and data on board-certified radiologists developed by the American Board of Medical Specialties. These proportions were used in developing appropriate weights for geographic distributions and demographic proportions within radiology [11]. Given the population from which the sample and the consequent completions were derived, the margin of error for the statistics shown from this study, at the 95% confidence level, is ±2.3%.
Data Collection
The survey was conducted online during October and November 2021 by an independent, third-party market research firm.
Pretesting
Pretesting was performed on October 11, 2021. The questionnaire was e-mailed to a small subset of the overall sample list (11% of the original sample, or 5,000 individuals [3,368 from the ACR member database, 1,440 ACR nonmembers, and 192 from the RBMA sample]). Pretest results were evaluated the next day by ACR staff members and consultants from the third-party market research firm.
Findings from the pretest assisted in the finalization of the survey instrument; improvements were made to the structure and flow that made the experience of completing the survey easier and less complex for respondents.
Deduplication
An additional quality-control measure was implemented before data collection, namely, that fully qualified responses were analyzed to determine how many unique establishments (because respondents may not be from what one might strictly define as a practice, the term establishment is used instead of practice) were represented in the survey data to avoid duplicate responses from the same practices. Factors such as organization name, city and state, practice type, role, number of locations, and number of physicians were all scrutinized. Three rules were established to identify duplicate practices. These rules aimed to identify survey responses that were (1) substantially similar (containing more identical Workforce Survey responses than not), (2) substantially similar or identical regarding the name of the practices, or (3) substantially similar or identical geographical location. If two of three conditions were met, responses were classified as duplicate establishments. When determining which response to include in establishment-level analysis, the focus of the role indicated by each respective respondent was used to determine which respondent was better able to describe the practice. Those who identified themselves as partners or owners were given precedence over those who identified themselves practitioners or clinicians, while CEOs, chief operating officers, and chairs were given precedence over business managers and accounting professionals. Establishment analysis indicated that 2021 Workforce Survey data represent 376 unique establishments.
Full Survey
The full survey was fielded on October 28, 2021. At the same time, first reminders were sent to those who were provided the survey during pretesting. The first reminder for the fully launched survey was sent to those who had not completed the survey on November 8, 2021, with a second reminder sent on November 15, 2021. The survey was closed to respondents on November 30, 2021.
RESULTS
Survey Sample
A survey was sent to 1,736 RBMA members, 30,440 ACR members, and 13,015 ACR nonmembers, with receipt of 1,702 total survey responses. This included 407 decision makers from both ACR and RBMA member databases (fully qualified) representing 376 unique practices, 987 non–decision makers or “rank and file” radiologists (partially qualified), and 308 retired ACR members, representing 376 unique radiology practices across multiple practice settings.
Sixty-four percent of radiologists were men, 28% were women, and <1% represented all other genders. The median age of survey respondents was 51 years (men, 51 years; women, 48 years). Eighteen percent of respondents were younger than 35 years, 33% were 35 to 45 years of age, 18% were 46 to 55 years of age, 15% were 56 to 65 years of age, and 17% were older than 65 years.
Survey Length
The mean length of interview (LOI) for fully qualified respondents was 19.2 min, and the median LOI was 15.7 min. LOIs for partially qualified and retired respondents were 5 min or less.
Hiring Patterns in 2021
Sixty-two percent of practices hired radiologists in 2021. On average, practices hired 2 radiologists in 2021, with academic practices hiring the largest average number (3.5). Forty-five percent of radiologists hired in 2021 were hired by independent private practices. Academic practices hired 27% of radiologists. National radiology practices, entities, or cooperatives that are partially or wholly supported by private equity or venture capital (national and management services organization [MSO]); hospitals, hospital systems, or hospital-affiliated physician practice groups (hospital and system); and uniformed or US Department of Veterans Affairs (VA) practices hired smaller percentages of radiologists (Fig. 1). Eighty-seven percent of hired radiologists were hired full-time. Thirteen percent of radiologists hired in 2021 were hired for part-time work. Of hired full-time radiologists, 37% were hired by independent private practices. Other practice types hired smaller percentages of full-time radiologists (Fig. 1). Independent private practices hired the largest proportion of part-time radiologists (6% of hires), while academic practices hired 3%. Other practice types hired much smaller proportions of the part-time radiologists (Fig. 1).
Fig. 1.
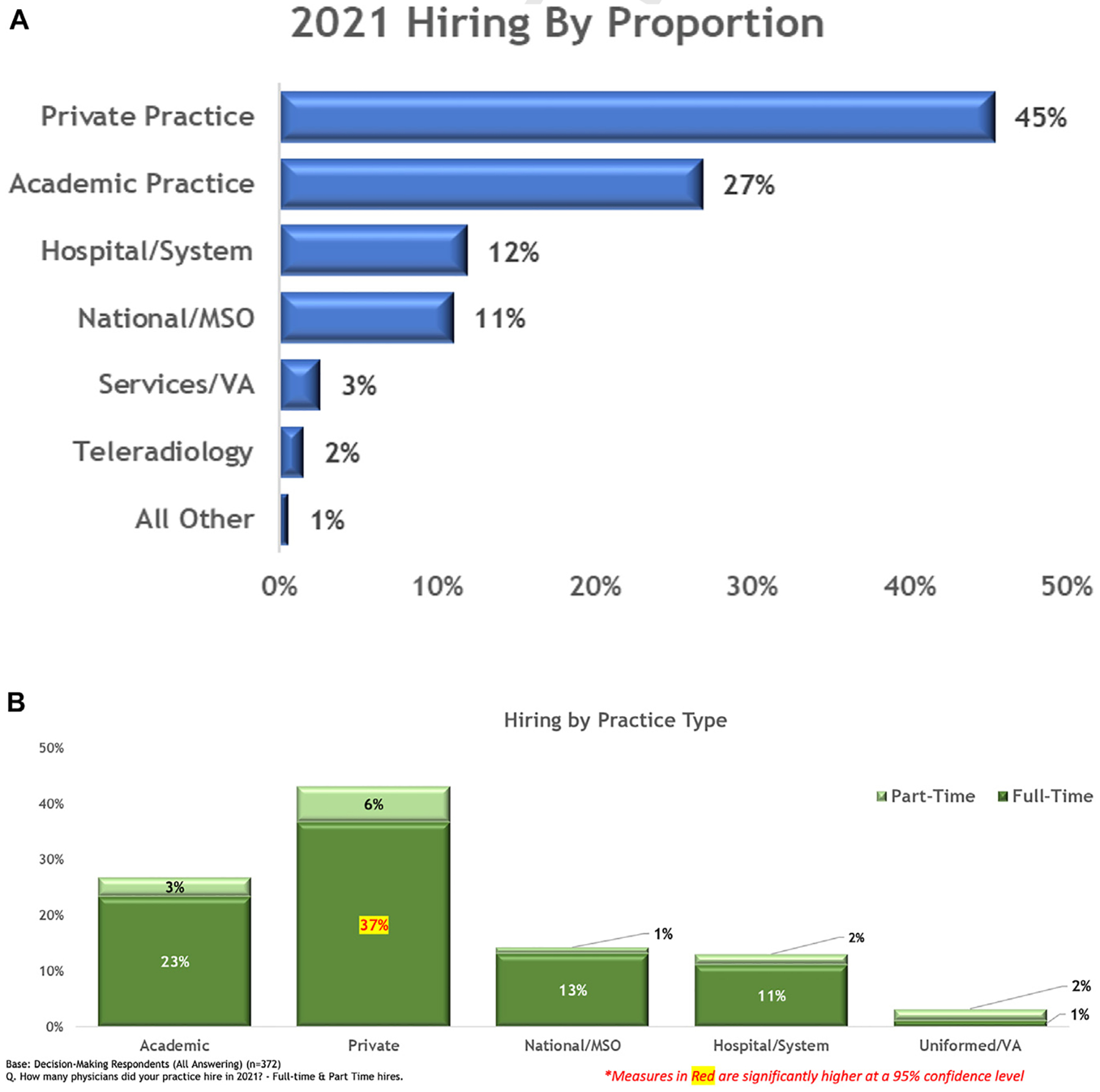
(A) Hiring in 2021 by proportion. (B) Part-time versus full-time hiring by practice type. Other practice types were <1% and are not included in the figure. MSO = management services organization; VA = US Department of Veterans Affairs.
Body imaging radiologists and breast imaging radiologists represented the largest proportion hired in 2021 (17% each). Neuroradiologists and interventional radiologists were also among the top subspecialties hired in 2021 (Fig. 2). Hiring in 2021 by subspecialty and practice type is summarized in Table 1.
Fig. 2.
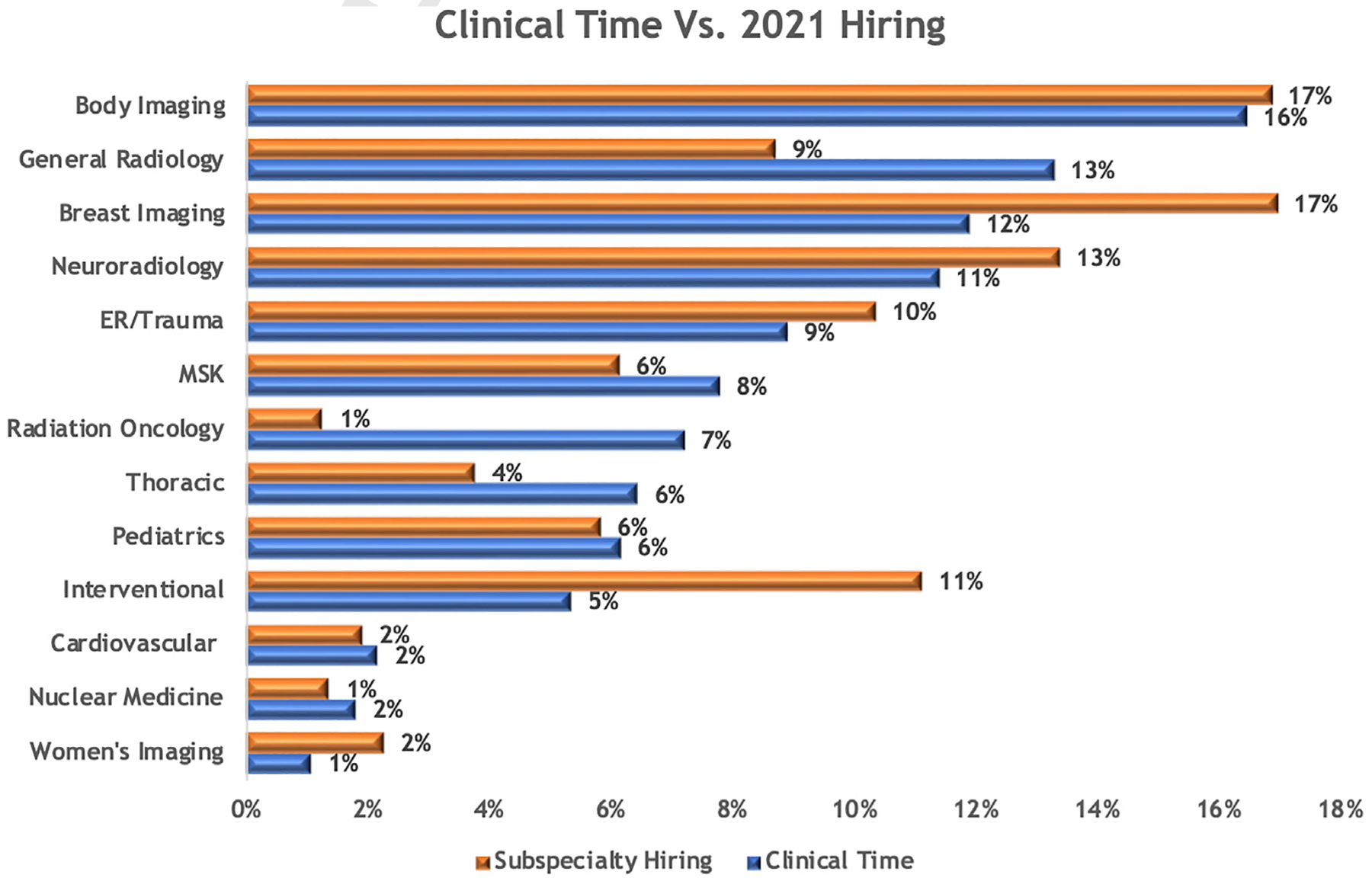
Clinical time versus 2021 hiring. ER = emergency room; MSK = musculoskeletal.
Table 1.
Subspecialty hiring needs in 2021 by practice type
| Academic | Private | National/MSO | Hospital/System | |
|---|---|---|---|---|
| Breast imaging | 15% | 42% | 57% | 39% |
| Body imaging (GI, GU, MRI, ultrasound) | 47% | 34% | 27% | 33% |
| Neuroradiology | 12% | 30% | 42% | 19% |
| Interventional | 28% | 29% | 26% | 23% |
| Musculoskeletal | 14% | 29% | 8% | 11% |
| General practice of radiology | 6% | 25% | 28% | 23% |
| We did not hire/do not anticipate hiring any physicians | 2% | 13% | 9% | 20% |
| Women’s imaging | 4% | 11% | 17% | 6% |
| Thoracic | 26% | 5% | 4% | 6% |
| Pediatrics | 24% | 5% | 13% | 9% |
| Emergency/trauma | 19% | 5% | 10% | 6% |
| Cardiovascular | 13% | 5% | 2% | 1% |
| Nuclear medicine | 9% | 3% | 10% | 7% |
| Radiation oncology | 12% | 2% | — | 9% |
Note: GI = gastrointestinal; GU = genitourinary; MSO = management services organization.
Hiring in 2021 Relative to Clinical Activity
Radiologists indicated that they spent 16% of their clinical time in body imaging. This is similar to the percentage of 2021 hires dedicated to body imaging. Interventional radiologist hiring in 2021 substantially exceeded the percentage of clinical time in this subspecialty. Breast imaging and women’s imaging hiring in 2021 also exceeded relative clinical time in the subspecialty (Fig. 2).
Hiring Plans for 2022
Hiring needs for 2022 are similar to 2021 hiring patterns (Fig. 3). Breast imaging is the most important hiring need for practices in 2022 (37% of practices), followed by body imaging (35%). Subspecialties in greater demand for 2022 than 2021 include cardiovascular radiology, emergency and trauma radiology, neuroradiology, and general practice of radiology. Private practices and national and MSO practices are more likely than academic practices to include breast imaging in their top three hiring needs and least likely to indicate that pediatrics is one of their top three 2022 hiring needs. Academic practices are least likely among all practice types to include general radiologists as one of their top hiring needs for 2022 but are more likely than any other practice type to seek emergency and trauma radiologists.
Fig. 3.

Anticipated hiring in 2022 by subspecialty. GI = gastrointestinal; GU = genitourinary.
Practice Type
Practice types have previously been defined by the ACR [11]. Private practice is the predominant radiology practice type, comprising more than one-third of radiologists and half of radiology practices (Figs. 4 and 5). Private practices employ more physicians than any other practice type and are the dominant practice type among small (<50 employees) and midsized (50–499 employees) practices (78% and 67%, respectively).
Fig. 4.
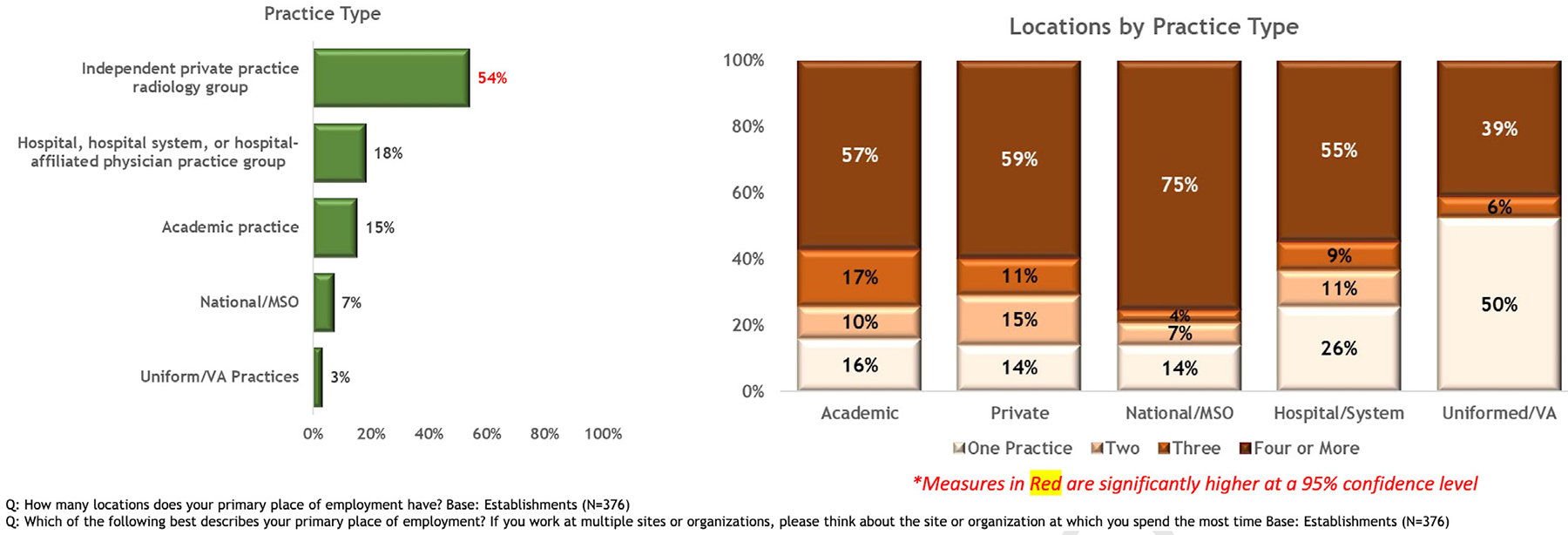
Practice type (left) and number of locations by practice type (right). Other practice types were <1% and are not included in the figure. MSO = management services organization; VA = US Department of Veterans Affairs.
Fig. 5.
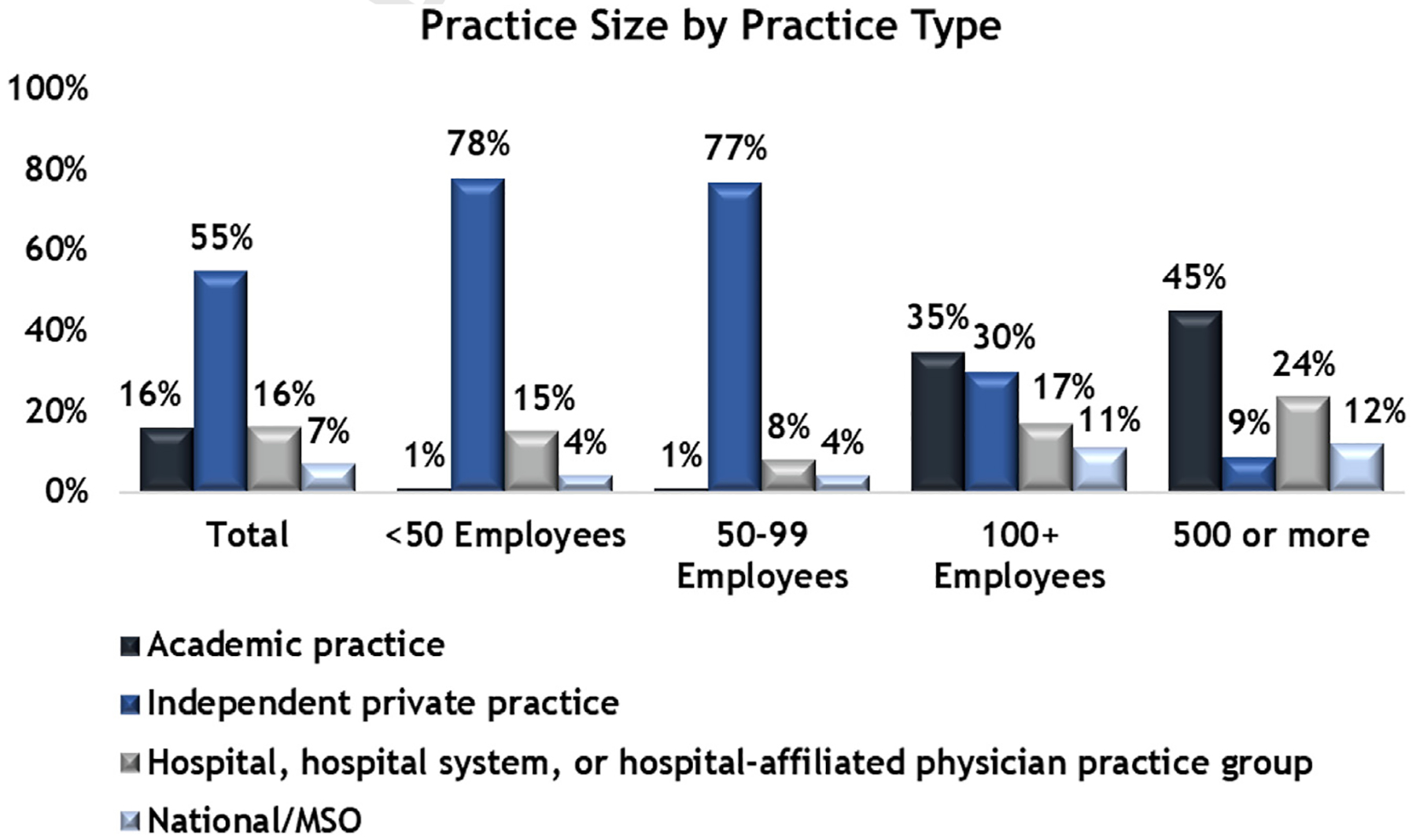
Practice size by practice type. Other practice types were <1% and are not included in the figure. MSO = management services organization.
Hospital-based practices represent 18% of the total practices, and academic practices represent 15% of practices (Fig. 4). Academic practices employ 28% of radiologists, and when including employees of all kinds (eg, not just radiologists), academic practices account for 45% of very large practices (500 employees or more), the largest percentage of employees in very large practices (Fig. 5). Thirty-nine percent of practices had <50 employees, 30% had 50 to 499 employees, 28% had 500 or more employees, and 3% of practices did not know.
A majority of radiology practices have four or more locations, and the number of physicians per practice varies among practice types. Practices with four or more locations are 3 times more numerous than practices with three or fewer locations. National practices are the most likely to have four or more locations (Fig. 4).
Telework
Respondents report that the majority of practices (82%) allow telework (defined in the survey as remote work) of some kind. Sixty-seven percent allow telework during the day; 63% allow telework at night. Many practices allow telework only during certain hours, as needed. Academic practices are more likely to allow daytime telework than private practices. Uniformed and VA practices are least likely to allow telework either during the day or at night (Fig. 6).
Fig. 6.
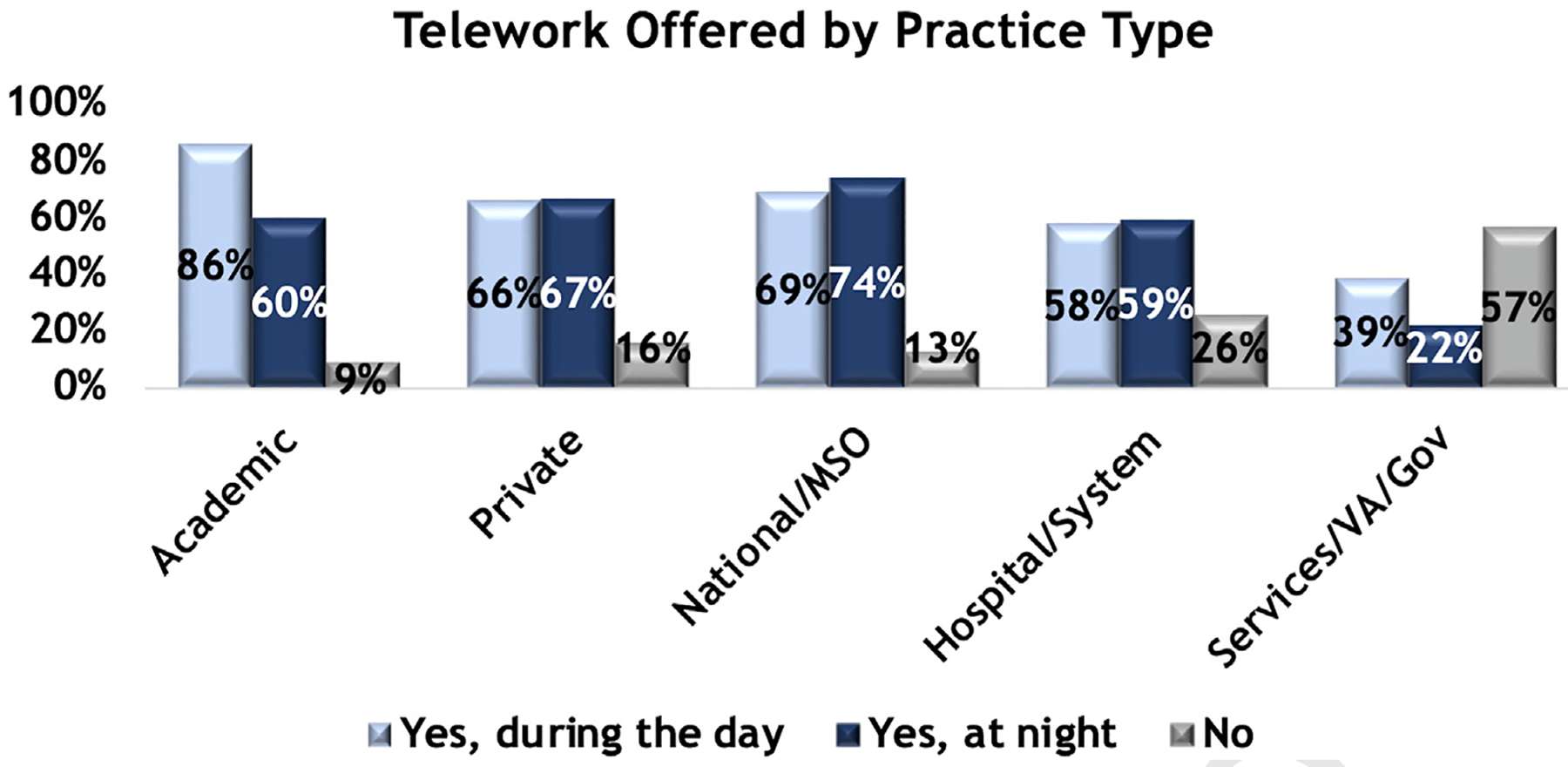
Whether telework is allowed, by practice type and time of day. Other practice types were <1% and are not included in the figure. Gov = government; MSO = management services organization; VA = US Department of Veterans Affairs.
Currently, 36% of radiologists report that they work remotely. Nearly half of radiologists would like to work remotely in the future (44%). The largest proportion of radiologists working remotely, 36%, are in academic practices. Fewer than 2 in every 10 radiologists in nonacademic settings telework currently.
Radiologist Retention
Sixteen percent of rank-and-file radiologists are highly likely to seek new employment in 2022. Ninety-two percent of early-career independent private practice radiologists hope to remain in the same practice setting in 5 years, the highest rate of any practice type. Academic radiologists are less likely to indicate that they will stay in the same practice type in 5 years (66%), followed by hospital and system radiologists at 57% and by radiologists in national and MSO practice settings, 43% of whom indicate that they will remain in the same practice setting in 5 years. Academic practices showed the greatest turnover in 2021, losing between one and two radiologists per practice in 2021.
Retirement
A large majority of practices reported no radiologist retirements in 2021 (80%). Forty-eight percent of retirees were from independent private practice, the largest percentage of retirees relative to other practice types. The average age of retirement among male radiologists was 75 years, while that of female radiologists was 71 years. Of those who retired in 2021, 66% worked full-time before retirement. Substantially more radiologists retired from national practice (two to three per practice in 2021) than in private practice or hospital-based practices (fewer than one each on average). Ninety-eight percent of retirees indicated that they would not return to active practice. Sixty-one percent of retirees, however, maintained active licensure after retirement. Forty-eight percent of retirements were from independent private practice. The smallest percentage of retirements were from uniformed and VA practices, representing 2% of retirements.
Hiring Resources
Nearly one-quarter of practices used third-party hiring support in 2021 (23%). Practices that used third-party hiring at the greatest rates are those with greater than 500 employees (27%) relative to practices with fewer than 50 employees. Eighteen percent of practices with fewer than 50 employees used third-party hiring support. Thirty-one percent and 30% of national and MSO and academic practices, respectively, used third-party hiring support. Overall, of hiring done by third-party firms, 15% was by independent private practices. Academic practices used third-party firms to hire practice leaders more frequently. With the exception of uniformed and VA practices, third-party hiring firms were used for fewer than 50% of hires in all other practice types. Academic practices used other resources (eg, job boards, association or radiology membership organization job postings) for 60% of their hires. Similarly, private practice used resources other than third-party firms for 68% of their hires. Uniformed and VA practices used general career sites and third-party firms for 50% of their hires each.
DISCUSSION
Surveying radiology professionals across the United States, we sought to clarify radiology practice types, specific subspecialty needs, employment trends, and retirement trends through results from the 2021 ACR HR Commission and RBMA Workforce Survey. Prior analysis of this survey’s methodology showed that the responses received were sufficient for analysis and provide an accurate understanding of the radiology workforce. Salient results include the following:
Most practices hired radiologists in 2021, and most had similar hiring plans for 2022.
Breast imaging is the most important hiring need for 2022, followed by body imaging.
Private practices account for half of radiology practices, and academic practices constitute the majority of very large practices.
A large majority of practices allow some form of telework, and a large majority of radiologists currently telework or would like to in the future.
Fewer than one in six radiologists are highly likely to seek new employment in 2022 with the greatest turnover in academic practices.
The average age of retirement for radiologists is 75 years, and most radiologists work full-time until retirement.
Independent private practices hired the largest proportion of radiologists in 2021 (as they did in the most recent prior survey in 2019), with similar expectations for hiring in 2022. Body and breast imagers represented the largest percentage of overall hiring in 2021, versus neuroradiology and body imaging in 2019 (breast imagers were the highest percentage of planned hiring in 2020 at the time of the 2019 survey) [10]. Of note, however, although the percentage of time spent by radiologists practicing body imaging matched 2021 hiring, breast imaging hiring outpaced clinical time spent in that subspecialty. The reason for this differential in breast imaging cannot be elucidated by this survey but could be related to the unique clinical skills and training required for breast imaging, resulting in a need to hire more radiologists capable of performing this type of imaging. Alternatively, practices may have exceeded hiring relative to clinical activity because of anticipated continuing increases in breast imaging that are expected over time. Interventional radiology hiring also outpaced clinical activity. Again, the reason for this pattern is not clear from this survey but may be related to the unique set of clinical expertise required, overnight call requirements, or a combination of both. Other subspecialties in which hiring substantially outpaced clinical activity included neuroradiology and emergency and trauma radiology.
Our study revealed that the majority of radiologists plan to stay in their current positions for the next 5 years. This was especially true at private practices compared with other practices. This may be related to the autonomy of private practice compared with other models [6]. In contrast, a previous study showed that between 2014 and 2018, there was job separation among approximately 40% of radiologists [3]. Radiologists may choose to leave a practice for multiple reasons, including retirement, changing jobs, termination, resignation, burnout, and transitioning to a different career [6,7,12–15]. The AMA estimates the total indirect and direct costs to replace a physician on the order of $1 million [16]. In the context of the current wide-open job market, radiology practice leaders can look at these data with some optimism in a challenging time of recruitment.
Independent private practices are smaller and more numerous and tend to have fewer locations than larger practice types. Academics and national practices tend to be larger practices and better resourced with regard to staffing and locations. Practices with staffing flexibility may be better able to compensate for both short- and long-term staffing difficulties, and these practices may be more attractive to new hires searching for job opportunities that provide better work-life balance than smaller practices do. Work-life balance is consistently one of the top three considerations for specialty selection among medical students and is also a top three consideration for subspecialty selection among radiology trainees [17]. A major contributor to burnout is loss of professional autonomy, including control of schedule, call responsibility, and work pattern [18]. The availability of part-time work, schedule flexibility, and ability to take family or medical leaves when needed are critical to attracting and retaining radiologist, promoting work-life balance, and reducing burnout.
Remote working opportunities (telework) are a highly desirable work setting. Telework has various definitions, with the common theme of working off-site from the location where images are acquired [19]. Technology updates have improved the transmission of images, enabling timely interpretation without negatively affecting workflow [20]. The coronavirus disease 2019 pandemic may have, by necessity, accelerated the implementation of technology in practices, allowing telework. Not only did more than one-third of radiologists work remotely in 2021, an even greater proportion would like to work remotely in the future. Academic practices and the large majority of radiology practices that allow telework both during the day and at night have the largest percentage of radiologists working remotely. Of note is that academic practices also share a larger proportion of women. By accommodating telework, it appears that this is a highly desirable work environment that may contribute to improved work-life balance in an increasingly diverse workforce.
Like all survey-based studies, our study had limitations that offer multiple opportunities for future research. We did not define practice type for respondents. Radiology appears to be undergoing an evolution with respect to the definition of practice type. The previously relatively distinct lines between these definitions have blurred with consolidation of practices and practice types; for example, some national practices are run locally, national practices and MSO practices are not a homogenous group, and some practices with residents but no medical school affiliation may fall under multiple practice type definitions. Similarly, the concept of teleradiology has evolved from one in which large independent contractors previously provided services to groups, typically during overnight shifts, to one that is often offered within radiology groups and used during daytime, evening, and overnight shifts. The distinction has blurred over time, and respondents may have defined telework in a variety of ways. For example, specific questions regarding intramural versus extramural teleradiology work [20] were not asked but would be of interest for future studies. Finally, although economies of scale may be available at large practices of more than 500 radiologists, there may be differences in the function and opportunities in these practices. Further work is needed to fully understand this important subsegment of our workforce and practice setting. To address these limitations and others that may arise, the Workforce Survey will undergo annual refinement with input from the ACR HR Commission, ACR environmental intelligence, the RBMA, and the third-party market research firm. We plan to report on survey changes and results annually.
Supplementary Material
TAKE-HOME POINTS.
Most practices hired radiologists in 2021 and had similar hiring plans for 2022, with breast imaging as the most important area, followed by body imaging.
A large majority of practices allow some telework, and a large majority of radiologists currently telework or would like to in the future.
Fewer than one in six radiologists are highly likely to seek new employment in 2022, with the greatest turnover at academic practices.
The average age of retirement for radiologists is 75 years, and most radiologists work full-time until retirement.
ACKNOWLEDGMENTS
The authors acknowledge members of the ACR HR Commission for assistance with survey development, Dominick Parris from ACR environmental intelligence, and Mitch Sanders and Jon Siegel from Meliora Research for assistance with survey development, data collection, and data analysis.
This work was supported in part by the ACR. Dr Duszak declares Unpaid service as a Chancellor, American College of Radiology; Dr Parikh declares this work was supported in part by the NIH/NCI Cancer Center Support Grant (award number P30 CA016672). Dr Duszak is a medical adviser and shareholder of Ethos Medical. All other authors state that they have no conflict of interest related to the material discussed in this article. Drs Dibble and Rubin are partners. Dr Parikh, Dr Duszak, Mr Parris, and Ms Tarrant are non-partner/non-partnership track/employees.
Footnotes
ADDITIONAL RESOURCES
Additional resources can be found online at: https://doi.org/10.1016/j.jacr.2023.02.041.
REFERENCES
- 1.Association of American Medical Colleges. The complexities of physician supply and demand: projections from 2019 to 2034. Available at: https://www.aamc.org/media/54681/download. Accessed September 29, 2022.
- 2.Smith-Bindman R, Kwan ML, Marlow EC, et al. Trends in use of medical imaging in US health care systems and in Ontario, Canada, 2000–2016. JAMA 2019;322:843–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Santavicca S, Hughes DR, Fleishon HB, et al. Radiologist-practice separation: recent trends and characteristics. J Am Coll Radiol 2021;18:580–9. [DOI] [PubMed] [Google Scholar]
- 4.Parikh JR, Bender CE. How radiology leaders can address burnout. J Am Coll Radiol 2021;18:679–84. [DOI] [PubMed] [Google Scholar]
- 5.Giess CS, Ip IK, Cochon LR, et al. Predictors of self-reported burnout among radiology faculty at a large academic medical center. J Am Coll Radiol 2020;17:1684–91. [DOI] [PubMed] [Google Scholar]
- 6.Sinsky CA, Brown RL, Stillman MJ, Linzer M. COVID-related stress and work intentions in a sample of US health care workers. Mayo Clin Proc Innov Qual Outcomes 2021;5:1165–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Harolds JA, Parikh JR, Bluth EI, Dutton SC, Recht MP. Burnout of radiologists: frequency, risk factors, and remedies: a report of the ACR Commission on Human Resources. J Am Coll Radiol 2016;13: 411–6. [DOI] [PubMed] [Google Scholar]
- 8.Farmakis SG, Chertoff JD, Barth RA. Pediatric radiologist workforce shortage: action steps to resolve. J Am Coll Radiol 2021;18: 1675–7. [DOI] [PubMed] [Google Scholar]
- 9.Bluth EI, Short BW, Willis-Walton S. 2012 ACR Commission on Human Resources Workforce Survey. J Am Coll Radiol 2012;9: 625–9. [DOI] [PubMed] [Google Scholar]
- 10.Bender CE, Bansal S, Wolfman D, Parikh JR. 2019 ACR Commission on Human Resources Workforce Survey. J Am Coll Radiol 2020;17: 673–5. [DOI] [PubMed] [Google Scholar]
- 11.Berland LL, Tarrant MJ, Heitkamp DE, Beavers KM, Lewis MC. Maintenance of certification in radiology: eliciting radiologist preferences using a discrete choice experiment. J Am Coll Radiol 2022;19: 1052–68. [DOI] [PubMed] [Google Scholar]
- 12.Bluth EI, Cox J, Bansal S, Green D. The 2015 ACR Commission on Human Resources Workforce Survey. J Am Coll Radiol 2015;12: 1137–41. [DOI] [PubMed] [Google Scholar]
- 13.Parikh JR, Rapoport RJ, Bluth EI, Fleishon HB, Donner EM III. Midcareer transition in radiology: threat or opportunity? J Am Coll Radiol 2015;12:624–9. [DOI] [PubMed] [Google Scholar]
- 14.Parikh JR, Bluth EI. Career alternatives for radiologists beyond clinical practice. J Am Coll Radiol 2016;13:738–42. [DOI] [PubMed] [Google Scholar]
- 15.Donner EM III, Sze G, Bluth EI. Retirement issues for radiologists: consensus statement on successful planning by the Commission on Human Resources of the ACR. J Am Coll Radiol 2015;12:235–8. [DOI] [PubMed] [Google Scholar]
- 16.Berg S. How much physician burnout is costing your organization. Available at: https://www.ama-assn.org/practice-management/economics/how-much-physician-burnout-costing-your-organization. Accessed September 29, 2022.
- 17.Yen AJ, Webb EM, Jordan EJ, Kallianos K, Naeger DM. The stability of factors influencing the choice of medical specialty among medical students and postgraduate radiology trainees. J Am Coll Radiol 2018;15:886–91. [DOI] [PubMed] [Google Scholar]
- 18.Chetlen AL, Chan TL, Ballard DH, et al. Addressing burnout in radiologists. Acad Radiol 2019;26:526–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hanna TN, Steenburg SD, Rosenkrantz AB, Pyatt RS Jr, Duszak R Jr, Friedberg EB. Emerging challenges and opportunities in the evolution of teleradiology. AJR Am J Roentgenol 2020;215:1411–6. [DOI] [PubMed] [Google Scholar]
- 20.Chung H, Parikh J. Telemammography: technical advances improve patient access in breast care. J Breast Imaging 2020;2:152–6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.