

Abstract
Aim:
The objective of this document is to provide guidance to the infertility specialist, gynecologist, embryologist, and counselors on the management of sub-fertility and brief them with the recent advances in the field. These recommendations will aid the aforementioned healthcare professionals in everyday clinical decisions about appropriate and effective care of their patients with the best available evidence.
Participants:
Extensive deliberations, discussion, and brainstorming was done between different reproductive medicine (RM) specialists, to develop the recommendations.
Evidence:
A systematic review of the literature published up to June 2019 was carried out using PubMed and Cochrane Collaboration Library. International guidelines, cohort studies, case series, observational studies, and randomized controlled trials currently available in the literature were reviewed. Indian data whatever available was also reviewed.
Process:
Primary meetings were held with leading reproductive medicine specialists. Each topic was brainstormed on by a group of reproductive medicine experts, who then prepared the first draft of the recommendation. These recommendations then were reviewed by Dr. Jaideep Malhotra, Dr. Gouri Devi, and Dr. Madhuri Patil along with the chief co-ordinator of each consensus to finalize the final draft.
Conclusions:
From the literature and discussion of the available evidence, several topics were identified for which evidence is inconsistent, insufficient, or non-existing. For the benefit of couples undergoing several treatments, the working committee recommends that future research, where possible in well–designed RCTs, will help in establishing evidence for a particular practice. In the Indian context, one also needs to take into consideration facilities and options available, cost, lack of insurance coverage, experimental nature of some advanced techniques used.
Keywords: Infertility, IVF, ICSI, investigations, ultrasound, genetics, unexplained infertility, poor responders, endocrinopathies, ovulatory disorders, polycystic ovary syndrome, IUI, IVF, ICSI, recurrent implantation failure, fertility preservation, third party reproduction, safety, ethical issues
Chapter 1: Investigating a Sub-fertile couple
OVERVIEW
Infertility can be caused by a number of underlying conditions including ovulatory disorders, tubal damage, male factors, and uterine or peritoneal problems. Before treatment is started, it is important that a clinical assessment, namely history taking and physical examination, is undertaken. In most cases, further diagnostic investigations are also undertaken to establish if a pathological condition is present. This guideline offers recommendations on the investigations for sub–fertile couples. The investigations are detailed for the couple together, as well as for the male and female partners individually.
1. Introduction
Begin infertility investigations if a woman of reproductive age has failed to conceive after 12 months of regular (2–3 times per week) unprotected vaginal sexual intercourse, in the absence of any known cause of infertility
The number and quality of oocytes are shown to decline with a woman’s age. Besides, there is clear evidence that overall fertility declines with age, which is in part related to a decline in ovarian reserve, but also a lower rate of embryo implantation and an increased chance of pregnancy loss. It has been established that the fecundity of women decreases gradually, but significantly beginning approximately at age 32 years and decreases more rapidly after 37 years
Because of the decline in fertility and increased time to conception related to advanced age, several international societies have recommended that women >35 years should receive expedited evaluation and treatment after 6 months of failed attempts to conceive, or earlier if clinically indicated
Several studies published during last few years have reported faster ovarian ageing in Indian women with 5–6 years difference in age of menopause, and corresponding earlier decline in fertility, when compared with their counterparts in western countries
-
Ethnic differences are reported to exist with ovarian ageing, as shown in a study by Iglesias C et al 2014. It was observed that similar ovarian reserve markers and ovarian response existed in women with a 6–year age difference in favor of the Spanish
-
»In a Pan–India survey conducted by the Menopause Society of India, average age of menopause in Indian women was reported as 46.2+4.9 years compared to 51 years in their western counterparts
-
»
A cut–off age of 32 years should be taken as risk factor for diminished ovarian reserve and fertility for Indian women as discussed in detail and agreed with consensus
-
Follow specific factors that may mandate earlier investigations (after 6 months of failed attempts to conceive or earlier if clinically indicated) in Indian women:
-
»If woman is aged ≥ 32 years
-
»A known cause of infertility or a history of predisposing factors for infertility exists
-
»
The term primary infertility is used when a woman has never conceived, and secondary infertility is the incapability to conceive in a couple who have had at least one successful conception in the past. Globally, most infertile couples suffer from primary infertility
-
Infertility affects up to 15% of the couples of reproductive age worldwide
-
»According to the World Health Organization estimate, the overall prevalence of primary infertility in India is between 3.9% to 16.8%
-
»In Indian states prevalence of infertility varies from state to state such as 3.7% in Uttar Pradesh, Himachal Pradesh, and Maharashtra, to 5% in Andhra Pradesh, and 15% in Kashmir, and prevalence varies in same region across tribes and caste
-
»
A detailed medical history of both partners and physical examination of female partner are mandatory and helpful to decide the extent of investigations necessary in individual infertile couple
Provide all infertile couples with pre–pregnancy counseling and offer general investigations to assess general health and detect medical and heritable genetic disorders having potentials to impact mother and/or child’s health
Focus basic standard investigations for the infertile couple on the major causes of infertility such as semen abnormalities, ovulation dysfunction, and fallopian tube obstruction/impaired function. Also, include the appropriate ovarian reserve tests under standard/basic infertility evaluation for women aged >32 years or those <32 years with risk factors for early/expedited oocyte depletion.
Counsel the infertile couple that only some of the causes of infertility are known, and after a conventional diagnostic assessment, in approximately 30% (reported range 15%-40%) of couples, subfertility remains unexplained. Further, even the most sophisticated array of diagnostic tests cannot reveal the defect causing infertility in many patients, with these causes remaining undiscovered at this time
Counsel the infertile couple that even subnormal tests/investigation reports may not always mean absolute infertility and some couples will achieve pregnancy even without treatment
2. Standard investigations for sub-fertile couples
General investigations for both partners
-
Investigations for female partner
-
»Assessment of ovulation
-
»Ovarian reserve tests
-
»Tubal and uterine assessment
-
»
Investigations for male partner
2.1 General investigations for both partners
The tests of general investigations are categorized under following headings:
Tests to assess general health and exclude common medical disorders having impact on mother or child during pregnancy
General investigations in male partner
Tests to exclude existing or significant risk of contacting common infections with serious risk of vertical transmission
Indications for genetic evaluation in subfertile couple
To assess fitness in advanced age women
Investigations in women with complex medical disorders
2.1.1 Tests to assess general health and exclude common medical disorders having impact on mother or child during pregnancy
2.1.1.1 Anemia
2.1.1.2 Urine analysis
2.1.1.3 Blood group and Rhesus typing
2.1.1.4 Impaired glucose tolerance and diabetes mellitus (DM)
-
WHO criteria 2 hour 75 gm OGTT
-
»Impaired glucose tolerance (IGT): 140–199 mg/dl
-
»DM ≥200 mg/dl
-
»
-
American Diabetic Association (ADA) criteria fasting glucose level
-
»Impaired fasting glucose (IFG) 100-125 mg/dl
-
»DM ≥126 mg/dl
-
»HbA1c measures the efficacy of glucose lowering treatment. A normal HbA1c cannot exclude DM or IGT
-
»
2.1.1.5 Thyroid dysfunction
There is reasonable evidence that overt hypothyroidism may be associated with infertility and pregnancy complications. Universal screening rather than a targeted screening is recommended in subfertile Indian women considering high incidence of thyroid disorders in India
Further evaluate women with subclinical hypothyroidism [serum thyroid stimulating hormone (TSH) between 2.5 and 10 mIU/L with normal FT4 concentration] detected during preconception by anti-thyroid peroxidase antibodies to decide regarding the need for treatment
2.1.1.6 Cervical cancer screening
2.1.1.7 Rubella immune status
2.1.1.8 Thalassemia and other hemoglobinopathies
Majority of β-thalassemia carriers will have an mean corpuscular volume (MCV) of <80 fl and mean corpuscular hemoglobin (MCH) of <27 pg with relatively high red blood cell (RBC) counts for the level of Hb and these indices can be used for initial screening. HbA2 levels of >4.0% along with reduced RBC indices are indicative of β-thalassemia carriers. Borderline HbA2 levels (3.3%–3.9%) must be interpreted with caution and may need confirmation by DNA methods. Atypical β-thalassemia carriers may have a normal MCV and/or MCH sometimes, and these individuals may be missed on screening using RBC indices. Carriers of variant HbS like Hb E and Hb S may also have normal indices in 20%–30% of cases. In cases with microcytosis, iron deficiency anemia, and anemia of chronic disease should be ruled out and specific investigations for thalassemia and other hemoglobinopathies considered
2.2 General investigations in male partner
Blood Hb estimation
Urine analysis
Blood group and Rhesus typing
Screening for blood sugars and / or HbA1c
Thyroid hormones
2.2.1 Tests to exclude existing or significant risk of contracting common infections with serious risk of vertical transmission
Offer universal preconception screening for HIV, syphilis, hepatitis B, and hepatitis C for both partners
In serodiscordant couples, additional tests would be required after a specialist consultation to assess the disease status and transmission risk. Additional or alternate procedures, counselling and decisions would be required to treat these couples
Routine TORCH (Toxoplasmosis, Rubella, Cytomegalovirus, and Herpes simplex) panel should not be done except to check for Rubella immune status
2.3 Indications for Genetic evaluation in sub-fertile couple
Offer peripheral blood Karyotype and Y chromosome microdeletion testing to infertile male patients diagnosed to have non-obstructive azoospermia or severe oligozoospermia (sperm density ≤10 million/ml)
Offer genetic counselling and testing to men with congenital absence of unilateral or bilateral vas deference, since they need cystic fibrosis transmembrane receptor gene (CFTR) screening
The patients with hypogonadotropic hypogonadism may need genetic tests and conselling according to clinical features
Investigate primary amenorrhea by karyotype analysis and selected mutation screening according to the patient’s clinical features
Consider karyotype analysis and FMRI gene screening in cases of Premature Ovarian Failure (POF)
Indicate detailed genetic testing and counselling in cases of consanguineous marriages, advanced age (either partner), family history of genetic diseases, mental retardation, genital malformations, previous affected baby, recurrent miscarriages, and recurrent implantation failures. Peripheral blood Karyotype is minimum basic investigation
Next generation sequencing (NGS) screening is a preferred method testing
Carrier screening based on prevalence of common genetic diseases after proper genetic counseling should be offered
All genetic analysis should be accompanied by expert counseling by a clinical geneticist both in male and female patients
2.4 Additional tests that may be required in women older than 35 years
Oocyte and embryo donation are accepted treatments of age related fertility decline. Pregnancies in advanced age are complicated by increased risks of maternal and perinatal morbidity and mortality. Common causes are diabetes, hypertensive disorders, and cardiac and thromboembolic events. It is mandatory for the care takers to evaluate these women completely to exclude or control any pre–existing medical disease
2.4.1 Recommended tests
Oral glucose tolerance test
Lipid profile
Liver function tests
Renal function tests
Electrocardiogram
X–ray chest
Echocardiography in post-menopausal women
USG/ mammogram
Whole abdomen ultrasound for abdominal organs
2.5 Investigations in women with specific medical disorders needing complete evaluation are:-
Turner’s syndrome
Cardiomyopathy
Treated malignancies
Hereditary thrombophilias with h/o thromboembolism
Bleeding disorders
Severe respiratory insufficiency
Ischemic heart disease
Renal transplant or chronic renal failure
Portal hypertension
2.6 General investigations for female partner
2.6.1 Assessment of ovulation
Although regular menstruation is strongly suggestive of ovulation, it should be confirmed by mid luteal progesterone (MLP)
Progesterone on day 21 in 28 day cycle/ progesterone every 7 days after day 21 in patients with irregular menstrual cycles till until the next menstruation
Values of ≥3 ng/ml are suggestive of ovulation and values of ≥10 ng/ml are suggestive of normal progesterone production
Urinary LH Kit
Ultrasound guided follicular monitoring
2.6.2 WHO classification of ovulation disorders
The WHO classifies ovulation disorders into three groups (Table 1)
The table below shows the diagnostic hormonal levels in anovulatory infertility
Table 1.
WHO classification of ovulatory disorders
| Group I: Hypothalamic/ pituitary failure | Kallmann’s syndrome hypogonadotrophic hypogonadism | 5% |
| Hypothalamic causes (hypogonadotropic hypogonadism) | Weight loss Exercise Chronic illness Psychological distress Idiopathic | |
| Causes of hypothalamic/ pituitary damage | Tumours (e.g. cranio-pharyngiomas) Cranial irradiation Head injuries Sarcoidosis Tuberculosis | |
| Systemic causes | Chronic debilitating illness Weight loss | |
| Endocrine disorders | Thyroid, Cushing’s syndrome | |
| Hyperprolactinemia Hypopituitarism | ||
| Group II: H/P dysfunction | Polycystic ovary syndrome | 90% |
| Group III: Ovarian failure | Premature ovarian failure (POF) Resistant ovary syndrome (ROS) | 5% |
Table 2.
Diagnostic Hormonal levels in anovulatory Infertility
| Hypothalamic: underweight | ↓FSH, ↓ LH, ↓E2 n FSH, ↓ LH, ↓ E2 |
| Hyperprolactinaemia | ↓ FSH, ↓ LH, ↓ E2 |
| Ovarian failure / menopause: | ↑↑ FSH, ↑ LH, ↓E2 |
| Mid-cycle | ↑ FSH, ↑↑ LH, ↑ E2 |
| PCOS | ↓/n FSH, ↑/n LH, ↑/n E2 |
FSH: follicle-stimulating hormone; LH: luteinizing hormone; E2: estradiol; PCOS: polycystic ovary syndrome.
2.6.3 Ovarian reserve tests
-
Ovarian reserve test are used to
-
»Improve efficacy, safety and cost effectiveness of treatment
-
»
Predict response to tailor correct stimulation regimen for adequate response so as to prevent complications and improve pregnancy outcomes
Response to the first cycle of controlled ovarian stimulation (COS) is the most important predictor of ovarian response
Ovarian reserve testing help for a strategic approach to ovarian stimulation (Table 3)
The figure 1 gives the different ovarian test that can be utilized to assess the ovarian reserve. The choice of the test will depend on local provision, such as laboratory resources and availability of a skilled ultrasonologist
Table 3.
Use of ovarian reserve test for strategic approach to ovarian stimulation in hyper and poor responders
| Anticipated excessive ovarian response, clinicians can provide guidance on the | Predicted poor ovarian response, clinicians may decide to counsel patients not to proceed with treatment |
|---|---|
| • AMH >3.5 ng/mL- high risk of OHSS, regardless of age | • Alter their treatment protocol |
| • Potential risks of OHSS and multiple pregnancy associated with treatment | • Exogenous agents • Not feasible to deny treatment based on low (1.0 ng/mL) AMH level |
| • Advise on low dose gonadotropin antagonist protocols | • Combination of low AMH levels & POR in the first IVF cycle suggest unfavourable prognosis and one must avoid further IVF |
| • GnRHa trigger • Stringent monitoring during treatment |
• Suggest egg donation at an early stage in their management |
AMH: anti-Müllerian hormone; OHSS: ovarian hyperstimulation syndrome; IVF: in-vitro fertilization; GnRHa: gonadotropin-releasing hormone agonist; POR: poor ovarian response.
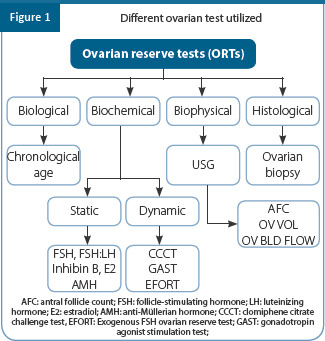
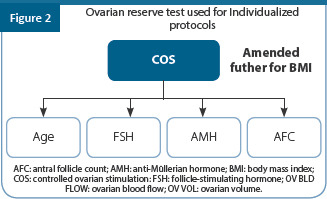
Of these test only age, AMH, AFC, and FSH are used to select the correct stimulation protocol. The dose of gonadotropin used depending on these ovarian reserve test is further amended for BMI (Figure 2)
2.6.3.1 Limitations of ovarian reserve tests (Table 4)
Table 4.
Limitations of the ovarian reserve tests used
| Ovarian reserve tests (ORTs) | Limitations |
|---|---|
| FSH | • Does not diagnose poor ovarian reserve until high thresholds reached |
| • Does not explain oocyte quality decline | |
| • Inter-cycle and inter-sample variations may result in a disparity in FSH measurements | |
| • Role limited in the evaluation of young healthy Women • Elevated day 3 FSH - heterogeneous group | |
| » true reduced ovarian reserve » due to the presence of heterophile antibodies | |
| » FSH receptor polymorphism in patients with otherwise normal ovaries | |
| Estradiol | • Prediction of ovarian reserve is still debatable |
| • No relationship has been found between serum E2 levels and pregnancy rates | |
| • Very low predictive accuracy, both for the poor response or excessive response | |
| Inhibin B | • Better predictor for cancellation than the ovarian response • It is influenced by the amount of fat in an individual with levels lower in obese women |
| AMH | • AMH concentrations able to predict the number of oocytes collected after ovarian stimulation |
| • No role in predicting oocyte quality or LBR | |
| • Expensive | |
| • Lack of standardization of AMH assay | |
| • Variable AMH measurements made by the different AMH assays, even when using the same clinical sample | |
| • Women with higher basal AMH concentration experience greater variation in AMH values over time | |
| AFC | • Access to quantity but not quality |
| • Inter/Intra-observer differences – may be reduced by 3D USG | |
| • Losing track of measured or not yet ---- One or two adjacent follicles | |
| • Inter-cycle variability | |
| • Poor predictive value for pregnancy | |
| Ovarian Volume | • Wide range in the definition of normal ovarian volume in the reproductive age group • Predictive value for pregnancy limited (1.0–1.4) • Has high false-positive test therefore not suitable as a routine test for ovarian reserve assessment |
| Dynamic test | • More expensive and invasive, time-consuming |
| • Done only in the research setting | |
| Ovarian Biopsy | • Invasive |
| • Follicular density varies | |
| • Long-term consequences |
2.6.3.2 Key points
AMH an excellent marker of ovarian response and can predict extremes of response as compared to FSH, but a weak predictor of clinical pregnancy
High accuracy for AMH and AFC in predicting poor response but only moderate accuracy for FSH
Significant negative interaction between age and AMH
AMH and age independent determinants of oocyte yield
Accuracy of AMH, AFC, and FSH in predicting zero prognosis cases is poor and can be possible only at extreme cut-off levels
All three Ovarian reserve tests (ORTs) have only a very small or no predictive effect on pregnancy rates
2.6.4 Tubal and uterine assessment
2.6.4.1 Tubal factors
Tubal factor infertility accounts for 25%–35%. The most common cause of tubal factor infertility is infection pelvic inflammatory diseases (PID)
Sexually transmitted infections (STIs) are the leading preventable cause of infertility by causing 70% of PID responsible for tubal damage
Other causes are endometriosis, previous surgery for ruptured appendix or other abdominal surgeries including surgery for ectopic pregnancies
-
The tests used to diagnose tubal factor infertility are hysterosalpingography, sonosalpingography, hysterosalphingo contrast sonography, and laparoscopy
-
»Hysterosalpingography (HSG)
-
»Sonosalpingography (SSG)
-
»Hysterosalpingo contrast sonography (HyCoSy) is same as SSG, the only difference is instead of normal saline, a radiocontrast dye is instilled inside the uterine cavity.
-
»Laparoscopy
-
»
2.6.4.2 Uterine factors
Ultrasonography (2D & 3D)
Hysterosalpingography has a sensitivity of between 50% for intracavitary lesions and it is unable to reliably distinguish between submucosal myomas and endometrial polyps. HSG has low sensitivity (50%) and a positive predictive value of 30%. It cannot differentiate between septate and bicornuate uterus hence MRI or 3D USG is necessary
Saline Infusion sonography and HSG have similar diagnostic accuracies (52% vs. 60%). It has a high positive predictive value (90%) for detecting intrauterine pathology. It does not involve radiation
Hysteroscopy
MRI
2.7 Investigations for male partner
2.7.1 Investigations
2.7.1.1 Semen analysis
Table 5.
WHO lower reference limits* for semen characteristics
| Criteria | Lowe reference value |
|---|---|
| Serum morphology (normal forms, %) | 1.5 (1.4–1.7) |
| Total sperm number (106 per ejaculate) | 39 (33–46) |
| Sperm concentration (106 per ml) | 15 (12–16) |
| Total motility(PR + NP, %) | 40 (38–42) |
| Progressive motility(PR, %) | 32 (31–34) |
| Vitality (live spermatozoa, %) | 58 (55–63) |
| Sperm morphology (normal forms, %) | 4 (3.0–4.0) |
| Other consensus threshold values | |
| ph | ≥ 7.2 |
| Peroxidase-positive leukocytes (106 per ml) | < 10 |
| MAR test (motile spermatozoa with bound beads, %) | < 50 |
| Immunobead test (motile spermatozoa with bound beads, %) | < 50 |
| Seminal zinc | ≥ 2.4 |
| Seminal fructose (micromole/ejaculate) | ≥ 13 |
| Seminal neutral glucosidase (milli units ejaculate) | ≥ 20 |
*5th centiles and their 95% confidence intervals, who: world health organization, 2010
2.7.1.2 Microscopic examination
-
Initial microscopic examination
-
»This provides an overview of the sample, to reveal:
- - Mucus strand formation.
- - Sperm aggregation or agglutination (the presence of agglutination is not sufficient evidence to deduce an immunological cause of infertility, but is suggestive of the presence of anti-sperm antibodies; further testing is required. Severe agglutination can affect the assessment of sperm motility and concentration)
- - The presence of cells other than spermatozoa, such as epithelial cells, “round cells” (leukocytes and immature germ cells) and isolated sperm heads or tails
-
»
-
Detailed microscopic examination
-
»Sperm motility
-
- Grade the motility of each spermatozoon as follows:
- # Progressive motility (PR): Spermatozoa moving actively, either linearly or in a large circle, regardless of speed
- # Non-progressive motility (NP): All other patterns of motility with an absence of progression, such as swimming in small circles, the flagellar force hardly displacing the head, or when only a flagellar beat can be observed
- # Immotility (IM): No movement
-
-
»Sperm vitality
- - The presence of a large proportion of vital but immotile cells may be indicative of structural defects in the flagellum; a high percentage of immotile and non-viable cells (necrozoospermia) may indicate epididymal pathology
-
»Sperm Numbers
- - It is recommended to calculate and report the total number of spermatozoa per ejaculate, as this parameter provides a measure of the capability of the testes to produce spermatozoa and the patency of the male tract.
-
»Sperm morphology
- - Strict Kruger’s criteria are used to evaluate the morphology
- - Coiled tails (>360°) may indicate epididymal dysfunction
- - Abnormal spermatozoa generally have a lower fertilizing potential, depending on the types of anomalies, and may also have abnormal DNA
- - Morphological defects have been associated with increased DNA fragmentation, an increased incidence of structural chromosomal aberrations, immature chromatin, and aneuploidy
-
»Presence of leucocytes/peroxidase positive cells
- - Excessive numbers of leukocytes in the ejaculate (leukocytospermia, pyospermia) may be associated with infection and poor sperm quality
-
»Assessment of immature germ cells in semen
- - Germ cells include round spermatids and spermatocytes, but rarely spermatogonia. They can be detected in stained semen smears, but may be difficult to distinguish from inflammatory cells when the cells are degenerating
-
»Testing for antibody coating of spermatozoa
- - The diagnosis of immunological infertility is made when 50% or more of the motile spermatozoa (progressive and non-progressive) have adherent particles. Particle binding restricted to the tail tip is not associated with impaired fertility and can be present in fertile men
-
»
2.7.1.3 Biochemical tests on seminal plasma
-
Seminal fructose
-
»The lower reference limit for fructose is 13 mol per ejaculate
-
»Low fructose in semen is characteristic of ejaculatory duct obstruction, bilateral congenital absence of the vas deferens, partial retrograde ejaculation, and androgen deficiency
-
»Other biochemical tests such as zinc, alpha- glucosidase are optional and not of much clinical significance
-
»
2.7.1.4 Computer aided sperm analysis (CASA)
-
CASA, including assessment of motility, concentration and morphology, has two advantages over manual methods:
-
»Has high precision
-
»Provides quantitative data on the kinematic parameters of spermatozoa (forward progression and hyperactivated motility, characteristic of capacitated cells)
-
»
The use of fluorescent DNA stains with CASA allows the concentration of motile sperm and percentage motility to be determined accurately, but scrupulous adherence to technique is required
The CASA instrument detects and counts fluorescent sperm heads. Without microscopic evaluation, there is no way of knowing if the spermatozoa are intact (the head is attached to a tail)
Semen analysis will provide the direction for further evaluation and treatment. If semen analysis is abnormal we need to evaluate further (Table 6)
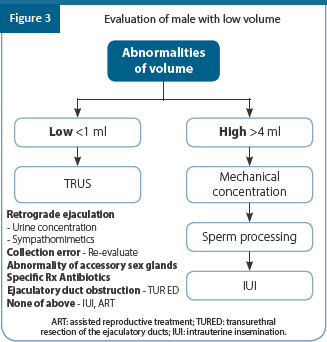
In presence of low volume, the male partner is evaluated as follows (Figure 3)
Table 6.
Investigations for male partner
| Medical and Sexual history | • Coital frequency and timing |
| • Duration of infertility and prior fertility | |
| • Childhood illnesses and developmental history | |
| • Systemic medical illnesses | |
| • Prior surgeries | |
| • Sexual history including sexually transmitted diseases | |
| • Gonadal toxin exposure including heat | |
| Physical Examination | • Secondary sexual characters |
| Recommended in cases of : | • Examination of penis |
| Abnormal Male history | • Palpation of testis and measurement of size |
| Abnormal semen analysis | • Presence and consistency of vas and epididymis |
| Unexplained Infertility | • Evaluation for varicocele |
| Treated female factor with persistent infertility | • Digital rectal examination |
| Ultrasound | For determination of |
| • Size of testis | |
| • Varicocele | |
| • Hydrocele | |
| • Epididymal cyst | |
| • Spermatocele | |
| • Epididymitis | |
| • Orchitis | |
| • Testicular torsion | |
| • Cryptorchidism | |
| Endocrine Evaluation Initially recommended in cases of Low sperm count especially if less 10 mill/ml Impaired sexual function Clinical findings suggestive of a endocrinopathy |
Minimal: |
| • FSH | |
| • Testosterone | |
| Additional in cases of low testosterone: | |
| • Repeat testosterone | |
| • SHBG | |
| • Prolactin | |
| • LH | |
| No role for evaluating AMH and Inhibin B | |
| Karyotyping | Klinefelters syndrome XXY and variants |
| Translocations | |
| Balanced | |
| Unbalanced | |
| Molecular genetics | • Y-chromosome microdeletion • Cystic Fibrosis Gene mutations |
| Sperm function test Diagnose some subtle changes and help clinically to direct therapy |
• Trial Wash |
| • HOS | |
| • TZI | |
| • CASA | |
| • DFI | |
| • Acrosome reaction | |
| • Mucus Penetration test | |
| • Estimation of ROS | |
| Not regularly performed prior to ART treatment because they are | |
| • complex • expensive | |
| • not rigorously tested | |
| • do not always provide clinically useful information • typically do not affect treatment • cannot be performed with good repeatability and reliability and at minimal cost | |
| Testicular Biopsy | Diagnostic / therapeutic testicular biopsy for ultimate |
| differentiation between obstructive and non-obstructive azoospermia | |
| Should be done only when facilities for cryopreservation are available | |
| Post ejaculation urine examination | To differentiate between retrograde ejaculation and an ejaculation |
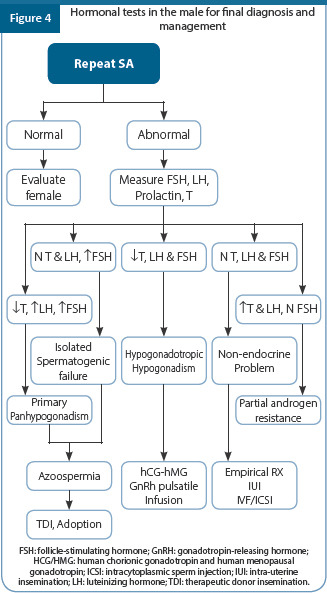
2.7.1.5 Diagnosis based on hormonal tests
In case of an abnormal semen analysis the diagnosis can be achieved by performing hormonal investigations. (Figure 4)
Evaluation of azoospermic male (Figure 5)

Summary of recommendations
Begin infertility investigations if a woman of reproductive age has failed to conceive after 12 months of regular (2–3 times per week) unprotected vaginal sexual intercourse, in the absence of any known cause of infertility
Several published reports suggest faster ovarian aging in Indian women, it is recommended that all Indian women >32 years of age should be considered for expedited evaluation after 6 months of failed attempts to conceive, or earlier, if there is a known cause of infertility or a history of predisposing factors for infertility
All infertile couples must be provided pre-pregnancy counseling, detailed medical history, physical examination and general investigations to assess general health and detect medical and heritable genetic disorders having potentials to impact the mother and/or child’s health
Given the high incidence of thyroid disorders in Indian population, routine screening by measurement of thyroid stimulating hormone (TSH) is recommended in all Indian subfertile women
As the major causes of infertility are semen abnormalities, ovulation dysfunction and fallopian tube obstruction/impaired function, the basic/ preliminary investigations for the infertile couple should be focused on these only. However, it is recommended that for women aged >32 years or those <32 years with risk factors for early/expedited oocyte depletion, appropriate ovarian reserve tests, should also be included under standard/basic infertility evaluation
At mid-luteal phase (day 21 of a 28-day cycle), serum progesterone should be checked to confirm ovulation even if the woman has regular menstrual cycles. follicular ultrasound examination (follicle monitoring) is an accepted option to assess ovulation
Endometrial biopsy for histologic endometrial dating is not recommended, however, endometrial biopsy should be performed in women with suspected pathology, such as chronic endometritis or neoplasia
Women with irregular menstrual cycles and/or suspected of ovulation disorder should be offered serum gonadotropins (FSH and LH) and other relevant hormones including estradiol, AMH, and prolactin
Ovarian reserve testing may be considered for women aged >32 or for women <32 with risk factors for decreased ovarian reserve, such as those with previous ovarian surgery, poor response to FSH, endometriosis, previous exposure to chemotherapy or radiation, or unexplained infertility
Ovarian reserve tests are also helpful prior to ART treatment to predict poor responders and over–responders and may be used for counseling and selecting appropriate controlled ovarian stimulation protocol. However, these tests cannot predict clinically important outcomes such as pregnancy and should not be used to exclude an infertile couple from seeking ART
Women who are not known to have comorbidities (such as pelvic inflammatory disease, previous ectopic pregnancy or severe endometriosis) should be offered HSG or saline infusion sonohysterography (SIS) as an initial screen test for tubal occlusion under initial investigations, because this is a reliable test to rule out tubal occlusion, and less invasive
Women who are thought to have comorbidities should be offered laparoscopy and dye test so that tubal and other pelvic pathology can be assessed and treated at the same time
Women should not be offered hysteroscopy on its own as part of the initial investigation unless clinically indicated
The results of semen analysis conducted as part of an initial assessment should be compared with the World Health Organization 2010 reference values
If the semen analysis is normal, there is no need for a repeat analysis. If azoospermia or severe oligozoospermia is reported in the initial semen analysis, a repeat test should be undertaken within two to four weeks
Advice further relevant investigations, counseling and referral to a specialist for men who have two abnormal semen analyses
Genetic tests may be required in selected cases of subfertile men and women based on medical history, clinical features, and standard investigation reports, and should be accompanied by expert counseling by a clinical geneticist in all cases
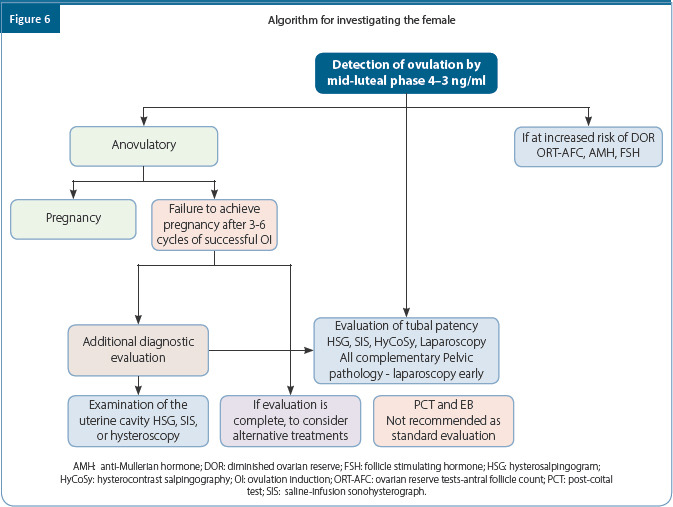
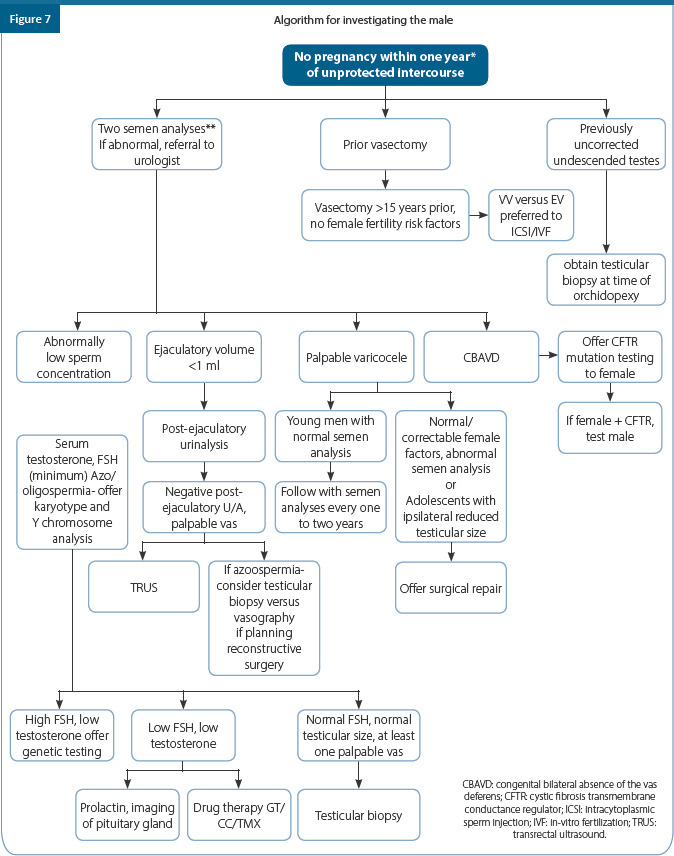
Table 7.
Important female reproductive hormone levels in blood and their clinical relevance (normal values should be guided by reference range of the laboratory used)
| Hormone Test | Timing | Normal range | Clinical relevance |
|---|---|---|---|
| Follicle stimulating hormone (FSH) | Day 3 of cycle | 4–8.9 IU/L | FSH>8.9 IU/L low ovarian reserve. FSH > 25 IU/L indicates Premature Ovarian Insufficiency (POI). Extremely low levels indicate hypogonadotropic hypogonadism. |
| Estradiol (E2) | Day 3 | 30–80 pg/ml | Abnormally high levels on day 3 (>80pg/ml) may indicate existence of a functional cyst or diminished ovarian reserve. Extremely low levels will be found in WHO Group 1 & Group 3 |
| Estradiol (E2). | Surge/hCG day | >200 pg/ml | The levels should be 150-200pg/ml per mature (18mm) follicle. |
| Luteinizing hormone (LH) | Day 3 | 3–10 IU//L | LH: FSH ratio >2 is an indication of PCOS. Extremely low levels of LH are seen in hypogonadotropic hypogonadism. |
| Luteinizing hormone (LH) | Surge day | >20 mlU/ml | The LH surge leads to ovulation within 48 hours. |
| Prolactin | 2–29 ng/ml | High levels >50- 100 ng/ml need further investigations to exclude prolactinoma | |
| Progesterone | Day 3 | <1.0 ng/ml | An elevated level may indicate a lower success rate for pregnancy. |
| Progesterone | Day 21 | >5 ng/ml (>15.9 nmol/L) | A level over 5 ng/ml indicates ovulation, but a level over 10ng/ml in a natural cycle indicates an adequate luteal phase |
| Anti-Mullerian hormone (AMH) | Any day of cycle | 1.2–3.5 ng/ml | There is no universal consensus on normal or cut off levels. AMH levels <0.75 – 1.2 ng/ml predict low response and >3.5 ng/ml predict high response in IVF cycles. |
| Thyroid stimulating hormone (TSH) | 0.35–5 mu/L | Subclinical hypothyroid in women desiring to become pregnant should be treated with the aim of keeping TSH <2.5mu/L | |
| Total testosterone | 8–70 ng/dl (0.5–3 nmol/L) | More than >2 SD above the mean for the assay used can suggest presence of androgen secreting ovarian or adrenal tumor | |
| Free testosterone | Follicular phase | 0.45–3.18 pg/ml | High quality assays such as LCMS/mass spectrometry and extraction/chromatography immunoassays should be used for the most accurate assessment of total or free testosterone |
| Luteal phase | 0.46–2.48 pg/ml | FAI or CFT are more reliable to assess biochemical hyperandrogenism in PCOS | |
| Dehydroepian-drosterone sulfate (DHEAS) | 20–24 yrs age | < 407 µg/dl | High levels can suggest an adrenal tumor |
| 25–34 yrs age | < 340 µg/dl | ||
| 35–44 yrs age | < 337 µg/dl | ||
| Androstenedione | 0.7–3 ng/ml (2.0–11 nmol/L) | Could be tested while investigating hyperandrogenism, if total or free testosterone not elevated | |
| Sex hormone binding globulin (SHBG) | 18–144 nmol/L | Increased androgen production often leads to lower SHBG. Free androgen Index (FAI) = (Total Testosterone ÷ SHBG) X 100 Normal FAI = 0.5%–6.5% | |
| 17 Hydroxy-progesterone (17-OHP) | Follicular phase | 0.32–1.47 ng/ml (<80 ng/dL) | Used for screening of congenital adrenal hyperplasia (CAH) due to 21–hydroxylase deficiency |
| Luteal phase | 0.25–2.91 ng/ml (<285 ng/dL) | Early morning 17– OHP levels of >200 ng / dL should prompt further evaluation. |
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| EBR | Begin infertility investigations if a woman of reproductive age has failed to conceive after 12 months of regular (2–3 times per week) unprotected vaginal sexual intercourse, in the absence of any known cause of infertility | A | II |
| EBR | In view of the several published reports suggesting faster ovarian ageing in Indian women, it is recommended that all Indian women >32 years of age should be considered for expedited evaluation after 6 months of failed attempts to conceive, or earlier, if there is a known cause of infertility or a history of predisposing factors for infertility | B | II |
| EBR | All infertile couples must be provided pre-pregnancy counselling, detailed medical history, physical examination and general investigations to assess general health and detect medical and heritable genetic disorders having potentials to impact mother and/or child’s health | A | II |
| EBR | In view of high incidence of thyroid disorders in Indian population, routine screening by measurement of TSH is recommended in all Indian subfertile women | A | II |
| EBR | As the major causes of infertility are semen abnormalities, ovulation dysfunction and fallopian tube obstruction/impaired function, the basic/preliminary investigations for the infertile couple should be focused on these only. However, it is recommended that for women aged >32 years or those <32 years with risk factors for early/expedited oocyte depletion, appropriate ovarian reserve tests, should also be included under standard/basic infertility evaluation | A | II |
| EBR | At mid-luteal phase (day 21 of a 28-day cycle), serum progesterone should be checked to confirm ovulation even if the woman has regular menstrual cycles | C | IV |
| EBR | Follicular ultrasound examination (follicle monitoring) is an accepted option to assess ovulation. | B | III |
| EBR | Endometrial biopsy for histologic endometrial dating is not recommended, however, endometrial biopsy should be performed in women with suspected pathology, such as chronic endometritis or neoplasia. | B | II |
| EBR | Women with irregular menstrual cycles and/or suspected of ovulation disorder should be offered serum gonadotropins (FSH and LH) and other relevant hormones including estradiol, AMH and prolactin. | B | III |
| EBR | Ovarian reserve testing may be considered for women aged >32 or for women < 32 with risk factors for decreased ovarian reserve, such as those with previous ovarian surgery, poor response to FSH, endometriosis, previous exposure to chemotherapy or radiation, or unexplained infertility | B | II |
| EBR | Ovarian reserve tests are also helpful prior to ART treatment to predict poor responders and over-responders and may be used for counseling and selecting appropriate controlled ovarian stimulation protocol. However, these tests cannot predict clinically important outcome such as pregnancy and should not be used to exclude an infertile couple from seeking ART | B | II |
| EBR | Women who are not known to have comorbidities (such as pelvic inflammatory disease, previous ectopic pregnancy or severe endometriosis) should be offered hysterosalpingography (HSG) or SIS as an initial screen test for tubal occlusion under initial investigations, because this is a reliable test to rule out tubal occlusion, and less invasive | A | II |
| EBR | Women who are thought to have comorbidities should be offered laparoscopy and dye test, so that tubal and other pelvic pathology can be assessed and treated at the same time | B | II |
| EBR | Women should not be offered hysteroscopy on its own as part of the initial investigation unless clinically indicated | A | I |
| EBR | The results of semen analysis conducted as part of an initial assessment should be compared with the World Health Organization 2010 reference values | A | II |
| EBR | If the semen analysis is normal, there is no need for a repeat analysis. If azoospermia or severe oligozoospermia is reported in the initial semen analysis, a repeat test should be undertaken within two to four weeks | A | I |
| CCR | Advice further relevant investigations, counselling and referral to specialist for men who have two abnormal semen analyses | B | - |
| EBR | Genetic tests may be required in selected cases of subfertile men and women based on medical history, clinical features and standard investigation reports, and should be accompanied by expert counselling by a clinical geneticist in all cases | B | III |
References
Fertility: assessment and treatment for people with fertility problems. NICE Clinical Guideline updated (2013). https://www.nice.org.uk>evidence>full-guideline-pdf-188539453.
Practice Committee Opinion of the American College of Obstetricians and Gynecologists and American Society for Reproductive Medicine. Female age-related fertility decline. Committee Opinion No.589. Obstet Gynecol 2014;295:1809-23
Advanced Reproductive Age and Fertility. Clinical Practice Guidelines No. 346. Journal of Obstetrics and Gynecology Canada 2017; 39 (8): 685-695.
Jindal UN. Mid-life fertility: Challenges & policy planning. Indian J Med Res 2018; 148 (Supplement):15-26.
Iglesias C, Banker M, Mahajan N, Herrero L, Meseguer M, Garcia- Velasco JA. Ethnicity as a determinant of ovarian reserve: differences in ovarian aging between Spanish and Indian women. Fertil Steril 2014;102:244 –9.
Ahuja M. Age of menopause and determinants of menopause age: A PAN India survey by IMS. J Midlife Health 2016;7:126-31 .
Infertility. National Health Portal of India 2016. http://www.nhp.gov.in.
Nandi A and Homburg R. Unexplained subfertility: diagnosis and management. The Obstetrician & Gynaecologist 2016;18:107-15.
Smith S, Pfiefer SM, Collins J. Diagnosis and management of female infertility. JAMA 2003;290:1767-70.
The Practice Committee of the American Society for Reproductive Medicine. Effectiveness and treatment for unexplained infertility. Fertil Steril 2006; 86 (5 Suppl);S111-4.
Consensus Documents for the Investigation of Infertility by Candian Fertility and Andrology Society (CFAS). August 2002.
The Federation of Obstetric & Gynecological Societies of India. Good Clinical Practice Recommendations on Preconception Care. 2016
Bajaj S. RSSDI clinical practice recommendations for the management of type 2 diabetes mellitus 2017. Int J Diabetes Dev Ctries.2018 Mar; 38 (Suppl 1):1-115.
Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017 Mar;27(3):315-389
FOGSI Gynaecologic Oncology Committee. FOGSI GCPR Screening and Treatment of Preinvasive Lesions of Cervix and HPV Vaccination . January, 2018
La Vignera S, Vita R, Condorelli RA, Mongioì LM, Presti S, Benvenga S, Calogero AE. Impact of thyroid disease on testicular function. Endocrine. 2017 Dec;58(3):397-407
Patel N, Kashanian JA. Thyroid Dysfunction and Male Reproductive Physiology. Semin Reprod Med. 2016 Nov;34(6):356-36
Practice Committee of American Society for Reproductive Medicine. Recommendations for reducing the risk of viral transmission during fertility treatment with the use of autologous gametes: a committee opinion. Fertil Steril. 2013 Feb;99(2):340-6
Ghosh K, Colah R, Manglani M, Choudhry V.P, Verma I, Madan N, Saxena R et al. Guidelines for screening, diagnosis and management of Hemogloginopathies. India J Hum Genet.2014 Apr-Jun;20(2): 101-119.
Practice Committee of the American Society for Reproductive Medicine in collaboration with the Society for Male Reproduction and Urology. Evaluation of the azoospermic male: a committee opinion. Fertil Steril. 2018 May;109(5):777-782
Malcolm CE, Cumming DC. Does anovulation exist in eumenorrheic women? Obstet Gynecol 2003;102:317-8.
Tammy J. L, Vitrikas K R. Evaluation and Treatment of Infertility. American Family Physician 2015;91(5):308-14.
Practice Committee of American Society for Reproductive Medicine. Diagnostic evaluation of the infertile female: a committee opinion. Fertil Steril. 2012;98(2):302-307.
Optimizing natural fertility: a committee opinion. Practice Committee of the American society for Reproductive Medicine in Collaboration with the society for Reproductive Endocrinology and Infertility. Fertil Steril 2017;107:52-8.
Cohlen B J, Van Santbrink E J P, Laven JSE. Ovulation Induction : Evidence based guidance for Daily Practice. CRC Press Taylor & Francis Group 2018: 11-15.
Robin G Gatto C, Catteau-Jonard S, Lefebuae – Maunoury C, Pigny P Duhamel A, Deiwailly De. Polycystic ovary – like abnormalities (PCO-L) in women with functional hypothalamic amenorrhea. In Clin Endocrinol Metab 2912; 97 (11): 4236-43
Wijeyaratne CN, Balan AH, Barth JH, Belchetz PE. Clinical manifestions and insulin resistance (IR) in polycystic ovary syndrome (PCOS) among South Asians and Caucasians: is there a difference? Clin Endocrinol (Oxf) 2002; 57:343-50.
Allahbadia GN, Merchant R. Polycystic ovary syndrome in the Indian subcontinent. Semin. Reprod. Med 2008;26(1):22-34.
Malik S, Verma S, Jain K, Talwar P, Prasad S, Dhorepatil B, Devi G Jindal U et al. Good clinical practice recommendations on management of infertility in patients from india with polycystic ovary syndrome. Fertil Sci & Res. 2015;2:107-32
Bhide P, Gudi A, Shah A, Homburg R. Serum anti- Mullerian hormone levels across different ethnic groups: a cross-sectional study. BJOG 2015;122:1625-29.
Rotterdam ESHRE / ASRM –Sponsored PCOS Consensus Workshop Group : Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004;81:19-25.
Balen AH. Polycystic ovary syndrome (PCOS). The Obstetrician & Gynaecologist: 2017;19:119-29.
International evidence- based guideline for the assessment and management of polycystic ovary syndrome 2018. Consensus guidelines by CREPCOS, MONASH University, ASRM and ESHRE. https://www.monash.edu
The ESHRE guideline group on POI: Management of women with premature ovarian insufficiency, Hum Reprod 2016; 31; 926-37
Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB. A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update 2006;12:685-718.
Maheshwari A, Fowler P, Bhattacharya S. Assessment of ovarian reserve- should we perform tests of ovarian reserve routinely? Hum Reprod 2006;21:2729-35.
Committee on Gynecologic Practice. Committee opinion no.618: Ovarian reserve testing. Obstet Gynecol 2015; 125:268-73.
Esteves SC, Roque M, Bedoschi GM, Conforti A, Humaidan P, Alviggi C. Defining low prognosis patients undergoing assisted reproductive technology: POSEIDON criteria- The why. Front Endocrinol 2018;9-461.
Juan A Garcia velasco, Manish banker (2017), Infertility management series: Investigating infertility,pp. 69 -77.
ASRM (2015), Diagnostic evaluation of the infertile female: a committee opinion, Fertil. Steril., Vol. 103, No, Pp.e44-e50.
Márcia Mendonça Carneiro (2014), What Is the Role of Hysteroscopic Surgery in the Management of Female Infertility? A Review of the Literature, Surgery Research and Practice, Pp.1-6.
Faten Mosbah Ibrahim Al-Zinaty, Mohammed Sayed Ali, Mohammed Mahmoud Al Sherbeeny, Tarek Aly Raafat (2018), Three-Dimensional Ultrasound versus Hysteroscopy in Uterine Cavity Assessment after Failed Intracytoplasmic Sperm Injection: a study for accuracy of a diagnostic test, The Egyptian Journal of Hospital Medicine, Vol. 75, No. 2, Pp.4565-4571.
Saravelos SH, Jayaprakasan K, Ojha K et al. Assessment of the uterus with three-dimensional ultrasound in women undergoing ART. Hum Reprod Update. 2017 Mar 1;23(2):188-210
Pleş L, Alexandrescu C, Ionescu CA, et al. Three-dimensional scan of the uterine cavity of infertile women before assisted reproductive technology use. Medicine (Baltimore). 2018; 97(41):e12764.
Bjorndahl L, Barratt C, Mortimer D, et al. ‘How to count sperm properly’: checklist for acceptability of studies based on human semen analysis. Human Reproduction, Volume 31, Issue 2, February 2016, Pages 227–232
Practice Committee of the American Society for Reproductive Medicine (ASRM). Diagnostic evaluation of an infertile male. Fertil Steril. 2015; 103(3):e18-25.
WHO Laboratory Manual for the Examination and Processing of Human Semen, Fifth Edition, 2010.
Practice Committee of the American Society for Reproductive Medicine (ASRM), Evaluation of the azoospermic male: a committee opinion. Fertil Steril 2018;109:777-82
Chapter 2: Ultrasound for Infertility
OVERVIEW
This guideline offers recommendations on the technique and safety of ultrasound scanning. It also provides recommendations for the use of the ultrasound scan for the evaluation of various gynecological pathologies. In addition to this, it provides recommendations for using the ultrasound for early first-trimester scan, ectopic pregnancy, evaluation of tubal patency, and sub-fertile man.
1. Overview of techniques and safety statement
1.1 Need for ultrasound in infertility:
To optimize the traditional anatomic diagnosis of the infertile male and female
To stratify patient care: expectant vs. medical vs. surgical vs. newer technique
Appropriate counseling of the patients in their specific infertility scenario
Ultrasound images provide a road map for surgery by determining the needed instruments, equipment’s, expertise, duration of surgery, cost and recovery time
Provides information to the patients with respect to the limitations associated with the success of the surgery and treatment.
Providing a fast decision on whether to perform surgery/surrogacy in women with uterine factor
The technique is cost-effective
1.2 Safety of ultrasound
Evidence suggests that ultrasound scanning has not produced any harm to patients from the time (over four decades) it is being used
Transvaginal scans and 3D/4D scans are also found to be safe
The embryonic heart should be evaluated by M–mode
Keep the examination times as short as required to produce a useful diagnostic result
Keep the output levels as low as is reasonably achievable (ALARA principle) while producing a useful diagnostic result
1.3 Category of infertility ultrasounds
The category of infertility ultrasounds should be specified in the requisition and in the report. The categories include: (Figure 1)

1.4 Components of a detailed gynecological scan
-
A detailed gynecological scan includes following components:
-
»Cervix and uterus–endometrium , myometrium
-
»Ovaries – antral follicle count, ovarian reserve, polycystic ovaries, follicular development, corpus luteum development, presence of physiological and pathological ovarian cyst
-
»Tubes – USG guided procedures to establish patency (SIS, HyCoSy), diagnosis of pathology (hydrosalpinx, ectopic pregnancy)
-
»Peritoneum, lymph nodes
-
»Abnormalities if any
-
»
1.5 Points be considered while performing a gynecological scan
-
»
In order to minimize chances of missing large lesions, wandering fibroids, and high located ovaries, a transabdominal scan is encouraged as a scout procedure
-
»
Transvaginal scanning should commence at the introitus
-
»
Each component of pelvic anatomy should be scanned from superior to inferior, medial to lateral, and anterior to the posterior extent; mobility of viscera is particularly important
-
»
During scanning, all negative and positive findings must be imaged and documented
-
»
Any variation from the protocol should be supported by valid reason and this should be documented in the report
-
»
Every institution/clinic can have its own limited protocol if there is resource restriction, shortage of staff or compromised equipment. The patient must be made aware of this institutional limitation
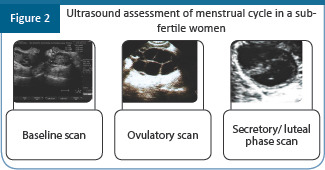
1.6 Assessment of the cycle should include the following (Figure 2)
2. Guidelines for the first visit scan
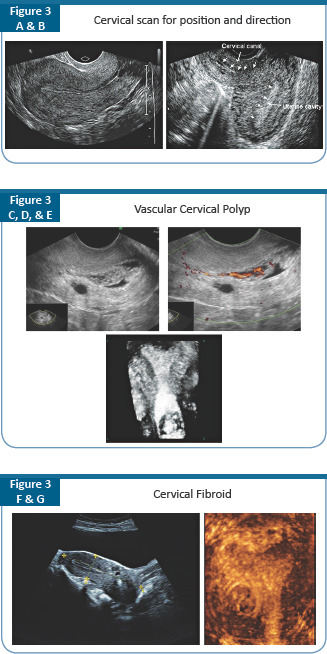
A detailed scan at the first visit of the patient can offer tremendous insight into the cause of infertility
Cervical scan: Position, direction and abnormality (Figure 3 A, B, C, D, E, F, and G)
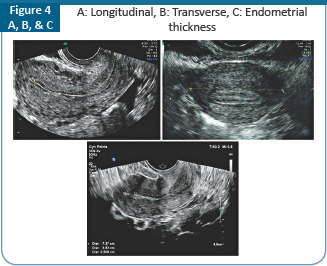
2.1 Evaluation of uterus (Figure 4 A, B and C)
-
»
Longitudinal, AP, and Transverse measurement
-
»
Uterocervical length
-
»
To identify uterine abnormalities – myoma, adenomyosis, polyps, intrauterine adhesions, endometrial abnormalities, congenital anomalies
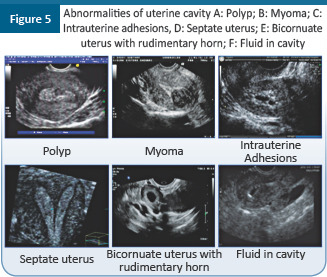
2.2 Evaluation of Uterine cavity
-
»
The intrauterine abnormalities that need to be looked for are shown in Figure 5 A–F
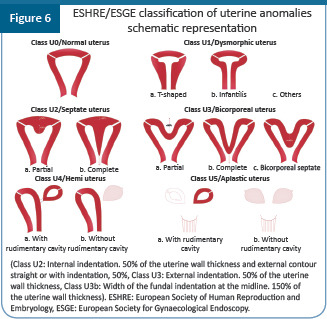
2.3 Female congenital uterine anomalies
-
»
The European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE) classification for the female genital tract anomalies is given in table 1 and Figure 6
Table 1.
The ESHRE/ESGE classification for the genital tract anomalies
| Uterine anomaly | Cervical or vaginal anomaly | ||
|---|---|---|---|
|
| |||
| Main class | Sub-class | Co–existent class | |
| U0 | Normal uterus | C0 Normal cervix C1 Separate cervix C2 Double normal cervix C3 Unilateral cervical aplasia C4 Cervical aplasia V0 Normal vagina V1 Longitudinal non–obstructing vaginal septum V2 Longitudinal obstructing vaginal septum V3 Transverse vaginal septum and/or imperforate hymen V4 Vaginal aplasia |
|
| U1 | Dysmorphic uterus | a. T–shaped b. Infantilis c. Others |
|
| U2 | Septate uterus | a. Partial b. Complete |
|
| U3 | Bicorporeal uterus | a. Partial b. Complete c. Biocorporeal septate |
|
| U4 | Hemi-uterus | a. With rudimentary cavity (communicating or horn) b. Without rudimentary cavity (horn without cavity/ no horn) |
|
| U5 | Aplastic | a. With rudimentary cavity (bilateral or unilateral horn) b. Without rudimentary cavity (bilateral or unilateral uterine remnants/aplasia) |
|
| U6 | Unclassified malformation | ||
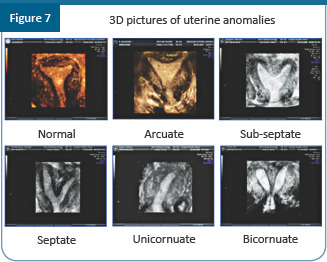
Combination of both 2D and 3D reveal the accurate diagnosis of uterine anomalies. (Figure 7)
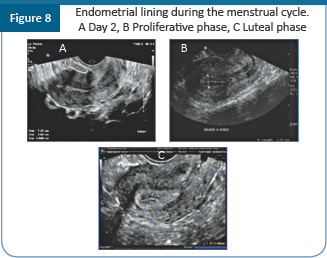
The uterine cavity ultrasound is also done for evaluating the endometrial development when monitoring an ovulation induction cycle (Figure 8 A–C). In the proliferative phase, after day, 7 the endometrium should be multilayered endometrium consisting of prominent outer and midline hyperechogenic lines and inner hypoechogenic regions. Under the influence of progesterone, the endometrium will be entirely homogenous and hyperechogenic. This pattern is usually seen in the luteal phase or when there is progesterone elevation in the late follicular phase
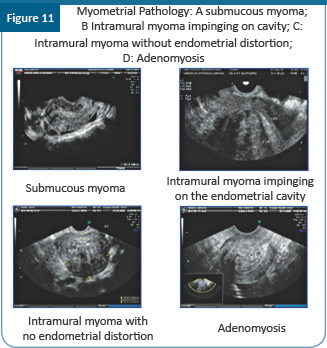
2.4 Evaluation of myometrial pathologies
Reporting protocol
The presence or absence of the fibroids
Location of the fibroid
Number of fibroids
Size of the fibroids
Presence of pedicles
Echogenicity/calcification of the fibroids
Degree of vascularization
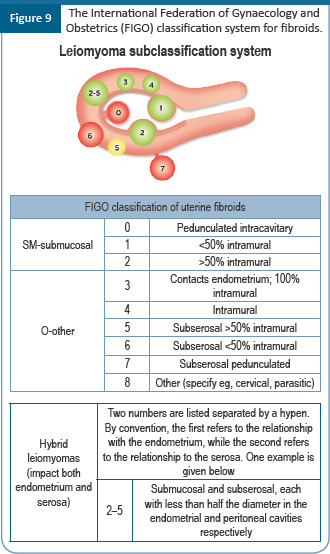
2.4.1 Classification system for fibroids
The International Federation of Gynaecology and Obstetrics (FIGO) classification is the most employed nowadays (Figure 9)
2.5 Ultrasound features of adenomyomas
-
Checklist for labelling
-
»The shape of focal lesions is elliptical rather than globular
-
»Rim vascularization is absent
-
»Presence of spoke wheel vascularization or radial arteries running through the lesion
-
»Calcification is absent in the lesions
-
»A mild mass effect disproportionate to the size of the abnormal area
-
»Adenomyomas can be associated with multiple, small, regular cysts vs. cystic fibroids which occur only after degeneration and are large, solitary and irregular in outline
-
»Adenomyosis is characterized by uterine enlargement: Anterior/posterior
-
»The enlargement can be focal/diffuse in the absence of fibroid
-
»Presence of improper defined hyperechogenic (heterotopic endometrial glands) and hypoechogenic areas (smooth muscle hyperplasia)
-
»Presence of small anechoic cysts in the myometrium
-
»In distinct endometrial/myometrial margin
-
»Minimal mass effect on the cavity/serosa compared to the size of the lesion
-
»The myometrium is diffusely echogenic
-
»Presence of echogenic nodules or linear striations radiating out from the endometrium into the myometrium
-
»An increased number of tortuous vessels that penetrate throughout the involved myometrium
-
»
Figure 10 shows the ultrasound pictures of fibroid uterus and adenomyosis
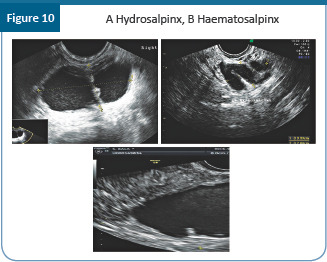
2.6 Tubal evaluation
The fallopian tubes can be visualized only in the presence of a pathology.
Hydrosalpinx
Sonographic features diagnostic for hydrosalpinx include a tubular or S–shaped cystic mass separate from the ovary, with “beads on a string” or “cogwheel” appearance. (Figure 11)
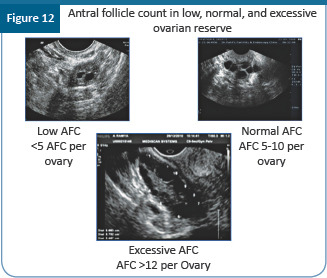
2.7 USG assessment of ovarian reserve
-
Antral follicle count (AFC): (Figure 12)
-
»Good correlation small follicle count and primordial pool and responsiveness. The AFC should be the first choice test
-
»The number of small antral follicles (2–6 mm) represents functional ovarian reserve
-
»
-
Ovarian volume (OV) :
-
»Good correlation between OV and age and primordial follicle pool
-
»Weak correlation with ovarian
-
»
-
4 D USG–Sono AVC
-
»It determines the hypoechoic aspect of the ultrasound, display is inverted to demonstrate fluid–filled areas within the 3D dataset which are the follicles
-
»Best model in predicting the number of oocytes retrieved
-
»Oocyte retrieval rate–60%
-
»
2.8 Ultrasound assessment of PCO
2.8.1 Rotterdam consensus
-
»
Polycystic ovary contains 12 or more follicles measuring 2–9 mm in diameter on day 2 or 3 of MC
and/or
-
»
Increased ovarian volume (>10 cm3)
-
»
No dominant follicle > 10 mm or CL
These features do not apply to women taking OCP, as ovarian size is reduced, even though the polycystic appearance may persist. Ultrasound is also not reliable in the diagnosis of polycystic ovaries in adolescent girls.
-
Ultrasonography criteria for diagnosing PCOS
-
»Transvaginal ultrasound is preferred because it often provides optimal visualization of the internal structure of the ovary
-
»Regularly menstruating women should undergo scanning during the early follicular phase (days 2–5)
-
»Oligomenorrhoeic or amenorrhoeic women may be scanned at random
-
»The entire ovary and both must be scanned
-
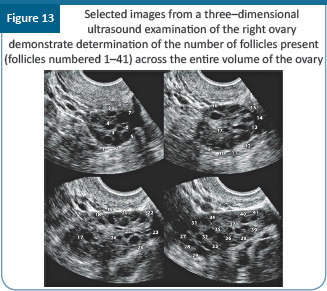
»One or both ovaries demonstrate 20 or more follicles measuring 2–9 mm in diameter (Figure 13), or
-
»The ovarian volume exceeds 10 cm3
-
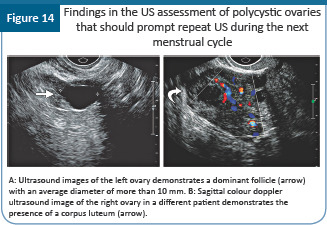
»If there is evidence of a dominant follicle (>10 mm) or a corpus luteum, the scan should be repeated in the next cycle between 2–4 (Figure 14)
-
»Only one ovary meeting either of these criteria is sufficient to establish the presence of polycystic ovaries
-
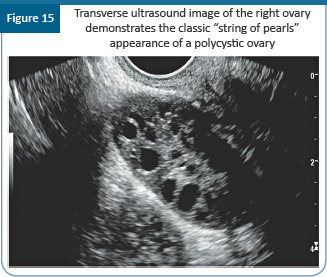
»To identify a polycystic ovary, subjective appearance should not be used in place of ovarian volume and follicle count (follicle distribution and increase in stromal echogenicity are omitted) (Figure 15)
-
»Ovarian volume should be calculated based on the simplified formula for a prolate ellipsoid (0.5 × length × width × thickness of the ovary)
-
»The mean of the diameters of any large cystic area should be used in ovoid structures and not the maximum diameter
-
»
-
Clinical consensus recommendations (CCR) and clinical practice points (CPP) for the assessment of PCOS includes:
-
»CCR
- - Ultrasound should not be used for the diagnosis of PCOS in those with a gynecological age of <8 years (<8 years after menarche), due to the high incidence of multifollicular ovaries in this life stage
- - The threshold for PCOM should be revised regularly with advancing ultrasound technology, and age-specific cut off values for PCOM should be defined
- - A transvaginal ultrasound approach is preferred in the diagnosis of PCOS, if sexually active and if acceptable to the individual being assessed.
- - Using endovaginal ultrasound transducers with a frequency bandwidth that includes 8 MHz
-
»CPP
- - If using older technology, the threshold for PCOM could be an ovarian volume ≥ 10 ml on either ovary
- - In patients with irregular menstrual cycles and hyperandrogenism, an ovarian ultrasound is not necessary for PCOS diagnosis; however, ultrasound will identify the complete PCOS phenotype
- - In transabdominal ultrasound reporting is best focused on ovarian volume with a threshold of ≥ 10 ml, given the difficulty of reliably assessing follicle number with this approach
-
»
2.9 Prediction of response
Table 2.
Ultrasound markers of high and low response
| Markers of high response | • Increased AFC |
| • Color doppler – Increased stromal velocity | |
| • Increased AMH | |
| Markers of low response | • High FSH and E2 |
| • Low AMH, Inhibin B, | |
| • AFC < 5 | |
| • Ovarian volume | |
| • Low flow at color doppler |
AMH: anti-Mullerian hormone; AFC: antral follicle count; FSH: follicle stimulating hormone; E2: estradiol.
3. Ultrasound for ovarian lesions
-
Morphological features of adnexal lesion
-
»An adnexal lesion is the part of an ovary or an adnexal mass that is judged from an assessment of ultrasound images to be inconsistent with normal physiologic function.
-
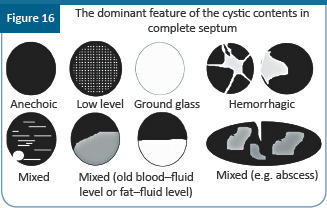
»Adrenal lesion arises due to the presence of cysts. The features of cystic content are given in Figure 16.
-
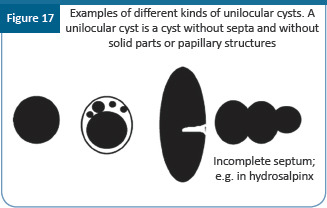
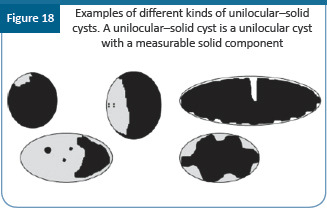
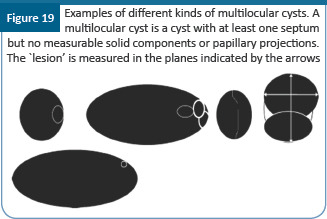
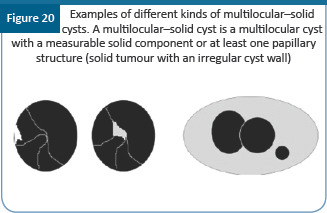
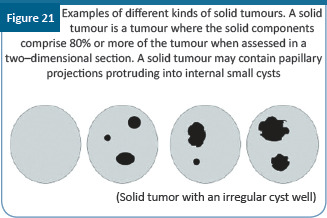
»The morphological features of various types of cysts that may be observed in an adnexal mass are given in Figures 17,18,19, 20, and 21
-
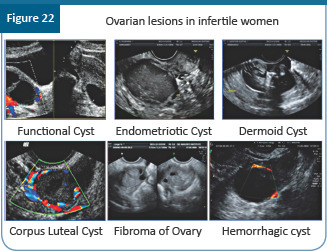
»Differential diagnosis of adnexal masses: It is important to remember that all adnexal or pelvic masses are not of gynecologic origin (Figure 22)
-
»
-
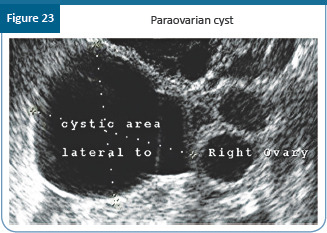
Fimbrial and paraovarian cysts (Figure 23)
-
»Fimbrial and paraovarian cysts are a common finding in women of reproductive age and represent embryological remnants
-
»These are small, round, unilocular, and thin walled
-
»No proven significance for fertility
-
»These should be separate from the ovaries
-
»Gentle pressure with the transducer will displace the cyst(s) away from the homo- lateral ovary, unless there are adhesions
-
»
4. Protocol for tubal patency evaluation
For patients presenting with infertility, tubal assessment is essential
To exclude hydrosalpinx and adhesions, transvaginal ultrasound scan is the primary investigation, especially for those females who also have other pathologies like pelvic inflammatory disease, previous history of ectopic pregnancy and endometriosis
For tubal occlusion, hysterosalpingography (HSG) is still considered a primary screen. This is a reliable test to rule out tubal occlusion and is less invasive
Screening for tubal occlusion using hysterosalpingo contrast ultrasonography (HyCoSy) should be considered when appropriate expertise is available. It is an effective alternative for women who are known to have other pathologies like pelvic inflammatory disease, previous history of ectopic pregnancy, and endometriosis
Where facility and expertise are available, HyCoSy can also be offered with 3D ultrasound. This can add to the information available with 2D HyCoSy
Laparoscopy with dye test is the investigation of choice for patients with pathologies that are likely to cause tubal damage. It is considered as a gold standard for the evaluation of tubal patency
5. Guidelines for the day 2 scan
-
Checklist for baseline scan (done on day 2 or day 3/day 4) when the ovaries are silent with no follicles >8 mm
-
»Follicular size is <10 mm
-
»Residual cystic areas should be excluded
-
»Assessment of pelvic pathology, if any
-
»Assessment of uterine cavity configuration if not done earlier
-
»To confirm that endometrium is <6 mm
-
»To perform antral follicle count
-
»
6. Imaging with Doppler and 3D/4D
The requirement from ultrasound where doppler & 3D/4D plays a significant role includes:
-
»
To confirm or exclude a lesion
-
»
Provide an anatomical diagnosis
-
»
Helps to identify pointers toward histopathology
-
»
Assess extent and contralateral involvement
-
»
To look for borderline tumours
-
»
Assess the rest of the abdomen and the pleura on either side.
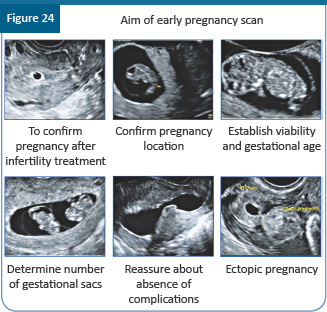
7. Early first trimester scan
Aims of the early pregnancy USG (Figure 24)
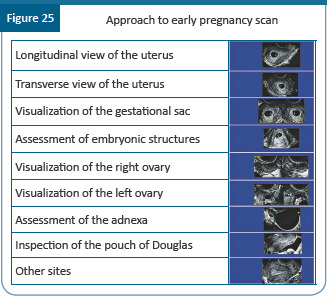
7.1 Systematic approach
-
Early sonographic markers which are found to be associated with poor pregnancy viability includes:
-
»Embryonic bradycardia
-
»Suboptimal embryonic growth
-
»Abnormal yolk sac
-
»Choriodecidual hematoma
-
»Peritrophoblastic hyperemia
-
»
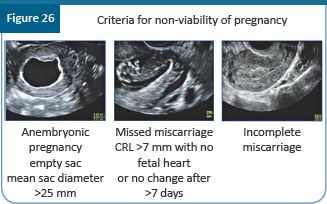
7.2 Diagnosis of miscarriage
Criteria for non-viability in the first trimester of pregnancy (Figure 26)
8. Ectopic pregnancy after assisted reproductive technology (ART)
The incidence of ectopic pregnancy after IVF ranges from 2.1% to 9.4% of all clinical pregnancies
Even if one pregnancy is located in the uterus, do not stop looking at the adnexa: There may be a concurrent adnexal gestation
Even if one pregnancy is located in the adnexa, keep looking: There may be a concurrent second adnexal gestation
-
Ultrasound technique for ectopic pregnancies
-
»Transabdominal ultrasound can be used
-
»Transvaginal scan: Preferably high frequency transducer with power doppler should be used
-
»Try 3D ultrasound
-
»Thoroughly inspect uterine cavity, ovaries, rest of adnexa, and the pouch of Douglas
-
»Assess the free fluid
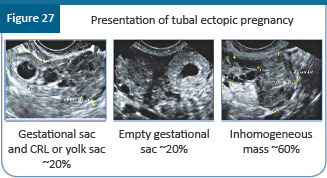
- - Presentation of tubal ectopic pregnancy (Figure 27)
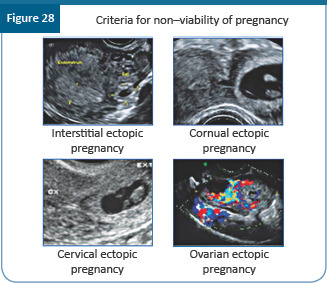
- - Other locations of ectopic pregnancy (Figure 28)
-
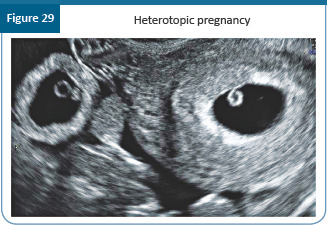
- Heterotopic pregnancy (Figure 29)
- # An ectopic pregnancy with an intra-uterine pregnancy
- # 1 in 7,500–30,000 spontaneous conceptions
- # 1–3 in 100 pregnancies conceived via ART
- # Heterotopic pregnancy (Figure 27)
-
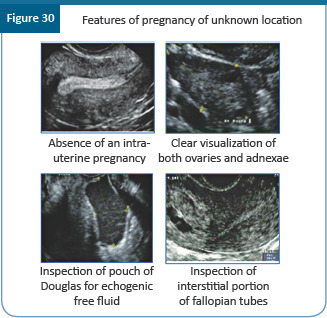
- Pregnancy of unknown location
- # Working diagnosis only
- # All women need follow-up to determine final outcome
- # PUL rates should be < 15%
- # Features of pregnancy of unknown location are seen in Figure 30
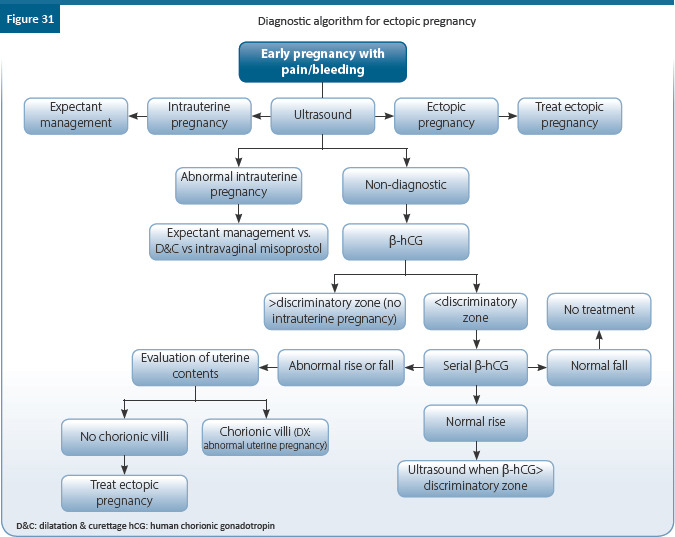
- - Diagnostic algorithm for ectopic pregnancy is given in Figure 28
-
»

9. Imaging in the infertile male
-
Imaging in infertile men is necessary in presence of abnormal semen analysis–low volume, severe oligoasthenospermia, azoospermia, hydrocele, and in those with a suspicion of absent vas, undescended testis, and varicocele
-
»Imaging helps to identify the causes of infertility, such as congenital anomalies and disorders that obstruct sperm transport and may be correctable
-
»Scrotal ultrasound is excellent for initial evaluation of male reproductive system and reproductive system, including the testes and extratesticular structures such as the epididymis for presence/absence, calcification, masses, cysts, hydrocele, and varicocele
-
»To assess the seminal vesicles and prostatic cysts, a transrectal scan is recommended
-
»
Recommendations
Appropriate selection of imaging modalities and accurate characterization of the various underlying reproductive abnormalities and treatment helps to guide individual management decisions and maximize infertility treatment outcomes
Two-dimensional US is the most widely available method for female evaluation and easiest to perform
Two-dimensional US should be performed in all women who present with sub-fertility
3D/4D USG and SIS–increase the specificity and sensitivity
If available 3D US should be done along with 2D US
2D USG in conjunction with HSG, increases accuracy particularly in the absence of 3D US, or where SIS is not practiced
All techniques are complementary to each other for accurate diagnosis and appropriate management
Baseline USG between 2–4 should be done in all before initiation of treatment in every cycle as it provides invaluable information on ovarian morphology and allows to choose appropriate stimulation regimen to prevent OHSS and multiple pregnancies and prediction of patients response to ovarian stimulation
USG monitoring of follicular growth is the most important tool in assessment of progress in ovarian stimulation and should be used in all patients undergoing ovulation induction
Ultrasound improves chance of safe and effective treatment
USG also allows diagnosis of disorders and complications of ovulation
Monitoring luteal phase helps confirm ovulation and pregnancy by b-hCG assay and USG documentation of pregnancy (20 days post ovulation when b hCG is 1000 mIU/ml), an end-point desired of tracking ovulation
Ultrasound in the male should be done in all with azoospermia, oligoasthenospermia, hydrocele, and suspicion of absent vas deferens, undescended testis, and varicocele
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CPP | Appropriate selection of imaging modalities and accurate characterization of the various underlying reproductive abnormalities and treatment helps to guide individual management decisions and maximize infertility treatment outcomes | - | - |
| CPP | Two-dimensional US is the most widely available method for female evaluation and easiest to perform | - | - |
| CPP | Two-dimensional US should be performed in all women who present with sub-fertility | - | - |
| CPP | 3D/4D USG and SIS–increase the specificity and sensitivity | - | - |
| CPP | If available 3D US should be done along with 2D US | - | - |
| CPP | 2D USG in conjunction with HSG, increases accuracy particularly in the absence of 3D US, or where SIS is not practiced | - | - |
| CPP | All techniques are complementary to each other for accurate diagnosis and appropriate management | - | - |
| EBR | USG at first visit evaluates the cervix, uterus, ovaries, and adenexa to provide diagnostic information and guidance to management | B | II |
| EBR | Baseline USG between 2–4 should be done in all before initiation of treatment in every cycle as it provides invaluable information on ovarian morphology and allows to choose appropriate stimulation regimen to prevent OHSS, multiple pregnancies, and prediction of patients response to ovarian stimulation | B | II |
| EBR | USG monitoring of follicular growth is the most important tool in assessment of progress in ovarian stimulation and should be used in all patients undergoing ovulation induction | A | II |
| EBR | Ultrasound improves chance of safe and effective treatment | C | III |
| EBR | USG also allows diagnosis of disorders and complications of ovulation | B | III |
| EBR | Monitoring luteal phase helps confirm ovulation and pregnancy by b-hCG assay and USG documentation of pregnancy (20 days post ovulation when beta hCG is 1000 mIU/ml), an end point desired of tracking ovulation | B | II |
| EBR | Ultrasound in the male should be done in all with azoospermia, oligoasthenospermia, hydrocele and suspicion of absent vas deferens, undescended testis, and varicocele | B | III |
References
SCoR/BMUS Guidelines for Professional Ultrasound Practice.2018. Available online on: https://www.bmus.org/static/uploads/resources/SCoR__BMUS__Guidelines_Amend_Mar_2019_final_DecHwyx.pdf
Di Spiezio Sardo A, Mazzon I et al. Hysteroscopic myomectomy: A comprehensive review of surgical techniques. Human Reproduction Update.2008; 14(2):101 -19.
Lasmar RB, Xinmei Z et al. Feasibility of a new system of classification of submucous myomas: A multicenter study. Fertility and Sterility.2011; 95(6):2073 -2077.
Munro MG, Critchley HO et al. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011; 113(1):3-13.
Cunningham RK, Horrow MM et al. Adenomyosis: A sonographic diagnosis. RadioGraphic.2018; 38(5):1576–89.
Grimbizis GF, Gordts S et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum Reprod.2013; 28(8):2032–44.
Boyle J, Teede HJ et al. Polycystic ovary Syndrome-an update. 2012; 41(10):752 -6.
Williams T, Mortada R et al. Diagnosis and treatment of polycystic ovary syndrome. Am Fam Physician. 2016 ;94(2):106 -13.
Lee TT, Rausch ME. Polycystic ovarian syndrome: Role of imaging in diagnosis. Radiographics. 2012;32(6):1643-57.
Teede HJ, Misso ML et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril 2018; 110(3):364-79.
Timmerman D, Testa AC et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet Gynecol 2008;31:681–90.
Timmerman D, Valentin L et al. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: A consensus opinion from the International Ovarian Tumor Analysis (IOTA) group. Ultrasound Obstet Gynecol 2000; 16:500 -05.
Chapter 3: Genetic Analysis for Infertility Detection
OVERVIEW
This guideline offers recommendations on the requirement of genetic analysis for the detection of infertility in adult male and females. It also gives an overview of few tests recommended for the genetic analysis required for infertile patients.
1. Introduction
Chromosomes carry genes that determine the existence and form of organisms
Genes are made of DNA, where the particular DNA sequence determines the function of the gene
Genetic disease or disorder is the result of changes or mutations, in an individual’s DNA which can be inherited or acquired/De novo (spontaneous or induced by UV light/chemicals/radiation)
Chromosomal abnormalities as a result of abnormal chromosome number, structure, or rearrangement can result in infertility
Infertility is genetic in origin in at least 10%–15% of men and 5%–10% of women
Genetic defect seen in >20% of cases with azoospermia
20% of cases of genetic counselling is related to fertility problems
Genetic testing helps to finalize a causal diagnosis; and to asses the genetic risk for the offspring in case of successful treatment
But only few genetic tests are routinely applied in clinical practice
2. Genetic abnormalities associated with infertility
2.1 In males
-
Genes can interfere with male fertility during gonads development (in utero life). Eg: Testicular dysgenesis, gonadotrophin action (hormones and receptors), eg: Kallmann syndrome, organs malformations, eg: Cystic fibrosis (CBAVD and CFTR), at gametogenesis level, eg: Y microdeletion and sexual behaviour abnormalities. Chromosomal aberrations are responsible for 5%–10% cases of azoospermia and severe oligospermia
-
»Chromosomal aberrations–sex chromosome
- - 47,XXY and mosaicisms (Klinefelter syndrome)
- - 47,XYY and other YY–aneuplodies
- - 46,XX and 45, X males
- - Structural Y chromosomal aberrations (del, rings, inversions, etc)
- - Chromosomal aberrations–autosomes
-
»
Translocations (Robertsonian, reciprocal)
Inversions
Other structural anomalies
-
Clinical syndromes (Trisomy 21, etc)
-
»Gene mutations–sex chromosome
- - Y–linked–microdeletions Yq11 (5%–10% case of azoospermia and severe oligospermia)
- - X–linked–Kallmann syndrome, androgen insensitivity syndrome, Kennedy disease (2%–3% cases of azoospermia and severe oligospermia)
-
»Gene mutations–Autosomal
- - Complex genetic syndromes with infertility as minor manifestation or major manifestation (with mutation of CFTR, FSH-β, LH-β, FSH-R, LH-R genes) responsible for 5% male Infertility and 60%–70% cases of CBAVD
-
»
2.2 In females
Incidence: 1.5%–3.3% among sub-fertile women verses 0.16% in general population. These are mostly aneuploidies and rearrangements involving sex chromosomes with small to moderate reproductive risk
-
Chromosomal aberrations of sex chromosomes
-
»Turners syndrome with/without mosaicism
-
»Gonadal dysgenesis with Y cell line
-
»X–autosomal translocation
-
»47, JHRS_ISAR_IFS with/without mosaicism
-
»
-
Autosomal chromosomal aberrations
-
»Robertsonian translocation
-
»Reciprocal translocation
-
»Inversions
-
»
-
X–linked gene mutations
-
»Fragile X syndrome
-
»Kallmann syndrome
-
»Complete androgen sensitivity syndrome
-
»
-
Gene mutations in autosomal chromosomes resulting in complex genetic syndromes with infertility as minor manifestation or major manifestation
-
»With mutation of FSHβ gene, FSHR gene, LHR gene, GnRHR gene, steroid enzyme genes (CYP17, CYP19, HSD17B3, autoimmune regulatory (AIRE) gene , FOXL2 gene , HOXA13 gene, BPES
-
»
3. Genetic screening for infertility: When should it be done?
3.1 Male
Depending on semen analysis and clinical findings, the infertile male patient needs genetic evaluation to identify pattern of inheritance (autosomal-dominant, autosomal-recessive or X-linked)
In men with severe oligo-astheno-teratozoospermia and azoospermia physical examination for secondary sexual characteristic, testicular size, and consistency, epididymal abnormalities, varicocele, a per rectal examination for seminal vesicular, and prostatic abnormalities should be done
Presence of globozoospermia or round head syndrome also require genetic testing
FSH and testosterone should be done and if abnormal test for SHBG, prolactin, LH, E2, and repeat testosterone
Karyotype analysis and Y–chromosomal microdeletion screening should be performed in patients with azoospermia or severe oligozoospermia in order to rule out structural chromosomal abnormalities, Klinefelter syndrome, and Y chromosome microdeletions
Men with azoospermia with decreased seminal volume, pH and markers of epididymal (a-glucosidase), and seminal vesicle (fructose) function in the presence of normal luteinizing hormone (LH), follicle–stimulating hormone (FSH) and testosterone levels. need CFTR gene screening
If clinical findings suggest hypogonadotropic hypogonadism (HH) like low sex steroid and low gonadotropin levels, perform HH mutation screening
Oligozoospermic men with hypospermatogenesis and normal FSH levels (<8 IU/L) should be evaluated for FSH and LH receptor polymorphism
If Kennedy syndrome suspected androgen receptor CAG repeats abnormalities should be tested for
3.2 Females
Genetic testing in the female is required in presence of primary or secondary amenorrhea, polycystic ovary syndrome (PCOS), premature ovarian insufficiency (POI), poor ovarian reserve or response, hyper-response, recurrent implantation failure or pregnancy loss (RPL), endometriosis, adenomyosis, leomyoma, unexplained infertility, hypogonadotropic hypogonadism (HH), and those who would be subjected to gonadotoxic chemotherapy or radiotherapy
Immense clinical variability in features associated with GnRH deficiency resulting in hypogonadotropic hypogonadism may be due to mutations of two distinct genes in an individual, which may generate a more severe phenotype than a single–gene alteration.
Look for symptoms and signs of diminished ovarian reserve, early menopause, endometriosis, and hyperandrogenemia
Look for symptoms and signs of Turner’s syndrome (short stature, webbed neck, puffiness or swelling (lymphedema) of the hands and feet, skeletal abnormalities, heart defects, high blood pressure, and kidney problems
Kallmann syndrome–primary amenorrhoea , anosmia, hypogonadism, bimanual synkinesia, and renal anomalies
Familial premature ovarian failure (POF), the incidence of which varies from 4% to 31% associated with hypergonadotropic hypogonadism. The inheritance of POF may be autosomal dominant sex-limited or X-linked. The POF risk is 2–fold higher in women with the FMR1 premutation
Congenital absence of the uterus and vagina (Mayer– Rokitansky–Kuster–Hauser) syndrome – There is complete aplasia of the vagina and uterus with two rudimentary horns and normal fallopian tubes or vaginal aplasia with either symmetric uterine hypoplasia or aplasia of one horn, tubal malformation, and other associated malformations. Tendency to familial distribution suggests the potential for a genetic link (mutation of the WNT4 gene)
Hemoglobinopathies
Genetic conditions like galactosemia, cystic fibrosis, Prader Willi etc. also cause the genetic changes and may induce infertility
Recognition of mosaic turners and Klinefelter’ syndrome early will enable us to cryopreserve the gametes, thus preserving fertility.
4. Genetic tests for the detection of infertility
4.1 Genetic testing done by
Comprehensive chromosome screening (CCS)
aCGH
SNP microarray
qPCR
NGS
4.2 For males
Karyotype in non–obstructive azoospermia and severe oligospermia
“Y” microdeletion in non–obstructive azoospermia and severe oligospermia
CFTR gene mutation in obstructive azoospermia
Androgen receptor mutation in non–obstructive azoospermia and severe oligospermia
INSL3/RXFP2 gene mutation in cryptorchidism
HH gene mutation in HH and Kallmann syndrome
Testing for sperm aneuploidy and DNA fragmentation is still debatable
4.3 For females
Karyotype–Turner syndrome (46X) and Swyer syndrome (46XY)
Diagnosis of Kallmans syndrome (KAL1, FGFR1, and CHD7 genes)
CFTR mutation
POI - FMR1 mutation in Fragile-X Syndrome
5. What is the need of these recommendations?
-
These recommendations will help in providing options for couples with increased genetic risk
-
»Genetic counselling
-
»To accept the risk
-
»Refrain from having children
-
»Adoption
-
»Sperm or oocytes donation
-
»Prenatal diagnosis (PND)
-
»Preimplantation genetic diagnosis/screening (PGD/PGS)
-
»
6. Preimplantation genetic testing (PGT)
6.1 PGT Test
It is a test performed to analyze the DNA from oocytes (polar bodies) or embryos (cleavage stage or blastocyst) for HLA-typing or for determining genetic abnormalities
PGT for aneuploidies (PGT-A): Formerly known as PGS or CCS–screens for the presence of all 46 chromosomes. PGT – A is done in good prognosis patients (adequate number of embryos) and indications being advanced age (>37 years), recurrent implantation failure, recurrent pregnancy loss (without known genetic abnormality), severe male factor infertility, and embryo selection
PGT for monogenic/single gene defects (PGT-M): Formerly known as PGD for single gene disorders or HLA typing – Examples: Cystic fibrosis, BRCA, Huntington’s disease
PGT for chromosomal structural rearrangements, X linked and autosomal chromosomal abnormalities (PGT-SR). Formerly known as PGD for chromosome rearrangements; examples: chromosome translocations, and inversions
6.1.1 Day of biopsy
One could do a polar body, blastomere biopsy on day 3 or trophectoderm biopsy on day 5. The advantages and disadvantages of the same are given in the Figure 1
Therefore, whenever possible, trophectoderm biopsy should be the method of choice in embryo biopsy and should be performed by experienced hands
No increase in live birth rate (LBR) but fewer miscarriages
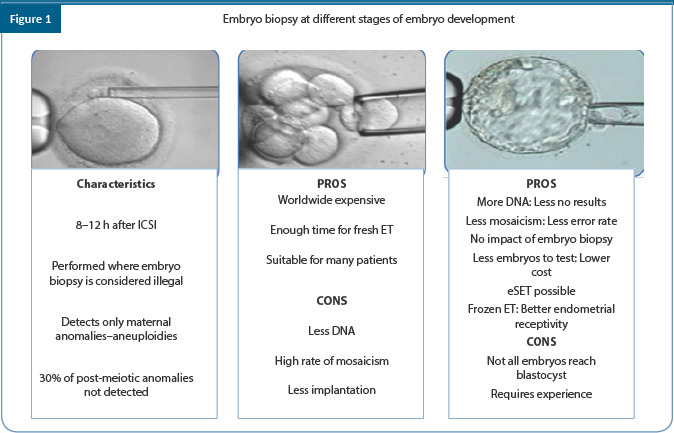
6.1.2 Disadvantages to PGT
Poor lab condition might hamper blastocyst formation, mandating a state of ART lab conditions
Poor morphology embryos–may degenerate at biopsy
Failure to amplify
Embryo loss during long–term in vitro culture, embryo cryopreservation, and inter–clinic variability in expertise.
Less transfers
Less embryos cryopreserved
No effect on time to pregnancy
Mosaicism is still a possibility and there is no consensus on degree of mosaicism and the best practice. Risk of having false positive results due to mosaicism.
Long-term safety of children born after embryo biopsy still needs further research
Invasive procedure with increased cost
7. Genetics in recurrent pregnancy loss (RPL)
The rate of cytogenetic abnormalities is lower in cases of RPL (30%–50% of losses) compared to up to 70% in sporadic early pregnancy losses
Approximately 50% of all clinically recognized spontaneous miscarriages have a chromosome abnormality. Of these, about 9% have a 45,X constitution, 30% have trisomy, 10% are either triploid or tetraploid, and 2% have a structural rearrangement
Numerical and structural chromosomal abnormalities are important causes of RPL
Balanced translocations or inversions can lead to unbalanced gametes depending on specific recombination and segregation patterns. The attendant reproductive risk depends on the type of rearrangement and its parental origin
Single Gene Disorders: Uncommon e.g. metabolic disorders (typically autosomal recessive with RPL e.g. storage disorders) and hemoglobinopathies (especially alpha thalassemia major)
Couples with recurrent miscarriage (RM) are twice as likely as controls to have single gene defects like hereditary thrombophilias due to Factor V Leiden defect and prothrombin gene (G20210A) mutations, C677T polymorphism in the MHFTR gene which controls DNA methylation associated with
7.1 Who needs testing?
Threshold of >3 losses should be used for epidemiological studies while clinical evaluation to be offered after two consecutive first trimester pregnancy losses
A putative diagnosis should be made and treated in approximately 50% of patients with RPL
Balanced parental chromosome rearrangements are found in 3% to 5% of couples with RPL (5- to 10–fold more common than general population) therefore parental karyotype test is recommended based on genetic history (e.g. previous birth of child with congenital abnormalities, offspring with unbalanced chromosome abnormalities in the family, or detection of a translocation in the pregnancy tissue). This test also provides an idea of likelihood of a subsequent pregnancy loss or healthy live birth which depends on the chromosome involved and the type of rearrangement
Conventional karyotype and fluorescence in situ hybridization (FISH) is not recommended referred currently because of limitations (Karyotype limitation: Failure of tissue culture; FISH: Limited as it only uses probes for certain chromosomes)
Use array comparative genomic hybridization (CGH) test over conventional karyotype
Summary of recommendations
All genetic analysis should be accompanied by expert counseling by a clinical geneticist both in male and female patients
Parental karyotype is carried out after individual assessment of risk
Depending on the clinical findings, the infertile male patient needs genetic evaluation. Karyotype analysis and Y-chromosomal microdeletion screening should be performed in patients with azoospermia or severe oligozoospermia in order to rule out structural chromosomal abnormalities, Klinefelter syndrome, and Y–chromosome microdeletions
Infertile patients with obstructive azoospermia need CFTR gene screening
Patients with HH mutation screening may be performed according to clinical features which suggest hypogonadotropic hypogonadism
Primary amenorrhea should be investigated by karyotype analysis and selected mutation screening according to the patient’s clinical features
Karyotype analysis and FMR1 gene screening is recommended in cases of POF early diagnosis by genetic investigation in turners and POI may instead lead to the advice of early conception or oocyte harvesting and preservation
For women with hypergonadotropic hypogonadism, it is important to consider Turner syndrome, but in those with 46,XX ovarian failure, about 15% of women may have mutations in genes
For eugonadal disorders, test for FSHR mutations in abnormal ovarian response, WNT4 mutations in mullerian aplasia, and estrogen receptor gene (ESR1) mutation in complete estrogen insensitivity syndrome (CEIS)
Karyotype analysis of both partners is recommended in all couples with recurrent implantation failure and RPL
Chromosomal defects explain a high proportion of pregnancy failures
No routine genetic test can be recommended so far in patients with PCOS
Single gene defects which cause infertility are conditions associated with hypogonadotropic hypogonadism e.g. Kallmann syndrome, defective signalling through the kisspeptin
PGT–A is not recommended routinely but may be done in women with advanced maternal age, recurrent pregnancy loss, or recurrent implantation failure
PGT–M is recommended in all patients known for single gene disorders
PGT-SR for abnormal karyotype reduces the miscarriage rate
References
Amato P, Simpson JL. The genetics of polycystic ovary syndrome. Best Practice & Research Clinical Obstetrics & Gynaecology. 2004 Oct 1;18(5):707-18.
Greene AD, Patounakis G, Segars JH. Genetic associations with diminished ovarian reserve: a systematic review of the literature. Journal of assisted reproduction and genetics. 2014 Aug 1;31(8):935-46.
Kara E, Simoni M. Genetic screening for infertility: When should it be done?. Middle East Fertility Society Journal. 2010 Jul 1;15(3):139-45.
Kate UV, Pokale YS, Jadhav AM, Gangane SD. Chromosomal aberrations and polymorphic evaluation in males with primary infertility from Indian population. Journal of clinical and diagnostic research: JCDR. 2014 Oct;8(10):SC01.
Kumar M, Pathak D, Venkatesh S, Kriplani A, Ammini AC, Dada R. Chromosomal abnormalities & oxidative stress in women with premature ovarian failure (POF). The Indian journal of medical research. 2012 Jan;135(1):92.
Safai A, Vasei M, Attaranzadeh A, Azad F, Tabibi N. Chromosomal abnormality in patients with secondary amenorrhea. Archives of Iranian Medicine (AIM). 2012 Apr 1;15(4).
Zegers-Hochschild LF, Adamson D, Dyer S, Racowsky C, de Mouzon J, Sokol R, Rienzi L, Sunde A, Schmidt L, Cooke ID, Simpson JL. The International Glossary on Infertility and Fertility Care: Led by ICMART in Partnership with ASRM, ESHRE, IFFS, March of Dimes, AFS, GIERAF, ASPIRE, MEFS, REDLARA, FIGO. Human Reproduction. 2017;32(Supplement 1):65-.
Zorrilla M, Yatsenko AN. The genetics of infertility: Current status of the field. Current genetic medicine reports. 2013 Dec 1;1(4):247-60.
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CPP | All genetic analysis should be accompanied by expert counselling by a clinical geneticist both in male and female patients. | - | - |
| CPP | Parental karyotype is carried out after individual assessment of risk. | ||
| EBR | Depending on the clinical findings, the infertile male patient needs genetic evaluation. Karyotype analysis and Y–chromosome microdeletion screening should be performed in patients with azoospermia or severe oligozoospermia in order to rule out structural chromosomal abnormalities, Klinefelter syndrome and Y–chromosome microdeletions. | A | I |
| EBR | Infertile patients with obstructive azoospermia need CFTR gene screening. | A | I |
| EBR | Patients with HH mutation screening may be performed according to clinical features which suggest hypogonadotropic hypogonadism. | B | II |
| EBR | Primary amenorrhea should be investigated by karyotype analysis and selected mutation screening according to the patient’s clinical features. | A | I |
| EBR | Karyotype analysis and FMR1 gene screening is recommended in cases of POF. | A | I |
| EBR | Early diagnosis by genetic investigation in Turner and POI may instead lead to the advice of early conception or oocyte harvesting and preservation. | B | II |
| EBR | For women with hypergonadotropic hypogonadism, it is important to consider Turner syndrome, but in those with 46,XX ovarian failure, about 15% of women may have mutations in genes. | C | III |
| CCR | For eugonadal disorders, test for FSHR mutations in abnormal ovarian response, WNT4 mutations in mullerian aplasia, and ESR1 mutation in CEIS. | C | - |
| EBR | Karyotype analysis of both partners is recommended in all couples with RIF and RPL | A | I |
| EBR | Chromosomal defects explain a high proportion of pregnancy failures | A | I |
| EBR | No routine genetic test can be recommended so far in patients with PCOS. | B | III |
| EBR | Single gene defects which cause infertility are conditions associated with hypogonadotropic hypogonadism e.g. Kallmann syndrome, defective signalling through the kisspeptin. | C | IV |
| EBR | PGT–A is not recommended routinely but may be done in women with advanced maternal age, RPL or RIF | B | II |
| EBR | PGT–M is recommended in all patients with known for single gene disorders. | A | I |
| EBR | PGT–SR for abnormal karyotype reduces the miscarriage rate. | A | II |
Chapter 4: Guidelines on Endoscopy in Infertility & ART
OVERVIEW
Indian Society for Assisted Reproduction (ISAR) has dedicated this year towards better practices, better outcomes and keeping that in mind the three organizations ISAR, IFS, & ACE have come together to prepare Minimum Standards of Infertility Practice: A Consensus Statement. This paper provides advice for clinicians regarding role of fertility enhancing endoscopic surgeries in infertility patients.
1. Introduction
30% of infertility cases are due to presence of pelvic factors of infertility
Therapeutic options for infertility in presence of adequate seminal and ovarian functions is reproductive surgery for pelvic factor or invitro fertilization (IVF)
Aim of reproductive surgery in infertility is to optimize the implantation of the blastocyst in the uterine cavity for an optimal outcome
Fertility enhancing endoscopic surgery is a broad spectrum, multifaceted approach which encompasses all minimal access surgery techniques adopted in order to improve the fertility rate of a couple
It primarily involves the use of hysteroscopy and laparoscopy to confirm and treat the causes of female infertility
In a couple with infertility, female infertility contributes to almost 40% cases. These can be attributed to problems from ovarian issues [poly cystic ovary (PCO), cysts–simple, hemorrhagic, dermoid], tubal factors (hydrosalpinx, distal or proximal tubal block, excessively tortuous tube), uterine factors (fibroid, adenomyosis, poor endometrial growth), or infections in genital tract, or pelvic adhesions
A laparoscopy coupled with hysteroscopy can evaluate all these factors as a single procedure
2. Laparoscopy related surgeries
Myomectomy
-
Endometriosis related surgery
-
»Cystectomy, ablation/fulguration of endometriotic spots
-
»
Adhesiolysis
Tubal de–linking
Tubal anastomosis
PCO drilling
3. Hysteroscopy related surgeries
Polypectomy
Hysteroscopic adhesiolysis
Hysteroscopic septal resection and metroplasty
Submucous myoma resection
Lateral metroplasty
4. Combined approach
Diagnostic hysterolaparoscopy with selective chromopertubation
Tubal cannulation
In this guideline, different gynecological conditions and the recommendations for their surgical management in infertility patients will be discussed
5. Guidelines in management of myomas/fibroid uterus
Summary of evidence
Fibroids may or may not impact the fertility potential significantly
-
Accepted indications for removal of fibroids are:
-
»The presence of a submucous fibroid 2–5 cm
-
»Intramural fibroid >4 cm/distorting the cavity or close to the junctional zone
-
»Infertility of >3 years
-
»Prior to ART
-
»Large fibroid altering tubo-ovarian relationship
-
»
-
Relative/optional
-
»Multiple large fibroids (space problem for pregnancy)
-
»Low large cervical fibroid likely to obstruct labour
-
»History of repeated abortions with fibroids of significant size
-
»
Subserosal fibroids do not appear to have an impact on fertility. Submucus fibroid adversely affect reproductive outcome and its removal improves the outcome. There are insufficient high quality studies on the impact of intramural (IM) fibroid or removal of IM fibroid on reproductive outcome. Some studies have shown a negative effect on IVF results, while others have concluded that IM myoma does not affect IVF results. Junctional zone (JZ) IM myomas have unfavourable ART outcomes compared to other IM myoma and myomectomy should be considered for JZ myomas.
Recommendations for assessment of fibroids
| Category | Recommendation | Grade | Quality of Evidence |
|---|---|---|---|
| EBR | Adequately evaluate and classify fibroids in women with infertility, particularly those impinging on the endometrial cavity, using transvaginal ultrasound, hysteroscopy, hysterosonography, or magnetic resonance imaging | A | III |
| EBR | In addition to an assessment of fibroid size and location within the uterine cavity, include evaluation of the degree of invasion of the cavity and thickness of residual myometrium to the serosa as preoperative assessment of submucosal fibroids. A combination of hysteroscopy and transvaginal ultrasound or hysterosonography are the modalities of choice | B | III |
| EBR | A hysterosalpingogram is not an appropriate exam to evaluate and classify fibroids. | D | III |
| CCR | Preoperative assessment of submucosal fibroids is essential to the decision on the best approach for treatment | C | — |
Recommendations for management of fibroids
| Category | Recommendation | Grade | Quality of Evidence |
|---|---|---|---|
| EBR | Submucosal fibroids are managed hysteroscopically. The fibroid size should be <5 cm, although larger fibroids have been managed hysteroscopically, but repeat procedures are often necessary | B | III |
| EBR | In women with otherwise unexplained infertility, submucosal fibroids should be removed in order to improve conception and pregnancy rates | A | II |
| EBR | There is little evidence on the use of Foley catheters, estrogen, or intrauterine devices for the prevention of intrauterine adhesions following hysteroscopic myomectomy | B | III |
| EBR | Removal of subserosal fibroids is not recommended | D | III |
| EBR | There is fair evidence to recommend against myomectomy in women with intramural fibroids (hysteroscopically confirmed intact endometrium) and unexplained infertility, regardless of their size | D | II |
| EBR | If the patient has no other options, the benefits of myomectomy should be weighed against the risks, and management of intramural fibroids should be individualized | C | III |
| EBR | If fibroids are removed abdominally, efforts should be made to use an anterior uterine incision to minimize the formation of postoperative adhesions | A | II |
| EBR | Widespread use of the laparoscopic approach to myomectomy may be limited by the technical difficulty of this procedure. Patient selection should be individualized based on the number, size, and location of uterine fibroids and the skill of the surgeon | A | III |
| CCR | In the infertile population, cumulative pregnancy rates by the laparoscopic and the mini-laparotomy approaches are similar, but the laparoscopic approach is associated with a quicker recovery, less postoperative pain, and less febrile morbidity. (II-2) | B | — |
6. Guidelines in management of endometriosis
The incidence of endometriosis in the reproductive age group is 6%–10%, however, laparoscopic incidence of this condition can be as high as 9%–50%. The stages of endometriosis are enumerated in Figure 1.
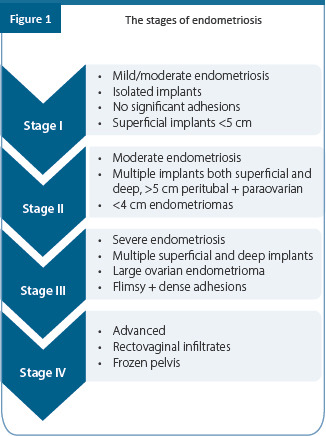
6.1 Diagnosis of endometriosis
Summary of evidence
Endometriosis associated symptoms, include dysmenorrhea, chronic pelvic pain, deep dyspareunia, cyclical intestinal complaints, fatigue/weariness, and infertility. The evidence on the value of clinical examination for the diagnosis of endometriosis is weak. Vaginal examination can facilitate the detection of nodules of the vagina, uterosacral ligaments or pouch of Douglas. Rectovaginal digital examination may allow the detection of endometriosis of rectovaginal septum. Use of transvaginal sonography (TVS), and magnetic resonance imaging (MRI) helps in diagnosing ovarian and deep endometriosis. TVS is useful for both identifying and ruling out rectal endometriosis
Laparoscopy with or without histological verification is widely used to diagnose and rule out the presence of endometriosis. Laparoscopy with histology as a diagnostic intervention is safe and predictive of disease
The evidence concludes that serum CA–125 measurement in the diagnosis of endometriosis grade I/IV is limited, whereas it has some role in the diagnosis of endometriosis grade III/IV
Barium enema, transvaginal sonography, transrectal sonography and MRI should be used to diagnose and know the extent of disease in deep endometriosis
Recommendations for the diagnosis of endometriosis
| Category | Recommendation | Grade | Quality of evidence |
|---|---|---|---|
| CPP | It is recommended that clinicians should consider the diagnosis of endometriosis in the presence of gynecological symptoms such as: dysmenorrhea, non–cyclical pelvic pain, deep dyspareunia, infertility, and fatigue in the presence of any of the above | — | — |
| CPP | It is recommended that clinicians should consider the diagnosis of endometriosis in women of reproductive age with non–gynecological cyclical symptoms (dyschezia, dysuria, hematuria, rectal bleeding, shoulder pain) | — | — |
| CPP | Perform a through clinical examination including per abdominal, per vaginal, per rectal and rectovaginal examination after proper counselling in women with suspected endometriosis | — | — |
| CCR | Suggest diagnosis of deep endometriosis in patients with deep pelvic pain and findings of nodules and/or induration of the rectovaginal wall | C | — |
| CCR | Suspect endometrioma during examination and finding of adnexal mass | C | — |
| CCR | Absence of clinical evidence during examination does not rule out the disease | C | — |
| CCR | A transvaginal USG can exclude or diagnose an ovarian endometrioma typically seen as a simple or complex cyst with internal echoes to solid masses but usually without internal vascularity | A | — |
| CCR | In women with symptoms of endometriosis, TVS is useful to identify rectovaginal involvement | A | — |
| EBR | Laparoscopy remains the gold standard for diagnosis of endometriosis | A | II |
| CCR | CA-125 is poorly sensitive for diagnosis. However, it has a role in treatment follow-up | A | — |
| CPP | One should assess ureter, bladder, and bowel involvement by additional imaging techniques (barium enema, transvaginal sonography, transrectal sonography, and MRI) if there is a clinical suspicion of deep endometriosis based on history or physical examination | — | — |
6.2 Treatment guidelines
Surgical management for endometriosis associated pain
Laparotomy and laparoscopy (excision/ablation) are equally effective in the treatment of endometriosis-associated pain. Laparoscopy may be a better option compared to laparotomy as it is associated with less pain, shorter hospital stay and quicker recovery. Both ablation and excision of peritoneal disease are equally effective for treatment of endometriosis-associated pain
Laparoscopic uterosacral nerve ablation (LUNA) does not offer any beneficial effect compared to ablation or excision in endometriosis associated pain. Presacral neurectomy (PSN) may be beneficial in reducing pain but associated with increased risk of adverse effects such as bleeding, constipation, and urinary urgency
Cystectomy is superior to drainage and coagulation or CO2 laser vaporization of ovarian endometrioma (≥ 3 cm) with regard to the recurrence of endometriosis–associated pain and the recurrence of endometrioma. Surgery for deep endometriosis is effective in reducing pain but is associated with substantial intraoperative and postoperative complications
Recommendation for surgical treatment in endometriosis–associated pain
| Category | Recommendation | Grade | Quality of Evidence |
|---|---|---|---|
| CCR | Endometriosis identified at laparoscopy, should be surgically treated to reduce endometriosis–associated pain Laparoscopic approach is better than laparotomy for both diagnosis and treatment | A | -- |
| CCR | Both ablation and excision are effective in reducing endometriosis pain in women with peritoneal endometriosis pain Fulguration of cyst wall should be avoided in cases with poor ovarian reserve | C | - |
| EBR | Laparoscopic uterosacral nerve ablation (LUNA) should not be performed to reduce endometriosis–associated pain | A | III |
| CCR | Presacral neurectomy (PSN) though effective in reducing endometriosis–associated midline pain, requires a high degree of skill and is associated with potentially hazardous complications | A | - |
| CCR | Cystectomy is better than drainage and coagulation or as it reduces endometriosis–associated pain and decreases recurrence rate of the endometrioma | A | - |
| CCR | Surgical removal of deep endometriosis, reduces endometriosis–associated pain, and improves quality of life | B | - |
| EBR | Preoperative hormonal therapy does not improve operative outcome | A | II |
| EBR | Postoperative hormonal treatment does not improve the outcome of surgery for pain and should be avoided | A | II |
| EBR | Postoperative use of a levonorgestrel–releasing intrauterine system (LNG-IUS) or a combined hormonal contraceptive for at least 18–24 months, should be used for the secondary prevention of endometriosis–associated dysmenorrhea | A | III |
| CPP | Avoid repeated surgery in these patients as this can reduce ovarian reserve | - | - |
6.3 Management of infertility in women with endometriosis
Summary of evidence
The pregnancy rate (PR) is reduced to halve in women with endometriosis undergoing ART treatment. Detrimental effect of endometriosis was seen on implantation and PRs. Moreover one needs to balance the beneficial and harmful effects of surgery for endometriosis on the reproductive outcomes of ART
In stage I and II endometriosis operative laparoscopy is more effective than diagnostic laparoscopy in improving ongoing pregnancy rates. Ovarian endometriosis ablation, cyst wall cauterization, and vaporization with CO2 laser decrease anti-Müllerian hormone (AMH) and antral follicle count (AFC)
Place for surgery for DE before ART is only if there is no pregnancy after three IVF-intracytoplasmic Sperm Injection (ICSI), whereas in women >35 years, removal of DE might be proposed after failure of 2 IVF–ICSI cycles
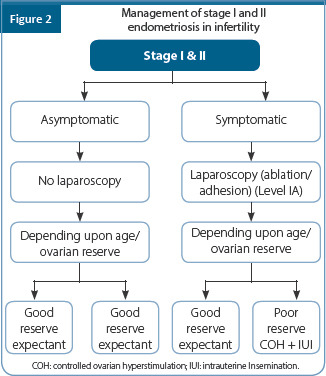
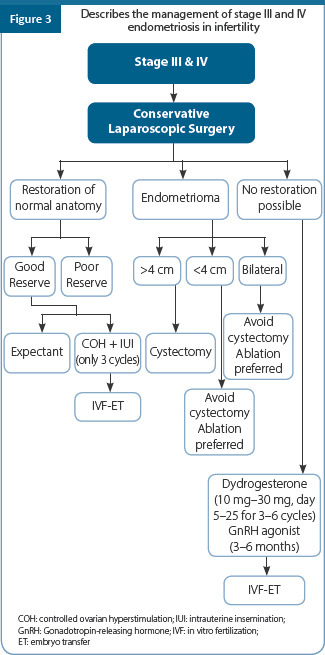

Recommendations for management of infertility in women with endometriosis
| Category | Recommendation | Grade | Quality of evidence |
|---|---|---|---|
| EBR | In infertile women with AFS/ASRM stage I/II endometriosis, operative laparoscopic viz excision or ablation of the endometriosis lesions and adhesiolysis, rather should be performed to increase ongoing pregnancy rates | A | II |
| EBR | In infertile women with endometrioma larger than 3 cm, there is no evidence that cystectomy prior to treatment with ART to improves PRs | A | II |
| EBR | In stage III/ IV: Operative laparoscopy instead of expectant management increases chances of spontaneous pregnancy | A | III |
| CPP | In women with endometrioma larger than 3 cm, clinicians should consider cystectomy prior to ART only to improve endometriosis–associated pain or the accessibility of follicles | — | — |
| CPP | Counselling of women with endometrioma regarding the risks of reduced ovarian function after surgery and the possible loss of ovary is essential. The decision to proceed with surgery should be considered carefully if the woman has had previous ovarian surgery | — | — |
| CCR | The effectiveness of surgical excision of deep nodular lesions before treatment with ART in women DE is not well established with regard to reproductive outcome | C | — |
| CPP | ART should be recommended in presence of tubal dysfunction or in presence of male factor or if other management options fail | B | — |
| CPP | Recurrence rate of endometriosis is not increased with controlled ovarian stimulation | — | — |
*AFS: American Fertility Society (AFS); ASRM: American Society for Reproductive Medicine.
7. Guidelines in the management of adenomyosis
Summary of evidence
Prevalence ranges from 8% to 27% and in endometriosis the prevalence is about 54%. Adenomyosis could be either diffuse or focal and may not affect implantation, but may be associated with pelvic pain, infertility, and early pregnancy loss. Adenomyosis can be diagnosed by 2D and 3D USG, MRI, histopathology, and at hysteroscopy
In adenomyosis detection of junctional zone (JZ) involvement is very important as JZ has emerged as a hormone–dependent structure that governs uterine peristalsis outside pregnancy. Adenomyosis is associated with lower clinical and ongoing pregnancy rates and higher miscarriage rate. Medical management includes COC’s, gonadotropin-releasing hormone (GnRH) agonists, Progestins, [medroxyprogesterone acetate (MPA), dienogest, danazol, levonorgestrel intrauterine system (LNG-IUS)], selective progesterone receptor modulators (SPRM), and selective estrogen receptor modulators (SERM) which may avoid surgery but is not very effective in relief of pain. The chance of conception remains low in these cases
Surgical management
Summary of evidence
The conservative surgical techniques involved excision of the adenomyotic tissue or adenomyoma and hysteroplasty either laparoscopically or via laparotomy. Conservative surgery can result in the reduction in myometrial capacity with higher incidence of abortion, premature labour, uterine rupture, and caesarean section. There is no fixed duration for which the patient needs be given contraception after surgery but is beneficial to be given for 6 months
-
In women with adenomyosis planning to undergo IVF treatment, the following management strategies should be considered
- GnRH analogue therapy for 2–6 months before IVF
- Long GnRH analogue protocol rather than GnRH antagonist should be considered as it helps to induce decidualization of the adenomyotic
- Two–Staged IVF could be considered. Patients can undergo ovarian stimulation, oocyte retrieval, and fertilization and embryo freezing followed by frozen–thawed embryo transfer (FET) at a later stage. Prior to the FET, GnRH analogue suppression therapy for 3 months leads to the shrinkage of adenomyosis
- Single embryo transfer to prevent multiple pregnancies is preferred in adenomyosis as it has been associated with increased incidence of preterm delivery, preeclampsia, and second trimester miscarriage when compared with the control group
Moreover, in women who have undergone adenomyomectomy prior to IVF should have single embryo transfer (SET) to avoid multiple pregnancy with a view to minimize the risk of scar rupture.
Recommendations for surgical management of adenomyosis
| Category | Recommendation | Grade | Quality of evidence |
|---|---|---|---|
| CPP | Focal adenomyosis can be treated by laparoscopy. However, for diffuse adenomyosis laparotomy is preferred as the junction of normal and abnormal tissue is better delineated by palpation | — | — |
| CPP | Laparoscopic adenomyomectomy results in incompletely repaired muscle defects, compared with laparotomy surgery. Thus, the risk of uterine rupture is believed to increase during subsequent pregnancies following laparoscopic procedures | — | — |
| CPP | Energy sources can cause extensive tissue denaturation, making the tissue hard and difficult to heal after repair | — | — |
| CPP | Women after surgery for adenomyosis should be advised contraception for 6 months | — | — |
8. Laparoscopy in PCOS
8.1 Laparoscopic ovarian drilling
Summary of evidence
Laparoscopic ovarian drilling is as effective and safe as gonadotrophin therapy with less incidence of multiple pregnancy, ovarian hyperstimulation syndrome (OHSS). It is indicated in women who hypersecrete luteinizing hormone (LH), either in natural cycles or in response to clomiphene citrate (CC), anovulatory women with polycystic ovary syndrome (PCOS) who need laparoscopic assessment of their pelvis and in those women it is not possible to monitor a gonadotropin treatment cycle. Laparoscopic ovarian drilling not recommended for prevention of hyperresponsiveness to exogenous gonadotropins or management of menstrual irregularity or hyperandrogenism
-
Poor reproductive outcome after laparoscopic ovarian drilling seen in women who are
-
»Obese (body mass index >25 kg/m2)
-
»Longer duration of infertility (>3 years)
-
»Low basal LH levels (<10 IU/L)
-
»Marked biochemical hyperandrogenism (testosterone levels ≥4.5 nmol/L, free androgen index >15)
-
»High basal anti-mullerian hormone (AMH) (≥7.7 ng/ml)
-
»
Recommendation for laparoscopic ovarian drilling in PCOS
| Category | Recommendation | Grade | Quality of evidence |
|---|---|---|---|
| EBR | Laparoscopic ovarian surgery could be second line therapy for women with polycystic ovary syndrome (PCOS), who are clomiphene citrate resistant, with anovulatory infertility and no other infertility factors | C | III |
| CCR | Laparoscopic ovarian surgery could potentially be offered as first line treatment if laparoscopy is indicated for another reason in women with PCOS with anovulatory infertility and no other infertility factors | C | — |
| CPP | Risks of laparoscopic ovarian drilling need to be explained where laparoscopic ovarian surgery is to be recommended, the following need to be considered: • Comparative cost with gonadotropins expertise required for use in ovulation induction • Intraoperative and postoperative risks are higher in women who are overweight and obese • There may be a small associated risk of lower ovarian reserve or loss of ovarian function • Periadnexal adhesion formation may be an associated risk |
— | — |
9. Bariatric surgery in PCOS
Summary of evidence
There is a direct causal relationship between PCOS, visceral obesity and metabolic syndrome.1 It is not a fertility treatment for inducing ovulation but can correct menstrual irregularities, result in hormone normalization and improved reproductive function with reduced need for fertility treatment post bariatric surgery has been noted. Pregnancy should be avoided for 12 months post surgery
Further methodologically rigorous trials are important to address the efficacy, safety and role of bariatric surgery in PCOS, which includes improving fertility
Recommendations for bariatric surgery in PCOS
| Category | Recommendation | Grade | Quality of evidence |
|---|---|---|---|
| CCR | Bariatric surgery should be considered as an experimental therapy in women with polycystic ovary syndrome (PCOS), for the purpose of having a healthy baby, with risk to benefit ratios currently too uncertain to advocate this as fertility therapy | C | - |
| CCR | Bariatric surgery could be considered as a second line therapy to improve fertility outcomes in adult women with PCOS who are anovulatory, have a body mass index ≥35 kg/m2, and who remain infertile despite undertaking an intensive (frequent multidisciplinary contact) structured lifestyle management program involving reducing dietary energy (caloric) intake, exercise, behavioural and/or drug interventions for a minimum of 6 months | C | - |
| CPP | If bariatric surgery is to be prescribed, the following need to be considered: • Comparative cost • The need for a structured weight management program involving diet, physical activity, and interventions to improve psychological, musculoskeletal, and cardiovascular health to continue postoperatively • Perinatal risks such as small for gestational age, premature delivery, possibly increased infant mortality • Potential benefits such as reduced incidence of large for gestational age fetus and gestational diabetes • Recommendations for pregnancy avoidance during periods of rapid weight loss and for at least 12 months after bariatric surgery with appropriate contraception • If pregnancy occurs, the following need to be considered: » Awareness and preventative management of preoperative and postoperative nutritional deficiencies is important, ideally in a specialist interdisciplinary care setting » Monitoring of fetal growth during pregnancy |
- | - |
10. Laparoscopic ovarian surgery for dermoid and simple cyst
Summary of evidence
When surgery is required for any type of ovarian cysts, it should be conservative and excision is preferred than ovariectomy. Moreover, laparoscopy is the preferred mode with the use of bipolar rather than monopolar cautery when required. Coagulation of the cyst walls should be avoided
Needle aspiration of a dermoid cyst must not be considered, owing to the risk of chemical peritonitis, and for this reason only excision is appropriate. No evidence also to support the utility of fine–needle aspiration of a unilocular cyst. These cysts should be treated by either surveillance or excision, depending on their size
Recommendations for laparoscopic ovarian surgery for dermoid and simple cyst
| Category | Recommendation | Grade | Quality of Evidence |
|---|---|---|---|
| CPP | Imaging techniques which include 2D and 3D ultrasound should be used for assessment of ovarian cyst to decide between expectant and surgical management | — | — |
| CPP | Expectant management should be followed in moderate sized dermoid cysts (4–6 cm) which are asymptomatic | — | — |
| CPP | When surgery is required for any type of ovarian cysts, it should be conservative and excision is preferred than ovariectomy | — | — |
| CPP | Laparoscopy is the preferred mode with the use of bipolar rather than monopolar cautery Coagulation of the cyst walls should be avoided | — | — |
| CPP | No evidence for needle aspiration of either a dermoid or simple cyst | — | — |
11. Tubal surgery
Summary of evidence
Tubal surgery is done for hydrosalpinx, proximal tubal obstruction, sterilization reversal, and adhesiolysis. One could perform either salpingectomy, salpingostomy, proximal tubal occlusion/ligation or aspiration of fluid from hydrosalpinx to treat hydrosalpinx before IVF. It is best to avoid tubal surgery and opt for IVF as a treatment modality if patients is >37 years, presence of decreased ovarian reserve, abnormal tubal mucosa, and lack of in training in tubal surgery
Reconstructive tubal surgery for hydrosalpinx can still be considered for selected women younger than 35 years, with mild tubal disease and no other co- existing infertility factors, and for those who cannot or refuse to undergo IVF treatment. In the presence of hydrosalpinx, the pregnancy rate was higher in the salpingectomy group, thus there is a definite beneficial effects of pre-IVF salpingectomy. Salpingectomy could be challenging, especially in the presence of dense periadnexal adhesions. Moreover, salpingectomy could also affect the ovarian blood flow and reduces the ovarian response during consequent IVF cycles
Proximal tubal occlusion with electrocoagulation or with clips is another option of treatment but the concern with method is that it may lead to an increased size of hydrosalpinx, as the fluid can no longer drain through the uterus. For this reason, consideration may be given to widely fenestrating the hydrosalpinges at the time of proximal occlusion
Laparoscopic sterilization reversal required shorter hospitalization compared to laparotomic reversal and was less expensive compared to robotic reversal. One must remember that for older women IVF could be a more cost effective than reversal of sterilization
-
Tubal anastomosis should not be considered when
-
»Final tubal length is less than 4 cm
-
»There are significant tubo–ovarian adhesions with mucosal damage
-
»In presence of stage 3–4 endometriosis
-
»Presence of male factor
-
»
Pelvic adhesions could be due to post pelvic infection, endometriosis and postsurgery. Salpingo–ovariolysis could be an option in the presence of tubal adhesions and the success of tubal surgery depends on extent of tubal damage, tubal wall thickness, distal ampullary diameter, health of distal tubal endothelium, extent and type of adhesions, and experience of the surgeon
Recommendations for tubal surgery in infertility
| Category | Recommendation | Grade | Quality of Evidence |
|---|---|---|---|
| CPP | Assessment for tubal surgery • The patient’s age and declining fertility should be considered when advising a patient to undergo tubal assessment or corrective surgery • Couples should be screened to exclude ovulatory disorders and semen abnormalities as these factors may preselect a couple for IVF treatment • With a known history of pelvic inflammatory disease, pelvic surgery, ectopic pregnancy or endometriosis, laparoscopy and dye studies is preferred for pelvic assessment in preference to hysterosalpingography or hysterocontrastsonography (HyCoSy). A finding of proximal tubal obstruction by hysterosalpingography necessitates confirmation by either fluoroscopic or hysteroscopic selective tubal catheterisation • Practitioners should have the necessary skills for and be prepared to undertake interventional procedures as part of a diagnostic laparoscopy procedure and the patient consented appropriately • Laparoscopic staging of tubal pathology as to site, type and extent of disease process particularly in relation to hydrosalpinx is important for prognosis and deciding to have tubal surgery or IVF |
— | — |
| EBR | Open microsurgery and laparoscopic tubal surgery • There is insufficient evidence to recommend one particular approach to surgery. The technique adopted should be determined by the skill of the surgeon and the available equipment |
C | III |
| EBR | Proximal tubal disease | ||
| • When available, selective salpingography and tubal catheterization or hysteroscopic tubal cannulation should be considered as they are less invasive treatment options with proven pregnancy results | C | III | |
| • Tubocornual anastomosis should only be attempted by surgeons trained in microsurgical techniques and with the appropriate equipment. Alternatively, IVF should be considered | C | III | |
| CCR | Distal tubal occlusion • Consider salpingoneostomy for <3 cm diameter thin walled hydrosalpinges free of adhesions which gives best results compared to fallopian tubes with both external and internal pathology • Intraoperative or preoperative salpingoscopy enabling direct endoscopic evaluation of tubal mucosa may facilitate a decision to perform conservative salpingoneostomy or on the basis of extensive tubal pathology salpingectomy in preparation for IVF • There was no improvement in pregnancy rate with use of postoperative hydrotubation with antibiotics and steroids or by carrying out second look laparoscopy and adhesiolysis • Commencing IVF concomitantly or after this period of time seems a sensible progressive step |
C | — |
| EBR | Hydrosalpinx and IVF • Consider salpingectomy for women with hydrosalpinges prior to IVF treatment. This should be undertaken laparoscopically with great care taken not to interfere with ovarian blood supply via the infundibulopelvic fold |
A | II |
| EBR | Reversal of sterilization • Surgical reversal of sterilization offers a high chance of tubal patency and fertility and should be offered to women wishing to conceive after Filshie or Hulka clip and Falope |
||
| ring sterilization | B | II | |
| • Request for renewed fertility arises because of a new partner, improved economic circumstances or more rarely death of a child | |||
| • To enable couples to reach a decision regarding IVF or reversal, data on cumulative live birth rates after invitro fertilization should be presented | |||
| • The main factors influencing successful reanastomosis are the site of anastomosis, length of residual fallopian tube, and surgical technique. | |||
| • For the most commonly encountered Filshie or Hulka clip and Falope ring sterilization microsurgery offers a high chance of tubal patency and fertility | |||
| • The live birth rate in patients aged over 40 following reanastomosis suggest that conception may occur more readily with natural ovulatory cycles than in stimulated cycles | |||
| • The reversal procedure can be performed via a 3–5 cm suprapubic incision and uterine manipulation enabling patients to be discharged the same day or following an overnight hospital stay • In younger women, particularly when they wish to consider having only one child in a new relationship, IVF may be a more realistic option because sterilization will continue to provide contraception following a successful birth |
|||
| CCR | Tubal adhesions • Surgical correction of peritubular adhesions, preferably with minimal access techniques is recommended when the adhesions are American Fertility Society (AFS) stage I and II and in the absence of distal tubal occlusion |
C | - |
| CPP | Adhesion prevention • Careful tissue handling is essential in reproductive surgery, however, adjuvant therapies do not improve the chance of pregnancy • Teaching and maintenance of preventative surgical technique for laparotomy and laparoscopic surgery are pivotal in reducing postoperative surgical adhesions • These techniques encompass gentle tissue handling, meticulous haemostasis, minimising ischemia and tissue dryness, use of nonreactive sutures, and prevention of infection • Successful adhesion preventive measures in the experimental animal including the use of hypothermia and insufflation with 3% oxygen should be considered for routine use following confirmation of usefulness in clinical studies • Whilst effective in reducing adhesion, there is no evidence from published studies that surgical barriers influence fertility, pain, and incidence of postoperative adhesions |
_ | _ |
12. Hysteroscopy in infertility and ART
12.1 Routine hysteroscopy in all infertility patients, before IVF or RIF
Summary of evidence
Hysteroscopy is a gold standard technique for uterine factor evaluation since it enables direct visualization of the uterine cavity and its relevant pathological disorders as well as the treatment of any detected abnormality. It has been shown to have no role in routine evaluation of infertility. There was also no impact on the pregnancy rates in women undergoing intrauterine insemination (IUI)
There is also no evidence for routine hysteroscopy before first ever IVF. It is done early in the presence of an abnormal hysterosalpingogram (HSG) or history or symptoms suggestive of endometrial or uterine pathology. Routine hysteroscopy does not improve live birth rates (LBRs) in infertile women with a normal TVS of the uterine cavity scheduled for a first IVF treatment. Therefore, women with a normal transvaginal ultrasound should not be offered routine hysteroscopy. The TROPHY trial concluded that outpatient hysteroscopy before IVF in women with a normal ultrasound of the uterine cavity and a history of unsuccessful IVF treatment cycles does not improve the livebirth rate. Moderate quality evidence indicates that endometrial injury performed between day 7 of the previous cycle and day 7 of the embryo transfer (ET) cycle is associated with an improvement in LBR and CPR in women with more than two previous failed ETs. When confounding factors like age and number of failed IVF cycles were removed, there was no statistical difference in the LBR and miscarriage rate. Thus, the two recent meta–analysis concluded that endometrial injury should be used restrictively and not as a routine procedure
Recommendations for use of routine hysteroscopy before first IVF or RIF
| Number | Category | Recommendation | Grade | Quality of Evidence |
|---|---|---|---|---|
| 8.1.1 | CRR | No role of routine hysteroscopy prior to IUI as it does not have any impact on pregnancy rates | B | — |
| 8.1.2 | EBR | Hysteroscopy before (first or subsequent) IVF/ICSI attempt in infertile women without intrauterine abnormalities does not improve LBR and therefore should not performed | A | II |
IUI: intrauterine insemination; IVF: in vitro fertilization; ICS: intracytoplasmic sperm injection;
12.2 Operative hysteroscopy
Summary of evidence
Hysteroscopic diagnosis and treatment of intrauterine abnormalities may improve pregnancy rates after ART, at least when compared with controls not receiving hysteroscopy but the quality of evidence is low
Endometritis can cause delayed endometrial maturation, leading to asynchrony with implantation, which can result in RIF and RPL. Endometritis can easily be identified at hysteroscopy and once identified it can effectively be treated with a course of doxycycline and normal fertility restored
Intrauterine synechiae can be a source of abnormal placentation, recurrent miscarriage, and preterm labour. PRs can be improved and miscarriage rates decreased with hysteroscopic adhesiolysis. Postoperative estrogen followed by progesterone and second–look hysteroscopy with adhesiolysis have all been used for treatment of recurrent synechiae after initial adhesiolysis. Intrauterine balloon application after operative hysteroscopy is of great value in preventing intrauterine adhesions. Mechanical agent like intrauterine device may not be helpful in prevention of postop adhesions
Auto–cross linked hyaluronic acid gel (ACP) significantly reduces the development of intrauterine adhesions postoperatively and its use is likely to be associated with reduction in severe adhesion. Intercoat gel has also been tried and it has shown to prevent de novo formation of IUAs and to improve the patency of the internal uterine ostium at follow–up hysteroscopy
-
Poor prognostic indicators for surgery in women with IUA include:
-
»Adhesions obliterating both ostia
-
»Age >35 years
-
»Amenorrhea/oligomenorrhea
-
»Abnormal ultrasound appearance
-
»Reformation of adhesions at second look
-
»
Recommendations for operative hysteroscopy in infertility
| Category | Recommendation | Grade | Quality of evidence |
|---|---|---|---|
| CCR | Intrauterine abnormalities can be diagnosed by 2D and 3D ultrasound, saline infusion sonogram (SIS), and HSG | B | — |
| CCR | MRI should not be routinely advised for diagnosis of intrauterine abnormalities | C | — |
| EBR | Operative hysteroscopy in infertile women improves clinical pregnancy rate in women diagnosed with intracavitary abnormalities (i.e. endometrial polyps and submucous fibroids) detected at US, HSG or SIS/gel instillation sonography (GIS) | A | III |
| CPP | Asymptomatic polyps in non–infertile women, less than 10 mm in size and at low risk of malignancy may be followed up without surgery. Polyps larger than 10 mm are unlikely to regress spontaneously. All symptomatic polyps require removal | — | — |
| CPP | Direct removal of polyps either by resection or hysteroscopic scissors is reported to reduce recurrence rate compared to visualising the polyp followed by removal by a polyp grasping forceps or curettage | — | — |
| CCR | Diagnosis and treatment of endometritis and adenomyosis at hysteroscopy allows treatment with improvement in the clinical pregnancy rate (CPR) and LBR | B | — |
| CCR | PRs can be improved and miscarriage rates decreased with hysteroscopic adhesiolysis in mild–to–moderate intrauterine adhesions | B | — |
| CCR | There is no role of blind cervical probing or blind curettage in these patients | C | — |
| CCR | The use of concomitant modalities like ultrasound and laparoscopy does not provide additional benefit. However, in expert hands and in properly selected patients, these may marginally reduce the complication (e.g. perforation) rate | B | — |
| CCR | PRs and LBRs do not improve much after hysteroscopic adhesiolysis of severe intrauterine adhesions | C | — |
| CCR | Postoperative estrogen followed by progesterone, balloon therapy, and second–look hysteroscopy with adhesiolysis may prevent recurrent synechiae formation after initial adhesiolysis | C | — |
| CCR | Adhesion barriers used post procedure is known to have short–term benefit. However, long–term benefit on overall fertility rate remains questionable | A | — |
| CCR | Role of preoperative, intraoperative or postoperative antibiotics has no proven benefit | C | — |
| CCR | Intrauterine devices (IUD) are not recommended. | C | — |
| CCR | Newer adhesive barriers like hyaluronic acid and auto-cross-linked hyaluronic acid gel reduce adhesion reformation Their efficacy in terms of post–treatment pregnancy rate is unknown | A | — |
| CCR | Use of stem cell therapy as an adjunctive treatment has limited evidence and should not be applied outside research settings | C | — |
| CCR | Relook hysteroscopy is advocated to assessment of uterine cavity after adhesiolysis | B | — |
12.3 Mullerian duct abnormalities
Summary of evidence
Septate uterus is associated with higher first-trimester abortion, pre re-look hysteroscopy term delivery and lower term births. Earlier surgery was recommended when sub-septation was 10 mm, but the new cut off for correction of septate uterus is 5.9 mm. Hysteroscopic septal resection reduces the incidence of first-trimester abortions, pre–term deliveries and increases the live birth rate, and also improves post IVF pregnancy rates
Management of patients with a T–shaped uterus is controversial and the beneficial effect of hysteroscopic metroplasty is questionable with no prospective studies or RCTs
One must remember that lateral metroplast may be associated with cervical incompetence, hysteroscopic endometritis in 1% to 5% of cases, destruction of normal endometrium due to use of monopolar cautery, and development of intrauterine adhesions. Uterine perforation at surgery and increased incidence of uterine rupture during pregnancy, increased risk of miscarriage (22%) and premature delivery (20%) adherent placenta, and cesarean section is also noted
Lateral metroplasty may be performed only in cases of repeated miscarriages, longstanding and unexplained infertility unrelated to the uterine anomaly, or following failed ART
Recommendations for surgery in mullerian duct abnormalities
| Category | Recommendation | Grade | Quality of Evidence |
|---|---|---|---|
| CCR | Hysteroscopic septal resection reduces the incidence of first trimester abortions, pre–term deliveries, and increases the live birth rate. | B | — |
| CCR | Earlier correction of uterine sub–septations was done when it was longer than 10 mm New cut off for correction of septate uterus is 5.9 mm | B | — |
| CPP | In a patient with no history of infertility or prior pregnancy loss, it may be reasonable to consider septum incision after counselling about the potential risks and benefits of the procedure | — | — |
| CPP | Performing enlargement metroplasty by making incisions on the lateral myometrial walls to a depth of 5 mm to 7 mm appears to improve the obstetrical prognosis only in cases of repeated miscarriages, longstanding and unexplained infertility, and should not be done in all cases | — | — |
| CCR | Arcuate uterus have no adverse impact on early pregnancy and therefore hysteroscopic resection is not necessary | B | — |
Summary of recommendations
Infertile women undergoing IUI, there is no evidence of a treatment effect of laparoscopy prior to IUI for the ongoing pregnancy rate per patient (compared to immediate treatment with IUI)
-
Reproductive surgery may be complimentary before IVF to enhance its success and not all surgeries can improve IVF outcome. Surgeries that may help are:
-
»Adhesiolysis so that the ovary can be accessed by TVS
-
»Removal of large endometriomas, which preclude access to follicular aspiration
-
»Hydrosalpinx
-
»
-
Reproductive surgery indicated beyond a reasonable doubt
-
»Adhesions around the fallopian tube, ovaries or the ampulla (Level B-C)
-
»Intramural myomas >5 cm and those close to the junctional zone (Level B)
-
»Hydrosalpinx (Level A)
-
»Tubectomy reversal. (Level B-C)
-
»Hysteroscopic surgery for polyps, submucous myoma (Level A)
-
»IUA and metroplasty (Level B-C)
-
»
-
Reproductive surgery having contradictory evidence
-
»In PCOS–laparoscopic ovarian drilling is second–line treatment for OI in PCOS
-
»Endometriosis and endometrioma or recurrent endometrioma
-
»Deep rectovaginal endometriosis without pain
-
»Adenomyosis
-
»Severe tubal disease or occlusion due to disease
-
»Routine laparoscopy, hysteroscopy
-
»Endometrial scratch
-
»
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| EBR | Infertile women undergoing IUI, there is no evidence of a treatment effect of laparoscopy before IUI for the ongoing pregnancy rate per patient (compared to immediate treatment with IUI) | B | III |
| EBR | Reproductive surgery may be complimentary before IVF to enhance its success and not all surgeries can improve IVF outcome. Surgeries that may help are: | B | III |
| EBR | • Adhesiolysis so that the ovary can be accessed by TVS | B | II |
| EBR | • Removal of large endometriomas, which preclude access to follicular aspiration | C | IV |
| EBR | • Hydrosalpinx | A | I |
| EBR | Reproductive surgery indicated beyond a reasonable doubt | A | I-III |
| EBR | • Adhesions around the fallopian tube, ovaries or the ampulla | B | III |
| EBR | • Intramural myomas >5 cm and those close to the junctional zone | B | II |
| EBR | • Hydrosalpinx | A | I |
| EBR | • Tubectomy reversal. | B | III |
| EBR | • Hysteroscopic surgery for polyps, submucous myoma | A | I |
| EBR | • IUA and metroplasty | B | III |
| EBR | Reproductive surgery having contradictory evidence | ||
| EBR | • In PCOS–laparoscopic ovarian drilling is second–line treatment for OI in PCOS | B | II |
| EBR | • Endometriosis and endometrioma or recurrent endometrioma | B | III |
| EBR | • Deep rectovaginal endometriosis without pain | C | IV |
| CCR | • Adenomyosis | C | IV |
| EBR | • Severe tubal disease or occlusion due to disease | C | III |
| EBR | • Routine laparoscopy, hysteroscopy | A | I |
| EBR | • Endometrial scratch | A | I |
References
Hart R, Khalaf Y, Yeong CT, Seed P, Taylor A, Braude P. A prospective controlled study of the effect of intramural uterine fibroids on the outcome of assisted conception. Human reproduction. 2001 Nov 1;16(11):2411-7.
Khalaf Y, Ross C, El-Toukhy T, Hart R, Seed P, Braude P. The effect of small intramural uterine fibroids on the cumulative outcome of assisted conception. Human Reproduction. 2006 Oct 1;21(10):2640-4.
Oliveira FG, Abdelmassih VG, Diamond MP, Dozortsev D, Melo NR, Abdelmassih R. Impact of subserosal and intramural uterine fibroids that do not distort the endometrial cavity on the outcome of in vitro fertilization–intracytoplasmic sperm injection. Fertility and sterility. 2004 Mar 1;81(3):582-7.
Sunkara SK, Khairy M, El-Toukhy T, Khalaf Y, Coomarasamy A. The effect of intramural fibroids without uterine cavity involvement on the outcome of IVF treatment: a systematic review and meta-analysis. Human Reproduction. 2009 Nov 12;25(2):418-29.
Horne A.W., Critchley H.O. The effect of uterine fibroids on embryo implantation // Sem. Reprod. Med. — 2007. — Vol. 25, ? 6. —P. 483—490.
Bazot M, Lafont C, Rouzier R, Roseau G, Thomassin-Naggara I and Daraï E. Diagnostic accuracy of physical examination, transvaginal sonography, rectal endoscopic sonography, and magnetic resonance imaging to diagnose deep infiltrating endometriosis. Fertil Steril 2009; 92:1825–1833.
Eskenazi B, Warner M, Bonsignore L, Olive D, Samuels S and Vercellini P. Validation study of nonsurgical diagnosis of endometriosis. Fertil Steril 2001; 76:929–935.
Hudelist G, Ballard K, English J, Wright J, Banerjee S, Mastoroudes H, Thomas A, Singer CF and Keckstein J. Transvaginal sonography vs. clinical examination in the preoperative diagnosis of deep infiltrating endometriosis. Ultrasound Obstet Gynecol 2011; 37:480–487.
Abrao MS, Goncalves MO, Dias JA, Jr., Podgaec S, Chamie LP and Blasbalg R. Comparison between clinical examination, transvaginal sonography and magnetic resonance imaging for the diagnosis of deep endometriosis. Hum Reprod 2007; 22:3092–3097.
Bazot M, Bornier C, Dubernard G, Roseau G, Cortez A and Darai E. Accuracy of magnetic resonance imaging and rectal endoscopic sonography for the prediction of location of deep pelvic endometriosis. Hum Reprod 2007; 22:1457–1463.
Bergamini V, Ghezzi F, Scarperi S, Raffaelli R, Cromi A and Franchi M. Preoperative assessment of intestinal endometriosis: A comparison of transvaginal sonography with water-contrast in the rectum, transrectal sonography, and barium enema. Abdom imaging 2010; 35:732–736.
Jacobson TZ, Duffy JM, Barlow D, Koninckx PR and Garry R. Laparoscopic surgery for pelvic pain associated with endometriosis. Cochrane Database Syst Rev 2009:CD001300.
Healey M, Ang WC and Cheng C. Surgical treatment of endometriosis: a prospective randomized double- blinded trial comparing excision and ablation. Fertil Steril 2010; 94:2536–2540.
Carmona F, Martínez-Zamora MA, Rabanal A, Martínez-Román S and Balasch J. Ovarian cystectomy versus laser vaporization in the treatment of ovarian endometriomas: a randomized clinical trial with a five-year follow-up. Fertil Steril 2011; 96:251–254.
Hart RJ, Hickey M, Maouris P and Buckett W. Excisional surgery versus ablative surgery for ovarian endometriomata. Cochrane Database Syst Rev 2008:CD004992.
Daraï E, Lesieur B, Dubernard G, Rouzier R, Bazot M and Ballester M. Fertility after colorectal resection for endometriosis: results of a prospective study comparing laparoscopy with open surgery. Fertil Steril 2011; 95:1903–1908.
Kondo W, Bourdel N, Tamburro S, Cavoli D, Jardon K, Rabischong B, Botchorishvili R, Pouly J, Mage G and Canis M. Complications after surgery for deeply infiltrating pelvic endometriosis. BJOG 2011; 118:292–298.
Harb HM, Gallos ID, Chu J, Harb M, Coomarasamy A. The effect of endometriosis on in vitro fertilisation outcome: a systematic review and meta-analysis. BJOG: An International Journal of Obstetrics & Gynaecology. 2013 Oct;120(11):1308-20.
Jacobson TZ, Duffy JM, Barlow D, Farquhar C, Koninckx PR and Olive D. Laparoscopic surgery for subfertility associated with endometriosis. Cochrane Database Syst Rev 2010:CD001398.
Asgari Z, Rouholamin S, Hosseini R, Sepidarkish M, Hafizi L, et al. (2015) Comparing ovarian reserve after laparoscopic excision of endometriotic cysts and hemostasis achieved either by bipolar coagulation or suturing: a randomized clinical trial. Arch Gynecol Obstet 293(5): 1015-1022.
Ballester M, Oppenheimer A, Mathieu d’Argent E, Touboul C, Antoine JM, Nisolle M, Daraï E. Deep infiltrating endometriosis is a determinant factor of cumulative pregnancy rate after intracytoplasmic sperm injection/in vitro fertilization cycles in patients with endometriomas. Fertil Steril. 2012;97:367-72.
Kunz G, Herbertz M, Beil D, Huppert P, Leyendecker G. Adenomyosis as a disorder of the early and late human reproductive period. Reproductive biomedicine online. 2007 Jan 1;15(6):681-5.
Costello, M.F., Lindsay, K., McNally, G., 2011. The effect of adeno- myosis on in vitro fertilisation and intra-cytoplasmic sperm in- jection treatment outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 158, 229–234.
A Hashimoto, T. Iriyama, and S. Sayama, “Adenomyosis and adverse perinatal outcomes: increased risk of second trimester miscarriage, preeclampsia, and placental malposition,” The Journal of Maternal-fetal Neonatal Medicine, vol. 23, no. 1-6, p. 18, 2017.
ESHRE TT, ASRM-Sponsored PCOS Consensus Workshop Group. Consensus on infertility treatment related to polycystic ovary syndrome. Fertility and sterility. 2008 Mar 1;89(3):505-22.
Hashim HA. Predictors of success of laparoscopic ovarian drilling in women with polycystic ovary syndrome: an evidence-based approach. Archives of gynecology and obstetrics. 2015 Jan 1;291(1):11-8.
Medeiros LR, Rosa DD, Bozzetti MC, Fachel JM, Furness S, Garry R, et al. Lap- aroscopy versus laparotomy for benign ovarian tumour. Cochrane Database Syst Rev 2009:CD004751.
Daniilidis, A., Balaouras, D., Chitzios, D., Theodoridis, T., Assimakopoulos, E. Hydrosalpinx: Tubal surgery or in vitro fertilisation?. J. Obstet. Gynaecol 2017; 37: 550–556
Johnson, N., van Voorst, S., Sowter, M.C., Strandell, A., Mol, B.W.J. Surgical treatment for tubal disease in women due to undergo in vitro fertilisation. Cochrane Libr 2010
Grynnerup, A.G., Lindhard, A., Sørensen, S. Anti- Muïllerian hormone levels in salpingectomized compared with nonsalpingectomized women with tubal factor infertility and women with unexplained infertility. Acta Obstet. Gynecol. Scand. 2013; 92: 1297–1303
NICE. Fertility: Assessment and Treatment for People with Fertility Problems. National Institute for Health and Clinical Excellence, 2013.
Elbareg AM, Essadi FM. Impact of routine hysteroscopy (HS) prior to intrauterine insemination (IUI) on pregnancy rates (PR) among infertile couples at Al-Amal Hospital, Misurata, Libya. J Pregnancy Reprod. 2017 Nov 4;1(4):1-4.
Elsetohy KA, Askalany AH, Hassan M, Dawood Z. Routine office hysteroscopy prior to ICSI vs. ICSI alone in patients with normal transvaginal ultrasound: a randomized controlled trial. Arch Gynecol Obstet 2015;291:193–199.
El-Toukhy T, Campo R, Khalaf Y, Tabanelli C, Gianaroli L, Gordts SS, Gordts S, Mestdagh G, Mardesic T, Voboril J, Marchino GL. Hysteroscopy in recurrent in-vitro fertilisation failure (TROPHY): a multicentre, randomised controlled trial. The Lancet. 2016 Jun 25;387(10038):2614-21.
Nastri CO, Lensen SF, Gibreel A, Raine-Fenning N, Ferriani RA, Bhattacharya S, Martins WP. Endometrial injury in women undergoing assisted reproductive techniques. Cochrane database of systematic reviews. 2015(3).
Mak JS, Chung CH, Chung JP, Kong GW, Saravelos SH, Cheung LP, Li TC. The effect of endometrial scratch on natural-cycle cryopreserved embryo transfer outcomes: a randomized controlled study. Reproductive biomedicine online. 2017 Jul 1;35(1):28-36.
van Hoogenhuijze NE, Kasius JC, Broekmans FJ, Bosteels J, Torrance HL. Endometrial scratching prior to IVF; does it help and for whom? A systematic review and meta-analysis. Human Reproduction Open. 2019 Jan 29;2019(1):hoy025.
Chen Sar-Shalom Nahshon, Lena Sagi-Dain, Zofnat Wiener-Megnazi, Martha Dirnfeld, The impact of intentional endometrial injury on reproductive outcomes: a systematic review and meta-analysis, Human Reproduction Update, Volume 25, Issue 1, January-February 2019, Pages 95–113,
Attilio Di Spiezio Sardo, Costantino Di Carlo, Silvia Minozzi, Marialuigia Spinelli, Vanna Pistotti, Carlo Alviggi, Giuseppe De Placido, Carmine Nappi, Giuseppe Bifulco, Efficacy of hysteroscopy in improving reproductive outcomes of infertile couples: a systematic review and meta-analysis, Human Reproduction Update, Volume 22, Issue 4, July/August 2016, Pages 479–496,
McQueen D, Bernardi L, Stephenson M. Chronic endometritis in women with recurrent early pregnancy loss and/or fetal demise. Fertil Steril 2014; 101:1026–30.
Johnston-MacAnanny E, Hartnett J, Engmann L, Nulsen J, Sanders M, Benadiva C. Chronic endometritis is a frequent finding in women with recurrent implantation failure after in vitro fertilization. Fertil Steril 2010;93:437–41.
Robinson J, Colimon L, Isaacson K. Postoperative adhesiolysis therapy for intrauterine adhesions (Asherman’s syndrome). Fertil Steril 2008;90:409–14.
Revaux A, Ducarme G, Luton D. Prevention of intrauterine adhesions after hysteroscopic surgery. Gynecologie, obstetrique & fertilite. 2008 Mar;36(3):311-7.
Sardo AD, Spinelli M, Bramante S, Scognamiglio M, Greco E, Guida M, Cela V, Nappi C. Efficacy of a polyethylene oxide–sodium carboxymethylcellulose gel in prevention of intrauterine adhesions after hysteroscopic surgery. Journal of minimally invasive gynecology. 2011 Jul 1;18(4):462-
Fuchs N, Smorgick N, Ami IB, Vaknin Z, Tovbin Y, Halperin R, Pansky M. Intercoat (Oxiplex/AP gel) for preventing intrauterine adhesions after operative hysteroscopy for suspected retained products of conception: double-blind, prospective, randomized pilot study. Journal of minimally invasive gynecology. 2014 Jan 1;21(1):126-30.
Bhandari S, Bhave P, Ganguly I, Baxi A, Agarwal P. Reproductive outcome of patients with Asherman’s syndrome: A SAIMS experience. Journal of reproduction & infertility. 2015 Oct;16(4):229.
Detti L, Hickman H, Levi D’Ancona R, Wright AW, Christiansen ME. Relevance of uterine subseptations: what length should warrant hysteroscopic resection?. Journal of Ultrasound in Medicine. 2017 Apr;36(4):757-65
Venetis, C.A., Papadopoulos, S.P., Campo, R., Gordts, S., Tarlatzis, B.C., Grimbizis, G.F. Clinical implications of congenital uterine anomalies: a meta-analysis of comparative studies. Reprod. Biomed. Online. 2014; 29: 665–683
NICE guidelines. Hysteroscopic metroplasty of a uterine septum for recurrent miscarriage. https://www.nice.org.uk/guidance/ipg510/ chapter/1-Recommendations 2015
Abuzeid, M., Ghourab, G., Abuzeid, O., Mitwally, M., Ashraf, M., Diamond, M. Reproductive outcome after IVF following hysteroscopic division of incomplete uterine septum/arcuate uterine anomaly in women with primary infertility. Facts Views Vis. Obgyn. 2014; 6: 194–202
Chan Y, Jayaprakasan K, Tan A et al. Reproductive outcomes in women with congenital uterine anomalies: a systematic review. Ultrasound Obstet Gynecol. 2011;38(4):371-82.
Fernandez H, Garbin O, Castaigne V et al. Surgical approach to and reproductive outcome after surgical correction of a T-shaped uterus. Hum Reprod. 2011;26(7):1730-4.
Ferro J, Labarta E, Sanz C, Montoya P, Remohi J. Reproductive outcomes after hysteroscopic metroplasty for women with dysmorphic uterus and recurrent implantation failure. Facts, views & vision in ObGyn. 2018 Jun;10(2):63.
Chapter 5: Advice on Preconception Care
OVERVIEW
This guideline offer recommendations to highlight the benefits of preconception care by outlining the interventions that are effective and beneficial. This guideline will act as a blueprint to the standards of preconception care in India. These recommendations highlight the benefits of preconception care, outline preconception interventions, and provide the evidence to make the case for preconception care. It is aimed primarily at women aged 18 years or older presenting to healthcare professionals or general practitioners or any maternity service providers.
1. Definition of preconception care
Preconception care comprises a range of interventions aimed at identifying and modifying medical, behavioral, and social risks to women’s and men’s health during their reproductive years
Preconception care is aimed at identifying, preventing, and managing risk factors that adversely affect maternal-fetal outcomes before conception
2. Need for preconception care
-
Health inequalities is a global problem and more so in India. The reason behind this is the diversity in:
-
»Socioeconomic status
-
»Access to education
-
»Culture
-
»Social makeup
-
»Dietary habits
-
»Beliefs and way of life in general
-
»
There is ample evidence to prove that timely preconception interventions correlate positively with improved maternal and neonatal outcomes as it focuses on health irrespective of an individual’s reproductive plans. The preconception period is a singular unique time to address health inequalities before they set in
A woman’s health at conception is the biggest predictor of pregnancy outcomes. Correcting it at this time ensures a better start for infants in life and sustained efforts will make the benefit percolate through generations
3. Some Indian statistics
-
In 2015, India was declared maternal and neonatal tetanus free, similar accolades remain to be achieved on other accounts
-
»One in two pregnancies in India is unintended as opposed to 2 in 5 globally
-
»53% of women in the reproductive age group in India have iron–deficiency anemia
-
»40% of Indian women have a lifetime risk of suffering domestic violence, especially during pregnancy
-
»Approximately 11.8 million teenage pregnancies occur in India per year
-
»The neonatal mortality rate remains at about 28 per 1000 live births and is as high as 50% in teenage pregnancies
-
»Around 3.2% of Indian women smoke i.e. about 12 million women. The ones that do smoke take more than 7 puffs a day. Indian girls start smoking at 17.7 years of age as opposed to boys at 18.5 years
-
»
4. Benefits of preconception care
Reduces maternal and child morbidity and mortality
Prevent unplanned pregnancies
Prevent preterm birth, low birth weight, and stillbirths
Prevent birth defects
Prevent neonatal infections
Prevent underweight and stunting
Prevent vertical transmission of human immunodeficiency virus (HIV); sexually transmitted infections (STIs)
5. Barriers in preconception care implementation in India
Fragmented health care service delivery system
Poor health care budgets
Lack of identification and treatment services for high–risk behaviors
Inadequate availability and penetration of counseling services
Lack of practice guidelines and protocols for uniformity of care
Not all preconception interventions supported by robust evidence
End–user diversity leading to women most in need of preconception care least likely to receive it
6. Constituents of preconception care
-
It encompasses if and when a couple will like to choose to be parents and their fitness for pregnancy. Preconception care includes the following:
-
»Management of pre–existing health conditions
-
»Assistance in ceasing risky behaviors
-
»Promoting healthy behaviors
-
»
7. Preconception care recommendations
7.1 Reproductive planning
-
Opportunistically discuss reproductive goals–
- Discuss factors that will affect the optimum outcome–medications, lifestyle, habits, activities, and health conditions
- Discuss about effecting of ageing on ovarian reserve and oocyte quality and aneuploidy in the embryos
- Also, discuss the possibility of premature ovarian insufficiency at a younger age
7.2 Contraception
When not planning for a pregnancy, counsel for and offer a full range of contraception–Cafeteria approach
Counsel for and support birth spacing
Encourage late age for first conception
7.3 Genetic and family history
Take a thorough personal and family history. Especially ask for consanguinity and ethnic background (thalassemias)
Identify risk factors for genetic conditions
Offer genetic counseling and carrier screening and testing to a high–risk population
Advice about the age–related increased risk of genetic issues e.g. Down’s syndrome
7.4 Psychosocial issues
Screen for depression and anxiety disorders
Counsel and treat preexisting depression
Explain the risks of antidepressant medications
-
Look for signs of, and actively ask about exposure to domestic violence. Evaluate the patient’s safety and offer help as appropriate
-
»Ask about alcohol use and abuse and counsel about alcohol cessation
-
»Ask about tobacco use and offer counseling and treatment for the cessation of smoking
-
»Ask for use of recreational drugs
-
»Educate about fetal alcohol syndrome and the risks of smoking to the fetus
-
»Provide access to behavioral interventions to reduce tobacco, alcohol, and drug use
-
»
7 .5 Infection screening
-
Screen and treat all women who are at risk of infection f–Chlamydia, gonorrhea, all high–risk women, herpes simplex virus infection, HIV, syphilis, and tuberculosis
-
»Counsel about the risk of vertical transmission
-
»Universal screening for HIV
-
»Treat women with active and latent disease before pregnancy. Screen for periodontal and urinary infections and treat accordingly
-
»
7.6 Vaccination
| Name of the vaccine | Recommendation |
|---|---|
| Hepatitis B | • Vaccinate all high–risk women |
| • Counsel chronic carriers about the prevention of vertical transmission | |
| Influenza | • Vaccinate all women during influenza season and women at risk of influenza–related complications |
| MMR | • Screen for immunity |
| • Vaccinate all non–immune women non–pregnant women | |
| • Consider vigorous counselling in patients to avoid pregnancy for 3 months post vaccination | |
| DPT | • Tetanus vaccination may protect against neonatal tetanus |
| • Vaccinate with Tdap* between 27 to 36 weeks’ gestation to reduce the risk of neonatal tetanus | |
| Varicella | • Screen for immunity |
| • Vaccinate all non–immune women who are not pregnant | |
| • Subject to patient counselling to avoid pregnancy for 1 month post vaccination |
*Tetanus, diphtheria, and pertussis (whooping cough)
7.7 Exercise, diet, nutrition and supplements
Assess BMI and consider counselling of women in those with obesity, overweight, or underweight regarding achieving a healthy body weight before pregnancy
Screen for anemia and diabetes
Supplement iron and folic acid
Monitor nutritional status
7.7.1 Exercise
Moderate–intensity physical exercise, 30 minutes/day
No detrimental effect of moderate exercise in the preconception period
High contact sports are contraindicated e.g. mountaineering, deep sea diving, etc
Promoting exercise
Consider use of Iodized salt
7.7.2 Recommended supplements
7.7.2 Recommended supplements
| Nutrient | Target population | Recommended dose | Helps |
|---|---|---|---|
| Folic acid | All women preconception high risk (previous NTD, an anticonvulsant medication, GDM, malabsorption, obese) | 400–500 µg daily for at least four weeks before pregnancy and the first 12 weeks of gestation, 5 mg daily for at least four weeks before pregnancy and the first 12 weeks of gestation | Prevention of NTD such as spina bifida and anencephaly |
| Iodine | All women | 150 µg daily while pregnant and breastfeeding | Production of maternal thyroid hormone, fetal brain, and CNS development |
| Vitamin D | Women with vitamin D deficiency | 1000 IU/day (vitamin D 30–49 nmol/L) 2000 IU/day (vitamin D <30 nmol/L) | Reduces the risk of small–for–gestational–age babies and impaired fetal skeletal development |
| Iron | Women with iron deficiency | Oral supplement with at least 60 mg of elemental iron daily | Prevention of anemia |
| Vitamin B12 | Vegans and vegetarians | 2.6 µg/day or intramuscular injection 1000 µg/ampoule | Infant neurological sequelae |
| Calcium | Women with an inadequate dietary intake (<1000 mg daily) | At least 1000 mg daily | Prevention of pre-eclampsia |
CNS: central nervous system; GDM: gestational diabetes mellitus; NTD: neural tube defects.
7.7.3 Nutrients to restrict
7.7.3 Nutrients to restrict
| Nutrient | Target population | Recommended limitation | Why? |
|---|---|---|---|
| Vitamin A | All women | Dietary sources do not pose a risk at normal levels Limit vitamin A supplements to 3000 IU per day All synthetic derivatives of retinol should be ceased at least one month before conception | Increased risk of miscarriage and CNS malformations |
| Mercury–containing fish | All women | Avoid fish containing high levels of mercury and eat two to three serves of other types of fish per week | Increased risk of negative effects on the fetal brain and CNS |
| Caffeine | All women | Limit to 300 mg or less per day (i.e., 2 or 3 cups) | Increased risk of fetal growth restriction |
CNS: central nervous system.
7.8 Chronic medical conditions
Optimize control of any preexisting medical condition
Where possible make the patient medication free
Where not possible use the least harmful drug at the least possible needed for control
Prefer monotherapy to polypharmacy
Inform and counsel that one–third of preexisting medical conditions can worsen in pregnancy
Offer TOP if the pregnant patient was already exposed to known teratogenic agent
7.8.1 Diabetes
-
»
Discontinue most oral hypoglycemic and start insulin
-
»
Metformin may be continued
-
»
Advice weight loss where indicated
-
»
Inform and counsel about the risk of miscarriage and fetal macrosomia
-
»
Avoid ACE inhibitors, statins due to the risk of fetal renal damage and fetal demise seen in animal studies, limited data available in humans
7.8.2 Hypertension
-
»
Counsel for the risk of superadded preeclampsia.
-
»
Advice regular BP checkups
-
»
Counsel about the risk of low birth weight baby and intrauterine growth restriction (IUGR)
-
»
Avoid ACE inhibitors, alpha receptor blockers due to fetal renal complications
7.8.3 Hypo and hyperthyroidism
-
»
TSH screening is a must for all women preparing for a pregnancy
-
»
In cases of active thyroid disease, it is desirable to aim for TSH in the range of 2–3.5 mIU/L (≤2.5 mIU/L) for better outcomes
-
»
Propylthiouracil (PTU) is preferred in preconception and the first trimester
Methimazole may be used in second and third trimesters
There is a risk of teratogenicity in the first trimester
If surgery is needed for goiter this may be done in the preconception period
If radioiodine has been used to avoid pregnancy for 3 months
7.8.4 Asthma
Inhaled steroids and b–agonists are safe for use
Oral steroids are associated with increased risk of pre-eclampsia, reduced birth weight, and oral clefts
7.8.5 Seizure disorder
Postpone conception until seizure free for a year
Most antiepileptics are teratogenic
Higher doses and polytherapy increase the risk of congenital anomalies
Monotherapy at least effective dose should be achieved before conception
Where possible it is best for the patient to be medication free and disease under control
7.8.6 Thrombophilia
Warfarin is teratogenic
Shift to heparin during preconception care
Low-molecular-weight heparin (LMWH) is preferred anticoagulant for preconception and pregnancy
7.8.7 Preconception care for men
Enquire about male reproductive health issues at the preconception visit
When the couple is planning for a pregnancy, discuss medical conditions, activities, and lifestyle issues
When not planning for pregnancy offer contraception
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| Lifestyle | |||
| CPP | • The use of illicit drugs and alcohol during pregnancy has adverse effects on the neonate, and these children are at risk for altered neurodevelopmental outcome and poor health status. Detection of drug and alcohol abuse is essential to counsel them preconceptionally about the effects on mother and fetus | - | - |
| CPP | • Screening of women and girls for tobacco use (smoking and smokeless tobacco) at all clinical visits and also informing about passive smoke and harmful effects on pregnant women and unborn children | - | - |
| CPP | • Counsel about health risks associated with smoking during pregnancy include intrauterine growth restriction, placenta previa, and abruptio placentae Additionally, adverse pregnancy outcomes may occur including premature rupture of membranes, low birth weight, and perinatal mortality. Smokers of reproductive age should be counselled about the associated risks of smoking and the negative outcomes associated with pregnancy | - | - |
| CPP | • Intervention, known as the 5 A’s, is appropriate for use during routine prenatal office visits and includes the following five steps: Ask, Advise, Assess, Assist, and Arrange | - | - |
| CPP | • Providing brief tobacco cessation advice, pharmacotherapy (including nicotine replacement therapy, if available) and intensive behavioural counselling services | - | - |
| CCR | • Treating substance use disorders, including pharmacological and psychological interventions | C | - |
| CCR | • Counsel on healthy balanced diet. Inform that women needs around 2,000 kcal to maintain her weight. Being obese (body mass index [BMI] >30) increases the risk of hypertension in pregnancy and gestational diabetes by almost 11 times, as well as other pregnancy complications, such as miscarriage, shoulder dystocia, blood clots, and still birth | C | - |
| CPP | • Recommend regular moderate exercise | - | - |
| Nutritional Conditions | |||
| • Screening for anemia and diabetes | - | - | |
| CPP | • Supplementing iron and folic acid | A | - |
| CCR | • Information, education, and counselling | - | - |
| CPP | • Monitoring nutritional status | - | - |
| CPP | • Supplementing energy–and nutrient–dense food | - | -- |
| CPP | • Management of diabetes, including counselling people with diabetes mellitus | - | - |
| • Promoting exercise | A | II | |
| EBR | • Iodization of salt | ||
| • Counsel on the importance of vitamin D for calcium absorption, and maintenance of healthy bones and teeth is widely known. Inform that insufficient vitamin | - | - | |
| CPP | D during pregnancy results in calcium deficiency, which can lead to maternal | - | - |
| CPP | osteomalacia (softening of bones), pre–eclampsia, low birth weight, and increased risk of neonatal tetanic seizures and childhood rickets | - | - |
| CPP | |||
| CCR | • Supplement Vitamin D if required | C | - |
| Environmental health | |||
| CPP | • Providing guidance and information on environmental hazards and prevention | - | - |
| CPP | • Protecting from unnecessary radiation exposure in occupational, environmental, and medical settings | - | - |
| CPP | • Avoiding unnecessary pesticide use/providing alternatives to pesticides | - | - |
| CPP | • Protecting from lead exposure | - | - |
| CPP | • Informing women of childbearing age about levels of methyl mercury in fish | - | - |
| CPP | • Promoting use of improved stoves and cleaner liquid/gaseous fuels | - | - |
| CPP | • Occupational exposures–Material Safety Data Sheets for employer | - | - |
| CPP | • Counsel on effects of chemotherapy and radiation exposure in early pregnancy | - | - |
| Genetic conditions | |||
| CPP | • Taking a thorough family history to identify risk factors for genetic conditions Family planning | - | - |
| CPP | • Genetic counselling | - | - |
| CPP | • Carrier screening and testing of racial/ethnic background/family history | - | - |
| EBR | » Sickle cell anemia | ||
| » Cystic fibrosis | B | III | |
| » Thalassemia | |||
| » Tay–Sachs disease | |||
| CCR | • Appropriate treatment of genetic conditions | C | - |
| CPP | • Community–wide or national screening among populations at high risk | - | - |
| CPP | Sexually transmitted infections (STIs) Providing age–appropriate comprehensive sexuality education and services | - | - |
| CPP | • Promoting safe sex practices through individual, group, and community–level behavioural interventions | - | - |
| CPP | • Promoting condom use for dual protection against STIs and unwanted pregnancies | - | - |
| CPP | • Ensuring increased access to condoms | - | - |
| CCR | • Screening for STIs | C | - |
| CPP | • Increasing access to treatment and other relevant health services | - | - |
| HIV | |||
| CPP | • Family planning | - | - |
| CPP | • Promoting safe sex practices and dual method for birth control (with condoms) and STI control | - | - |
| CPP | • Provider–initiated HIV counselling and testing, including male partner testing | - | - |
| EBR | • Providing antiretroviral therapy for prevention and pre–exposure prophylaxis | A | II |
| CPP | • Providing male circumcision | - | - |
| EBR | • Providing antiretroviral prophylaxis for women not eligible for, or not on, antiretroviral therapy to prevent mother–to–child transmission | B | I |
| CCR | • Determining eligibility for lifelong antiretroviral therapy | C | - |
| Vaccine–preventable diseases | |||
| EBR | • Vaccination against rubella | A | II |
| EBR | • Vaccination against tetanus and diphtheria | A | II |
| EBR | • Vaccination against hepatitis B | A | II |
| Mental health | |||
| CPP | • Assessing psychosocial problems | - | - |
| CPP | • Providing educational and psychosocial counselling before and during pregnancy | - | - |
| CPP | • Counselling, treating, and managing depression in women planning pregnancy and other women of childbearing age | - | - |
| CPP | • Strengthening community networks and promoting women’s empowerment | - | - |
| CPP | • Improving access to education for women of childbearing age | - | - |
| CPP | • Reducing economic insecurity of women of childbearing age | - | - |
| Too–early, unwanted, and rapid successive pregnancies | |||
| CPP | • Influencing cultural norms that support early marriage | - | - |
| CPP | • Providing age–appropriate comprehensive sexuality education | - | - |
| CPP | • Providing contraceptives and building community support for preventing early pregnancy and contraceptive provision to adolescents | - | - |
| CPP | • Engaging men and boys to critically assess norms and practices regarding gender–based violence and coerced sex | - | - |
| CPP | • Educating women and couples about the dangers to the baby and mother of short birth intervals | - | - |
| Chronic disease | |||
| CPP | • Identification and management of chronic diseases like asthma, diabetes mellitus, hypothyroidism, heart disease, obesity, and dental disease | B | - |
| CCR | • If on any medication, its use should be continued to control disease in women during the preconception period. Switching medication may be appropriate during the preconception period if suitable alternatives exist with less risk to the pregnant woman or fetus | B | - |
| EBR | • Certain drugs taken preconceptionally may be a risk factor for negative pregnancy outcomes and therefore should be used with caution. | B | |
| • Isotretinoins: If used in pregnancy to treat acne, it can result in miscarriage and birth defects. | B | II | |
| EBR | • Anti–epileptic drugs: Certain types e.g. valproic acid are teratogens | A | III |
| EBR | • Oral anticoagulants such as warfarin have shown to be teratogenic. Early exposure during pregnancy could be avoided preconceptionally by switching to safer drugs | A | II |
| EBR | • In presence of chronic medical conditions | B | II |
| EBR | • Diabetes–optimize control | A | II |
| EBR | • Hypertension–avoid ACE inhibitors, angiotensin II receptor antagonists | A | I |
| EBR | • Epilepsy–consider increased dose of folic acid | B | II |
| EBR | • DVT–switch from warfarin (Coumadin) to heparin | A | I |
| EBR | • Acne–stop isotretinoins (e.g. Accutane) | B | III |
| EBR | • Depression/anxiety and other mental health issues–discuss current benefit/risk medication data | C | IV |
| Assess any complications from previous pregnancies | |||
| CPP | • Cesarean section | - | - |
| • Premature delivery | |||
| • Hypertensive disorder of pregnancy | |||
| • Diabetes | |||
| • Rh incompatibility | |||
| • Postpartum hemorrhage | |||
| • Thrombotic event (DVT/PE) | |||
| Other pre–conceptional advice | |||
| CPP | Screen for domestic violence | - | - |
| CPP | Screen for social issues (e.g. place to live, child care, transportation) | - | - |
| CPP | Counsel on the use of over–the–counter medications, nutritional supplements, and naturopathic substances | - | - |
ACE: angiotensin-converting enzyme; DVT: deep venous thrombosis; HIV: human immunodeficiency virus; PE: pulmonary embolism.
References
Centers for Disease Control and Prevention. Preconception Health and Health Care. 2015. Available at: http://www.cdc.gov/preconception/index.html. Accessed 20th Sept 2019.
Johnson K, Posner S, Biermann J, et al. Recommendations to improve preconception health and health care-United States. A report of the CDC/ATSDR preconception care work group and the select panel on preconception care. MMWR Recomm Rep. 2006;55(RR-6):1-23.
Sher J. Missed Periods: Scotland’s opportunities for better pregnancies, healthier parents and thriving babies the first time … and every time. NHS Greater Glasgow and Clyde (Public Health). 2016. http://www.nhsggc.org.uk/media/237840/missed-periods-j-sher- may-2016.pdf.
WHO news, August 2015. Available at: https://www.who.int/life-course/news/regional- news/tetanus-elimination-in-India/en/ Accessed 20th Sept 2019.
Singh S, Shekhar C, Acharya R, et al. The incidence of abortion and unintended pregnancy in India, 2015. Lancet Glob Health. 2018;6(1):e111-e120.
Singh S, Sedgh G, Hussain R. Unintended pregnancy: Worldwide levels, trends, and outcomes. Stud Fam Plann. 2010;41(4):241-50.
Rai RK, Fawzi WW, Barik A, et al. The burden of iron-deficiency anaemia among women in India: how have iron and folic acid interventions fared? WHO South East Asia J Public Health. 2018;7(1):18-23.
Kalokhe A, Del Rio C, Dunkle K, et al. Domestic violence against women in India: A systematic review of a decade of quantitative studies. Glob Public Health. 2017;12(4):498-513.
Aguayo VM, Paintal K. Nutrition in adolescent girls in South Asia. BMJ. 2017;357:j1309.
Sankar MJ, Neogi SB, Sharma J, et al. State of newborn health in India. J Perinatol. 2016;36(s3):S3-S8.
GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906.
National Institute for Health and Clinical Excellence. Preconception - advice and management. 2012. Available at: http://cks.nice.org.uk/pre-conception-advice- andmanagement#!management. Accessed 20th Sept 2019.
FSRH Clinical Effectiveness Unit. Statement from the clinical effectiveness unit pre- conception care 15th September 2016. Available at: file:///C:/Users/Isaac/Downloads/pre- conception-care-edit-15-9-16.pdf Accessed 20th Sept 2019.
Moos MK, Dunlop AL, Jack BW, et al. Healthier women, healthier reproductive outcomes: recommendations for the routine care of all women of reproductive age. Am J Obstet Gynecol. 2008;199(6 Suppl 2):S280-9.
Shapira SK, Dolan S. Genetic risks to the mother and the infant: assessment, counseling, and management. Matern Child Health J. 2006;10(5):S143-6.
Frieder A, Dunlop AL, Culpepper L, Bernstein PS. The clinical content of preconception care: women with psychiatric conditions. Am J Obstet Gynecol. 2008;199(6 suppl 2):S328-S332.
American College of Obstetricians and Gynecologists. Domestic violence. ACOG Education Bulletin 257. Washington, DC: ACOG; 1999.
Floyd RL, Jack BW, Cefalo R, et al. The clinical content of preconception care: alcohol, tobacco, and illicit drug exposures. Am J Obstet Gynecol. 2008;199(6 suppl 2):S333-39.
U.S. Preventive Services Task Force. Screening for chlamydial infection: recommendations and rationale. Am J Prev Med. 2001;20(3):90-4.
U.S. Preventive Services Task Force. Screening for gonorrhea. May 2005. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsgono.htm Accessed 20th Sept 2019.
Mofenson LM; Centers for Disease Control and Prevention, U.S. Public Health Service Task Force. U.S. Public Health Service Task Force recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV-1 transmission in the United States. MMWR Recomm Rep. 2002;51(RR-18):1-38.
U.S. Preventive Services Task Force. Screening for syphilis infection. July 2004. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspssyph.htm. Accessed 20th Sept 2019.
National Collaborating Centre for Women’s and Children’s Health; National Institute for Health and Clinical Excellence. Antenatal care: routine care for the healthy pregnant women. London, England: RCOG Press; 2008.
Lumley J, Watson L, Watson M, Bower C. Periconceptional supplementation with folate and/or multivitamins for preventing neural tube defects. Cochrane Database Syst Rev. 2000;(2):CD001056.
Elsinga J, de Jong-Potjer LC, van der Pal-de Bruin KM, et al. The effect of preconception counselling on lifestyle and other behaviour before and during pregnancy. Womens Health Issues. 2008;18(6):S117-25.
Wilson RD, Davies G, Désilets V, et al.; Genetics Committee and Executive and Council of the Society of Obstetricians and Gynaecologists of Canada. The use of folic acid for the prevention of neural tube defects and other congenital anomalies. J Obstet Gynaecol Can. 2003;25(11):959-73.
Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. MRC Vitamin Study Research Group. Lancet. 1991;338(8760):131-137.
Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. JAMA. 2004;291(23):2847–850.
Siega-Riz AM, Siega-Riz AM, Laraia B. The implications of maternal overweight and obesity on the course of pregnancy and birth outcomes. Matern Child Health J. 2006;10(5 suppl):S153–56.
Tsai AG, Wadden TA. Systematic review: an evaluation of major commercial weight loss programs in the United States. Ann Intern Med. 2005;142(1):56-66.
Hayman M, Brown W. Exercise in pregnancy and the postpartum period. Victoria: Sports Medicine Australia, 2016.
Royal College of Obstetricians and Gynaecologists. Physical activity for pregnant women (Infographic). London: RCOG, 2017.
Qublan HS, Yannakoula EK, Al-Qudah MA, El-Uri FI. Dietary intervention versus metformin to improve the reproductive outcome in women with polycystic ovary syndrome. A prospective comparative study. Saudi Med J. 2007;28(11):1694-1699.
Dunlop AL, Jack BW, Bottalico JN, et al. The clinical content of preconception care: women with chronic medical conditions. Am J Obstet Gynecol. 2008;199(6 suppl 2):S310-27.
Lydakis C, Lip GY, Beevers M, Beevers DG. Atenolol and fetal growth in pregnancies complicated by hypertension. Am J Hypertens. 1999;12(6):541-47.
De Groot L, Abalovich M, Alexander EK, et al. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97(8):2543-65.
Schatz M. The efficacy and safety of asthma medications during pregnancy. Semin Perinatol. 2001;25(3):145-52.
National Asthma Education and Prevention Program (National Heart, Lung, and Blood Institute). Working Group on Asthma and Pregnancy. Working Group report on managing asthma during pregnancy: recommendations for pharmacologic treatment. NIH publication 04-5236. Bethesda, Md.: National Institutes of Health; 2005.
Green KA, Werner MD, Franasiak JM, et al. Investigating the optimal preconception TSH range for patients undergoing IVF when controlling for embryo quality. J Assist Reprod Genet. 2015;32(10):1469-76.
Stagnaro-Green A, Abalovich M, Alexander E, et al. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21(10):1081-125.
ACOG educational bulletin. Seizure disorders in pregnancy. Number 231, December 1996. Committee on Educational Bulletins of the American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 1997;56(3):279–86.
Silver RM, Warren JE. Preconception counseling for women with thrombophilia. Clin Obstet Gynecol. 2006;49(4):906–19.
Chapter 6: Medical & Surgical Management of Male Infertility
OVERVIEW
This guideline is of relevance to:
The professional groups who share in caring for couples seeking advice and treatment for fertility problems, such as gynecologists, andrologists, GPs, counselors, and nurses
Those with responsibilities for commissioning and planning fertility services in primary care trusts and Health Commission
People seeking advice and treatment for possible infertility
1. Introduction
Male factor is present in nearly 50% of cases
Offer examination and evaluation of all males coming to an infertility clinic
Infertility platform affords an opportunity to evaluate young males for other problems such as diabetes, hyperlipidemia, ischemic heart disease (IHD), renal failures, pituitary tumors, and testicular cancers
2. Investigations
2.1 Semen analysis
The most basic investigation is a good standardized semen analysis report with an abstinence period of 3–4 days
Semen analysis should be performed and further andrological assessments should be done if at least two semen analysis reports show abnormality
WHO parameters of semen analysis are not sufficient to interpret the fertility status or chance of pregnancy in either natural or assisted conception and male infertility workup thus goes far beyond a simple semen analysis
Reference values are shown in Table1 below
Table1.
Reference values of semen parameters in different WHO mannuals
| WHO laboratory manual for the examination of human semen and sperm–cervical mucus interaction 1992 | WHO laboratory manual for the examination of human semen and sperm–cervical mucus interaction 1999 | WHO laboratory manual for the examination and processing of human semen 2010 | |
|---|---|---|---|
| Volume | 2.0 | 1.5 | 1.5 (1.4-1.7) |
| pH | 7.2–7.8 | 7.2 | ≥7.2 |
| Concn (x 106ml) | 20 | 20 | 15 (12–16) |
| Total count | 40 | 40 | 39 (33–46) |
| Prog motility(%) | 50 | 50 | 32 (31–34) |
| % Normal morph | 30 | - | 4 (3.0–4.0) |
| Vitality (alive) | 75 | 75 | 58 (53–63) |
| WBC (x106) | 1.0 | 1.0 | <1.0 |
| %MAR | 20 | 50 | <50 |
MAR: mixed antiglobulin reaction; WBC: white blood cells; WHO: World Health Organization.
2.2 Hormonal investigations
Endocrine laboratory diagnosis is recommended in cases of low sperm count especially if less 10 mill/ml, impaired sexual function and clinical findings suggestive of a endocrinopathy
When semen parameters are abnormal assessment for serum follicle-stimulating hormone (FSH), and serum testosterone should be done. Additional luteinizing hormone(LH), prolactin & estradiol (E2), sex hormone binding globulin (SHBG) is done in men with low testosterone levels
An elevated FSH level greater than twice the normal upper limit is a reliable indicator of abnormal spermatogenesis and severe testicular dysfunction
However, focal areas of spermatogenesis may be present in patients with highly elevated FSH levels
Recently a stronger correlation has been demonstrated between inhibin B, anti-Müllerian hormone (AMH), and spermatogenesis as they reflect Sertoli cell function
Do not consider routine inhibin B and AMH estimation in andrological evaluation. Though levels correlate with testicular cytology but are not superior to FSH as predictors fort the presence of sperm in testicular sperm extraction (TESE)/ fine needle aspiration (FNA) in men with azoospermia
2.3 Sperm function Test
2.3.1 Hypo-osmotic swelling test
Provides information on membrane integrity of sperm and has a good correlation exist between spermatozoa showing positive HOS reaction and FR at IVF
2.3.2 Teratozoospermia index (TZI)
Normal values for TZI is <1.6. If TZI is >1.8. ICSI is beneficial irrespective of count and motility
Sperm survival test
Sperm survival tests are helpful in assessing IVF outcome and PRs.
Computer–assisted sperm analysis (CASA): A semi–automated technique for semen analysis. CASA is not superior to conventional semen analysis (Grade A). Advantages and disadvantages of CASA are given in Table 2
Table 2.
Advantages and disadvantages of CASA
| Advantages | Disadvantages |
|---|---|
| • High precision | • Sperm concentration, sample preparation and frame rate can affect accuracy of CASA |
| • Quantitative assessment of sperm kinetics | • Stains used also affect the accuracy of determining morphology |
| • Provides data on sperm density, motility, straight–line and curvilinear velocity, linearity, and average path velocity, amplitude of lateral head displacement, flagellar beat frequency, and hyperactivation | • Does not add any advantages in clinical practice |
| • Requires expensive equipment and still requires the active participation of a technician |
CASA: Computer–assisted sperm analysis
CASA is not superior to conventional semen analysis (Grade A)
2.3.3 Sperm DNA fragmentation test
-
There is evidence linking sperm DNA fragmentation to poor reproductive outcome and has impact on embryo/blastocyst development, progress of pregnancy, and pregnancy loss. It may contribute to the development of novel and more personalized approaches to test and treat male factor infertility
-
»Tests that measure the extent of DNA damage
- - SCD (Halo Test)
- - Acridine Orange Assay (AO)
- - Sperm chromatin structure assay (SCSA)
- - Comet Assay (single cell gel electrophoresis assay) quantifies the amount of DNA damage per spermatozoon.
- - TUNEL–Terminal deoxynucleotidyl transferase dUTP nick end labeling–directly measures single or double strand breaks in DNA
-
»DNA fragmentation index (DFI)–Threshold values
-
»
-
TUNEL assay was reported to have the higher precision specificity (91.6%) positive predictive value at a cutoff point of 16.8% as compared to other tests.
-
»SCSA and SCD test have a poor predictive value.
-
»TUNEL assay and Comet assay have fair predictive value after ART
-
»
| 0–15% | High fertility potential |
| >15% and <30% | Good to fair fertility potential |
| 30% and higher | Low to poor fertility potential |
2.3.3.1 Limitations of DNA fragmentation testing
-
Consider the following limitations of DNA fragmentation testing:
-
»Poor accuracy
-
»Poor reproducibility and assessment
-
»Lack of standardized protocols for different tests
-
»Intra assay variability
-
»Inter observer variability
-
»Variability in chosen cut off values
-
»Variable specificity and sensitivity
-
»
2.3.3.2 Sperm DNA fragmentation testing
Indications and evidence for testing
Not enough data to recommend routine sperm DNA testing
Table 3.
Indications for DFI testing
| Indication | Evidence |
|---|---|
| SDF is recommended in patients with grade 2/3 varicocele with normal conventional semen parameters and in patients with grade 1 varicocele with borderline/abnormal conventional semen parameter results SDF testing may allow clinicians to better select varicocelectomy candidates among those men with clinical varicocele and borderline to normal semen parameters | C |
| High DFI may provide a possible explanation for UI, RPL and IUI failure, therefore, it is reasonable to offer SDF testing to these infertile couples as these couples may be better served by IVF or ICSI sooner rather than later | C |
| DFI testing in patients with recurrent ART failure is indicated as it can provide useful prognostic information on subsequent ART cycles | C |
| Several studies have shown some benefit in using testicular sperm rather than ejaculated sperm in men with oligozoospermia, high SDF and recurrent IVF failure | B–C |
| Infertile men with evidence of exposure to pollutants or those found to have a modifiable lifestyle risk factor during evaluation should be offered SDF testing | C |
| DFI can help reinforce the importance of lifestyle modification, predict fertility, and monitor the patient’s response to intervention | C |
ART: assisted reproductive technology; DFI: DNA fragmentation index; RPL: recurrent pregnancy loss; SDF: sperm DNA fragmentation; ICSI: intracytoplasmic sperm injection; IUI: intrauterine insemination; IVF: in vitro fertilization; UI: unexplained infertility.
2.4 Genetic tests
-
Karyotyping: In all men with impaired spermatogenesis–moderate to severe oligospermia (5 million/ml) and azoospermia
-
»Klinefelters syndrome XXY and variants
-
»Translocations
- - Balanced
- - Unbalanced
-
»
-
Molecular genetics: In men with obstructive and non-obstructive azoospermia, severe oligoasthenoteratozoospermia
-
»Y-chromosome microdeletion–AZFc variable phenotype, AZFa, and AZFb in non-obstructive azoospermia
-
»Cystic fibrosis transmembrane conductance regulator (CFTR) mutation in presence CBAVD and obstructive azoospermia
-
»
ASA (antisperm antibody tests) is not recommended routinely
2.5 Ultrasound in male infertility
-
Ultrasound for evaluation of male infertility, should be done in following conditions:
-
»Accurate measurement of testicular volume,
-
»Testicular and epididymal inflammatory and neoplastic lesions
-
»Diagnosis and doppler imaging of varicoceles.
-
»TRUS in seminal vesicular and prostatic abnormalities
-
»Penile blood flow evaluation in erectile dysfunction
-
»Location of the block in RTO by vasography
-
»Locating undescended testes
-
»
2.6 Testicular biopsy
Diagnostic/therapeutic testicular biopsy is done for ultimate differentiation between obstructive and testicular azoospermia. It should be done only when facilities are available for cryopreservation of obtained sperms
-
Testing for sperm oxidative stress:
- - Laboratory signs suggesting possible sperm oxidative stress
- - Poor sperm motility
- - Teratozoospermia
- - High number of round cells (? leukocytes) in semen
- - Increased semen viscosity
- - Poor sperm membrane integrity on HOST
- - Poor fertilization on routine IVF
- - Poor sperm motility after overnight incubation with the oocyte
- - Poor blastocyst development in the absence of a clear female factor (advanced maternal age/poor ovarian reserve)
2.7 Measurement of ROS
Chemiluminescence, which measures total seminal ROS (from WBC, abnormal spermatozoa, and seminal fluid). As the standardization of testing and the availability of these tests remain limited, it will be some time before this test will become a part of regular evaluation for male sub fertility
Cut Off values for ROS: Normal ROS levels in washed sperm suspensions range from 0.10 to 1.03×106 cpm per 20×106 sperm
-
ROS why not a mainstream investigation in the evaluation of male infertility
-
»Normal or reference values are not established at this point
-
»Use of seminal WBC levels as basis of ROS levels, although proven and well–accepted, has yet to establish definite cut–off points
-
»Even low WBC levels (below the WHO cut–off) are associated with ROS
-
»
2.8 Other sperm function tests
-
Other sperm function test like acrosome reaction, acrosin activity test, creatine kinase, sperm penetration assays, and sperm zona binding tests are usually not done
-
»Emerging technologies like microarray, proteomics, epigenetics (aberrant DNA methylation, and RNA assay technologies including RNA–sequencing may help in elucidating the functional role of the spermatozoa
-
»
3. Medical management
-
Abnormalities that can be seen in the male after semen testing
-
»Volume–Low or high
-
»Viscosity–Hyper viscous
-
»Count–Absent or low
-
»Motility Hyper viscous–Low or absent
-
»Morphology–High Teratozoospermia index
-
»Agglutination–Anti–sperm antibody
-
»Infection
-
»
3.1 Medical management of male sub–fertility
3.1.1 GnRH
Indicated only in hypothalamic hypogonadism. GnRh therapy is given with the use of micropumps either SC/IV. Administration with micropumps for several months makes compliance difficult
3.1.2 Gonadotropin therapy
-
Indicated only in hypothalamic hypogonadism with low FSH & LH levels
-
»Offer gonadotropin therapy with 2000 units of hCG twice a week with hMG 75 IU or rFSH 100-150 IU two to three times a week for 3 months
-
»First spermatozoa appear in the ejaculate after a median of 7 months in 80% of azoospermic men (Borgress et al)
-
»Offer therapy 6 months prior to planned fatherhood
-
»Consider using hMG instead of FSH to reduce cost and ensure compliance
-
»Consider that treatment may have to be given for longer periods of 12 to 18 months
-
»Not beneficial in men with normal gonadotropin levels
-
»
3.1.3 Anti–estrogen therapy–CC/Tamoxifen
CC Clomiphene citrate (CC) 25 mg or Tamoxifen 20 mg for 6 months. Tamoxifen is preferred to CC as it exerts a weaker estrogenic action
Most results controversial with some studies report benefit, while others do not
Establishment of clear–cut guidelines for use necessary
3.1.4 Aromatase inhibitors
High estrogen levels in combination with low testosterone levels impair proper spermatogenesis as elevated levels of E2 lead to feedback inhibition of the HPG axis, thus decrease LH, which is necessary for the production of testosterone, and FSH to optimize sperm production. Anastrozole 1 mg daily, or letrozole 2.5 mg daily increase testosterone, decrease estrogen levels, and inhibit the peripheral metabolism of testosterone. It is this effective in restoring LH, FSH, and testosterone levels, improving semen parameters, and re–establishing fertility
3.1.5 Androgens
3.1.5.1 Mesterolone
Suppress tubular testicular function resulting in temporary oligospermia or azoospermia allowing function to rebound after treatment is stopped. No benefit reported and therefore not used
3.1.5.2 Testosterone undecanoate
-
To promote androgen bioactivity in epididymis and in accessory glands as it results in amplification in bioavailability of DHT in peripheral blood
-
»Not used any more as it can lower FSH & LH & thus inhibit spermatogenesis by negative feedback mechanism.
-
»According to Anne Jecquier (male infertility, 2003) 6–10 injections of testosterone administered daily can render a normospermic male, azoospermic
-
»
Do not offer testosterone replacement for treatment of male infertility
Testosterone replacement therapy (TRT) should be provided for symptomatic patients with primary and secondary hypogonadism who are not considering parenthood
Offer TRT in Late-onset hypogonadism (LOH) (andropause) and in hypogonadism for steroidogenesis
3.1.6 Food and vitamin supplementation
Carnitine, zinc, folic acid, astaxanthin, vit C, vit E, COQ may improve male infertility
Direct effect on sertoli cells & epididymal function and improves spermatogenesis
Involved in cellular respiration, improving motility, and preventing oxidative stress
The Table 4 below gives the overview of management of male sub–fertility
Table 4.
Overview of management of male sub–fertility
| Medical treatment | Surgical treatment | Assisted reproduction | Third part reproduction |
|---|---|---|---|
| GnRh | Varicocele ligation | IUI | Donor insemination |
| Gonadotropins | Microsurgical repair of vasal obstruction | IVF | Adoption |
| Anti-estrogen therapy–CC, Tamoxifen | Epididymal obstruction | ICSI | |
| Androgens–Mesterolone and testosterone | Transurethral resection of the ejaculatory ducts (TURED) | TESA–ICSI | |
| Sperm Vitalizers: l–carnitine, CoQ10 |
CC: clomiphene citrate;TESA: testicular sperm aspiration; ICSI: intracytoplasmic sperm injection; IUI: intrauterine insemination; IVF: in vitro fertilization
3.1.7 Other endocrinopathies and systemic diseases
Thyroid, adrenal, hypothalamus, and pituitary
Diabetes, hypertension, renal disease, and malignancy
Antibiotics for genital tract infection
3.2 Management of oxidative stress (OS)–related infertility
3.2.1 Lifestyle management is considered as the first and main treatment of OATS
-
In >80% of males, medical treatment is ineffective. Consider the following general measures:
-
»Lifestyle modification (smoking, poor diet, alcohol, obesity, stress)
-
»Minimize environmental exposure to heat, pollutions, and toxins
-
»Control diabetes, hypercholestremia, and weight reduction
-
»Avoid activities heating the scrotum
-
»Proper ventilation/use of personal protective equipment to reduce exposure to chemicals/metals linked with OS
-
»Direct treatment of the underlying stimulus for sperm OS. For example, antibiotic treatment infection
-
»Surgery–Varicocele ligation or the use of TESA ICSI improve sperm DNA quality
-
»Vitamin and antioxidant supplements and food supplementation, with or without the addition of anti–inflammatory medications to decrease leukocyte ROS production
-
»Optimize laboratory procedures
-
»Minimization of iatrogenic OS by limiting semen centrifugation time and avoidance of use of cryo–preserved sperm if possible
-
»
3.3 Management of high DFI
3.3.1 What can be done to avoid iatrogenic sperm DNA fragmentation?
Short abstinence periods (1 day) and serial ejaculation
Patients should be instructed to deliver specimens just before performing ART
Sperm sample should be processed as soon as possible
Incubation time after processing should not exceed 4 hours
Thawing of cryopreserved specimens should be done just before performing ART
Use of testicular sperm should be considered in preference to ejaculated sperm
3.4 Management of high sperm DFI (Figure 1)
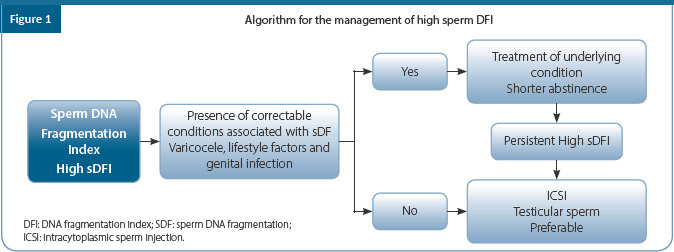
3.4.1 Evidences on sperm DNA damage with ejaculated sperm vs. testicular sperm
Sperm DNA damage is reported to be higher in ejaculated sperm as compared to testicular sperm. DNA damage occurs during transit through epididymis due to ROS which are released from leukocytes, immature sperms, or by dysfunctional mitochondrial metabolism
SDF levels measured by TUNEL assay were found to be lower in testicular sperm as compared to ejaculated sperm. Using testicular sperm in ICSI (44.4%) also led to higher pregnancy rate as compared to ejaculated sperm (23%)
When 81 testicular sperm cycles were compared with 91 ejaculated sperm cycles in couples where male partner had OATS with high SDF (as measured by SCD method). The birth weight was significantly higher and the miscarriage rate was significantly lower in the testicular group
3.5 Medical treatment in leucocytospermia
-
Leucocytospermia is characterized by pus cells >1 X 106
-
»Neutrophil granulocytes need to be differentiated from round cells and immature sperm cells and hence a stained smear is needed
-
»
-
The WHO cutoff is 1 X 106
-
»Many authors Agarwal et al, Cleaveland Clinic–2014 have challenged the value and suggested the lower cutoff 1 to 1
-
»
Occurs usually due to prostatitis/seminal vesiculitis (as per WHO criteria). i.e., accessory gland infection
Bacteriospermia may or may not be present
Consider performing semen culture
Leucocytospermia causes production of ROS and free radicals which causes sperm DNA fragmentation and reduces sperm motility
Common organisms involved are E. coli, urea plasma, Chlamydia, Klebsiella, and Pseudomonas.
Antibiotics used – Doxycycline, auinolones, Mikacin, azithromycin
It is an important cause of OATS hence needs to be treated
Results of treatment are satisfactory and results in increased sperm count and motility
Offer antibiotic therapy in combination with antioxidant treatment
Offer antibiotics for minimum 15 to 21 days. Dose of antibiotic should be according to body weight
Table 5.
Main antibiotics and their eradications rates
| Antibiotic | Eradication rate (%) |
|---|---|
| Ciprofloxacin | 40–77 |
| Levofloxacin | 75 |
| Azithromycin | 80 |
| Doxycycline | 77 |
| Clarithromycin | 80 |
| Azithromycin + ciprofloxacin | 62–77 |
3.6 Medical treatment in hyperprolactinemia
Consider MRI to rule out pituitary microadenoma for levels above 100 ng/ml
High prolactin levels inhibit GnRh
Offer bromocriptine 2.5–5 mg/day for 1–3 months or cabergoline 1 mg/week or 0.5 mg/twice a week for 1–3 months
Monitor PRL levels
3.7 Medical treatment in immunologic infertility
Characterized by immotile sperms or agglutinated sperms
May benefit with intrauterine insemination (IUI) and assisted reproductive treatment (ART)
3.8 Erectile dysfunction
PDE5 inhibitors such as sildenafil–viagra, tadalafil–Cialis, vardenafil-Levitra or udenafil–Udezire
3.9 Situational anejaculation
Offer simple methods like comfortable room, getting the sample from home, accompaniment of the partner, masturbation with visual stimulation, silastic condoms, use of stimulants like sildenafil, and vibrators to treat and prevent it
3.10 Ejaculatory dysfunction (ED)
Ejaculatory dysfunction is the inability of a man to efficiently ejaculate semen from the penis at the moment of sexual climax
Ejaculatory dysfunction is the most prevalent form of male sexual dysfunction and is a common cause of male infertility
Ejaculatory dysfunction is classified into four types: premature ejaculation, delayed ejaculation, retrograde ejaculation and anejaculation (no ejaculation)
Treatments for ejaculatory dysfunction include medications, behavioral therapy (for premature ejaculation) and sometimes surgery
Behavioral therapy (pause, squeeze, stop, and start)–masters and Johnsons exercises
-
Topical treatment with xylocaine and prilocaine spray
-
»Drug treatment with tramadol, dapoxetine, clomipramine, and other SSRI
-
»
3.11 Retrograde ejaculation
Occurs when the semen enters the bladder instead of coming out through the urethra during orgasm
3.11.1 Diagnosis
It is diagnosed when the patient gets dry orgasm and the antegrade ejaculate is minimal or absent
Urine may be cloudy after orgasm due to semen
Post orgasm urine shows presence of sperms
It is usually harmless but maybe the cause of male infertility
3.11.2 Treatment
Treatment is not always necessary and many people live with this problem with normal sex life.
Consider treatment when the resulting male infertility becomes an issue
Drugs are available for toning the internal sphincter (Table 6 below); however, drugs may not work and have a number of side effects
Table 6.
Drug treatment for retrograde ejaculation
| Generic name | Dose | Frequency |
|---|---|---|
| Pseudoephedrine | 120 mg | 90 min prior to ejaculation |
| Pseudoephedrine | 60 mg | 4x daily x 2 days prior to ejaculation |
| Imipramine | 20–50 mg | Daily for 1 month |
| Phenylephrine | Nasal | 1–2 hours prior to ejaculation |
| Ephedrine | 30–60 mg | 1–2 hours prior to ejaculation |
| Ephedrine (inhalers) | 1–2 hours prior to ejaculation | |
| Chlorpheniramine | Twice daily x 1 month | |
| Bromopheniramine | Twice daily x 1 month |
3.11.3 Harvesting sperms to restore fertility in retrograde ejaculation
Administer oral alkalinizing agents to alkalize the urine
Urine is collected by voiding or catheterization immediately after an orgasm
Concentrate the sperms by centrifugation and maybe used for IUI, in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI)
ICSI is the procedure of choice in case of sperms retrieved from patients with retrograde ejaculation
3.12 Management of non-obstructive azoospermia (NOA)
Hypergonadotropic hypogonadism or eugonism
FSH raised, testosterone low or normal
There is an imbalance between circulating testosterone and estrogen with an altered (low) T/E ratio <10
Administration of aromatase inhibitor for 2–3 months prior to retrieval can result in significant improvement in T/E ratio and subsequent retrieval rates in both TESE and micro TESE
3.13 Antioxidants in the management of Male sub-fertility
-
Two types on the basis of their actions
- Preventive anti–oxidants are metal chelators or binding proteins, such as lactoferrin and transferrin, which prevent the formation of ROS
- Scavenging antioxidants, like vitamins C and E, remove the ROS that is already present
Table 7 highlights the type of antioxidants used for management of male sub-fertility
Table 7.
Types of antioxidants used in male sub-fertility management
| Enzymatic antioxidants | Non-enzymatic antioxidants | Other antioxidants |
|---|---|---|
| Glutathione reductase and glutathione peroxidase | Vitamin E | Albumin |
| Vitamin C | Taurine/hypotaurine | |
| Carnitine | ||
| Superoxide dismutase | Carotenoids | Inositol |
| Cysteines | Selenium | |
| Catalase | Pentoxifylline | Zinc |
| Astaxanthin | Coenzyme Q10 |
Key points on anti-oxidant therapy
Proper dose should be administered to prevent pro–oxidant effect resulting in an abrupt fall in sperm motility and viability and an increase in lipoperiroxidation
High doses of vitamin C may cause kidney stone formation and therefore should be given with caution
4. Surgical management
4.1 Varicocele
Varicocele associated with substantial risk of deteriorating testicular function
Consider operating the palpable varicoceles with male sub fertility
Efficacy of varicocelectomy as a treatment is controversial but beneficial in severe and symptomatic cases
Microsurgical varicocelectomy comes nearest to being the ideal operation and is the gold standard
Do not offer treatment for varicoceles in infertile men who have normal semen analysis and in those with subclinical varicocele
Offer treatment for varicoceles in adolescents with progressive failure of testicular development documented by serial clinical examination.
Varicocele and azoospermia
Varicocele is present in 5%–10% of azoospermic men
Do not suggest surgery for all
Varicocele ligation is effective in NOA only in cases of late maturation arrest and hypospermatogenesis and ineffective in early maturation arrest and SCO (sertoli cell only syndrome)
Post varicocelectomy, sperms in ejaculate may be found in 21%–50% of patient and TESE may be avoided
4.2 Surgical sperm retrieval (SSR)
4.2.1 Goals of SSR
Minimal damage to reproductive tract, there by reserving chances for repeat retrieval attempts
To obtain good quality sperm for immediate use for ICSI + cryopreservation
To preserve Leydig cell function & avoid LOH
The different sperm retrieval techniques are highlighted in Tables 8 and 9
Table 8.
Sperm retrieval techniques
| Open biopsy | MESA | TESE |
|---|---|---|
| Percutaneous | PESA | TESA |
| PESE | Percutaneous biopsy | |
| TEFNA | ||
| Mapping |
MESA: microsurgical epididymal sperm aspiration; PESA: percutaneous epididymal sperm aspiration; TESA: Testicular Sperm Aspiration, TEFNA:Testicular Fine-Needle Aspiration.
Table 9.
Indications for sperm retrieval techniques
| Technique | Acronym | Indications |
|---|---|---|
| Percutaneous epididymal sperm aspiration | PESA | Obstructive azoospermia (OA) |
| Microsurgical epididymal sperm aspiration | MESA | OA |
| Open epididymal fine–needle aspiration | Not defined | OA |
| Percutaneous testicular sperm aspiration; percutaneous testicular fine–needle aspiration | TESA; TEFNA | Obstructive azoospermia, Failed epididymal retrieval in OA cases; Epididymal agenesis in CAVD cases; Favorable testicular histopathology1 in NOA cases; Previous successful TESA/TEFNA attempt in NOA cases |
| Testicular sperm extraction (single or multiple biopsies) | TESE | Obstructive azoospermia; Failed epididymal retrieval in OA cases; Failed TESA/TEFNA in OA cases; Non–obstructive azoospermia |
| Single seminiferous tubule biopsy | Not defined | Obstructive azoospermia; Failed epididymal retrieval in OA cases; Failed TESA/TEFNA in OA cases; Non–obstructive azoospermia |
| Microsurgical testicular sperm extraction | Micro-TESE | Non-obstructive azoospermia |
MESA: microsurgical epididymal sperm aspiration; NOA: non-obstructive azoospermia; PESA: percutaneous epididymal sperm aspiration; TESA: Testicular Sperm Aspiration, TEFNA:Testicular Fine-Needle Aspiration.
4.2.2 SSR-in NOA
Efficiency of sperm retrieval in non-obstructive azoospermia (NOA) depends on method of sperm collection
If TESA fails, then TESE should be avoided because of chance of hematoma and increased bleeding
TESE may be done on the opposite side
Micro TESE is a better technique
TESE has a better successful retrieval rates (SRR) than TEFNA (testicular fine–needle aspiration)
4.3. Micro TESE
Micro TESE is based on the premise that potential areas of spermatogenesis are present even in the smallest of testes and even in cases of high FSH
-
Indications
-
»Hypovolemic testis ( <10 cc), small gonads
-
»Repeated negative outcome in routine TESE
-
»Klinefelter syndrome
-
»Hypogonadotropic hypogonadism
-
»Torsion testis, damaged testis
-
»
4.3.1 Micro TESE in NOA
The reported micro TESE retrieval rate range from 35%–77%
Multiple controlled studies demonstrated that micro TESE performs significantly better than TESA or TESE with minimal damage to testicular tissue
Micro TESE is more effective in SRR in men with testicular volume of <10 ml (42% vs. 27%)
Up to 37% of success rate was achieved when operating time was increased from 2 hours to 4 hours
SRR with TESA and micro TESE is comparable when testicular volume is more than 10 ml, hence TESA, TESE is first choice in such cases
4.4 Surgical reconstruction procedures in obstructive azoospermia
-
Treatment of obstructive azoospermia
-
»Microsurgical repair of vasal obstruction: patency rate of 80% and conception rate of 40%
-
»Epididymal obstruction: low success rate
-
»Low volume ejaculate and severe oligozoospermia: Transurethral resection of the ejaculatory ducts (TURED)
-
»
Extremely cost effective in carefully selected cases in centers of microsurgical excellence
In obstructive azoospermia (OA) and microsurgery is restricted to vasovasal anastomosis and TURED
4.5 Retrieval vs. reconstruction
Better pregnancy rates are achieved with sperm retrieval technique with ICSI than following reconstructive surgery. However, this is more expensive and has a single event impact
Reconstructive surgery is cheaper in the long run and has a multiple event impact
-
Retrieval is preferred to reconstruction because of the following reasons:
-
»Even after reconstruction the sperm count and motility remains low
-
»Late surgical failures are known
-
»There is a chance of antibody formation
-
»Reverse motility is sometimes seen
-
»Reconstruction requires greater surgical expertise
-
»
4.6 Testicular biopsy
Testicular biopsy should be performed when the information obtained will directly help future therapy or enable sperm retrieval
The testicular tissue should be collected in culture media. Formalin should not be used as it will distort histological features
The tissue should be cut with fine sharp iris scissors
In the era of ICSI and sperm retrieval, diagnostic testicular biopsy has become obsolete:
Every attempt at testicular biopsy produces an area of fibrosis and avascularity which jeopardises further chances of sperm retrieval
Today a testicular biopsy is restricted to a micro biopsy combined with retrieval
Genetic counselling should be done in all cases of azoospermia when sperm retrieval is attempted, in all couples with a genetic abnormality in clinical and genetic investigations and in patients who carry potential inheritable disease.
Consider providing long–term endocrine follow–up for all men with KLFS and androgen replacement therapy, which is considered to be necessary
Men with Yq microdeletion and their partners who wish to proceed with ICSI should be informed that microdeletions will be passed to sons, but not to daughters
Consider using sperm retrieval techniques only when cryostorage of the material obtained is available
Consider genetic counseling needed in CBAV where both the man and his partner carry the CFTR gene mutation
Testicular biopsy and cryopreservation should be performed in all cases of testicular microcalcification (TM), who belong to one of the high risk groups–Infertility, spermatogenic failure bilateral TM, atrophic testes (<12 CC), history of undescended testes, and testicular germ cell tumour (TGCT)
Offer cryopreservation of semen or sperms for all candidates going for chemotherapy, radiotherapy or surgical interventions that might interfere with spermatogenesis or cause ejaculatory disorders
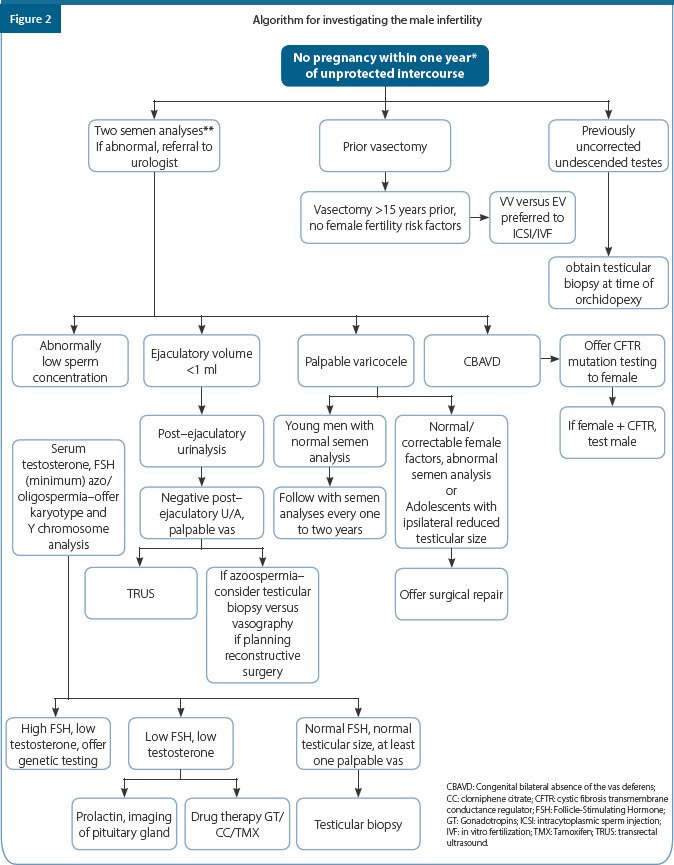
Summary of recommendations
| Category | Recommendation | Grade of evidence | Quality of evidence |
|---|---|---|---|
| CCR | Perform semen analyses according to the guidelines | A | - |
| CCR | Perform further andrological assessment when semen analysis is abnormal in at least two tests | A | - |
| EBR | An initial endocrine evaluation should include at least a serum testosterone and FSH. It should be performed if there is: (1) an abnormally low sperm concentration, especially if less than 10 million/ml; (2) impaired sexual function; or (3) other clinical findings suggestive of a specific endocrinopathy | A | II |
| EBR | Insufficient evidence in the literature to support the routine use of DNA integrity testing in the evaluation and management of the male partner of an infertile couple | B | III |
| EBR | There is insufficient data to support the routine use of reactive oxygen species testing in the management of the male partner of an infertile couple | A | III |
| EBR | For men with OA, NOA, and severe OAT, perform karyotyping and appropriate genetic testing and offer genetic counselling | A | II |
| CCR | Karyotype testing should be performed on all males with severe oligozoospermia (<5×106/ml) or NOA prior to any therapeutic procedure | A | - |
| EBR | Do not test for microdeletions in men with OA when ICSI is used because spermatogenesis should be normal | A | I |
| EBR | Inform men with Yq microdeletion and their partners who wish to proceed with ICSI that microdeletions will be passed to sons, but not to daughters | A | I |
| EBR | In men with structural abnormalities of the vas deferens (unilateral or bilateral absence), test the man and his partner for CFTR gene mutations | A | I |
| EBR | Specialized sperm function tests (tests for anti-sperm antibodies, CASA, sperm cervical mucus interaction) on semen are not required for diagnosis of male infertility. They may be useful in a small number of patients for identifying a male factor contributing to unexplained infertility, or for selecting therapy, such as assisted reproductive technology | B | - |
| CCR | Scrotal ultrasonography is indicated in those patients in whom physical examination of the scrotum is difficult or inadequate or in whom a testicular mass is suspected | B | -- |
| EBR | Use sperm retrieval techniques, such as MESA, TESE, and PESA only when cryostorage facilities of the material obtained is available | B | II |
| EBR | For azoospermia caused by vasal or epididymal obstruction, perform microsurgical vasovasostomy or tubulovasostomy | B | III |
| EBR EBR |
Do not treat varicoceles in infertile men who have normal semen analysis and in men with a subclinical varicocele Treat varicoceles in men with a clinical varicocele, oligospermia and otherwise unexplained infertility in the couple | A A |
II III |
| EBR | Testosterone replacement therapy should be offered only for symptomatic patients with primary and secondary hypogonadism who are not considering parenthood | A | II |
| EBR | Do not use testosterone replacement for the treatment of male infertility | A | II |
| EBR | In men with hypogonadotropic hypogonadism, induce spermatogenesis by an effective drug therapy (hCG/hMG/rFSH) | A | I |
| EBR | If undescended testes are corrected in adulthood, perform simultaneous testicular biopsy for detection of intratubular germ cell neoplasia of unclassified type ( ITGCNU) | B | II |
| EBR | Do not use hormonal treatment of cryptorchidism in adults | A | II |
| EBR | Use medical treatment of male infertility only for cases of hypogonadotropic hypogonadism. | A | I |
| EBR | No recommendation can be made for treatment with gonadotropins, antiestrogens and antioxidants for treatment of idiopathic male infertility | B | II |
| EBR | There are insufficient data to recommend the use of supplemental antioxidant therapies for the treatment of men with abnormal semen parameters and/or male infertility | C | IV |
| EBR | Offer simultaneous sperm cryopreservation if testicular biopsies are performed for fertility diagnosis. | A | I |
| EBR | Offer cryopreservation of semen to all men who are candidates for chemotherapy, radiation or surgical interventions that might interfere with spermatogenesis or cause ejaculatory disorders | A | I |
| EBR | Offer specific treatments for ejaculatory disorders before performing sperm collection and ART | A | III |
| EBR | IVF with or without ICSI may be considered the primary treatment option when such treatment is required to treat a female factor, regardless of the semen parameters | A | I |
| EBR | IVF can be attempted provided that more than approximately 2 million motile sperm can be harvested from an ejaculate, with an expectation of success close to that of IVF for other indications | A | I |
| EBR | ICSI should be offered if there is a chance of failure of fertilization with IVF: Less than 2 million motile sperm per ejaculate, less than 4% of sperm with normal morphology, less than 5% of sperm with progressive motility, sperm autoimmunity, and defects of sperm-oocyte interaction | A | I |
References
Agarwal A, Cho CL, Esteves SC, Majzoub A. Reactive oxygen species and sperm DNA fragmentation. Translational Andrology and Urology. 2017 Sep;6(Suppl 4):S695.
Aitken RJ. Oxidative stress and the etiology of male infertility. Journal of assisted reproduction and genetics. 2016 Dec 1;33(12):1691-2.
Baazeem A, Belzile E, Ciampi A, Dohle G, Jarvi K, Salonia A, Weidner W, Zini A. Varicocele and male factor infertility treatment: a new meta-analysis and review of the role of varicocele repair. European urology. 2011 Oct 1;60(4):796-808.
Belker A. Vasectomy reversal. In Andrology for the Clinician 2006 (pp. 119-121). Springer, Berlin, Heidelberg.
Calogero AE, Condorelli RA, Russo GI et al. Conservative Nonhormonal Options for the Treatment of Male Infertility: Antibiotics, Anti-Inflammatory Drugs, and Antioxidants. Biomed Res Int. 2017;2017:4650182.
Castillo J, Amaral A, Oliva R. Sperm nuclear proteome and its epigenetic potential. Andrology. 2014 May;2(3):326-38.
Coccia ME, Becattini C, Criscuoli L, Fuzzi B, Scarselli G. A sperm survival test and in-vitro fertilization outcome in the presence of male factor infertility. Human reproduction (Oxford, England). 1997 Sep 1;12(9):1969-73.
Esteves SC, Agarwal A. Novel concepts in male infertility. International braz j urol. 2011 Feb;37(1):5-15.
Esteves SC, Miyaoka R, Agarwal A. Sperm retrieval techniques for assisted reproduction. International braz j urol. 2011 Oct;37(5):570-83.
Esteves SC, Roque M, Bradley CK, Garrido N. Reproductive outcomes of testicular versus ejaculated sperm for intracytoplasmic sperm injection among men with high levels of DNA fragmentation in semen: systematic review and meta-analysis. Fertility and sterility. 2017 Sep 1;108(3):456-67.
Esteves SC, Roque M, Garrido N. Use of testicular sperm for intracytoplasmic sperm injection in men with high sperm DNA fragmentation: a SWOT analysis. Asian journal of andrology. 2018 Jan;20(1):1.
Esteves SC. Clinical relevance of routine semen analysis and controversies surrounding the 2010 World Health Organization criteria for semen examination. International braz j urol. 2014 Aug;40(4):433-53.
Jenkins TG, Aston KI, Pflueger C, Cairns BR, Carrell DT. Age-associated sperm DNA methylation alterations: possible implications in offspring disease susceptibility. PLoS genetics. 2014 Jul;10(7).
Jodar M, Selvaraju S, Sendler E, Diamond MP, Krawetz SA, Reproductive Medicine Network. The presence, role and clinical use of spermatozoal RNAs. Human reproduction update. 2013 Nov 1;19(6):604-24.
Kläver R, Gromoll J. Bringing epigenetics into the diagnostics of the andrology laboratory: challenges and perspectives. Asian journal of andrology. 2014 Sep;16(5):669.
Kolettis PN, Thomas AJ Jr (1997) Vasoepididymostomy for vasectomy reversal: a critical assessment in the era of intracytoplasmic sperm injection. J Urol 158:467–470
Lewis SE, Kumar K. The paternal genome and the health of the assisted reproductive technology child. Asian journal of andrology. 2015 Jul;17(4):616.
Lobo N, Satchi M. The diagnosis and management of men with low sperm motility. Trends in Urology & Men’s Health. 2019 Sep;10(5):24-7.
Matthews GJ, Schlegel PN, Goldstein M (1995) Patency following microsurgical vasoepididymostomy and vasovasostomy: temporal considerations. J Urol 154:2070–2073
Milardi D, Grande G, Vincenzoni F, Castagnola M, Marana R. Proteomics of human seminal plasma: identification of biomarker candidates for fertility and infertility and the evolution of technology. Molecular reproduction and development. 2013 May;80(5):350-7.
Munasinghe D, Weerasooriya M, Liyanage J, Wakkumbura H. The Most Common Seminal Parameter Which Could Be Affected In The Males With Fertility Issues. Journal of Medicine and Health Research. 2019 Jul 25:12-6.
Osman A, Alsomait H, Seshadri S, El-Toukhy T, Khalaf Y. The effect of sperm DNA fragmentation on live birth rate after IVF or ICSI: a systematic review and meta-analysis. Reproductive biomedicine online. 2015 Feb 1;30(2):120-7.
Pahune PP, Choudhari AR, Muley PA. The total antioxidant power of semen and its correlation with the fertility potential of human male subjects. Journal of Clinical Diagnostic Research. 2013;7(6):991–995.
Simon L, Emery BR, Carrell DT. diagnosis and impact of sperm DNA alterations in assisted reproduction. Best Practice & Research Clinical Obstetrics & Gynaecology. 2017 Oct 1;44:38-56.
Thomas AJ, Padron OF. Obstructive azoospermia and vasoepididymostomy. In Male Infertility and Sexual Dysfunction 1997 (pp. 244-257). Springer, New York, NY.
Wang C, Swerdloff RS. Limitations of semen analysis as a test of male fertility and anticipated needs from newer tests. Fertility and sterility. 2014 Dec 1;102(6):1502-7.
Chapter 7: Management of Pelvic Infections and Pathologies
OVERVIEW
This guideline offers recommendations on the diagnostic tests, treatment regimens, and health promotion principles needed for the effective management of pelvic inflammatory disease (PID) covering the management of the initial presentation, as well as how to reduce transmission and future infection. It is aimed primarily at women aged 16 years or older presenting to health care professionals.
1. Introduction
Pelvic infection is one of the most common, serious infections in non–pregnant women of reproductive age
-
Goals of the therapy include:
-
»Resolution of clinical symptoms and signs
-
»Eradication of pathogens from the genital tract
-
»Prevention of sequel including infertility, ectopic pregnancy, and chronic pelvic pain
-
»Prevention of recurrence
-
»
Neisseria gonorrhea and Chlamydia trachomatis (C. trachomatis) have been identified as the causative agents. C. trachomatis is the commonest identified cause accounting for 14%–35% of cases, whilst Gardnerella vaginalis, anaerobes and other organisms commonly found in the vagina may also be implicated. Mycoplasma genitalium has been associated with upper genital tract infections in women and is a very likely cause of PID. Pathogen negative PID is common. Genital tuberculosis is one of the causes of PID in India
2. Factors associated with PID
2.1 Factors related to sexual behavior
Young age not using barrier contraception, having multiple partners, recent new partner (within previous 3 months), past history of sexually transmitted infections (STIs) in the patient or their partner
2.2 Instrumentation of the uterus/interruption of the cervical barrier
Termination of pregnancy, insertion of intrauterine device within the past 6 weeks, hysterosalpingography, in vitro fertilization (IVF), intrauterine insemination (IUI), hysteroscopy
2.3 Genital tuberculosis
Genital tuberculosis (GTB) is a chronic disease with low–grade symptoms. Mycobacterium reaches the genital tract by hematogenous spread from the foci, lungs being the most common primary focus
Presenting symptoms are infertility, menstrual irregularities, chronic pelvic pain, and abnormal vaginal discharge
Organ involvement in GTB involves fallopian tubes, 90%–100%; endometrium, 50%–80%; ovaries, 20%–30%; and the cervix, 5%–15%
2.3.1 Fallopian tubes
The infection in tuberculous endosalpingitis with the hematogenous route of spread starts from endosalpinx making tubes swollen, edematous, and irregular with the formation of hydrosalpinx, pyosalpinx, tubo–ovarian masses, and dense adhesions
The infection in tuberculous exosalpingitis starts in the muscularis mucosa of oviducts with hyperemia, flimsy adhesions, and miliary tubercles on the surface of the tubes. Beading, closed tubes, tubo–ovarian masses, hydrosalpinx, pyosalpinx, and the development of synechiae formation occurs later
2.3.2 Ovaries
Ovaries are affected in 20%–30% of the patients with adhesions, caseation, adnexal cyst, or mass formation with defective ovarian function and reserve, and sometimes complete destruction of ovary
Tubo–ovarian cyst can sometimes manifest as an acute abdomen simulating acute appendicitis and may be diagnosed on laparoscopy or laparotomy
2.3.3 Peritoneum
Various types of adhesions are formed in the pelvis and abdomen, such as perihepatic synechiae (Fitz-Hugh-Curtis syndrome), hanging gallbladder sign and ascending colonic synechiae and frozen pelvis in the abdomino–pelvic tuberculosis
3. Clinical features
3.1 Acute PID staging
3.1.1 Centre of Disease Control (CDC) diagnostic criteria
-
Presence of one or more of the following minimum clinical criteria on pelvic examination:
-
»Lower abdominal tenderness
-
»Adnexal tenderness
-
»Cervical movement
-
»
-
One or more of the following additional criteria can be used to enhance the specificity of the minimum clinical criteria and support a diagnosis of PID:
-
»Oral temperature >38.3 °C
-
»Abnormal cervical or vaginal discharge
-
»Elevated erythrocyte sedimentation rate
-
»Elevated C–reactive protein
-
»
Laboratory documentation of sexually transmitted diseases (STDs) is recommended
Definitive criteria for diagnosis of PID
Histopathological evidence of endometritis on endometrial biopsy (curatage not recommended)
Tubo–ovarian abscess on sonography or other radiological test
Laparoscopy abnormality consistent with PID
3.2 Stages
Stage 1
Women who fulfill the Centers for Disease Control and Prevention (CDC) major diagnostic criteria and ≥1 of its minor criteria, but who do not have overt peritonitis and who do not have prior documented STD upper track infections
Stage 2
The above said criteria plus peritonitis
Stage 3
Women with demonstrable tubo–ovarian complex or tubo–ovarian abscess evident on physical or ultrasonographic examination
Stage 4
Women with ruptured tubo–ovarian abscesses
4. Investigations
Complete blood count
C–reactive protein
Erythrocyte sedimentation rate
Test for syphilis
Test for human immunodeficiency virus (HIV)
Urine pregnancy test
Urine analysis
Urine culture
4.1 Vaginal wet mount
Presence of white blood cells (WBC) suggests PID but their presence is nonspecific, whereas absence of WBCs has a good negative predictive value.
Cervical chlamydia and gonorrhea testing for organisms if facilities are available
4.2 Imaging
Consider chest x-ray in suspected cases of GTB (genital tuberculosis). Active pulmonary TB (fibrocavitory disease, infiltrations, mediastinal or hilar lymphadenopathy, miliary tuberculosis) or old healed lesions of past TB can be detected with chest x-ray
-
Consider ultrasonography (USG) to investigate:
-
»Tubo–ovarian masses
-
»Fluid in pouch of Douglas
-
»Hydrosalpinges
-
»Heterogeneous or thin endometrium
-
»Endometrial fluid
-
»Intrauterine synechiae
-
»
Computerized axial tomography scan can be considered to diagnose masses in the abdomen and pelvis with ascites, thickened and enhanced peritoneum, with lesions in the abdominal viscera and lymph nodes
Higher resolution obtained with magnetic resonance imaging (MRI) can be considered to show presence of tubo–ovarian masses
Hysterosalpingography (HSG) can be considered as a part of infertility evaluation. HSG shows evidence of GTB in the form of tubal occlusion, diverticula, pouching, hydrosalpinx, and multiple constrictions
HSG findings of uterine tuberculosis include irregular margins, filling defects, and signs of intra uterine synechia
HSG should be avoided in women with acute infection
4.3 Blood test
Full blood count is considered to diagnose anaemia, raised leucocytes and lymphocytes, and raised ESR in tuberculosis
Serological tests are not considered sensitive and specific
4.4 Microbiological tests
Consider endometrial biopsy, curettage or aspirate performed in the luteal phase (day 21) for the diagnosis of G TB
Perform the WHO approved rapid diagnostic tests (WRDT) which are cartridge based nucleic acid amplification test (CBNAAT/GeneXpert MTB/RIF) and liquid culture by mycobacterial growth indicator tube (MGIT) on endometrial sample sent in saline and histopathology (available in all government hospital free of charge)
High false positivity of polymerase chain reaction (PCR) is reported. Avoid starting antitubercular treatment (ATT) only on positive PCR unless there is evidence of FGTB (female genital tuberculosis) clinically on examination, or on radiology or endoscopy. A positive CBNAAT (cartridge based nucleic acid amplification test) result is a useful confirmation
4.5 Diagnostic laparoscopy
-
»
Consider laparoscopy and look for typical findings of tubal congestion, hydrosalpinx, rigid tubes, and tubercles on the surface
-
»
During a diagnostic laparoscopy, consider taking a biopsy, or perform drainage, removal of hydrosalpinx and tubo-ovarian masses
5. Complications requiring admission to hospital
-
The three reported complications of PID are:
-
»Acute/chronic pelvic pain
-
»Infertility
-
»Ectopic pregnancy
-
»
Approximately 25% of patients with a history of PID may suffer from chronic pelvic pain, which is related to cyclic menstrual changes, but it also may be the result of adhesions or hydrosalpinx
Note that PID may produce tubo–ovarian abscess (TOA) and may progress to peritonitis and Fitz–Hugh−Curtis syndrome (perihepatitis)
It is important to note a rare but life–threatening complication of acute rupture of a TOA may result in diffuse peritonitis and necessitate urgent abdominal surgery
Ectopic pregnancy should be ruled out
In women with immunosuppression secondary to HIV, symptoms associated with PID may be more severe, but may respond well to standard antibiotic therapy
Note the right upper quadrant pain associated with perihepatitis with the Fitz–Hugh Curtis syndrome
6. Differential diagnoses
Ectopic pregnancy, acute appendicitis, endometriosis, complications of an ovarian cyst, urinary tract infection, irritable bowel syndrome, functional pain
Tuberculosis is suspected if there is no response to the initial management
7. Management
7.1 General measures
Advise rest for those with severe disease, offer appropriate analgesia
Offer intravenous therapy for patients with more severe clinical disease such as pyrexia >38°C, clinical signs of tubo–ovarian abscess, or signs of pelvic peritonitis
Advise patients to avoid intercourse to avoid reinfection, until they and their partner(s), have completed the treatment
Outpatient therapy is as effective as inpatient treatment for patients with clinically mild to moderate PID
-
Choice of treatment regimen should be influenced by following:
-
»Offer oral therapy for mild and moderate cases as outpatients
-
»Offer intravenous therapy, which should be continued until 24 hours after clinical improvement and switched to oral therapy
-
»
Arrange all the investigation as appropriate, ensure that sexual partner is treated
-
Prescribe drug treatment, such as:
-
»Ibuprofen/paracetamol to provide pain relief
-
»Empirical antibiotics as soon as presumptive diagnosis of PID is made clinically
-
»Screen women for STI before starting antibiotics
-
»Manage sexual partner of women appropriately
-
»
In women with intrauterine contraceptive (IUD or levonorgestrel system present with PID)
Consider removal of the device if patient request or if symptoms do not resolve within 72 hour after a review of 48–72 hours in situ
Offer emergency hormonal contraception if the device is removed
7.2 Antibiotics
7.2.1 First line regimens
If risk of gonococcol infection is low
-
Offer ceftriaxone 1 gm as a single intramuscular dose followed by oral doxycycline 100 mg twice daily plus oral metronidazole 400 mg twice daily for 14 days
or
Offer ceftriaxone 1 gm intramuscular followed by oral ofloxacin 400 mg twice daily plus oral metronidazole 400 mg twice daily for 14 days
-
If none of the above first line regimen is suitable then alternative regimen
-
»Offer ceftriaxone 1 gm as a single intramuscular dose followed by oral azithromycin 1 gm per week for 2 weeks, but there is less evidence to support this
-
»
-
If risk of gonococcal infection is high
-
»Offer ceftriaxone 1 gm as a single intramuscular dose followed by doxycycline 100 mg twice daily plus oral metronidazole 400 mg twice daily for 14 days
-
»Do not recommend azithromycin for gonococcal PID
-
»Do not recommend the regimen of doxycycline and metronidazole without intramuscular ceftriaxone
-
»Do not replace intramuscular ceftriaxone with oral cephalosporin
-
»Offer same treatment for women infected with HIV as those of not infected with HIV
-
»
7.2.1.1 In-patient regimens
Offer ceftriaxone 2 gm IV/IM once daily, doxycycline 100 mg twice daily (oral doxycycline may be used if tolerated) followed by oral doxycycline 100 mg twice daily plus oral metronidazole 400 mg twice daily to complete 14 days
Offer clindamycin 900 mg IV three times a day plus IM/IV Gentamicin (3–6 mg/kg as a single daily dose with renal monitoring)
-
This may be followed by either:
-
»Oral clindamycin 450 mg four times daily for 14 daysor
-
»Oral doxycycline 100 mg twice daily plus oral metronidazole 400 mg twice daily for 14 days
-
»
7.2.1.2 Alternative regimen
-
Offer ofloxacin 400 mg IV twice daily plus IV metronidazole 500 mg three times daily for 14 days
or
Offer ceftriaxone 500 mg intramuscular single dose plus oral azithromycin 1 gram single dose followed by a second dose of oral azithromycin 1 gram after one week
7.3 Surgical management
Reevaluate for possible laparoscopic or surgical intervention in patients who do not improve in 72 hours and reconsider for other possible diagnoses
Perform laparoscopic pelvic lavage, abscess drainage, and adhesion lysis when necessary
USG guided or CT guided drainage may be considered under appropriate circumstances
Most TOAs (60%–80%) resolve with antibiotic administration
Reserve laparotomy for patients experiencing surgical emergencies (abscesses that have ruptured or that have not responded to medical management and laparoscopic drainage) and for patients who are not candidates for laparoscopic management. Consider guiding the treatment by intraoperative findings and the patient’s desire for fertility maintenance
Discuss various surgical treatment options, such as unilateral or bilateral salpingo-oophorectomy or hysterectomy. Perform the operation after the acute infection and inflammation have resolved. In patients with recurrent PID, dense pelvic adhesions may render surgery difficult
Infertility patients presenting with hydrosalpinx, perform a salpingectomy before ART to achieve better outcomes
7.4 Treatment of genital tuberculosis
-
Offer first–line drugs in combination:
-
»Four drugs isoniazid (H), rifampicin (R), pyrazinamide (Z), and ethambutol (E) for two months (HRZE), followed by H, R and E (HRE) daily for four months
-
»Thrice–weekly regimen is no longer used
-
»
In patients with advanced stage with scarring, severe fibrosis, and adhesions, treatment outcomes especially for infertility are poor. Offer early diagnosis and correct treatment to avoid complications and to restore fertility in such patients
7.5 Managing sexual partner
Contact the current and recent partner of women within last 6 months and offer advice, screening, treatment, and contact tracing
Offer screening for chlamydia and gonorrhea
Offer empirical treatment with broad spectrum antibiotic while waiting for result
Suggest abstinence for both the partner till the disease is cured
Discuss the use and offer barrier methods, and broad spectrum empirical treatments to all male partners
7.6 Advice to women
Provide advice to women to complete the course, screen for other sexually transmitted infections, the need for contact tracing and treat other partner
Discuss about risk of ectopic pregnancy, infertility, chronic pelvic pain, even if fertility is maintained
Discuss about severe, recurrent attacks and lack of proper treatment, contraceptive (dual contraception barrier with any other contraception), additional information about PID, that may compromise fertility
7.7 Follow up in women after PID treatment
-
Consider follow–up of women within 72 hours, If there is:
-
»No clinical improvement (decrease in tenderness) –consider admission, check antibiotic sensitivity from swab test, and adjust antibiotic treatment if necessary
-
»
Consider review after 2–4 weeks–confirm response of treatment, confirm sexual contact has been screened and treated, discuss the potential sequel of PID
At follow-up perform
Routine repeat testing after 2–4 weeks if initial testing for chlamydia was positive
Test of cure if initial testing for gonorrhea was positive.
-
Repeat testing after 3–5 week if possibility of persisting infection or recurrent infection is present
-
»Repeat testing after 4 weeks if initial test for Mycoplasma genitalium is positive
-
»
Repeat testing if symptoms persist, and during the presence of antibiotic resistance, poor compliance, possibility of reinfection, or if sensitivity testing is not done
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CCR | Clinical criteria for diagnosis of PID | C | - |
| CCR | Pain on cervical movements or in posterior or lateral fornices | C | - |
| CCR | Oral temperature >101° F (38.3 °C >) | B | - |
| CCR | Mucopurulent cervical discharge or abnormal vaginal discharge | C | - |
| CCR | Pain associated with fever and mucopurulent cervical or vaginal discharge Complex tubo-ovarian mass at ultrasound | B | - |
| Laboratory criteria for diagnosis of PID | |||
| CCR | The presence of abundant numbers of white blood cells (leukocytes) on saline microscopy of vaginal secretions | C | - |
| CPP | Elevated erythrocyte sedimentation rate | - | - |
| EBR | High C–reactive protein | B | III |
| CCR | Acute or chronic salpingitis or endometritis in histological evaluation of biopsy | B | - |
| EBR | demonstrates integration N. gonorrhoeae or C. trachomatis in the genital tract | B | II |
| EBR | Diagnostic laparoscopy or laparotomy for PID | C | II |
| EBR | Isolation of pathogenic bacteria from a bacterial specimen from the upper genital tract | B | II |
| EBR CPP CPP CPP CPP |
Laparoscopy has substantial value in the confirmation of the diagnosis of PID but is not sensitive enough to be considered a gold standard of diagnosis. Is required when • The symptomatic patient with high suspicion of other pelvic pathologies like ectopic pregnancy, ovarian cyst, endometrioma, ovarian torsion, appendicitis, cholecystitis, constipation, gastroenteritis, inflammatory bowel disease, perforated peptic ulcer, acute pancreatitis, Meckel diverticulitis, intestinal obstruction • Woman with the acute disease, which did not respond to outpatient treatment to PID • Any patient showing no improvement after approximately 72 h of hospital treatment to PID Laparoscopic abnormalities consistent with PID include erythema, edema, tubal adhesions, purulent exudate or purulent fluid in POD |
B - - - - |
II - - - - |
| Diagnostic Tests | |||
| CCR | Pregnancy test | B | - |
| EBR | Microscopic examination of vaginal discharge in saline solution | B | III |
| CPP | Complete blood count | - | |
| CCR | Nucleic acid amplification tests for C. trachomatis and N. gonorrhoeae | - | II |
| CPP | Urine test | B | - |
| EBR | C-reactive protein | - | II |
| EBR | HIV tests | A | II |
| EBR | Surface antigen and hepatitis B surface antibodies | A | II |
| EBR | Test for syphilis. | B | II |
| CCR | Ultrasound of pelvis and abdomen using both trans vaginal and transabdominal | B | |
| CCR | route | C | III |
| EBR | MRI in indicated cases | B | II |
| EBR | Endometrial biopsy with histopathological evidence of endometritis Laparoscopy | B | II |
| Treatment | |||
| CPP | • Rest, hydration, and sexual abstinence during treatment | - | - |
| CPP | • Symptomatic treatment–analgesics, antipyretics, and non–hormonal anti–inflammatory drugs | - | - |
| CPP | • Convene partners for clinical evaluation | - | - |
| CPP | • Guidance on the risks of new episodes of PID and other STDs | - | - |
| CPP | • Avoid unprotected sex • Outpatient antibiotic therapy– |
- | - |
| EBR | » Offer ceftriaxone1 gm as a single intramuscular dose followed by oral doxycycline 100 mg twice daily plus oral metronidazole 400 mg twice daily for 14 days | B | III |
| » Offer ceftriaxone 1 gm intramuscular followed by oral ofloxacin 400 mg twice | |||
| EBR | daily plus oral metronidazole 400 mg twice daily for 14 days | B | III |
| » Offer ceftriaxone 1gm as a single intramuscular dose followed by oral azithromycin 1 gm per week for 2 weeks, but there is less evidence to support this | B | III | |
| EBR | • Inpatient antibiotic therapy – indicated when there is lack of response to oral therapy, severe clinical disease, PID complicated with pelvic abscess, possible need for surgical intervention | B | II |
| EBR | • Offer ceftriaxone 2 gm IV/IM once daily, doxycycline 100 mg twice daily (oral doxycycline may be used if tolerated) followed by oral doxycycline 100 mg twice daily plus oral metronidazole 400 mg twice daily to complete 14 days | B | III |
| EBR EBR |
• Offer clindamycin 900 mg IV three times a day plus IM/IV gentamicin (3–6 mg/kg as a single daily dose with renal monitoring) followed by either: Oral clindamycin 450 mg four times daily for 14 days or oral doxycycline 100 mg twice daily plus oral metronidazole 400 mg twice daily for 14 days | B | III |
| EBR | • Surgical treatment is indicated for clinical treatment failure, presence of pelvic mass that persists or increases, despite the clinical treatment, suspected rupture of tube-ovarian abscess; hemoperitoneum or POD abscess | B | II |
| EBR | • In chronic PID with development of hydrosalipinx, either the tube is removed or disconnected from the cornual end to increase the chance of pregnancy | A | I |
| EBR | In Indian context it is important to rule out genital tuberculosis | B | II |
| Follow-up | |||
| EBR | • Review with 72 hours to evaluate clinical improvement. Admit to hospital if there is no substantial improvement | B | III |
| EBR | • Consider review after 4 weeks after therapy to evaluate adequate adherence and response to treatment | B | III |
| EBR | • Screening and treatment of male partner | B | III |
| EBR | • Discuss potential sequelae of PID | C | III |
References
Fifer H, Saunders J, Soni S, et al. British Association for Sexual Health and HIV national guideline for the management of infection with Neisseria gonorrhoeae (2019).
European Guideline for the Management of Pelvic Inflammatory Disease. 2012
Guideline development group, Ross J, Cole M, Evans C, et al. PPI representative United Kingdom National Guideline for the Management of Pelvic Inflammatory Disease (2019 Interim Update)
Pelvic Inflammatory Disease (PID). Centers for Disease Control and Prevention 2015. Available on: https://www.cdc.gov/std/tg2015/pid.htm Assessed on: 20th June 2019
Sharma JB, Sharma E, Sharma S, et al. Female genital tuberculosis: Revisited. Indian J Med Res 2018; 148, Suppl S1:71–83
Hemsel DL, Ledger WJ, Martens M et al. Concerns regarding the Centers for Disease Control’s published guidelines for pelvic inflammatory disease. Clin Infect Dis. 2001; 32(1):103–7.
Chapter 8: Managing Endometriosis –The Indian Perspectives
OVERVIEW
This guideline covers diagnosis and management of endometriosis. It aims to raise awareness regarding the signs and symptoms of endometriosis, and provides clear advice on actions to be taken when women with such signs and symptoms first present in healthcare settings. It also provides advice on the range of treatments available.
1. Introduction
Endometriosis is a benign disease and is defined by the presence of endometrial glands and stroma outside the uterus
Microscopically, the endometrial glands and stroma are seen with hemosiderin-laden macrophages
Prevalence of endometriosis
Endometriosis affects the women from menarche to menopause. The prevalence of endometriosis varies with age and clinical presentation
The prevalence of asymptomatic endometriosis is 1%–7%
The overall prevalence of endometriosis in reproductive aged women is between 3%–10%
Among women in reproductive age group, 12%–32% women with complaint of pelvic pain have endometriosis, and 9%–50% women with infertility have endometriosis
It is estimated that 176 million women all over the world suffer from endometriosis. In India, 26 million is reported to have endometriosis
Association with endometriosis: The reported association is with fibroids (26%), Mullerian anomalies (20%) and ovarian malignancy (1.3%–1.9%)
2. Risk factors, protective factors, and sites for endometriosis
2.1 Various risk factors associated with endometriosis are:
Infertility
Early age at menarche
Shorter menstrual cycle
Heavy menstrual bleeding
Nulliparity
Mullerian anomalies
Diethylstilbestrol exposure
Dioxin exposure
Endometriosis in first degree relative
Prior medical or surgical therapy for endometriosis
2.2 Various protective factors are:
Multiparity
Lactation
Increased body mass index (BMI)
Increased waist–to–hip ratio
Diet high in vegetable and fruit
2.3 Sites of endometriosis
Pelvic
Ovaries
Posterior cul-de-sac
Broad ligament
Uterosacral ligament
Extra pelvic: Abdominal wall, the urinary and gastrointestinal tract, thorax and nasal mucosa
3. Signs and symptoms of endometriosis
Symptoms of endometriosis
Endometriosis can be asymptomatic.
Pain is the most common presenting feature. Patient can present with dysmenorrhea, dyspareunia, and chronic pelvic pain, dysphasia, and disturbances in menstrual cycle
Endometriosis also presents frequently with infertility. Almost 50% women with infertility have endometriosis
Extra pelvic endometriosis
-
»
Colon and rectum is the most common site of extra pelvic disease
-
»
Extra pelvic endometriosis presents as abdominal and back pain, abdominal distension, cyclic rectal bleeding, constipation, and obstruction
Ureteral involvement can lead to obstruction and cyclic pain, dysuria, and hematuria
Pulmonary endometriosis manifests as pneumothorax, hemothorax or hemoptysis during menses
In umbilical endometriosis, umbilical mass is palpated with cyclic pain in umbilical region
Scar endometriosis manifests as cyclic pain and swelling at scar site
Signs of endometriosis
-
External genitalia
-
»Normal or episiotomy scar endometriosis
-
»
-
On per speculum examination
-
»Blue coloured implants or red proliferative lesions
-
»
Pelvic tenderness
Focal thickening, nodularity, and induration of uterosacral ligaments
Adnexal mass
Retroverted fixed uterus
4. Differential diagnosis of endometriosis
Consider the following for differential diagnosis of endometriosis:
-
»
Pelvic inflammatory disease (PID)/tubo–ovarian mass
-
»
Ectopic pregnancy
-
»
Ovarian cysts
-
»
Ovarian malignancy
5 Diagnosis of endometriosis
5.1 Ultrasonography
Consider using ultrasonography to diagnose or rule out an ovarian endometrioma
The typical ultrasonography feature of endometrioma is a cystic lesion with diffuse low–level internal echoes, described as “ground–glass appearance”
Multilocularity and echogenic foci in the wall are also seen in endometrioma
Overlapping of sonographic imaging of endometrioma and hemorrhagic cyst may be observed, hence, consider performing a followup ultrasound after 6–12 weeks
5.2 Magnetic resonance imaging (MRI)
Consider MRI for detection and differentiation of ovarian endometrioma from other cystic ovarian masses. MRI detects only 30%–40% peritoneal lesions observed at surgery
MRI helps to differentiate between acute hemorrhage and blood clots
Consider MRI for assessing endometriomas for enhancing mural nodules and for restricted diffusion in those suspected of undergoing malignant transformation
5.3 Cancer antigen (CA) 125
Do not use serum CA 125 as a marker for screening of endometriosis, as the levels of CA 125 are elevated in advanced endometriosis, but the overall sensitivity and specificity is low
Serial CA 125 determinations may be useful to predict the recurrence of endometriosis as the levels decrease after treatment of endometriosis
5.4 Laparoscopy
Laparoscopy is the standard technique for inspection of pelvis and to establish a definitive diagnosis of endometriosis
Perform a complete inspection in a clockwise or counterclockwise direction with a blunt probe, with palpation of lesions to check for nodularity as a sign of deeply infiltrative endometriosis of the bowel, bladder, uterus, tubes, ovaries, cul-de-sac, or broad ligament
Laparoscopic appearance
Superficial peritoneal lesions
These are located on the pelvic organs or pelvic peritoneum
Classically seen as bluish or blue–brown lesions and are associated with hemosiderin deposits
-
Observed laparoscopic appearances are as follows:
-
»Typical powder burn or gunshot
-
»Dark brown puckered lesions
-
»Red implants
-
»Small cysts with old hemorrhage
-
»Serous or clear vesicles
-
»Scarring or white plaques
-
»Characteristic findings include typical powder–burn or gunshot lesions on the serosal surfaces of the peritoneum
-
»
Endometrioma (endometriosis cyst)
-
»
These are formed by the invagination of ovarian cortex and are characterized by fibrosis and retraction of cortex
-
»
There is presence of glandular endometrial tissue and blood clots. These are also called as “chocolate cyst”
-
»
Deep endometriosis is defined as endometriosis infiltrating deeper than 5 mm. This may give the appearance of minimal disease, thus resulting in underestimation of severity
6 Classification of endometriosis
Revised American Society for Reproductive Medicine classification (Figure 1)
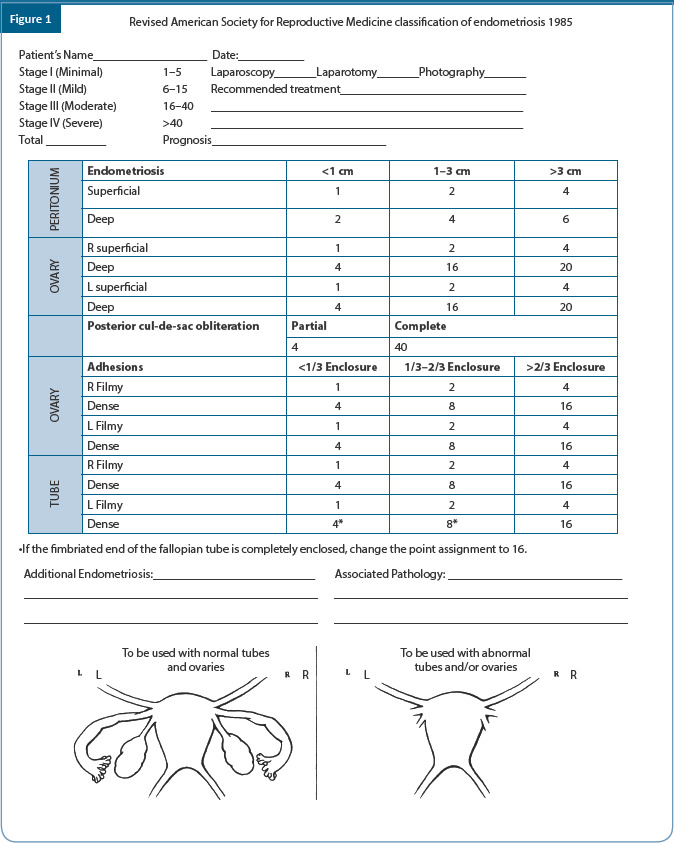
Endometriosis fertility index (Figure 2)
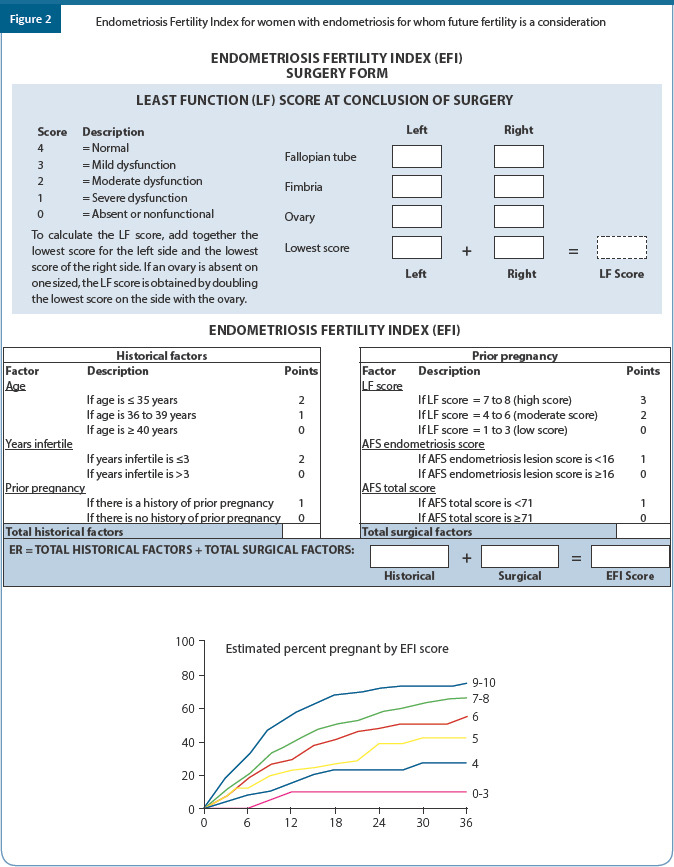
The endometriosis fertility index (EFI) is used to predict fecundity after endometriosis surgery
In addition to providing a detailed score to the appendix (fallopian tubes, fimbriae of fallopian tubes, ovaries) by calculating the least–function scores, the EFI also combines conception–related factors such as age, duration of infertility, and gravidity history
The EFI score ranges from 0–10 (0–poorest prognosis, 10–best prognosis)
7 Endometriosis and infertility
The mechanisms of infertility associated with endometriosis remain controversial and include distorted pelvic anatomy, altered hormonal and cell-mediated function, altered peritoneal function, endocrine and ovulatory abnormalities, and abnormal uterotubal transport
These factors lead to poor oocyte quality, impaired fertilization, and implantation
8 Recurrent endometriosis
-
Risk factors of recurrent endometriosis are:
- Younger age at the time of surgery (<25 years)
- Bilaterality
- Size of endometriotic lesion
- Revised AFS score >24
- Pre-operative cyst rupture
- Type and extent of surgery (laparoscopy less risk vs laparotomy)
9. Endometriosis and cancer
Some cancers (ovarian cancer, specially endometroid and clear cell cancer and non-Hodgkin’s lymphoma) are slightly more common in women with endometriosis
Women with endometriosis have lower risk of cervical cancer
Endometriosis is not associated with an altered risk of uterine cancer
The relationship between endometriosis and breast cancer is uncertain
10. Management of endometriosis
Consider the following management strategies:
Medical
Surgical
ART [intrauterine insemination (IUI); in vitro fertilisation (IVF); intracytoplasmic sperm injection (ICSI)]
Approach to a patient:
Perform a detailed infertility workup in a patient with endometriosis and any other cause related to infertility other than endometriosis should be ascertained, as despite enormous amount of information there is still uncertainty regarding etiologies and treatment
Management is still challenging in patients of endometriosis with subfertility
-
Treatment depends on
-
»Age of the patient
-
»Extent of the disease
-
»Stage of endometriosis
-
»Duration of infertility
-
»Previous therapy
-
»
Priority of the patient and cost of treatment should also be taken under consideration
Treatment modalities and preferences vary in patients based on classification. Patients with mild endometriosis on one end can be treated like those with unexplained infertility and those with severe disease require IVF
10.1 Medical management
Medical management improves the quality of life for patients with endometriosis
Therapies for endometriosis cause hormonal suppression and most of them have contraceptive effects
According to Cochrane review, subfertile women should not be prescribed hormonal ovarian suppression to improve fertility as first–line treatment in endometriosis patients who wish to conceive
a. Preoperative medical management
-
Not recommended
-
»Changes appearance of endometriosis
-
»Leads to delayed diagnosis
-
»Expensive and may cause side effects
-
»Delay in attempting pregnancy
-
»No difference for pain relief or infertility
-
»
b. Postoperative medical management
-
No evidence of benefit is reported
-
»Leads to ovulation suppression
-
»It works well for pain but does not appear to improve fertility
-
»As ovulation and periods are stopped, fertility may be reduced
-
»
c. Current place of dienogest in the treatment of endometriosis
Dienogest is a fourth–generation progestin of 19–nortestosterone derivative
It is well tolerated with no androgenic, glucocorticoid or mineralocorticoid activity
It binds to the progesterone receptor with high specificity, and produces a potent progestogenic effect related to the high circulating levels of the unbound molecule
Dienogest is associated with relatively moderate inhibition of gonadotropin secretion, leading to a reduction in the endogenous production of estradiol
When given continuously, dienogest induces a hypoestrogenic, local endocrine environment, causing a decidualization of endometrial tissue followed by atrophy of the endometriotic lesions
It also inhibits aromatase and COX-2 expression as well as prostaglandin E2 production in endometriotic stromal cells
It also normalizes the activity of natural killer cells and decreases the release of interleukin-1b by macrophages
Dienogest increases progesterone receptor expression and decreases proinflammatory cytokines
Dienogest at 2 mg once daily is used as the optimal dose in the treatment of endometriosis for duration of 12–F24 weeks
Several trials assessed the role of dienogest pretreatment for endometriosis in comparison to gonadotropin releasing hormone agonist in patients of endometriosis undergoing IVF; no significant difference was noted in number of oocyte retrieved, pregnancy, and miscarriage rate. The dienogest pretreatment was less expensive than the GnRH ultra-long protocol
10.2 Surgical management
10.2.1 Is surgery effective for infertility associated with endometriosis?
Surgical management is warranted for women with symptoms of dysmenorrhea, dyschezia, and chronic pelvic pain
-
Operative laparoscopy (excision or ablation of the endometriotic lesions) including adhesiolysis is indicated in infertile women with the American Fertility Society (AFS)/ American Society for Reproductive Medicine (ASRM) stage I/II endometriosis, rather than performing diagnostic laparoscopy only, to increase ongoing pregnancy rates
-
»Consider CO2 laser vaporization of endometriosis, instead of monopolar electrocoagulation, since laser vaporization is associated with higher cumulative spontaneous pregnancy rates
-
»Nowadays bipolar electrocoagulation is considered safe over monopolar energy source, as there is less likelihood of complications with the same
-
»As per the Cochrane review, it has been agreed that operative laparoscopic surgery improves ongoing pregnancy rate in stage I and II endometriosis when compared to diagnostic laparoscopy alone [evidence level A]
-
»Consider the conservative surgical management through laparotomy or laparoscopic approach
-
»With development of fine surgical skills, laparoscopy is now considered as gold standard in the surgical management of endometriosis
-
»Laparoscopic approach to the management of endometrioma is preferred over laparotomy, as laparoscopy offers benefits of magnification and illumination, shorter hospital stay, faster postoperative recovery, less analgesic requirement, and less morbidity
-
»
10.2.2 Managing ovarian endometrioma
The decision for operative ovarian endometrioma is taken based on clinical symptoms and ovarian reserve
In case laparoscopy is done
Excision of the endometrioma capsule (>3 cm) is recommended instead of drainage and electrocoagulation of the endometrioma wall, to increase clinical pregnancy rates
Counsel women with endometrioma regarding the reduction of ovarian reserve following surgery
Malignancy should be ruled out, as it is associated with endometrioma in 0.8% of cases
In recurrent endometrioma there is no role of USG guided aspiration and the side effects include leakage, pelvic adhesion, and ovarian abscess
10.2.3 Intraoperative steps to prevent complications
Preservation of the vascular blood supply to the ovary is important, as proper blood supply is vital for the preservation of ovarian volume and antral follicular counts
So it is postulated that when approaching the hilus, where the ovarian tissue is more functional and the plane of cleavage is less visible, partial cystectomy is performed and the remaining tissue is electro coagulated or CO2 laser is used for vaporization
Adhere strictly to the principles of microsurgery
Remove all visible endometriotic disease
Identify the plane of dissection clearly between the cyst wall and normal ovarian tissue to avoid inadvertent injury to normal ovarian tissue. Use hydrodissection or dilute vasopressin injection beneath the capsule
Identify the ureters clearly during adhesiolysis and release of ovaries from ovarian fossa
Avoid spillage of endometriotic contents as this may increase the risk of recurrence of the disease and adhesion formation
Agents for preventing adhesion during surgery:
Promote the use of oxidized regenerated cellulose during operative laparoscopy for endometriosis as it prevents adhesion formation
Anti–adhesion agents like polytetrafluoroethylene surgical membrane, hyaluronic acid products, have been effective for adhesion prevention in pelvic surgeries, although their specificity is yet to be proven in women with endometriosis
11. ART in endometriosis
Perform IUI with COS, instead of expectant management in infertile women with AFS/ASRM stage I/II endometriosis, as it increases live birth rates
11.1 Ovulation induction and IUI
Age, duration of infertility, ovarian reserve, and male factor should also be taken under consideration
Advise patients to begin attempting to conceive soon after laparoscopic surgery
Clomiphene citrate (CC) and IUI is an effective treatment option resulting in a higher clinical pregnancy rate compared to natural contact and timed intercourse
Treatment with gonadotrophins and IUI results in a higher clinical pregnancy rate compared to CC and IUI
Endometriosis and infertility have decreased per cycle conception rate compared with male factor and unexplained infertility
Also, repetitive superovulation with IUI (3–4 cycles) may have a plateau effect over time, so timely decision for IVF to be considered
11.2 Indication for IVF
Primarily IVF would be suggested if during laparoscopy severe endometriosis is found compromising tubal function
Secondly, after cystectomy if no conception even after superovulation and IUI for 3–4 cycles
Early referral for IVF in case of reduced ovarian reserve, tubal factor, and male factor
11.2.1 Stimulation protocol for IVF
Ultra-long protocol
Down regulation for 3 months with gonadotropin-releasing hormone (GnRH) in women with endometriosis increases the odds of clinical pregnancy by more than 4–fold
With the use of GnRH agonist and transvaginal oocyte retrieval, there is increased success in use of IVF for endometriosis associated infertility
Controlled ovarian stimulation (COS) using GnRH agonists or antagonists is effective in IVF patients with mild–to–moderate endometriosis and in those with endometrioma who did not undergo surgery
GnRH agonist protocol
-
»
Women with all stages of endometriosis who underwent luteal phase GnRH agonist down– regulation followed by IVF/ICSI treatment had a similar pregnancy and live birth rate and lower miscarriage rate when compared with women with tubal factor infertility
GnRH antagonist protocol
A good choice for poor responders, patients with poor ovarian reserve due to ovarian endometrioma or after its surgical excision in IVF cycles as they cause immediate suppression of luteinizing hormone (LH) surge
Similar implantation and clinical pregnancy rates have been reported in both the agonist and antagonist groups but higher number of embryos was available for cryopreservation in those patients treated with GnRH agonist
OCP’S
The preoperative use of OC before IVF/ICSI given for a period of 6–8 weeks in patients with severe endometriosis have reported higher clinical pregnancy rates compared to endometriosis patients treated without OCs and comparable to that of control patients without endometriosis
11.2.2 Precautions during ovum pick-up with endometrioma
In women with endometrioma, clinicians may use antibiotic prophylaxis at the time of oocyte retrieval to reduce the risk of ovarian abscess
Vaginal preparation with better bactericidal substances as well as stronger antibiotic prophylaxis might be useful in the prevention of PID - To decide
Other preventive measures during ovum pickup are the use of strict asepsis in the surgical field, avoiding successive punctures of the vaginal wall and ovarian capsule, avoiding puncture, and aspiration of the endometrioma
11.3 Need for oocyte donor
If ovarian reserves are poor, the couple has to be counseled regarding need for oocyte donor
11.4 Role of frozen embryo transfer (FET)
Frozen–thawed embryo transfer (FET) achieves higher pregnancy rates as compared to fresh transfers as it improves endometrial receptivity
Conclusion
Do not offer hormonal suppressive therapy to women with endometriosis who are trying to conceive
In infertile women with AFS/ASRM stage I/II endometriosis, clinicians may perform IUI with controlled ovarian stimulation, instead of expectant management, as it increases live birth rates
IVF–ET is better therapeutic option in moderate–to–severe endometriosis
Repeated surgery to be avoided
Summary of recommendation
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CCP | Clinicians should consider the diagnosis of endometriosis in the presence of gynecological symptoms such as: dysmenorrhea, non-cyclical pelvic pain, deep dyspareunia, infertility, fatigue or non-gynecological cyclical symptoms (dyschezia, dysuria, hematuria, rectal bleeding, shoulder pain). | - | -- |
| EBR | Recommended to perform transvaginal sonography to diagnose or to exclude an ovarian endometrioma and rectovaginal endometriosis | A | II |
| EBR | Recommended not to use immunological biomarkers, including CA-125, in plasma, urine or serum to diagnose endometriosis | A | II |
| EBR | For endometriosis-associated pain it is recommended to prescribe hormonal treatment [hormonal contraceptives (level B), progestagens (level A), anti- progestagens (level A), or GnRH agonists (level A)] | A-B | II |
| EBR | For pain from rectovaginal endometriosis refractory to other medical or surgical treatment, one can prescribe aromatase inhibitors in combination with oral contraceptive pills, progestagens, or GnRH analogues | B | III |
| EBR | Recommended to ablate and/or excise peritoneal endometriosis | C | III |
| EBR | When performing surgery in women with ovarian endometrioma, clinicians should perform cystectomy instead of drainage and coagulation to prevent decrease in ovarian reserve | A | I |
| EBR | In infertile women with endometriosis, recommended not prescribe hormonal treatment for suppression of ovarian function to improve fertility | A | II |
| EBR | In infertile women with AFS/ASRM stage I/II endometriosis, clinicians may perform intrauterine insemination with controlled ovarian stimulation, instead of expectant management, as it increases live birth rates | C | III |
| CPP | It is recommended to offer ART for infertility associated with endometriosis, especially if tubal function is compromised, in the presence of male factor infertility, and/or other treatments have failed. | - | - |
| CCR | In women with endometrioma, it is beneficial to use antibiotic prophylaxis at the time of oocyte retrieval, although the risk of ovarian abscess following follicle aspiration is low. | D | - |
| EBR | GnRH agonists for a period of 3 to 6 months prior to COS for ART may improve CPRs | B | III |
| EBR | In infertile women with endometrioma larger than 3 cm there is no evidence that cystectomy prior to treatment with ART improves pregnancy rate. | A | |
| EBR | Removal of endometrioma should be considered in presence of endometrioma larger than 3 cm only to improve endometriosis-associated pain or the accessibility of follicles. | II |
References
Hughes E, Brown J, Collins JJ, et al. Ovulation suppression for endometriosis. Cochrane Database SysRev 2007:CD000155
Surgery for ovarian endometriomata. Cochrane Database Syst Rev2008:CD004992.
Jacobson TZ, Duffy JM, Barlow D, et al. Laparoscopic surgery for subfertility associated with Endometriosis. Cochrane Database Syst Rev 2010:CD001398.
Brown J, Farquhar C. Endometriosis: An overview of Cochrane reviews. Cochrane Database Sys
Rev 2014:CD009590
ASRM Practice Committee. Fertil Steril 2012;98:591-8.
ESHRE Endometriosis Guideline. HR 2014;29(3):400-12.
Endometriosis: diagnosis and management (NG73) NICE 2017
Working group of ESGE, ESHRE and WES. Recommendations for the Surgical Treatment of Endometriosis. Part 1: Ovarian Endometrioma. Human Reproduction Open, pp. 1–6, 2017
Hirsch M, Begum MR, Paniz E, et al. Diagnosis and management of endometriosis: a systematic review of international and national guidelines. BJOG 2018;125:556–564.
Marc A. Fritz MD, Leon Speroff MD. Clinical Gynecologic Endocrinology and Infertility. 8th edition. Lippincott Williams & Wilkins. December 20, 2010.
Jonathan S. Berek. Berek and Novak’s Gynecology 15th Edition. Lippincott Williams and Wilkins, 2012.
Chapter 9: Endocrinopathies and its Management in Infertility
OVERVIEW
Endocrinopathies are common in women of childbearing age. These disorders are also known to have adverse effects on reproductive functions, resulting in subfertility. Therefore, it is necessary to recognize symptoms and make a correct diagnosis for proper management to avoid adverse effects on outcome of infertility treatment. The following recommendations are based on latest guidelines/recommendations from global societies, the Cochrane database, large meta–analysis, available Indian literature, prevalent practices in India, and consensus amongst experts in the field of infertility and reproductive endocrinology.
1. Thyroid disorders
1.1 Hypothyroidism
1.1.1 Preconception hypothyroidism and sub fertility
The effects of hypothyroidism on female reproductive hormones include decrease in sex hormone binding globulin (SHBG), decrease in total estradiol, increase in the unbound fraction of testosterone and estradiol, and decreased metabolic clearance of estrone and androstenedione. These changes may lead to alteration of the pituitary ovarian axis. Pulsatile gonadotrophin releasing hormone (GnRH) secretion is impaired. Hyperprolactinemia is a well–known finding in hypothyroidism especially when thyroid underactivity is profound
Overt hypothyroidism is known to be associated with anovulatory cycles and subfertility, while the association between subclinical hypothyroidism, and subfertility is uncertain (Negro, 2018). Hypothyroid women may have no menstrual disturbances or may present with features of oligovulation or anovulation. Oligomenorrhea or amenorrhea and menorrhagia may be seen probably reflecting estrogen breakthrough bleeding. Treatment of hypothyroidism with thyroxine usually reverses hormonal alterations, and restores ovulation and normal menstrual pattern
1.1.2 Preconception screening for hypothyroidism
Screening can be targeted based on presence of risk factors (Table 1) or can be undertaken universal–irrespective of any risk factors
Table 1.
High risk factors for hypothyroidism1,6
| • Women residing in geographic areas with high prevalence of thyroid disorders |
| • Women over age 30 years of age |
| • Women with infertility |
| • Obesity (pre–pregnancy/first trimester body mass index (BMI) ≥23 kg/m2) [BMI= weight in kg/height in m2] |
| • Women with a family history or autoimmune thyroid disease or hypothyroidism |
| • Women with a goiter |
| • Women with thyroid antibodies, primarily thyroid peroxidase antibodies |
| • Women with symptoms or clinical signs suggestive of thyroid hypofunction |
| • Women with type 1 DM or other autoimmune disorders |
| • Women with a prior history of miscarriage or preterm delivery |
| • Women with prior therapeutic head or neck irradiation or prior thyroid surgery |
| • Women currently receiving levothyroxine replacement |
| • Women living in a region with presumed iodine deficiency |
Recommendation
It is recommended to do targeted screening for hypothyroidism women presenting for preconception counselling. (Grade B)
It is recommended to do universal screening for hypothyroidism in women presenting with infertility and/or planned to undergo any form of infertility treatment. (Grade B)
Two Indian studies found the incidence of hypothyroidism to be 23.9% (TSH>4.2) and 53.7% (TSH>4.6) in women with infertility (Mohana Priya, Verma Indu). While other studies have shown that the incidence of subclinical hypothyroidism (SCH) is similar in infertile women and the general population, with higher mean TSH in the infertile population (Lincoln, Poppe).
1.1.3 Preconception treatment of hypothyroidism
Recommendation
It is recommended to treat all women with overt hypothyroidism and planning to conceive or undergoing any form of infertility treatment. (Grade A)
It is recommended to treat subclinical hypothyroidism in women undergoing any form of infertility treatment, if serum TSH is higher than the first trimester pregnancy specific range. (Grade B)
Hypothyroid women already on thyroxine, undergoing infertility treatment should be readjusted on thyroid replacement doses to maintain TSH levels below the reference range for first trimester. (Grade B)
Hypothyroid women undergoing controlled ovarian stimulation (COS) for assisted reproductive techniques (ART) may need an increment of thyroxine dosage. TSH level is known to increase during COS. Therapeutic regimens used for COS induce a deterioration of thyroid function especially in TPO antibody positive women. On the other hand, SCH likely adversely affects ART outcomes in a dose related fashion.
Overt hypothyroidism should always be treated with hormone replacement in women planning to conceive. Women already on thyroxine generally need escalation of thyroid dose by 30% when pregnancy is diagnosed
1.2. Hyperthyroidism
1.2.1 Preconception hyperthyroidism
Reported prevalence of overt hyperthyroidism in India ranges from 1.2% to 2.5% (22-24).
The commonest cause of maternal thyrotoxicosis is Graves’ disease associated with thyroid stimulating immunoglobulin G antibodies.
Hyperthyroidism if diagnosed prior to conception should be managed prior to advising the woman to conceive. Contraception should be used till euthyroid state is achieved.
Preconception recommendations
Thyrotoxic women should be stabilized to a euthyroid state before attempting pregnancy. (Grade A)
2. Hyperprolactinemia
Prolactin (PRL) secretion in excess may suppress the activity of the hypothalamic–pituitary–ovarian axis in the nonpregnant state. Hyperprolactinemia leads to a decrease in gonadotropin secretion with decreased LH pulse frequency and amplitude. This may result in oligo/anovulation and hence infertility. A prolonged and marked suppression of hypothalamic–pituitary–gonadal axis by chronically elevated prolactin levels may lead to signs of estrogen deficiency, most important being osteoporosis. Among women with infertility, prevalence of hyperprolactinemia was found to be 46%. Another study found the prevalence of hyperprolactinemia to range from 0.4% in an unselected normal adult population to as high as 9%–17% in women with reproductive disorders.
Hyperprolactinemia can be physiologic, iatrogenic, pituitary related, systemic or idiopathic (Table 2). Medications that are responsible are the ones that act as dopamine antagonists or the ones that interfere with dopamine secretion. Regardless of etiology, hyperprolactinemia may remain asymptomatic or it may present with hypogonadism, infertility, and galactorrhea. Bone loss occurs in many women secondary to hyperprolactinemia–mediated sex steroid attenuation.
Table 2.
Etiology of hyperprolactinemia (21)
| Physiologic | Medications | Pituitary | Systemic |
|---|---|---|---|
| Pregnancy | Metoclopramide | Prolactinomas | Primary hypothyroidism |
| Lactation | Domperidone | Stalk transection | Renal failure |
| Sleep | Antipsychotic agents (phenothiazines, haloperidol, risperidone, paliperidone) | Stalk effect in patients with non-functioning sellar and suprasellar masses | Adrenal insufficiency |
| Coitus | Opioids | Somatotropinomas and other co-secreting tumors | Spinal cord lesions |
| Food consumption | Cocaine | Radiation therapy | Chest wall lesions |
| Stress | Verapamil | PCOS | |
| Alpha methyldopa | Ectopic prolactin secretion | ||
| Monoamine oxidase inhibitors | Prolactin receptor gene mutations | ||
| Fluoxetine | Nipple stimulation |
2.1 Recommendations for diagnosis of hyperprolactinemia
In women presenting with oligo/anovulatory infertility (irregular menstrual cycles), it is recommended to test for serum prolactin levels. (Grade A)
Single measurement of serum prolactin level 2.5 times above the reference range limit confirms the diagnosis of hyperprolactinemia. (Grade B)
Excessive venipuncture stress should be avoided. Sample may be taken at any time of the day. (Grade C)
The initial determination of serum prolactin should avoid excessive venipuncture stress and can be drawn at any time of the day. A single determination is usually enough to establish the diagnosis, but when in doubt, sampling can be repeated on a different day at 15 to 20 min intervals to account for possible prolactin pulsatility. Normal values are higher in women than in men and are generally lower than 25 mcg/liter.
In patients with asymptomatic hyperprolactinemia, assessment for macroprolactin should be done using polyethylene glycol precipitation test. (Grade C)
Patients with asymptomatic hyperprolactinemia, should be assessed for the presence of macroprolactin. Retrospective studies have shown that approximately 40% patients with hyperprolactinemia have macro–prolactinemia. Since, macro–prolactinemia is a common cause of hyperprolactinemia, routine screening for macroprolactin will eliminate unnecessary diagnostic testing and treatment. Polyethylene glycol precipitation is the test done to detect the presence of macroprolactin in the serum.
In presence of a very large pituitary tumor and a mildly elevated prolactin level, serial dilution of serum samples is recommended to eliminate an artifact that can occur in patients with exuberant PRL secretion leading to a falsely low prolactin value (“hook effect”) (Grade A)
Serum prolactin levels are known to parallel prolactinoma size. Macroprolactinomas are generally associated with prolactin levels greater than 250 mcg/l. Many a times, there may be a dissociation between the size of prolactinoma and serum prolactin levels. A common cause of such discrepancy is the ‘hook effect’, which is an assay artifact that may be observed when high serum prolactin concentrations saturate antibodies in the immunoradiometric assay used to estimate serum prolactin level.
In women with elevated prolactin, it is recommended to rule out pregnancy, rule out causative medicine use, to get serum TSH and free/total T4 testing, and to do renal function test in order to establish the etiology (Table 2) (Grade A)
If other causes are ruled out, contrast–enhanced MRI head with pituitary images is recommended. (Grade A)
In women with confirmed elevated prolactin level, pregnancy should be ruled out in those of childbearing age, medication use should be excluded, levels of thyrotropin and free T4 should be measured, and renal function should be assessed.
Imaging: Once other possible causes of an elevated prolactin level have been ruled out, MRI of the head should be performed, with the use of contrast material, and pituitary images obtained.
2.2. Preconception Hyperprolactinemia management
2.2.1 Drug induced hyperprolactinemia
Asymptomatic drug induced hyperprolactinemia does not require treatment. (Grade A)
In symptomatic women with drug induced hyperprolactinemia, if feasible, consideration should be given to discontinuation or substitution of the drug for 3 days and recheck prolactin levels. (Grade B)
When discontinuation of the drug is not feasible, use of dopamine agonists is controversial. (Grade C)
Oral contraceptives may be used in symptomatic women with drug–induced hyperprolactinemia to regularize cycles and to improve symptoms of estrogen deficiency. (Grade B)
If possible, establish temporal relation between prolactin elevation and initiation of medication. Obtain a pituitary magnetic resonance image (MRI) if the onset of the hyperprolactinemia does not coincide with therapy initiation. In patients with symptomatic hyperprolactinemia related to medication, attempt discontinuation of the medication for 3 days or substitution of an alternative drug, followed by remeasurement of serum prolactin. Discontinuation or substitution of an antipsychotic agent should not be undertaken without consulting the patient’s physician.
If discontinuation or substitution of the drug is not feasible in symptomatic women, use of dopamine agonists in such women is controversial. Studies suggest that dopamine agonist therapy is effective only in 75% of such patients but may lead to exacerbation of the underlying psychosis. Use of oral contraceptives in women may improve symptoms of estrogen deficiency but not those of hyperprolactinemia.
2.2.2 Idiopathic hyperprolactinemia and prolactinomas
Dopamine agonists are recommended for the management of macroprolactinomas and for symptomatic microprolactinomas as well as idiopathic hyperprolactinemia. (Grade A). Symptomatic micro–prolactinomas as well as idiopathic hyper–prolactinemia with amenorrhea may also be managed with oral contraceptives. (Grade B)
Cabergoline is preferred over other dopamine agonists in the presence of hyperprolactinemia of idiopathic origin or with prolactinomas. (Grade A)
It is recommended to monitor therapy with serum prolactin level at 1 month after starting dopamine against to make dose adjustments as required. (Grade B)
Women with prolactinomas who are controlled on dopamine agonists, require repeat MRI at 1 year
Women with macroprolactinomas and with persistent high prolactin levels or with new onset of symptoms despite receiving dopamine agonists should have repeat MRI at 3 months. (Grade B)
Dopamine agonist may be discontinued after 2 years of initiation of treatment if serum prolactin has normalized and there is no visible remnant tumor on MRI. (Grade A)
Dopamine agonist therapy lowers prolactin levels, decreases tumor size, and restores gonadal function for patients harboring symptomatic prolactin–secreting microadenomas or macroadenomas. Cabergoline is preferred to other dopamine agonists because it has higher efficacy in normalizing prolactin levels, as well as a higher frequency of pituitary tumor shrinkage. The incidence of unpleasant side effects is lower with cabergoline; hence drug compliance may be superior for this medication. With careful clinical and biochemical follow–up, therapy may be tapered and perhaps discontinued in patients who have been treated with dopamine agonists for at least 2 years, who no longer have elevated serum prolactin, and who have no visible tumor remnant on MRI.
Asymptomatic patients harboring microprolactinomas or with idiopathic hyperprolactinemia do not need treatment with dopamine agonists.
2.3 Subfertility and hyperprolactinemia
It is recommended that, women with hyper-prolactinemia presenting with oligo/anovulation and infertility, be managed with dopamine agonists. Women with high prolactin levels with normal ovulation do not need treatment with dopamine agonist. (Grade A)
Patients with asymptomatic hyperprolactinemia, should be assessed for the presence of macroprolactin. Retrospective studies have shown that approximately 40% patients with hyperprolactinemia have macroprolactinemia which has no biological activity. With dopamine agonists cyclic menses are restored in 70%–90% women, within 6–8 weeks of initiation of treatment and ovulatory cycles return in 50%–75% of treated women. Cabergoline is more effective than bromocriptine in achieving and maintaining normal prolactin levels, restoring ovulatory cycles and is better tolerated.
Those failing to ovulate with dopamine agonists or in women with drug induced hyperprolactinemia where drug cannot be discontinued or prolactin levels should not be reversed, may be considered for ovarian stimulation with gonadotropins. (Grade B)
Discontinuation or substitution of an antipsychotic agent should not be undertaken without consulting the patient’s physician. Reversing prolactin levels to normal may negate the drug effect also. Those failing to ovulate with dopamine agonists can be treated with gonadotropin for ovarian stimulation.
| Comparison between cabergoline and bromocriptine | ||
|---|---|---|
| Bromocriptine | Cabergoline | |
| Half-life | 6–20 h | 63–69 h |
| Duration of action | 24 h | 7–14 h |
| Dosing | Twice daily | Once or twice weekly |
| Recommended dose | 5–7.5 mg daily | 1–2 mg weekly |
| Normalization of prolactin (%) | 48–59 | 83–93 |
| Restoration of fertility (% | 48–52 | 72 |
3. Adrenal disorders
3.1 Congenital adrenal hyperplasia (CAH)
CAH consists of a group of inherited disorders that result from decreased cortisol synthesis due to deficiency of one or more of the enzymes involved in steroidogenesis or affecting steroidogenic pathways. Decrease in cortisol production leads to feedback rise in adrenocorticotropic hormone (ACTH) release with resultant chronic adrenal stimulation and hyperplasia. The precursors of steroid synthesis before the enzymatic block are increased in concentrations. This may include increased synthesis of adrenal androgens. The symptoms of the disease generally result from deficiency of cortisol and/or mineralocorticoids and excess of androgens, depending on the enzyme/enzymes that are deficient and whether any residual enzyme activity is present.
All forms of CAH are inherited as autosomal recessive disorders. The most common form results from deficiency of 21–hydroxylase (21–OHD), responsible for more than 90% of the cases. Other enzyme deficiencies that may result in CAH are: 11–β hydroxylase, 3–β hydroxysteroid dehydrogenase, 17 hydroxylase, 17–β hydroxysteroid dehydrogenase, aromatase, P450 oxidoreductase, steroid acute regulatory protein.
3.1.1 Classification
CAH due to 21–hydroxylase deficiency can be classified as under (Table 4).
Table 4.
Classification of congenital adrenal hyperplasia (CAH)
| Classification | Residual enzyme activity | Presentation | Aldosterone | Cortisol |
|---|---|---|---|---|
| Classic–salt wasting type | 0% to 1% | • Symptoms of gluco-corticoid & mineralocorticoid deficiency since birth • Virilized external genitalia in girls at birth |
Low | Low |
| Classic–simple virilizing type | 2% to 20% | • Virilized external genitalia in girls at birth | Normal | Low |
| Non classic CAH (NCCAH) | 20% to 50% | • Symptoms of hyperandrogenism in adolescent and adult females | Normal | Normal |
Treatment mainly consists of glucocorticoid (GC) with or without mineralocorticoid (MC) supplementation. This lowers production of ACTH and hence reverses adrenal hyperfunctioning and its effects. In young girls and adults presenting for the first time in adolescence or later non–classic CAH (NCCAH) is the one mostly seen which is the mildest form of CAH owing to of 21–hydroxylase deficiency.
3.1.2 Diagnosis of CAH and NCCAH
In symptomatic individuals, screen with early–morning (before 8 AM) baseline serum 17–hydroxyprogesterone measurement. (Grade A). In menstruating women sampling should be done in the early follicular phase. (Grade B)
In individuals with borderline 17–OHP level, it is recommended to get co–syntropin stimulation test done. (Grade A)
-
Genotyping should be considered only when (Grade B)
-
»Results of the adrenocortical profile after a co–syntropin stimulation test are equivocal, or
-
»Co–syntropin stimulation cannot be accurately performed (i.e., patient receiving glucocorticoid), or
-
»For purposes of genetic counseling
-
»
In symptomatic individuals, past infancy, screening with an early–morning (before 8 AM) baseline serum 17–hydroxyprogesterone (17–OHP) measurement is recommended. Random measurements of 17–OHP have not been shown to be helpful since these often yield normal levels in patients with NCCAH. In menstruating females, it is recommended to sample in the early follicular phase. Co–syntropin stimulation test: Baseline samples are collected for 17-OHP after which synthetic ACTH (co–syntropin) is administered with a standard dose of 250 μg for older children and adults. (Figure 1). Repeat blood work is collected 60 minutes after administration to determine the stimulated values of 17–OHP. While stimulated 17–OHP levels with classic CAH typically exceed 20,000 ng/dl, those with NCCAH will have 17–OHP levels within the range of 1,500–10,000 ng/dl post stimulation.
For patients with nondiagnostic stimulated 17–OHP values, genotyping may confirm the diagnosis.
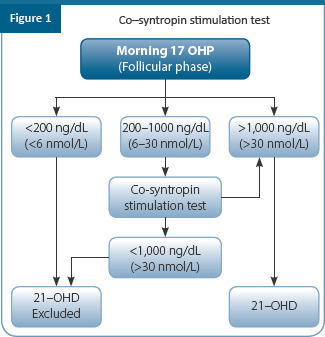
3.1.3 Management of CAH and NCCAH
Young women not planning pregnancy
Women diagnosed as NCCAH and presenting with hyperandrogenism and menstrual irregularities may be managed with oral contraceptives and antiandrogens if required. (Grade B)
Asymptomatic non–pregnant women with NCCAH do not require treatment. (Grade A)
Clinically, many young women with NCCAH are asymptomatic. When symptomatic, the presentation is quite variable among individuals and varies with age in the same individual. Initial clinical presentation of NCCAH is before the age of 10 years in 11% of cases and between the ages of 10 and 40 years in 80%.
Symptomatology includes premature pubarche, under 8 years of age in girls and under 9 years in boys. Incidence of NCCAH among children with precocious puberty ranges from 5%–30% according to different studies. Rapid progression of bone age and truncated final height may also be seen. During adolescence and adulthood, women with NCCAH generally have symptoms like PCOS. Presenting symptoms include hirsutism (78%), menstrual dysfunction (54.7%), and decreased fertility (12%), and alopecia (Witchel). Acne is reported in about 33% of NCCAH patients. The presence of hirsutism correlates with increasing age, indicating progressive nature of the disease. Osteoporosis may be a late feature, as a consequence of prolonged corticosteroid therapy.
Young women with classic CAH should continue glucocorticoid and mineralocorticoid therapy as prescribed by endocrinologist. (Grade A). A baseline bone mineral density (BMD) measurement should be considered in young women. (Grade C). Oral contraceptives may be added to improve symptoms of hyperandrogenemia
During the transition from adolescence to adulthood in girls with classic CAH, need for continuation of glucocorticoid and mineralocorticoid for long term benefits, should be stressed to prevent noncompliance. Addition of oral contraceptive pills to the regimen might help to reduce androgen concentrations, should be especially considered in heterosexually active women, not desiring pregnancy. Osteoporosis prophylaxis, including vitamin D and calcium supplementation should also continue.
3.1.4 Young women planning pregnancy
In women with classic CAH who are trying to get pregnant, dexamethasone should be substituted with hydrocortisone or prednisolone. (Grade A)
Fertility treatment in classic CAH with optimized GC therapy to normalize androgen and progesterone levels, most women desiring pregnancy will achieve spontaneous conceptions. Women who fail to ovulate despite adequate treatment may be given oral ovulation induction agents. Women with low sex steroid production may need COS with IVF with adequate hormone replacement. In some women with uncorrected or partially corrected virilized external genitalia, genitoplasty may be required to improve sexual function.
In infertile women (anovulatory infertility) with NCCAH or those with a history of miscarriage, and currently planning to conceive, treatment with a GC that does not cross placenta is recommended. (Grade B)
Infertile women with NCCAH who fail to ovulate with glucocorticoids may be treated with oral ovulogens or with gonadotropins. (Grade B)
Table 5 enumerates the different glucocorticoids that can be used whereas table 6 elicits dose for the maintenance therapy
Table 5.
Choice of glucocorticoids (GC) in infertile women with NCCAH
| Glucocorticoids | Usage in | Features |
|---|---|---|
| Short acting GC: Hydrocortisone | • Neonates and children • Treatment of pregnant women with CAH |
• Multiple daily dosing required • Closely resembles cortisol in action. • Does not cross placenta |
| Long acting GC: Dexamethasone | • Prenatal treatment of fetal CAH with aim to prevent female fetal virilization at birth | • Highest suppression of steroid synthesis • Greatest decrease in BMD and highest weight gain tendency • Crosses placenta |
| Long acting GC: Prednisolone | • Adults | • Side effect profile: less severe than dexamethasone • Crosses placenta but fetal uptake is limited |
Table 6.
Maintenance in infertile women with NCCAHt
| Long-acting corticosteroid | Dose (mg/d) | Daily doses |
|---|---|---|
| Hydrocortisone | 15–25 | 2–3 |
| Prednisone | 5–7.5 | 2 |
| Prednisolone | 4–6 | 2 |
| Methylprednisolone | 4–6 | 2 |
| Dexamethasone | 0.25–0.5 | 1 |
| Fludrocortisone | 0.05–0.2 | 1–2 |
In women with Infertility with NCCAH hydrocortisone seems to be the appropriate treatment; as it lowers adrenal androgen secretion, normalizes menstrual cycles, and reduces the incidence of miscarriages (Bidet, Pham, Smith). Twice-a-day hydrocortisone dose schedule is considered reasonable (Table 3). The clinical criteria for therapeutic efficacy are regular cycles and rise in P4 indicating resumption of ovulation; the biochemical criteria consist of fall in plasma testosterone and androstenedione values to normal levels (Feldman). Women who fail to ovulate with hydrocortisone therapy may be considered for ovulation induction with clomiphene citrate.
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| EBR | Endocrine disorders should be identified, addressed, treated and body weight normalized | B | II |
| EBR | It is recommended to do targeted screening for hypothyroidism women presenting for preconception counselling | B | II |
| EBR | It is recommended to do universal screening for hypothyroidism in women presenting with infertility and/or planned to undergo any form of infertility treatment | B | III |
| EBR | Anti-thyroperoxidase (TPO) and/or anti–thyroglobulin (TPG) antibodies have a negative impact on fertility and pregnancy, which makes it mandatory to measure the thyroid antibodies in women who wish to conceive or those who have had BOH despite euthyroid status | B | III |
| Women with hypothyroidism and thyroid antibodies should be treated with L-thyroxine, | |||
| EBR | • It is recommended to treat all women with overt hypothyroidism and planning to conceive or undergoing any form of infertility treatment | A | I |
| CCR | • It is recommended to treat subclinical hypothyroidism in women undergoing any form of infertility treatment, if serum TSH is higher than the first trimester pregnancy specific range | B | III |
| EBR | • Hypothyroid women already on thyroxine, undergoing infertility treatment should be readjusted on thyroid replacement doses to maintain TSH levels below the reference range for first trimester | B | II |
| Hyperthyroidism | |||
| EBR | Thyrotoxic women should be stabilized to a euthyroid state with the average dose of radioactive iodine (370 MBq), before attempting pregnancy | A | I |
| EBR | No significant damage to the gonads noted with this dose but conception is avoided until 6 months after administration | B | |
| EBR | Hyperprolactinemia | A | II |
| CCR | In women presenting with oligo/anovulatory infertility (irregular menstrual cycles), it is recommended to test for serum prolactin levels | C | IV |
| CCR | In patients with asymptomatic hyperprolactinemia assessment for macroprolactin should be done using polyethylene glycol precipitation test | A | I |
| EBR | In women with elevated prolactin, it is recommended to rule out pregnancy, rule out causative medicine use, to get serum TSH and free/total T4 testing, and to do renal function test in order to establish the etiology | A | II |
| EBR | If other causes are ruled out, contrast enhanced MRI head with pituitary images is recommended | A | I |
| EBR | Hyperprolactinemia should be treated with dopamine agonists Cabergoline is preferred over other dopamine agonists in the presence of hyper- | A | II |
| EBR | prolactinemia of idiopathic origin or with prolactinomas It is recommended to monitor therapy with serum prolactin level at 1 month after starting dopamine against to make dose adjustments as required | B | II |
| EBR | Congenital adrenal hyperplasia (CAH) | A | I |
| EBR | In symptomatic individuals, screen with early–morning (before 8 AM) baseline serum 17–hydroxyprogesterone measurement | B | III |
| EBR | In menstruating women sampling should be done in the early follicular phase | A | II |
| EBR | In individuals with borderline 17–OH Progesterone level, it is recommended to get co–syntropin stimulation test done | B | III |
| EBR | Women diagnosed as non–classical CAH (NCCAH) and presenting with hyperandrogenism and menstrual irregularities may be managed with oral | A | II |
| EBR | contraceptives and antiandrogens if required | A | I |
| CCR | Asymptomatic non pregnant women with NCCAH do not require treatment Young women with classic CAH should continue glucocorticoid and mineralocorticoid | C | - |
| CCR | therapy as prescribed by endocrinologist A baseline bone mineral density (BMD) measurement should be considered in young | C | |
| EBR | women Oral contraceptives may be added to improve symptoms of hyperandrogenemia Infertile women with NCCAH who fail to ovulate with glucocorticoids may be treated with oral ovulogens or with gonadotropins | B |
References
ATA, 2017
ASRM, 2015
National guidelines for screening of hypothyroidism in pregnancy, Ministry of Health and Family Welfare of Government of India, 2014.
Kalra S, Agarwal S, Aggarwal R, et al. Trimester-specific thyroid- stimulating hormone: an Indian perspective. Indian J Endocrinol Metab. 2018;22(1):1.
Management of Thyroid Dysfunction during Pregnancy and Postpartum: An Endocrine Society Clinical Practice Guideline, USPSTF, 2012.
Aimee Seungdamrong, The Impact and Management of Subclinical Hypothyroidism for Improving Reproductive Outcomes such as Fertility and Miscarriage, Semin Reprod Med, 2016.
Roberto Negro. Thyroid and Assisted Reproduction Technologies: A Brief Clinical Update with Recommendations for Practice, Endocrine, Metabolic & Immune Disorders - Drug Targets, 2018
Yen_&_Jaffe’s_Reproductive_Endocrinology.
Deokar PG, Nageotte AN, Lange MJ, Basutkar DG (2016) Prevalence of thyroid disorders in a tertiary care center. J Curr Res 8(9):26–31
Usha Menon V, Sundaram KR, Unnikrishnan AG, Jayakumar RV, Nair V, Kumar H. High prevalence of undetected thyroid disorders in an iodine sufficient adult south Indian population. J Indian Med Assoc 2009; 107:72-7.
Abraham R, Murugan VS, Pukazhvanthen P, Sen SK. Thyroid Disorders In Women of Puducherry. Indian J Clin Biochem 2009; 24:52-9.
Melmed S, Casanueva FF, Hoffman AR, et al: Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96:273–288, 2011.
Klibanski A, Beitins IZ, Merriam GR, et al: Gonadotropin and prolactin pulsations in hyperprolactinemic women before and during bromocriptine therapy. J Clin Endocrinol Metab 58:1141–1147, 1984.
Winters SJ, Troen P: Altered pulsatile secretion of luteinizing hormone in hypogonadal men with hyper-prolactinemia. Clin Endocrinol (Oxf) 21:257–263, 1984.
Sharma N, Baliarsingh S, Kaushik GG: Biochemical association of hyperprolactinemia with hypothyroidism in infertile women. Clin Lab 58:805–810, 2012.
Biller BM, Luciano A, Crosignani PG, et al: Guidelines for the diagnosis and treatment of hyperprolactinemia. J Reprod Med 44:1075–1084, 1999.
Schlechte JA 2003 Clinical practice. Prolactinoma. N Engl J Med 349:2035–2041
GillamMP, MolitchME,LombardiG,ColaoA2006Advancesin the treatment of prolactinomas. Endocr Rev 27:485–534
Klibanski A: Clinical practice. Prolactinomas. N Engl J Med 362: 1219–1226, 2010
Casanueva FF,MolitchME,SchlechteJA,AbsR,BonertV,Bron- stein MD, Brue T, Cappabianca P, Colao A, Fahlbusch R, Fideleff H, Hadani M, Kelly P, Kleinberg D, Laws E, Marek J, Scanlon M, Sobrinho LG, Wass JA, Giustina A 2006 Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf) 65:265–273
Mancini T, Casanueva FF, Giustina A 2008 Hyperprolactinemia and prolactinomas. Endocrinol Metab Clin North Am 37:67–99, viii
Donadio F, Barbieri A, Angioni R, Mantovani G, Beck-Peccoz P, Spada A, Lania AG 2007 Patients with macroprolactinaemia: clin- ical and radiological features. Eur J Clin Invest 37:552–557
McKenna TJ 2009 Should macroprolactin be measured in all hy- perprolactinaemic sera? Clin Endocrinol (Oxf) 71:466–469
Cavallaro R, Cocchi F, Angelone SM, Lattuada E, Smeraldi E 2004 Cabergoline treatment of risperidone-induced hyperprolactine- mia: a pilot study. J Clin Psychiatry 65:187–190
Webster J, Piscitelli G, Polli A, Ferrari CI, Ismail I, Scanlon MF. A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea. Cabergoline Comparative Study Group. N Engl J Med. 1994;331(14):904–909. doi:10.1056/NEJM199410063311403
Speroff, Eighth edition
71. Azziz R, Hincapie LA, Knochenhauer ES, et al. Screening for 21-hydroxylase-deficient nonclassic adrenal hyperplasia among hyperandrogenic women: a prospective study. Fertil Steril. 1999; 72:915–25. [PubMed: 10561000]
72. Speiser PW, Arlt W, Auchus RJ, Baskin LS, Conway GS, Merke DP, Meyer-Bahlburg HFL, Miller WL, Murad MH, Oberfield SE, White PC. Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(11): 4043–4088.
73. New MI, Lorenzen F, Lerner AJ, et al. Genotyping steroid 21-hydroxylase deficiency: hormonal reference data. J Clin Endocrinol Metab. 1983; 57:320–6. [PubMed: 6306039]
77. Moran C, Azziz R, Carmina E, Dewailly D, Fruzzetti F, Ibañez L, et al. 21- Hydroxylase-deficient nonclassic adrenal hyperplasia is a progressive disorder: a multicenter study. Am J Obstet Gynecol. (2000) 183:1468–74. doi: 10.1067/mob.2000.108020
78. Christine M. Trapp and Sharon E. Oberfield. Recommendations for Treatment of Nonclassic Congenital Adrenal Hyperplasia (NCCAH): an Update. Steroids. 2012 March 10; 77(4): 342–346. doi:10.1016/j.steroids.2011.12.009.
79. Moran C, Azziz R, Weintrob N, Witchel SF, Rohmer V, Dewailly D, et al. Reproductive outcome of women with 21-hydroxylase-deficient nonclassic adrenal hyperplasia. J Clin Endocrinol Metab. (2006) 91:3451–6. doi: 10.1210/jc.2006-0062
81. Witchel SF. Non-classic congenital adrenal hyperplasia. Steroids. (2013) 78:747–50. doi: 10.1016/j.steroids.2013.04.010
82. Kemp MW, Newnham JP, Challis JG, Jobe AH, Stock SJ. The clinical use of corticosteroids in pregnancy. Hum Reprod Update. 2016;22(2):240–259. doi:10.1093/humupd/dmv047
Chapter 10: Ovulatory Disorders
OVERVIEW
This document highlights good practice recommendations on ovulatory disorders for practicing gynecologists in India. Management of ovulatory disorders poses a constant challenge in practicing gynecologists, embryologists, and infertility specialists. These recommendations are based on several guidelines/recommendations from global societies, the Cochrane database, large meta-analysis, available Indian literature, prevalent practices in India, and consensus amongst experts in the field of ovulatory infertility. These recommendations concentrate on the need to strengthen and promote meaningful research that will be applicable to Indian patients and Indian practice.
1. Introduction
Ovulatory disorders account for infertility in up to 40% of women. In most of the cases, ovulatory disorders are associated with irregular periods (oligomenorrhea) or an absence of periods (amenorrhea)
A cut-off age of 32 years should be taken as a risk factor for diminished ovarian reserve
2. Classification of anovulatory infertility
World Health Organization (WHO) classification of ovulatory disorders (Table 1)
Table 1.
Classification of ovulatory disorders
| Group I: Hypothalamic/pituitary failure | Weight loss, systemic illness, Kallmann’s syndrome, hypogonadotrophic hypogonadism | 5% |
| Hyperprolactinaemia, hypopituitarism | ||
| Group II: Hypothalamic/pituitary dysfunction | PCOS | 90% |
| Group III: Ovarian failure | Premature ovarian failure (POF) Resistant ovary syndrome (ROS) | 5% |
3. Diagnosis of anovulatory infertility
3.1 Menstrual irregularity
Menstrual irregularity may suggest the presence of ovulatory disorders. In women with ovulatory disorders, oligomenorrhea, amenorrhea and/or prolonged cycles are very common
3.2 Physical examination
-
According to WHO Consensus Statement,
-
»BMI
- - Normal BMI: 18.0–22.9 kg/m2
- - Overweight: 23.0–24.9 kg/m2
- - Risk/high-risk: >25 kg/m2 (risk of obesity); and >27.5 kg/m2 (high–risk)
-
»Waist circumference (women)
- - 72 cm (avoid gaining weight and maintain physical activity)
- - >80 cm (seek medical help to manage obesity–related risk factors)
-
»
Underweight may signify a hypothalamic cause and overweight could indicate endocrinopathy like PCOS
Other signs of endocrinopathy–alopecia, hirsutism, acne, stigmata of thyroid dysfunction
-
Clinical hyperandrogenemia should be assessed and scored for severity
-
»To evaluate hirsutism, a modified Ferriman Gallwey score (mFG) can be used: A score of ≥4 is relevant but relevance may vary with ethnicity
-
»To evaluate alopecia, the Ludwig visual score can be used
-
»
3.3 Laboratory investigations
3.3.1 Diagnostic hormonal levels in anovulatory infertility
Table 2.
Hormone levels in different anovulatory disorders
| Hypothalamic: Underweight | ↓FSH, ↓ LH, ↓E2 n FSH, ↓ LH, ↓ E2 |
| Hyperprolactinaemia | ↓ FSH, ↓ LH, ↓ E2 |
| Ovarian failure/menopause | ↑↑ FSH, ↑ LH, ↓E2 |
| Mid-cycle | ↑ FSH, ↑↑ LH, ↑ E2 |
| PCOS | ↓/n FSH, ↑/n LH, ↑/n E2 |
Testosterone will be low or normal in women classified under group I WHO. Testosterone testing in women with the group I and III is not helpful. In women with group II, assessment of biochemical hyperandrogenism by assessing free androgen index (FAI), calculated free testosterone (cFT), and calculated bioavailable testosterone (cBT) should be considered in diagnosing PCOS
Women on oral contraceptive pills have an altered testosterone level due to alteration in sex hormone–binding globulin. Contraceptive should be withdrawn for 3 months before measuring androgens
3.3.2 Tests for confirming ovulation
Follicular monitoring by ultrasound is a reliable option
Progressive growth and collapse of the follicle with increased internal echoes and fluid in the cul-de-sac are markers of ovulation
Serum progesterone in the mid–luteal phase on day 21 of a 28 days menstrual cycle
Women with prolonged, irregular cycles if day 21 progesterone suggests anovulation test after day 28th weekly till menstruation
A value of >3 ng/mL is considered as ovulation. Progesterone has a pulsating release thus single level may not be useful unless elevated. Values of >/= 10ng/ml are suggestive of normal progesterone production
Urinary LH kit
3.3.3 Baseline pelvic scan
Baseline scan is the scan done between from 2nd to 4th day of the cycle time when the ovaries are quiescent with no follicles > 8mm. It is done to
-
»
Assess endometrium < 7 mm
-
»
Identify adnexal abnormalities
-
»
Identify uterine abnormalities
-
»
Identify ovarian cyst
-
»
To identify the type of the ovary
-
»
Assess ovarian reserve by AFC
-
»
Decide stimulation protocols for adequate response and avoid OHSS
Prerequisites for OI: OI initiated on Day 2/3 only if:
-
»
Follicular size is <10 mm
-
»
Absence of ovarian cyst
-
»
Endometrial thickness <6 mm
3.3.4 Testing ovarian reserve status
The figure 1 enumerates all available ovarian test
Analysis of ovarian reserve should be done before starting the ovarian stimulation to select the correct stimulation protocol to decide dose to prevent ovarian hyperstimulation or poor response. Most Individualized protocols are based on age, AMH, AFC, and FSH, which are further amended according to the BMI
Ovarian reserve testing is beneficial in determining the dose of gonadotropins in women undergoing ovarian stimulation. Ovarian reserve also helps to prevent ovarian hyperstimulation or poor response
-
Specific factors must be followed that may mandate earlier investigations (after 6 months of failed attempts to conceive or earlier if clinically indicated) in Indian women:
-
»Aged ≥32 years
-
»Family history of early menopause or a known cause of infertility
-
»Unexplained infertility
-
»Ovarian surgery, chemotherapy or radiotherapy
-
»Show signs of shortened menstrual cycles or oligomenorrhea or amenorrhea
-
»Poor ovarian response and AFC on a basic scan
-
»
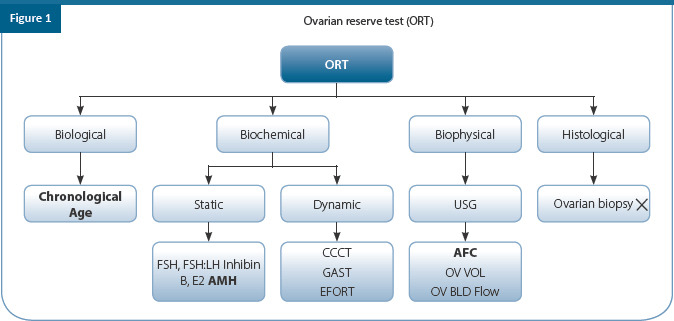
3.3.5 Other investigations
Prolactin/thyroid function test
Androgen profile if PCOS
SHBG and GTT
Lipid profile
Semen analysis
Tubal patency assessment
3.4 Predictors of ovarian response
Response can be predicted based on AMH, AFC, FSH. Additional test like Inhibin B, estradiol, day 10 progesterone values, and ovarian volume are used to predict poor response. The table 3 gives the predictor of high and poor ovarian response
AMH and AFC along with age the good predictors of response to COS but do not predict ART outcomes “Live birth rate”
FSH alone is not a good predictor of ovarian response
Ovarian volume, ovarian blood flow, inhibin B, estradiol E2 clomiphene challenge tests are not to be considered as they are not beneficial in testing. Basal estradiol values are not used singularly but only to interpret FSH values
Table 3.
Predictors of ovarian response
| Markers of normal response | • AFC - > 8 <14 |
| • AMH – 1.25–3.5 ng/ml | |
| Markers of high response | • AFC > 4 |
| • AMH >3.5 ng/ml | |
| • Color doppler – Increased stromal velocity | |
| Markers of low response | • Age–> 36 years |
| • FSH > 10 mIU/ml | |
| • E2 > 75 pg/ml | |
| • AMH < 1.25 ng/ml | |
| • Inhibin B < 45 pg/ml | |
| • P4 on day 10 of COS > 1.1ng/ml | |
| • AFC < 5 | |
| • Ovarian volume – < 3 cm3 | |
| • Large inter–cycle variability in basal FSH | |
| • Low flow at color Doppler |
AFC: antral follicular Count; AMH: anti-Müllerian Hormone; E2: estradiol; FSH: follicle stimulating hormone.
4. Treatment of anovulatory disorders
Etiology and treatment of anovulatory disorders is highlighted in Table 4.
Table 4.
Etiology and treatment of anovulatory disorders
| Etiology | Examples | Suitability for ovulation induction treatment | Drug treatment | Next step |
|---|---|---|---|---|
| Group I Hypogonadotropic ↓FSH, ↓LH, and ↓E2 | Underweight, anorexia; intense exercise as in athletes, ballerinas | Not unless correction of weight, reduction in exercise (as appropriate) is achieved | Gonadotropins: LH + FSH or pulsatile GnRH pump | ART – IVF/ICSI |
| Cranial tumors, irradiation, and hypophysitis | Not until the primary disease is treated with medical or surgical measures as indicated | Gonadotropins | ||
| Sheehan syndrome | Yes | Gonadotropins | ||
| Kallmann’s syndrome, idiopathic | Yes, after addressing lifestyle if necessary | Gonadotropins or pulsatile GnRH pump | ||
| Hyperprolactinemia (this can result in secondary hypothalamic hypogonadism) | Pathological: drugs (e.g. phenothiazines, metoclopramide), pituitary microadenomas or macroadenomas. Other causes: stress, exercise, physical examination, PCOS | No, hyperprolactinemia should be corrected first either by medical or surgical means as indicated | Dopamine agonists, e.g. bromocriptine | |
| Group II Normogonadotropi c ↔FSH, ↔ or ↑LH, ↔ or ↑E2 | PCOS, idiopathic | Yes, after correcting weight and lifestyle factors | Letrozole 2.5 - 5 mg day 3 - 7 is first line therapy Clomiphene citrate 50-150 mg Day 2-6 for 6- 9 cycles if ovulatory | Gonadotropins or LOD; last option is IVF |
| Group III Hypergonadotropic ↑FSH and LH, ↓E2 | Premature ovarian failure: Genetic causes: Turner syndrome, fragile X syndrome, gonadal dysgenesis. Iatrogenic: surgery, chemotherapy, and radiation Autoimmune causes: polyendocrinopathy syndrome Infections (rare): viral oophoritis Idiopathic autoimmune disorders | No | Egg donation program | Long–term HRT |
↑ = increased; ↓ = decreased; ↔ = normal E2 = estradiol; FSH = follicle-stimulating hormone; GnRH = gonadotropin- releasing hormone; HRT = hormone replacement therapy; IVF = in vitro fertilization; LH = luteinizing hormone; LOD = laparoscopic ovarian drilling; PCOS = polycystic ovary syndrome.
4.1 WHO Group I–Anovulatory infertility due to hypogonadotropic hypogonadism
Choice of therapy (Table 5)
Table 5.
Treatment of anovulatory infertility
| Condition | Treatment |
|---|---|
| Hypothalamo-pituitary failure | • Gonadotrophins 75 – 225 IU hMG |
| • GnRH pulses Dose - 15 ug or 20-25 ug either IV or SC respectively at 90 minutes interval till hCG administration | |
| Hyperprolactenemia | Dopamine agonists |
| • Bromocriptine 2.5 – 20 mg daily | |
| • Cabergoline 0.25 - 1 mg twice weekly | |
| • Quinagolide 25 – 150 daily | |
| Hypothalamo – Pituitary dysfunction PCOS | • Weight loss |
| • Clomiphene citrate (CC)/Letrozole/Tamoxifen | |
| • CC – 50- 150 mg Day 2-6 | |
| • Letrozole 2.5 – 5 mg Day 3-7 | |
| • Gonadotrophins IUI cycle - start with 37.5 – 75 IUI and increase if necessary | |
| • Gonadotrophins IVF cycle – Start with dose of 100- 225 IU depending on age, BMI, AFC and AMH | |
| • GnRH analogues - GnRH antagonist preferred in PCOS women | |
| • Others one can use GnRH agonist Long or short protocol or GnRH antagonist depending on AMH and AFC | |
| • Ovarian surgery – LOD Beneficial in Lean PCOS and those with high LH concentrations Insulin sensitizers: May have a role in PCOS women | |
| • Metformin can be used in the dose of 500 mg twice or three times a day can be increased by 500 mg till a maximum dose of 2500 mg per day | |
| • A dose of 850 mg twice a day may also be used | |
| Hypergonadotrophic hypogonadism | • Success rate poor |
| • GnRHa in ultra short protocol with hMG | |
| • Oocyte donation/Adoption | |
| • HRT to prevent osteoporosis and CVS disease |
The choice between pulsatile GnRH or gonadotropins in this category depends on the intactness of the pituitary. Pulsatile GnRH may be used if the pituitary is intact. It is given subcutaneously or intravenously every 90 minutes. Its place in current practice needs to be evaluated
Gonadotropin therapy is ideal and more cost–effective that can be considered even when the pituitary is not functioning. Both FSH and LH are required for ovulation induction as there is no endogenous LH. With only FSH, follicles may grow but results in inadequate estrogen production. The dose of gonadotropin to achieve monofollicular growth, a low–dose step–up must be considered to avoid hyperstimulation
Counselling for prolonged stimulation is also recommended and luteal support is needed after ovulation induction as endogenous gonadotropin secretion is likely to be inadequate to support normal luteal function. Follicular monitoring should be a must
Treatment with exogenous progesterone or additional small doses of hCG–2000 IU every 3 days during the luteal phase of ovulation induction cycles has been shown to increase the pregnancy rates
Assisted reproductive technology (ART)
Intrauterine insemination (IUI) may be combined with ovulation induction if there is no pregnancy. If ovulation induction along with IUI does not lead to pregnancy, then IVF can be considered
WHO Group II anovulatory infertility principles of treatment
Before treatment, the underlying disorders such as hyperprolactinemia, hypothyroidism, and adrenal disorders should be treated before commencing infertility therapy
Lifestyle modifications such as optimization of BMI, blood glucose levels, smoking cessation to be optimized, diet, exercise, sleep, anxiety, mental, social, and sexual health, and minimization of alcohol consumption are needed to be considered in the success of the treatment
Weight loss of 5% improves insulin sensitivity and may lead to spontaneous ovulation
The lowest effective dosage of fertility drugs is to be considered to achieve monofollicular ovulation
Counseling is essential as the number of days taken to ovulate may be more
Ovulation induction therapy should be administered monthly until pregnancy is achieved or for up to six cycles. In cases of unsuccessful therapy prolonged use of ovulation induction agents should be avoided, due to poor success rates
4.2 Ovulatory drugs for PCOS
Table below highlights the drugs used for ovulation induction
Table 6.
Medication used for ovulation induction
| Drugs used for ovulation Induction | GnRH analogues |
|---|---|
| Anti Estrogens | • GnRH agonists |
| 1. Clomiphene citrate | • GnRH antagonists |
| 2. Tamoxifen/Raloxifene | |
| Aromatase inhibitors | |
| 1. Letrozole | |
| 2. Anastrozole | |
| Gonadotropins | |
| • Urinary or highly purified hMG | |
| • Purified or highly purified u–FSH | |
| • Recombinant FSH (r–FSH) | |
| • Recombinant LH | |
| Combinations of oral agents with gonadotropins |
FSH: follicle stimulating hormone; GnRH: gonadotropin-releasing hormone; hMG: human menopausal gonadotropin; LH: luteinizing hormone.
4.2.1 First–line pharmacological management in women with anovulatory infertility
4.2.1.1 Role of letrozole in ovulation induction in anovulation infertility
Letrozole can be considered as the first–line drug in the therapeutic management of ovulation induction in women with PCOS with anovulatory infertility to avoid multiple pregnancy and ovarian hyperstimulation with clomiphene
Dose 2.5–5mg daily from day 3–7
Letrozole use is associated with a reduced risk of multiple pregnancy in comparison to clomiphene citrate
4.2.1.2 Clomiphene citrate
Starting dose 50 mg; maximum dose –150 starting on any day between day 2–5 and given for 5 days
Dose correlates with body weight, age, indication for use (anovulation, PCOS, COH), and past history
Dose cannot be accurately predicted
Requires empiric incremental titration to establish lowest effective dose
-
To be discontinued if two consecutive cycles anovulatory with maximum dose or If endometrial thickness <7 mm at ovulation
-
»CC failure could be due to
-
»Failure to ovulate due to high BMI, Free androgen index, LH or Insulin levels
-
»Ovulation but no conception due to
-
»antiestrogen effects on cervical mucus or endometrium
-
»High LH
-
»Improvement of results with CC if
- - Monitor for antioestrogen effects:
- - Decrease insulin
- - weight loss
- - insulin lowering medications
-
»
4.2.1.3 Adjuvants: hCG, dexamethasone, dopamine agonist
-
»
Decrease LH
-
»
Pretreatment suppression of LH and androgens with OC/progesterone
-
»
LOD
4.2.1.4 Addition of metformin to clomiphene citrate
Clomiphene improves ovulation and pregnancy rates and is preferred to administer along with metformin. Metformin alone in women with PCOS improves ovulation and pregnancy but not live birth rates due to increased pregnancy complications. Also, in most cases metformin is not used as an ovulation–inducing agent rather it is used as an insulin sensitizer
Women prescribed metformin should beinformed of the side–effects (such as nausea, vomiting, and other GI disturbances) associated with its use
Clomiphene could be combined with metformin, rather than persisting with clomiphene alone as it improves ovulation, pregnancy, and live birth rates in women with PCOS who are obese (BMI ≥30 kg/m2)
-
Monitoring is needed with clomiphene to avoid multiple pregnancy and hyperstimulation
-
»Ultrasound monitoring during the first cycle of treatment must be considered to ensure that they are taking a dose that minimizes the risk of multiple pregnancy, ensure a positive response, and adequate endometrial development
-
»
Importantly, while using clomiphene, the healthcare professional should be aware that
Routine luteal support not required unlike WHO group I
15% of women do not respond to clomiphene and are resistant
4.2.2 Second–line pharmacological/surgical management in women with anovulatory infertility
Gonadotropins or laparoscopic ovarian surgery is recommended as second–line therapy in women with group II anovulatory infertility with clomiphene–resistance after counseling on the benefits and risks of each therapy
4.2.2.1 Gonadotropins can be considered as second–line management
In specific selected cases, gonadotropins can be used as first–line treatment, provided that women can undergo monitoring and are counseled about risk and cost
Gonadotropins can be used in different ovulation induction regimens either a low–dose step–up or a step–down regimen. The risk of multiple pregnancy and ovarian hyperstimulation syndrome with the use of gonadotropins is very tough to establish. However, considering the low–dose step–up regimen (37.5–50 IU), the risk can be reduced and unifollicular development can be achieved in non–ART cycles
The Figure 2 a-f below show the different protocols with gonadotropins
In women with clomiphene-resistance, gonadotropin with the addition of metformin can be used along with considering the aspects such as patient counselling on cost, monitoring, risk of multiple pregnancy and ovarian hyperstimulation
According to the Leeds study (>10-year period; 1998–2008), gonadotropin ovulation induction showed an overall ovulation rate of 67.4% (523/775 cycles). The overall cumulative clinical pregnancy rate after 5–cycles was 47.7% (Figure 4) with a twinning rate of 10.8%
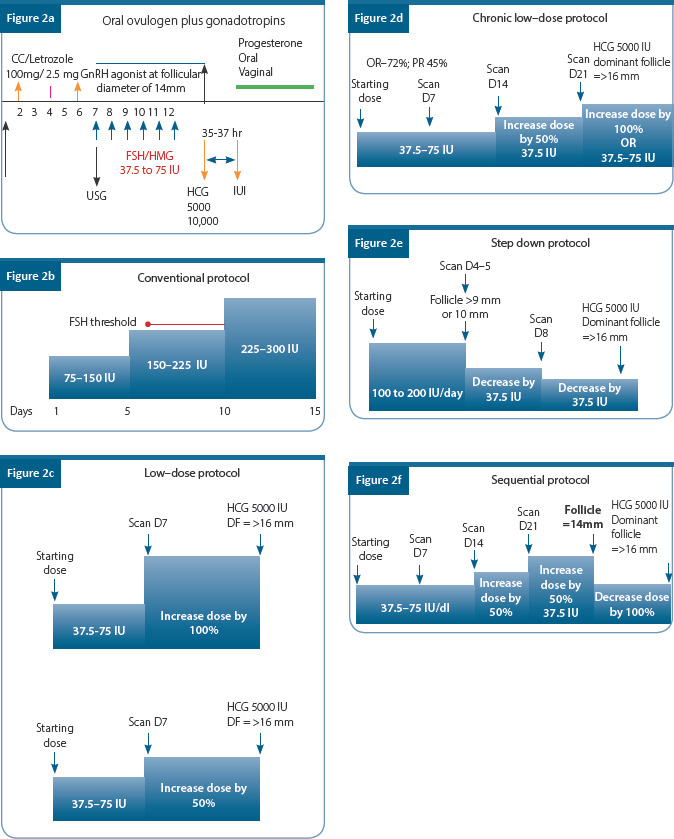
4.2.2.2 Laparoscopic ovarian surgery
The results with ovarian drilling are similar to gonadotropins but have the advantage of no intensive monitoring and spontaneous conception
The risks, advantages, and disadvantages should be explained to all women and decisions should be taken after comparing costs, recurrence of treatment, the existence of a person with expertise in chosen treatment side–effects, and risks like adhesions and decreased ovarian reserve which may occur with surgery
Laparoscopic ovarian drilling can be considered as first–line in Indian rural women who cannot come back repeatedly for monitoring
4.2.3 Anti–obesity agents and bariatric surgery in women with anovulatory infertility
To improve fertility, pharmacological anti–obesity agents and bariatric surgery can be used as an experimental therapy in PCOS women with anovulatory infertility who do not ovulate with maximum dose of ovulation induction drugs
4.2.4 Third–line management in women with anovulatory infertility
Role of in vitro fertilization (IVF)/ intracytoplasmic sperm injection (ICSI)
In PCOS women with anovulatory infertility where first–or second–line ovulation induction therapies have failed, IVF/ICSI can be recommended as third–line therapy in the absence of an absolute indication for IVF/ICSI
-
Women who are recommended to IVF/ICSI treatment, the GnRH antagonist protocol must be preferred and an elective frozen embryo transfer strategy could be considered
-
»Women with PCOS undergoing IVF ± ICSI therapy should be counseled before starting treatment, including on cost and risk of ovarian hyperstimulation syndrome and methods of tackling it
-
»
Either urinary or recombinant FSH can be used as there is insufficient evidence to suggest a difference between various FSH preparations. No significant differences were seen between human menopausal gonadotropins (hMG) and urinary FSH in rates per cycle of pregnancy, multiple pregnancy, miscarriage, ovulation, or overstimulation
-
Recombinant LH not recommended for use in combination with FSH therapy. Unlike the WHO I category, these women do not require LH during stimulation
-
»GnRH antagonist protocol is preferred in women with PCOS to avoid OHSS by using agonists trigger and freeze all policy
-
»Also, the GnRH agonist protocol should not be offered as it does not improve pregnancy rates, and it is associated with an increased risk of ovarian hyperstimulation. If GnRH agonist protocol is used, then human chorionic gonadotropins (hCG) smallest dose (1000 mg to 1500 mg daily) to trigger final oocyte and adjunct metformin therapy should be used as it reduces the risk of OHSS
-
»
4.2.5 Is fertile window extended in women with polycystic ovarian syndrome
-
»
Despite a higher oocyte yield in all age groups, women with PCOS over age 40 had similar CPR and LBR when compared to women with tubal factor infertility
-
»
Reproductive window may not be extended in PCOS and that patients with infertility should be treated in a timely manner despite indicators of high ovarian reserve
4.2.6. Long–term health outcomes of ovulation induction and ovarian stimulation
-
»
No direct association has been found between these treatments and invasive cancer
-
»
Information about long–term health outcomes in women and children is still awaited
-
»
For a better outcome, the use of ovulation induction or ovarian stimulation agents should be limited to the lowest effective possible dose and duration
4.3 WHO Group III anovulatory infertility principles of treatment:
-
»
The only realistic treatment option for women classified as WHO group III anovulatory infertility is egg donation. Besides, they require long-term hormone replacement therapy to prevent the deleterious effects of hypoestrogenism on their bones
Conclusion and future perspectives
Even though the evidence–based approach is practiced by the gynecologists, embryologists, and infertility specialists in reproductive medicine for a long–period, large multicenter, randomized controlled trials (RCTs) are rare in the field of ovulation induction. Also, there is a lack of RCTs or multicentre trials from India
There is a strong need to strengthen and promote meaningful research so we can have enough data to formulate our guidelines, otherwise, we will continue to depend on the guidelines and recommendations which may not apply to our patients and our practice in India
Summary of recommendations
Increase safety and effectiveness
Optimizing response to increase live birth rate
Minimize risk of OHSS and multiple pregnancy by stimulation individualization
Recommendations for ovulation induction, trigger, and LPS
| Category | Recommendation | Grade of Recommendation | Quality of evidence |
|---|---|---|---|
| EBR | For predicting high and poor response to ovarian stimulation, use of either antral follicle count (AFC) or anti–Müllerian hormone (AMH) is recommended over other ovarian reserve tests | A | I |
| CCR | Pre–treatment with estrogen and progesterone or COCP in an GnRH antagonist cycle is not recommended | C | - |
| EBR | GnRH antagonist protocol is recommended for PCOS women and for predicted high responders to improved safety and equal efficacy | A | I |
| EBR | There is insufficient evidence to recommend the addition of letrozole to gonadotropins in stimulation protocols for predicted high responders | C | IV |
| EBR | The GnRH antagonist protocol is recommended for predicted high responders. However, if GnRH agonist protocols are used, a reduced gonadotropin dose is probably recommended to decrease the risk of OHSS | C | III |
| EBR | The GnRH antagonist protocol is recommended for predicted normal responder women and in general IVF/ICSI population with regards to improved safety | B | II |
| EBR | GnRH antagonists and GnRH agonists are equally recommended for predicted poor responders | C | III |
| CCR | Clomiphene citrate alone or in combination with gonadotrophins, and gonadotropin stimulation alone are equally recommended for predicted poor responders | A | - |
| CCR | The addition of letrozole to gonadotropins in stimulation protocols is probably not recommended for predicted poor responders | C | - |
| EBR | A gonadotropin dose higher than 300 IU is not recommended for predicted poor responders | A | II |
| CCR | The use of modified natural cycle is probably not recommended over conventional ovarian stimulation for predicted poor responders | D | - |
| EBR | If GnRH agonists are used, the long GnRH agonist protocol is probably recommended over the short or ultrashort GnRH agonist protocol | C | III |
| EBR | The use of recombinant FSH (rFSH) and human menopausal gonadotropin (hMG) for ovarian stimulation is equally recommended | A | I |
| EBR | No advantage in using recombinant LH (rLH) + recombinant FSH (rFSH) for ovarian stimulation over hMG in regards to safety | C | III |
| EBR | Routine use of adjuvant metformin before and/or during ovarian stimulation is not recommended with the GnRH antagonist protocol for women with PCOS | A | II |
| CCR | Use of adjuvant growth hormone before and/or during ovarian stimulation is probably not recommended for poor responders | C | III |
| EBR | Use of testosterone or DHEAS before ovarian stimulation is probably not recommended for poor responders | C | III |
| CCR | Random-start ovarian stimulation is probably not recommended for the general IVF/ICSI population Should be reserved for ovulation Induction in cancer patients | C | - |
| Research point | Double stimulation in poor responders should only be used in the context of clinical research Can be considered for urgent fertility preservation cycles | Research point | - |
| CCR | All ovulation induction should be monitored by ultrasound The addition of a hormonal panel consisting of a combination of oestradiol, progesterone and LH measurements to ultrasound monitoring is probably not recommended | D | - |
| CPP | The decision on timing of triggering in relation to follicle size is multi-factorial, taking into account the size of the growing follicle cohort, the hormonal data on the day of pursued trigger, duration of stimulation, patient burden, financial costs, experience of previous cycles, and organizational factors for the centre. Most often, final oocyte maturation is triggered at sizes of several of the leading follicles between 16–22 mm | - | |
| CCR | A poor response to ovarian stimulation alone is not a reason to cancel a cycle | B | - |
| EBR | The use of recombinant hCG and urinary hCG is equally effective and either can be used for triggering final oocyte maturation during ovarian stimulation | A | II |
| EBR | hCG 5000 IU is preferred to 10,000 IU in an GnRH agonist cycle | C | III |
| EBR | A GnRH agonist trigger is recommended for final oocyte maturation in women at risk of OHSS | B | I |
| CCR | It is not recommended to administer recombinant LH for triggering final oocyte maturation | B | - |
| EBR | The use of GnRH agonist for final oocyte maturation with conventional luteal support and fresh transfer is not recommended in the general IVF/ICSI population | A | II |
| CCP | If the GnRH agonist trigger with triptorelin is applied, dosages ranging of 0.1–0.4 mg can be chosen | - | |
| EBR | The addition of a GnRH agonist to hCG as a dual trigger for final oocyte maturation is probably not recommended for predicted normal responders | C | II |
| EBR | Progesterone is recommended for luteal phase support after IVF/ICSI | A | I |
| CPP | Starting of progesterone for luteal phase support should be in the window between the evening of the day of oocyte retrieval and day 3 post oocyte retrieval | - | - |
| EBR | The addition of oestradiol to progesterone for luteal phase support is probably not recommended. | C | III |
| Research point | A GnRH agonist bolus, in addition to progesterone for luteal phase support in hCG triggered cycles can only be used in the context of a clinical trial. | Research only | - |
| CPP | A freeze–all strategy is recommended to eliminate the risk of late–onset OHSS and is applicable in both GnRH agonist and GnRH antagonist protocols. | - | |
| EBR | If a GnRH agonist trigger with freeze–all strategy is not used in patients at risk of OHSS, should be followed by luteal phase support with LH–activity | C | IV |
| EBR | In women classified as WHO group III anovulatory infertility, egg donation is the only realistic treatment option. Along with this, they must be considered for long–term hormone replacement therapy to prevent the deleterious effects of hypoestrogenism on their bones. | C | IV |
References
Quaas A, Dokras A. Diagnosis and treatment of unexplained infertility. Rev Obstet Gynecol.
2008;1(2):69-76. http://www.ncbi.nlm.nih.gov/pubmed/18769664. Accessed November 19, 2019.
Liu K, Case A; Reproductive endocrinology and infertility committee. Advanced reproductive age and fertility. J Obstet Gynaecol Can. 2011;33(11):1165–75.
Diagnostic evaluation of the infertile male: a committee opinion: Practice Committee of the American Society for Reproductive Medicine. Fertil Steril. 2015
Gorthi S, Balen AH, Tang T. Current issues in ovulation induction. The Obstetrician & Gynaecologist. 2012;14:188–196.
Prathibha D, Govardhani M, Krishna PT. Prolactin levels in infertility and bromocriptine therapy in hyperprolactinaemia. J Indian Med Assoc. 1994;92(12):397–9.
Agrawal M, Samal S, Hariharan C, Agarwal S. Prevalence of hyperprolactinemia in infertile cases and its correlation with TSH in a rural set up hospital. Int J Reprod Contracept Obstet Gynecol. 2013;2(4):626–30.
Binita G, Suprava P, Mainak C, Koner BC, Alpana S. Correlation of prolactin and thyroid hormone concentration with menstrual patterns in infertile women. J Reprod Infertil. 2009;10(3):207– 212.
Hivre MD, Bhale DV, Mahat RK, Bujurge AA. Study of serum TSH and prolactin levels in patients of female infertility. International Journal of Recent Trends in Science And Technology. 2013;9(1):144–5.
Taylor A. ABC of subfertility: extent of the problem. BMJ. 2003;327(7412):434–6.
Ahuja M. Age of menopause and determinants of menopause age: A PAN India survey by IMS. J Midlife Health. 2016;7(3):126–31.
Jeyaseelan L, Antonisamy B, Rao PS. Pattern of menstrual cycle length in south Indian women: a prospective study. Soc Biol. 1992;39(3-4):306–9.
WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–63.
Zimmerman Y, Eijkemans MJ, Coelingh Bennink HJ, et al. The effect of combined oral contraception on testosterone levels in healthy women: a systematic review and meta-analysis. Hum Reprod Update. 2014;20(1):76–105.
Nadaraja RND, Sthaneshwar P, Razali N. Establishing the cut off values of androgen markers in the assessment of polycystic ovarian syndrome. Malays J Pathol. 2018;40(1):33–9.
Binita G, Suprava P, Mainak C, et al. Correlation of prolactin and thyroid hormone concentration with menstrual patterns in infertile women. J Reprod Infertil. 2009;10(3):207–12.
Pleş L, Alexandrescu C, Ionescu CA, et al. Three-dimensional scan of the uterine cavity of infertile women before assisted reproductive technology use. Medicine (Baltimore). 2018; 97(41):e12764.
Priya D, Akhtar N, Ahmad J. Prevalence of hypothyroidism in infertile women and evaluation of response of treatment for hypothyroidism on infertility. Indian J Endocrinol Metab. 2015;19(4):504–506.
Verma I, Sood R, Juneja S, Kaur S. Prevalence of hypothyroidism in infertile women and evaluation of response of treatment for hypothyroidism on infertility. Int J Appl Basic Med Res. 2012;2(1):17–9.
Bharti G, Singh K, Kumari R, Kumar U. Prevalence of hypothyroidism in subfertile women in a tertiary care centre in North India. Int J Res Med Sci. 2017;5(5):1777–80.
WHO. Laboratory manual for the examination and processing of human semen, fifth edition, 2010.
Practice Committee of the American Society for Reproductive Medicine (ASRM), Evaluation of the azoospermic male: a committee opinion. Fertil Steril. 2018;109:777–82.
Leiva RA, Bouchard TP, Abdullah SH, Ecochard R. Urinary Luteinizing Hormone Tests: Which Concentration Threshold Best Predicts Ovulation? Front Public Health. 2017;5:320.
Chizen, D, Pierson, R. Transvaginal ultrasonography and female infertility. Glob libr women’s med. 2010;(ISSN:1756–2228).
Bjorndahl L, Barratt C, Mortimer D, et al. ‘How to count sperm properly’: checklist for acceptability of studies based on human semen analysis. Hum Reprod. 2016;31(2):227–32.
Hrehorcak M, Nargund G. “One-Stop” fertility assessment using advanced ultrasound technology. Facts Views Vis Obgyn. 2011;3(1):8–12.
Badawy A, Wageah A, EL Gharib M, Osman EE. Prediction and diagnosis of poor ovarian response: the dilemma. J Reprod Infertil. 2011;12(4):241–8.
Torrealday S, Kodaman P, Pal L. Premature Ovarian Insufficiency - an update on recent advances in understanding and management. F1000Res. 2017;6:2069.
Rasool S, Shah D. Fertility with early reduction of ovarian reserve: the last straw that breaks the Camel’s back. Fertil Res Pract. 2017;3:15.
Jirge PR. Ovarian reserve tests. J Hum Reprod Sci. 2011;4(3):108–13.
Jindal UN. Mid-life fertility: Challenges & policy planning. Indian J Med Res. 2018;148:S15–S26.
Singh N, Malik E, Banerjee A, et al. “Anti-Mullerian Hormone: Marker for ovarian response in controlled ovarian stimulation for IVF patients”: A first pilot study in the Indian population. J Obstet Gynaecol India. 2013;63(4):268–72.
Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence- based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018;33(9):1602–18.
Katsikis I, Kita M, Karkanaki A, et al. Anovulation and ovulation induction. Hippokratia.2006;10(3):120–7.
Costello MF, Garad RM, Hart R, et al. A review of second- and third-line infertility treatments and supporting evidence in women with polycystic ovary syndrome. Med Sci (Basel). 2019;7(7).
Chapter 11: Polycystic Ovarian Syndrome and Infertility Management Recommendations
OVERVIEW
This guideline offers recommendations on diagnosis, pharmacological, and surgical management of infertility associated with polycystic ovarian syndrome (PCOS). It also covers recommendations on counselling required for an infertile woman with anovulatory PCOS.
1. Introduction
PCOS is a complex endocrine, metabolic, reproductive, and psychological system disorder affecting women of reproductive age group
The prevalence rate of PCOS in India is 3.7%–22.5%
-
Cardinal features of PCOS include:
-
»
Chronic anovulation
-
»
Androgen excess
-
»
Polycystic ovarian morphology (PCOM)
-
»
2. PCOS and infertility
Clinical–pathological basis of infertility
Two out of the three criteria if present, qualify the patient as having PCOS. Since these symptoms are present in varying combinations, the resultant phenotypes are also many and varying
Based on the presence of anovulation, hyperandrogenemia, and PCOM, women with PCOS were divided into four phenotypes (as per Rotterdam criteria), Table 1
-
Clinical manifestations of PCOS
-
Metabolic aspects:
-
»
Obesity
-
»
Insulin resistance
-
»
Type 2 diabetes (10% by age 40s)
-
»
Cardiovascular disease
-
»
Table 1.
Characters of PCOS phenotype
| Androgen levels | LH levels | Ovarian size | AMH levels | Body weight | Insulin resistance | |
|---|---|---|---|---|---|---|
| PHENOTYPE A (Classic) | Increased | Increased | Increased | Increased | Increased | Increased |
| PHENOTYPE B (Classic, normal ovaries) | Increased | Moderately increased | Normal | Mild increase | Increased | Increased |
| PHENOTYPE C (Ovulatory) | Moderately increased | Normal | Moderately increased | Mild increase | Moderately increased | Moderately increased |
| PHENOTYPE D (Normo–androgenic) | Mild increase | Normal | Moderately increased | Normal | Normal | Normal |
Table 2.
Summary of recommendations for defining irregular cycles
| Category | Recommendation | Grade |
|---|---|---|
| CCR | When irregular menstrual cycles are present a diagnosis of PCOS should be considered and assessed according to the guidelines • Normal in the first year post menarche as part of the pubertal transition • >1 to <3 years post menarche: <21 or >45 days • >3 years post menarche to perimenopause: <21 or >35 days or <8 cycles per year • >1 year post menarche >90 days for any one cycle • Primary amenorrhea by age 15 or >3 years post thelarche (breast development) |
A |
| CCR | In an adolescent with irregular menstrual cycles, the value and optimal timing of assessment and diagnosis of PCOS should be discussed with the patient, taking into account diagnostic challenges at this life stage and psychosocial and cultural factors | A |
| CPP | For adolescents who have features of PCOS but do not meet diagnostic criteria, an “increased risk” could be considered and reassessment advised at or before full reproductive maturity, 8 years post menarche | — |
| CPP | Ovulatory dysfunction can still occur with regular cycles and if anovulation needs to be confirmed serum progesterone levels can be measured | — |
PCOS: polycystic ovary syndrome.
3. Investigations
-
Ultrasound scan (Table 3)
-
»
Rotterdam diagnostic criteria: Polycystic ovary contains 12 or more follicles measuring 2–9 mm in diameter on day 2 or 3 of MC and/or increased ovarian volume (>10 ml) with no dominant follicle >10 mm or CL
-
»
Does not apply to women taking OCP, as ovarian size is reduced, even though the polycystic appearance may persist
-
»
-
Androgen profile (Tables 4 and 5)
-
»
Testosterone – Total and free <5.0 nmol/l
-
»
FAI
-
»
+/- 17OH–P, adrenal profile
-
»
SHBG–surrogate for insulin resistance (16– 119 nmol/l)
-
»
Follicle-stimulating hormone (FSH), luteinizing hormone (LH)
Anti-Mullerian hormone (AMH): Evidence for assessment of AMH as a diagnostic modality is highlighted in Table 6
Assessment glucose intolerance/insulin resistance and lipid profile
Prolactin/Thyroid Function Test (TFTs)
Table 3.
Recommendations for assessment of PCOS on ultrasound
| Category | Recommendation | Grade |
|---|---|---|
| CCR | Ultrasound should not be used for the diagnosis of PCOS in those with a gynaecological age of <8 years (<8 years after menarche), due to the high incidence of multi–follicular ovaries in this life stage | A |
| CPP | Transabdominal ultrasound should primarily report ovarian volume with a threshold of >10 ml, given the difficulty of accurately assessing follicle number. | — |
| CCR | The transvaginal ultrasound approach is preferred in the diagnosis of PCOS, if sexually active and if acceptable to the individual being assessed | A |
| CPP | If using lower resolution USG transducers (frequency <8 MHz) the threshold for PCOM should be FNPO of ≥12 and/or ovarian volume of ≥10 ml. | — |
| CCR | Using endovaginal USG transducers with frequency bandwidth > 8 MHz the threshold for PCOM should be FNPO of ≥ 20 and/or an ovarian volume ≥ 10ml on either ovary, ensuring no corpora lutea, cysts or dominant follicles are present | B |
| CPP | In patients with irregular menstrual cycles and hyperandrogenism, an ovarian ultrasound is not necessary for PCOS diagnosis; however, ultrasound will identify the complete PCOS phenotype. | — |
| CPP | Clear protocols are recommended for reporting AFC per ovary and ovarian volume on ultrasound. Recommended minimum reporting standards include: • Last menstrual period • Transducer frequency • Approach/route assessed • Total follicle number per ovary measuring 2–9 mm • Three dimensions and volume of each ovary • Reporting of endometrial thickness and appearance is preferred – 3-layer endometrial assessment may be useful to screen for endometrial pathology • Other ovarian and uterine pathology, as well as ovarian cysts, corpus luteum, dominant follicles ≥equal 10 mm. |
— |
FNPO: follicle number per ovary.
Table 4.
Recommendations for clinical hyperandrogenism
| Category | Recommendation | Grade | Quality |
|---|---|---|---|
| CCR | A comprehensive history and physical examination should be completed for symptoms and signs of clinical hyperandrogenism, including acne, alopecia and hirsutism, in adolescents, severe acne, and hirsutism. | A | — |
| CCR | Health professionals should be aware of the potential negative psychosocial impact of clinical hyperandrogenism. Reported unwanted excess hair growth and/or alopecia should be considered important, regardless of apparent clinical severity. | A | — |
| CCR | Standardized visual scales are preferred when assessing hirsutism, such as the modified Ferriman Gallwey score (mFG) with a level ≥4–6 indicating hirsutism, depending on ethnicity, acknowledging that self–treatment is common, and can limit clinical assessment. | A | — |
| CCR | The Ludwig visual score is preferred for assessing the degree and distribution of alopecia. | A | — |
| CPP | There are no universally accepted visual assessments for evaluating acne. | — | — |
| CPP | The prevalence of hirsutism is the same across ethnicities, yet the mFG cut–off scores for defining hirsutism, and the severity of hirsutism varies by ethnicity (In Indian women >/–7). | — | — |
| CPP | As ethnic variation in vellus hair density is notable, over–estimation of hirsutism may occur if vellus hair is confused with terminal hair; only terminal hairs need to be considered in pathological hirsutism, with terminal hairs clinically growing >5mm in length if untreated, varying in shape, and texture and generally being pigmented. | — | — |
Table 5.
Recommendations for biochemical hyperandrogenism
| Category | Recommendation | Grade | Quality |
|---|---|---|---|
| EBR | Calculated free testosterone, free androgen index or calculated bioavailable testosterone should be used to assess biochemical hyperandrogenism in the diagnosis of PCOS | A | III |
| EBR | High quality assays such as liquid chromatography–mass spectrometry (LCMS)/mass spectrometry and extraction/chromatography immunoassays, should be used for the most accurate assessment of total or free testosterone in PCOS | B | III |
| EBR | Androstenedione and DHEAS could be considered if total or free testosterone are not elevated–provide limited additional information in the diagnosis of PCOS | B | III |
| CCR | Direct free testosterone assays, (radiometric or enzyme–linked assays) should not be used in assessment of biochemical hyperandrogenism in PCOS–demonstrate poor sensitivity, accuracy, and precision | A | — |
| CPP | Reliable assessment of biochemical hyperandrogenism is not possible in women on hormonal contraception, due to effects on sex hormone–binding globulin, and altered gonadotrophin–dependent androgen production | ||
| CPP | Where assessment of biochemical hyperandrogenism is important in women on hormonal contraception, drug withdrawal is recommended for three months or longer before measurement, and contraception management with a non–hormonal alternative is needed during this time | ||
| CPP | Assessment of biochemical hyperandrogenism is most useful in establishing the diagnosis of PCOS and/or phenotype where clinical signs of hyperandrogenism (in particular hirsutism) are unclear or absent | ||
| CPP | Interpretation of androgen levels needs to be guided by the reference ranges of the laboratory used, acknowledging that ranges for different methods and laboratories vary widely. Normal values are ideally based on levels from a well phenotype healthy control population or by cluster analysis of a large general population considering age and pubertal specific stages | ||
| CPP | Where androgen levels are markedly above laboratory reference ranges, other causes of biochemical hyperandrogenism need to be considered. History of symptom onset and progression is critical in assessing for neoplasia, however, some androgen–secreting neoplasms may only induce mild to moderate increases in biochemical hyperandrogenism. |
Table 6.
Assessment of AMH as diagnostic criteria
| Category | Recommendation | Grade | Quality |
|---|---|---|---|
| EBR | Serum AMH levels should not yet be used as an alternative for the detection of PCOM or as a single test for the diagnosis of PCOS. | B | III |
| CPP | There is emerging evidence that with improved standardization of assays and established cut off levels or thresholds based on large scale validation in populations of different ages and ethnicities, AMH assays will be more accurate in the detection of PCOM. | — | — |
3.1 Other assessments for PCOS
Metabolic screening
Clinical - Acanthosis nigricans and truncal obesity
Fasting Lipids –1–3 yearly
Screening for glucose tolerance in PCOS
-
WHO criteria
-
»
2 hour 75 gm glucose tolerance test (OGTT)
-
»
Impaired glucose tolerance (IGT) 140–199 mg/dl
-
»
Diabetes mellitus (DM) ≥200 mg/dl
-
»
-
ADA criteria
-
»
Fasting glucose level
-
»
IFG 100–125 mg/dl
-
»
DM ≥126 mg/dl
-
»
Insulin levels not done due to assay variability (depending on age, gender, and feeding status) and inaccuracy ( absence of validated assay)
-
»
Recommendations for diagnosing impaired glucose tolerance and diabetes mellitus is shown in Table 7.
Table 7.
Recommendations–Impaired glucose tolerance and type 2 diabetes
| Category | Recommendation | Grade |
|---|---|---|
| CCR | Health professionals and women with PCOS should be aware that, regardless of age, the prevalence of GDM, IGT, and type 2 diabetes (5 fold in Asia, 4 fold in the Americas and 3 fold in Europe) are significantly increased in PCOS, with risk independent of, yet exacerbated by, obesity | A |
| CCR | Glycaemic status should be assessed at baseline in all women with PCOS. Thereafter, assessment should be every one to three years, influenced by the presence of other diabetes risk factors | A |
| CCR | An oral glucose tolerance test (OGTT), fasting plasma glucose or HbA1c should be performed to assess glycaemic status. In high–risk women with PCOS (including a BMI >25kg/m2 or in Asians >23kg/m2, history of impaired fasting glucose, impaired glucose tolerance or gestational diabetes, family history of diabetes mellitus type 2, hypertension or high–risk ethnicity), an OGTT is recommended | A |
| CCR | A 75–g OGTT should be offered in all women with PCOS preconception when planning pregnancy or seeking fertility treatment, given the high risk of hyperglycaemia, and the associated comorbidities in pregnancy. If not performed preconception, an OGTT should be offered at <20 weeks gestation, and all women with PCOS should be offered the test at 24–28 weeks gestation | A |
Consensus for defining an Asian Indian for metabolic syndrome is highlighted in Table 8
Table 8.
Consensus for definition of Asian Indian for metabolic syndrome
| Definition | Abdominal obesity (cm) | Dysglycemia FBS mg/dl | Hypertension mm Hg | High Triglycerides mg/dl |
|---|---|---|---|---|
| International Diabetic Federation (IDF) | >80 Non–obligatory criteria | ≥ 100 | ≥130/≥85 | ≥150 |
| IDF | >80 Obligatory criteria | ≥ 100 | ≥130/≥85 | ≥150 |
| Modified national cholesterol education program, adult treatment plan III (NCEP, ATP III) | >88 Non–obligatory criteria | ≥ 100 | ≥130/≥85 | ≥150 |
Diagnosis of PCOS is that of exclusion. One needs to exclude other causes of menstrual irregularity and hyperandrogenaemia. (Table 9)
Table 9.
To diagnose PCOS exclude other disorders therefore PCOS is diagnosis of exclusion
| Condition | Exclude by |
|---|---|
| Pregnancy | Beta human chorionic gonadotropin |
| Ovarian failure | Follicle-stimulating hormone |
| Hypothyroidism | Thyroid-stimulating hormone |
| Hyperprolactinemia | Prolactin |
| Congenital adrenal hyperplasia | 17–OH progesterone |
| Ovarian tumor | Total testosterone (especially if >200 ng/dl) |
| Adrenal tumor | Dehydroepiandrosterone sulfate (especially if >800 mcg/dl) |
| Cushing’s syndrome | Serum cortisol |
Table 10.
Assessment of PCOS
| Clinical assessment | Androgen profile | Exclude secondary causes |
|---|---|---|
| • Menstrual cycle • Progesterone if cycles regular • Ovarian morphology (absence of HA and Irregular cycles) • AMH not recommended • Androgen excess • Impaired glucose tolerance |
• Free testosterone • Free androgen index • SHBG |
• Clinical history and examination • Thyroid function test • Prolactin • FSH • 17–OH progesterone |
AMH: anti-müllerian hormone, FSH: follicle-stimulating hormone; HA: hyper androgenism; SHBG: sex hormone binding globulin.
4. Management of infertility
4.1 Strategies
Preconceptional counselling
Lifestyle modifications
Pharmacological interventions
Surgical management
Assisted reproductive technologies
4.2 Pre–conceptional counselling
Clinical need/Rationale/Existing guidelines
Quality of life may be compromised in women with PCOS as the symptoms are associated with anxiety, depression, low self–esteem, perception of loss of feminine identity, and sexual dysfunction and this may trigger social isolation
Health care providers should be well aware of the physiological and emotional wellbeing of the woman with PCOS. Psychological co–morbidities require respectful consideration and assessment
Prior to initiating therapy, explanation on the purpose, proper information regarding the treatment, implication, expected results should be provided for patients. Although this may increase the consultation time, but it may help in building trust and rapport with the patient and justifies their right of being informed
-
Patient counselling prior to therapies should include:
-
»
Identify and rectify risk factors (cease smoking and limit alcohol consumption)
-
»
Offer education regarding the behavioral changes and chances of pregnancy
-
»
Importance of multivitamins, vitamin D, folate, iron, and calcium
-
»
Advice on healthy weight for obese women
-
»
Encourage exercise in PCOS women; however, exercise interventions do not always require clinical centers, expensive gyms and fitness centers
-
»
Ovarian hyperstimulation syndrome (OHSS), long term
-
»
Avoid pregnancy for 12–18 months after bariatric surgery
-
»
Recommendations
Consider counselling prior to initiating therapies for PCOS women in order to identify and correct the long term risk factors associated with fertility (Grade A, EL 4)
Provide pre-treatment counselling for PCOS women on weight reduction using lifestyle modification (Grade A, EL 4)
During the course of therapy, emphasis the role of a husband and family in the emotional wellbeing of subfertile PCOS women (Grade B, EL4)
Advise the patients on the duration of the procedure, types, side effects, success rate, and cost of treatment (Grade B, EL 4)
4.3 Lifestyle modifications
Clinical /Rationale/Existing guidelines
-
Evidence defines obesity as a BMI ≥25 for Asian Indians (Reference)
-
»
Additionally, obesity is strongly associated with PCOS and can occur in up to 50% of the patients
-
»
Compared to thin women with PCOS, obese women with PCOS are more likely to experience anovulation
-
»
There is an increased risk of the poor obstetric outcome, spontaneous abortion, preterm labor, maternal complications, thromboembolism, gestational diabetes mellitus, wound infection, and gestational hypertension in obese women
-
»
Therefore awareness, monitoring, early intervention are vital and there is a need for health care professionals in helping obese women with empathy to control their weight
-
»
4.3.1 Treatment of obesity is multifaceted
4.3.1.1 Diet and exercise
7% weight loss is recommended
Diet and exercise go hand in hand in achieving best outcomes in weight reduction
Consider yoga and meditation as a holistic approach for treating the root cause of PCOS (obesity and stress)
4.3.1.2 Diet and exercise along with pharmacological ovulation–inducing agents
Lifestyle management in comparison to clomiphene citrate alone or in combination with metformin showed a higher pregnancy rate
4.3.1.3 Pharmacological weight–reducing agents
Both orlistat and sibutramine have displayed weight loss resulting in improvement in cardiovascular risk factors, hyperandrogenemia, and insulin resistance (IR)
Do not consider these as first–line therapy in obese women with PCOS for reducing weight
Recommendations
Consider lifestyle modification as a first–line treatment for reducing weight before attempting pharmacological methods of ovulation induction in subfertile women with PCOS. (Grade A, EL 1)
-
Lifestyle modification should include
-
»
Calorie restriction with any hypocaloric diet (reduced by 500 kcal/day)
-
»
Moderate physical activity of 45–60 min/day
-
»
Restriction of excessive caffeine intake, alcohol consumption, and smoking (Grade A, El 2)
-
»
Consider appropriate age–related decline in fertility when considering the duration of lifestyle management interventions (Grade B, EL 4)
PCOS patients who are morbidly obese should avoid pharmacological methods of ovulation induction prior to weight reduction (Grade B, EL 4)
Consider pharmacological preparations in morbidly obese patients under medical supervision in case of unsuccessful weight reduction with diet or exercise alone (Grade B, EL 1)
4.4 Ovulation Induction
4.4.1 Aromatase inhibitors
Recommendations
-
Consider letrozole (2.5 mg/day for 10 days) as a first–line treatment for ovulation induction in women
-
»
Who have PCOS with anovulatory and no other infertility factors
-
»
Who has breast cancer and PCOS requiring oocyte cryopreservation
-
»
Consider other ovulation induction agents in case letrozole is not available or its use is not permitted
4.4.2 Clomiphene citrate
Recommendations
Consider clomiphene citrate as a first–line pharmacological agent in anovulatory PCOS women with subfertility at a starting dose of 50–100 mg/day starting from day 2 to day 5 of the menstrual cycle for 5 days. Clomiphene citrate (CC) recommended for ovulation induction is gradually increased by 50 mg/day at each cycle to a maximum of 150 mg/day for a maximum of six cycles (Grade A, EL 1)
Consider ultrasound monitoring in infertile PCOS women who are on clomiphene citrate for ovulatory response and also to reduce the risk of multiple pregnancies. Monitoring of LH levels can be another alternative in case ultrasound monitoring is not available. (Grade B, EL3)
4.4.3 Addition of Insulin–sensitizing agent- metformin
Clomiphene and insulin
Recommendation
-
Consider metformin in the following circumstances:
-
»
In PCOS patients with impaired glucose intolerance
-
»
In obese PCOS women co–administered with clomiphene citrate
-
»
In clomiphene citrate resistant PCOS women
-
»
In PCOS women who are at high risk of hyperstimulation
-
»
Sustained release preparations are recommended for better compliance
4.4.4 Gonadotropins and GnRH analogs
Recommendations
Offer gonadotropins as a second–line treatment for not more than three ovulatory cycles in PCOS women with CCR or who failed to conceive with no other subfertility factors (Grade A, EL 2)
Advise patients on the need for strict monitoring of cycle, the risk of OHSS and multiple pregnancies, treatment cost, and cycle cancellation criteria prior to initiating gonadotropin therapy (Grade B, EL 4)
Consider low–dose step-up protocol over step–down protocol when gonadotropins are indicated for reducing the chances of OHSS in PCOS patients with subfertility (Grade A, EL 2)
Consider gonadotropin at an initial dose of 37.5–75.0 IU/day for 7–10 days depending on BMI and previous response. In the case of follicle ≥12 mm is not developed or ovulation is triggered with the development of follicle ≥18 mm in size, then consider small dose increments of 50% of the initial or previous dose. (Grade B, EL 4)
Gonadotrophin induced ovulation is only triggered when there are fewer than three mature follicles and needs to be cancelled if there are more than two mature follicles with the patient advised to avoid unprotected intercourse. (CPP)
Gonadotrophins with the addition of metformin, could be used rather than gonadotrophin alone, in women with PCOS with anovulatory infertility, clomiphene citrate–resistance and no other infertility factors, to improve ovulation, pregnancy and live birth rates. (Grade B, EL 2)
-
Where gonadotrophins are prescribed, considerations include: (Grade B, EL 3)
-
»
Cost and availability
-
»
Expertise required for use in ovulation induction
-
»
Degree of intensive ultrasound monitoring required
-
»
Lack of difference in clinical efficacy of available GT preparations
-
»
Low dose gonadotrophin protocols optimise monofollicular development
-
»
Risk and implications of potential multiple pregnancy
-
»
4.5 Surgical management
4.5.1 Bariatric surgery
Recommendations
Consider bariatric surgery in obese subfertile PCOS women who are unsuccessful in reducing weight by lifestyle management as a second–line option (Grade B, EL 4)
Bariatric surgery is recommended as first–line therapy for weight reduction in PCOS patients with BMI >40 kg/m2 (Grade B, EL 4)
Advise to avoid conception after bariatric surgery for at least 12 months for PCOS women with subfertility as the effects of these interventions on the evolution of early pregnancy are not yet known (Grade B, EL 4)
4.5.2 Laparoscopic drilling
Recommendations
Consider laparoscopic ovarian drilling as a second-line therapy over gonadotropin therapy in anovulatory PCOS women who have failed first–line oral ovulation induction therapy or who have CCR (clomiphene resistant) and hypersecretion of LH levels with no other subfertility factors. (Grade A, EL 1)
LOD (laparoscopic ovarian drilling) should be considered in anovulatory PCOS women with CCR with no other subfertility factors, or who cannot access hospital facility for intensive monitoring, or required gonadotropin therapy or laparoscopic assessment of their pelvis (Grade C, EL4)
The number of punctures should be limited to a maximum of 4–6 depending on the size of the ovary at wattage 40 (Grade B, EL 4)
-
Where laparoscopic ovarian surgery is to be recommended, the following need to be considered:
-
»
Comparative cost
-
»
Expertise required for use in ovulation induction
-
»
Intra–operative and post–operative risks are higher in women who are overweight and obese
-
»
Are may be a small associated risk of lower ovarian reserve or loss of ovarian function
-
»
Periadnexal adhesion formation may be an associated risk
-
»
In non–fertility indications, severe male factors and in obstructive tubal disease, laparoscopic ovarian drilling (LOD) should not be considered
4.6 Assisted reproductive technology
4.6.1 Intrauterine insemination
Recommendations
Consider IUI along with ovulation induction in anovulatory subfertile PCOS women with associated male factor subfertility
Recommend IUI in anovulatory subfertile PCOS women with unsuccessful conception despite ovulation induction
4.6.2 In vitro fertilization
Recommendations
IVF is considered as third line treatment options who have failed to conceive or who have other indications for IVF (Grade A, EL 2)
Consider GnRH antagonist protocol over the GnRH agonist long protocol in anovulatory subfertile PCOS women undergoing IVF for reducing the incidence of severe OHSS at similar clinical pregnancy rates (Grade A, EL 2)
Gonadotropin should be considered at an initial dose of 75–225 IU/day for 7–10 days based on age and follicle size (Grade B, EL 4)
GnRH agonist should be used for trigger. Either single dose of Triptorelin 0.3mg (Decapeptyl®) or 1 mg of leuprolide acetate or buserelin
4.6.3 In vitro maturation
Recommendation
Consider IVM in units with sufficient expertise to achieve pregnancy and live birth rates in women with PCOS who are at standard IVF/ICSI treatment without the risk of OHSS, where an embryo is generated, vitrified, thawed, and transferred in a subsequent cycle
4.6.4 Luteal phase support
Recommendation
Offer luteal phase with progesterone in subfertile PCOS women who are undergoing ovulation induction or assisted reproduction (Grade A, EL 1)
HCG as LPS should be avoided
PCOS is an insulin resistance (IR) syndrome, a gender-specific form of Metabolic Syndrome, hence also called “Syndrome X”
There is ONE defect that is IR with consequent hyperinsulinemia
There are TWO underlying hormonal factors: Hyperinsulinemia and hyperandrogenemia
-
Its THREE key features are:
Oligo –/ anovulation
Hyperandrogenism
PCO morphology
There are FOUR possible phenotypes
Assessment of PCOS is based on clinical assessment, androgen profile and by excluding secondary causes (Table 1)
The diagnostic algorithm for PCOS is highlighted in Figure 1
Life-style modifications should be advised before OI in obese PCOS women
Dietary intervention and increased physical activity in overweight/obese improve IR and hyperandrogenism, menstrual function and fertility
Aromatase Inhibitors is as effective as CC and should be used as first line drug
CC still may be used for OI in women with AI resistance or failure
Metformin alone is less effective than CC in inducing ovulation in women with PCOS
Addition of metformin to CC may be indicated in specific sub–group of PCOS women
GT in low dose protocols aiming at monofollicular development is an effective treatment option
COS regimens offer an opportunity to correct abnormal systemic endocrine environment in vivo
Safer to use low dose step–up protocol
When the ovarian response has been previously documented, the threshold dose can be initiated from the start
LOD is as effective as GT for OI and achievement of pregnancy but with significantly less multiples
Management of anovulatory infertility in PCOS in depicted in Figure 2
iCOS with eSET should be order of the day to achieve optimal outcome after ART and Reduce complications
Modifying conventional stimulation protocols according to patients’ characteristics and ovarian reserve makes it patient–friendly and optimizes the chance of LBR
Metformin could be used alone in women with PCOS, with anovulatory infertility and no other infertility factors, to improve ovulation, pregnancy and live birth rates, although women should be informed that there are more effective ovulation induction agents
If metformin is being used for ovulation induction in women with PCOS who are obese (BMI ≥30kg/m2) with anovulatory infertility and no other infertility factors, CC could be added to improve ovulation, pregnancy and live birth rates
Adjunct metformin therapy could be used before and/or during follicle stimulating hormone ovarian stimulation in women with PCOS undergoing a IVF ± ICSI therapy with a GnRH agonist protocol, to improve the clinical pregnancy rate, and reduce the risk of OHSS
-
In a GnRH agonist protocol with adjunct metformin therapy, in women with PCOS undergoing IVF ± ICSI treatment, the following could be considered:
-
»
metformin commencement at the start of GnRH agonist treatment
-
»
metformin use at a dose of between 1000mg to 2550 mg daily
-
»
metformin cessation at the time of the pregnancy test or menses (unless the metformin therapy is otherwise indicated)
-
»
metformin side–effects
-
»
In IVF ± ICSI cycles, women with PCOS could be counselled on potential benefits of adjunct metformin in a GnRH antagonist protocol to reduce risk of OHSS
No conclusions is drawn regarding other insulin-sensitizing drugs as no studies reported primary outcomes
Vitamin D binds to vitamin D receptor and activates peroxisome proliferator activator receptor-δ (PPAR δ) which stimulates the expression of insulin receptor and enhances insulin–mediated glucose transport
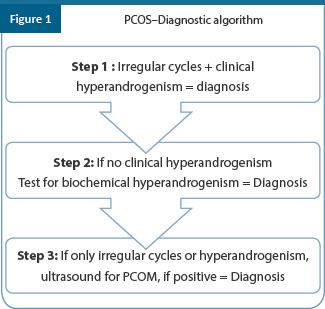
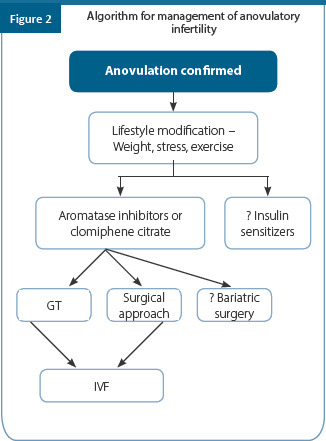
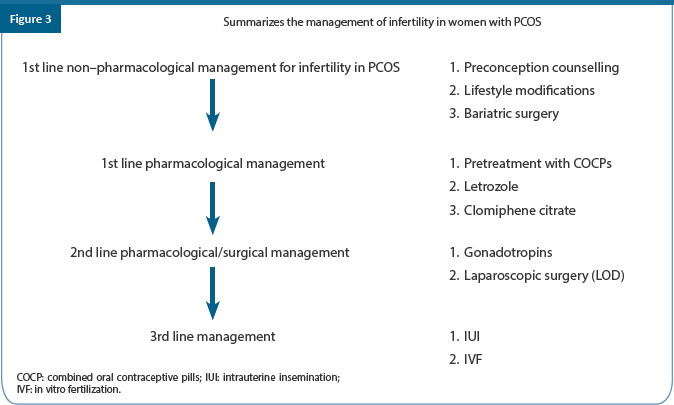
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CCR | Tubal patency testing should be considered prior to ovulation induction in women with PCOS where there is suspected tubal infertility. (Previous abdominal or pelvic sepsis, previous pelvic and/or abdominal surgery, cases of recurrent acute pelvic pain, history of sexual transmitted diseases or pelvic inflammatory disease, or endometriosis) | B | - |
| EBR | Lifestyle intervention (preferably multicomponent including diet, exercise and behavioural strategies) should be recommended in all those with PCOS and excess weight, for reductions in weight, central obesity, and insulin resistance | B | III |
| CPP | Achievable goals such as 5% to 10% weight loss in those with excess weight yields significant clinical improvements and is considered successful weight reduction within six months. Ongoing assessment and monitoring is important during weight loss and maintenance in all women with PCOS | - | - |
| CCR | All those with PCOS should be offered regular monitoring for weight changes and excess weight | A | - |
| CPP | Pregnancy needs to be excluded prior to ovulation induction | - | - |
| EBR | Letrozole should be considered first line pharmacological treatment for ovulation induction in women with PCOS with anovulatory infertility and no other infertility factors to improve ovulation, pregnancy and live birth rates | A | III |
| CPP | Where letrozole is not available or use is not permitted or cost is prohibitive, health professionals can use other ovulation induction agents | - | - |
| EBR | Clomiphene citrate could be used alone in women with PCOS with anovulatory infertility and no other infertility factors to improve ovulation and pregnancy rates | B | IV |
| EBR | Metformin could be used alone in women with PCOS, with anovulatory infertility and no other infertility factors, to improve ovulation, pregnancy and live birth rates, although women should be informed that there are more effective ovulation induction agents | B | II |
| EBR | Clomiphene citrate could be used in preference, when considering clomiphene citrate or metformin for ovulation induction in women with PCOS who are obese (BMI is ≥ 30 kg/m2) with anovulatory infertility and no other infertility factors | B | III |
| EBR | If metformin is being used for ovulation induction in women with PCOS who are obese (BMI ≥ 30kg/m2) with anovulatory infertility and no other infertility factors, clomiphene citrate could be added to improve ovulation, pregnancy and live birth rates | B | III |
| EBR | Clomiphene citrate could be combined with metformin, rather than persisting with clomiphene citrate alone, in women with PCOS who are clomiphene citrate-resistant, with anovulatory infertility and no other infertility factors, to improve ovulation and pregnancy rates | B | III |
| CPP | The risk of multiple pregnancy is increased with clomiphene citrate use and therefore monitoring needs to be considered | - | - |
| EBR | Gonadotrophins could be used as second line pharmacological agents in women with PCOS who have failed first line oral ovulation induction therapy and are anovulatory and infertile, with no other infertility factors | B | III |
| EBR | Gonadotrophins with the addition of metformin, could be used rather than gonadotrophin alone, in women with PCOS with anovulatory infertility, clomiphene citrate–resistance and no other infertility factors, to improve ovulation, pregnancy, and live birth rates | B | II |
| CPP | Gonadotrophin induced ovulation is only triggered when there are fewer than three mature follicles and needs to be cancelled if there are more than two mature follicles with the patient advised to avoid unprotected intercourse | - | - |
| EBR | Laparoscopic ovarian surgery could be second–line therapy for women with PCOS, who are clomiphene citrate resistant, with anovulatory infertility and no other infertility factors | B | III |
| CCR | In the absence of an absolute indication for IVF ± intracytoplasmic sperm injection (ICSI), women with PCOS and anovulatory infertility could be offered IVF as third–line therapy where first or second line ovulation induction therapies have failed | B | - |
| CPP | Women with PCOS undergoing IVF ± ICSI therapy need to be counselled prior to starting treatment including on: availability, cost and convenience increased risk of ovarian hyperstimulation syndrome options to reduce the risk of ovarian hyperstimulation | - | - |
| CPP | In women with anovulatory PCOS, the use of IVF is effective and when elective single embryo transfer is used multiple pregnancies can be minimised | - | - |
| CCR | Urinary or recombinant follicle stimulation hormone can be used in women with PCOS undergoing controlled ovarian hyperstimulation for IVF ± ICSI, with insufficient evidence to recommend specific follicle stimulating hormone (FSH) preparations | B | |
| EBR | A gonadotrophin releasing hormone antagonist protocol is preferred in women with PCOS undergoing an IVF ± ICSI cycle, over a gonadotrophin releasing hormone agonist long protocol, to reduce the duration of stimulation, total gonadotrophin dose and incidence of ovarian hyperstimulation syndrome (OHSS) | B | III |
| CPP | Human chorionic gonadotrophins is best used at the lowest doses to trigger final oocyte maturation in women with PCOS undergoing an IVF ± ICSI cycle to reduce the incidence of OHSS | - | - |
| CPP | Triggering final oocyte maturation with a gonadotropin–releasing hormone (GnRH) agonist and freezing all suitable embryos could be considered in women with PCOS having an IVF/ICSI cycle with a GnRH antagonist protocol and at an increased risk of developing OHSS or where fresh embryo transfer is not planned | - | - |
| CPP | In IVF ± ICSI cycles in women with PCOS, consideration needs to be given to an elective freeze of all embryos | - | - |
| EBR | Adjunct metformin therapy could be used before and/or during follicle stimulating hormone ovarian stimulation in women with PCOS undergoing a IVF ± ICSI therapy with a GnRH agonist protocol, to improve the clinical pregnancy rate, and reduce the risk of OHSS | B | III |
| CCR | In a GnRH agonist protocol with adjunct metformin therapy, in women with PCOS undergoing IVF ± ICSI treatment, the following could be considered: Metformin commencement at the start of GnRH agonist treatment metformin use at a dose of between 1000 mg to 2550 mg daily metformin cessation at the time of the pregnancy test or menses (unless the metformin therapy is otherwise indicated) | B | - |
| CCR | In units with sufficient expertise, IVM could be offered to achieve pregnancy and live birth rates approaching those of standard IVF ± ICSI treatment without the risk of OHSS for women with PCOS, where an embryo is generated, then vitrified and thawed and transferred in a subsequent cycle | B | - |
| CCR | Bariatric surgery should be considered an experimental therapy in women with PCOS, for the purpose of having a healthy baby, with risk to benefit ratios currently too uncertain to advocate this as fertility therapy | D |
References
Moreira S, Soares E, Tomaz G, et al. Polycystic ovary syndrome: A psychosocial approach. Acta Med Port. 2010; 23: 237–42.
Misra A, Chowbey P, Makkar BM, et al. Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. J Assoc Physicians India. 2009; 57: 163–70.
Hoeger KM. Obesity and lifestyle management in polycystic ovary syndrome. Clin Obstet Gynecol. 2007; 50: 277–94.
Mani H, Davies MJ, Bodicoat DH, et al. Clinical characteristics of polycystic ovary syndrome: Investigating differences in white and south Asian women. Clin Endocrinol (Oxf). 2015; 83: 542– 9.
Hart R, Doherty DA. The potential implications of a PCOS diagnosis on a woman’s long-term health using data linkage. J Clin Endocrinol Metab. 2015; 100: 911–9.
Jamil AS, Alalaf SK, Al-Tawil NG, Al-Shawaf T. Comparison of clinical and hormonal characteristics among four phenotypes of polycystic ovary syndrome based on the Rotterdam criteria. Arch Gynecol Obstet. 2016; 293: 447–56.
Panidis D, Tziomalos K, Papadakis E, et al. Associations of menstrual cycle irregularities with age, obesity, and phenotype in patients with polycystic ovary syndrome. Hormones (Athens). 2015; 14: 431–7.
Faucett AM, Metz TD, DeWitt PE, Gibbs RS. Effect of obesity on neonatal outcomes in pregnancies with preterm premature rupture of membranes. Am J Obstet Gynecol. 2016; 214: 287.e1–5.
Cody F, Unterscheider J, Daly S, et al. The effect of maternal obesity on sonographic fetal weight estimation and perinatal outcome in pregnancies complicated by fetal growth restriction. J Clin Ultrasound. 2016; 44: 34–9.
Gaudet L, Wen SW, Walker M. The combined effect of maternal obesity and fetal macrosomia on pregnancy outcomes. J Obstet Gynaecol Can. 2014; 36: 776–84
Maiya AG, Sheela RK, Kumar P. Exercise-induced weight reduction and fertility outcomes in women with polycystic ovarian syndrome who are obese and infertile: A preliminary report. J Exerc Sci Physiother. 2008; 4: 30–4.
Karimzadeh MA, Javedani M. An assessment of lifestyle modification versus medical treatment with clomiphene citrate, metformin, and clomiphene citrate-metformin in patients with polycystic ovary syndrome. Fertil Steril. 2010; 94: 216–20.
Sabuncu T, Harma M, Nazligul Y, Kilic F. Sibutramine has a positive effect on clinical and metabolic parameters in obese patients with polycystic ovary syndrome. Fertil Steril. 2003; 80: 1199–204.
Vosnakis C, Georgopoulos NA, Armeni AK, et al. Sibutramine administration decreases serum anti-Müllerian hormone (AMH) levels in women with polycystic ovary syndrome. Eur J Obstet Gynecol Reprod Biol. 2012; 163: 185–9.
Florakis D, Diamanti-Kandarakis E, Katsikis I, et al. Effect of hypocaloric diet plus sibutramine treatment on hormonal and metabolic features in overweight and obese women with polycystic ovary syndrome: A randomized, 24-week study. Int J Obes (Lond). 2008; 32: 692–9.
Kumar P, Arora S. Orlistat in polycystic ovarian syndrome reduces weight with improvement in lipid profile and pregnancy rates. J Hum Reprod Sci. 2014; 7:2 55–61.
Nidhi R, Padmalatha V, Nagarathna R, Ram A. Effect of a yoga program on glucose metabolism and blood lipid levels in adolescent girls with polycystic ovary syndrome. Int J Gynaecol Obstet. 2012; 118: 37–41.
Nidhi R, Padmalatha V, Nagarathna R, Amritanshu R. Effect of a holistic yoga program on anxiety symptoms in adolescent girls with polycystic ovarian syndrome: A randomized control trial. Int J Yoga. 2012; 5: 112–7.
Javnbakht M, Hejazi Kenari R, Ghasemi M. Effects of yoga on depression and anxiety of women. Complement Ther Clin Pract. 2009; 15: 102–4.
Thessaloniki ESHRE/ASRM-sponsored PCOS consensus workshop group. Consensus on infertility treatment related to polycystic ovary syndrome. Hum Reprod. 2008; 23: 462–77.
Long term consequences of polycystic ovary syndrome. RCOG. Green-top Guideline No. 33. Available from: https://www.rcog.org.uk/globalassets/documents/guidelines/gt33_longtermpcos.pdf.
Escobar-Morreale HF, Botella-Carretero JI, Alvarez-Blasco F, et al. The polycystic ovary syndrome associated with morbid obesity may resolve after weight loss induced by bariatric surgery. J Clin Endocrinol Metab. 2005; 90: 6364–9.
Eid GM, Cottam DR, Velcu LM, et al. Effective treatment of polycystic ovarian syndrome with Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2005; 1: 77–80.
Bobde JA, Bhosle D, Kadam R, Shelke S. Comparison of efficacy and safety of metformin, an oral contraceptive combination of Ethinyl estradiol and drospirenone alone or in combination in polycystic ovarian syndrome. J Obes Metab Res. 2014; 1: 112–7.
Bhattacharya SM, Jha A, DasMukhopadhyay L. Comparison of two contraceptive pills containing drospirenone and 20 μg or 30 μg Ethinyl estradiol for polycystic ovary syndrome. Int J Gynaecol Obstet. 2016; 132: 210–3
Adashi EY. Clomiphene citrate: mechanism(s) and site(s) of action--a hypothesis revisited. Fertility & Sterility. 1984; 42(3): p. 331–44.
Kamath MS, Aleyamma TK, Chandy A, George K. Aromatase inhibitors in women with clomiphene citrate resistance: A randomized, double-blind, placebo-controlled trial. Fertil Steril. 2010; 94: 2857–9.
Banerjee Ray P, Ray A, Chakraborti PS. Comparison of efficacy of letrozole and clomiphene citrate in ovulation induction in Indian women with polycystic ovarian syndrome. Arch Gynecol Obstet 2012; 285: 873–7.
Teede HJ, Misso ML, Costello MF. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018; 33(9): 1602-1618.
Homburg R. Clomiphene citrate − End of an era? A mini-review. Hum Reprod. 2005; 20: 2043– 51.
Messinis IE. Ovulation induction: A mini-review. Hum Reprod. 2005; 20: 2688–97.
Palomba S, Falbo A, Zullo F, Orio F Jr. Evidence-based and potential benefits of metformin in the polycystic ovary syndrome: A comprehensive review. Endocr Rev. 2009; 30: 1–50
Hoeger K, Davidson K, Kochman L, et al. The impact of metformin, oral contraceptives, and lifestyle modification on polycystic ovary syndrome in obese adolescent women in two randomized, placebo-controlled clinical trials. J Clin Endocrinol Metab. 2008; 93: 4299–306.
Tang T, Lord JM, Norman RJ, et al. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, d-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea, and subfertility. Cochrane Database Syst Rev. 2012; CD003053.
Johnson NP, Stewart AW, Falkiner J, et al. PCOSMIC: A multi-center randomized trial in women with polycystic ovary syndrome evaluating metformin for infertility with clomiphene. Hum Reprod. 2010; 25: 1675–83.
Cheraghi E, Soleimani Mehranjani M, Shariatzadeh MA, et al. Co-administration of metformin and N-acetyl cysteine fails to improve clinical manifestations in PCOS individual undergoing ICSI. Int J Fertil Steril. 2014; 8: 119–28.
Palomba S, Orio F Jr, Falbo A, et al. Prospective parallel randomized, double-blind, double- dummy controlled clinical trial comparing clomiphene citrate and metformin as the first-line treatment for ovulation induction in nonobese anovulatory women with polycystic ovary syndrome. J Clin Endocrinol. Metab 2005; 90: 4068–74.
Morin-Papunen L, Rantala AS, Unkila-Kallio L, et al. Metformin improves pregnancy and live- birth rates in women with polycystic ovary syndrome (PCOS): A multicenter, double-blind, placebo-controlled randomized trial. J Clin Endocrinol Metab. 2012; 97: 1492–500.
Creanga AA, Bradley HM, McCormick C, Witkop CT. Use of metformin in polycystic ovary syndrome: A meta-analysis. Obstet Gynecol. 2008; 111: 959–68.
Siebert TI, Kruger TF, Steyn DW, Nosarka S. Is the addition of metformin efficacious in the treatment of clomiphene citrate-resistant patients with polycystic ovary syndrome? A structured literature review. Fertil Steril. 2006; 86: 1432–7.
Moll E, van der Veen F, van Wely M. The role of metformin in polycystic ovary syndrome: A systematic review. Hum Reprod Update. 2007; 13: 527–37.
Homburg R, Hendriks ML, König TE, et al. Clomifene citrate or low-dose FSH for the first-line treatment of infertile women with anovulation associated with polycystic ovary syndrome: A prospective randomized multinational study. Hum Reprod. 2012; 27: 468–73
López E, Gunby J, Daya S, et al. Ovulation induction in women with polycystic ovary syndrome: Randomized trial of clomiphene citrate versus low-dose recombinant FSH as first-line therapy. Reprod Biomed Online. 2004; 9: 382–90.
Mukharjee S, Sharma S, Chakravarty BN. Comparative evaluation of pregnancy outcome in gonadotrophin-clomiphene combination vs. clomiphene alone in polycystic ovarian syndrome and unexplained infertility − A prospective clinical trial. J Hum Reprod Sci. 2010; 3: 80–4.
Stein I. Duration of infertility following ovarian wedge resection. West Journal of Surgery. 1964; 72: p. 237–559.
Gjønnæss H. Polycystic ovarian syndrome treated by ovarian electrocautery through the laparoscope. Fertility & Sterility. 1984; 41: p. 20–25S
S Ganesh A, Goswami SK, Chattopadhyay R, et al. Comparison of letrozole with continuous gonadotropins and clomiphene-gonadotropin combination for ovulation induction in 1387 PCOS women after clomiphene citrate failure: A randomized prospective clinical trial. J Assist Reprod Genet. 2009; 26: 19–24.
Tehraninejad, E.S, et al. Comparison of GnRH antagonist with long GnRH agonist protocol after OCP pretreatment in PCOS patients. Arch Gynecol Obstet. 2010; 282(3): p. 319–25.
Lainas TG. Flexible GnRH antagonist protocol versus GnRH agonist long protocol in patients with polycystic ovary syndrome treated for IVF: A prospective randomized controlled trial (RCT). Hum Reprod. 2010. 25(3): p. 683–9
Haydardedeoglu B. IVF/ICSI outcomes of the OCP plus GnRH agonist protocol versus the OCP plus GnRH antagonist fixed protocol in women with PCOS: a randomized trial. Arch Gynecol Obstet. 2012; 286(3): p. 763–9.
Jacobs H.S, R.R. Homburg. The endocrinology of conception. Baillieres Clin Endocrinol Metab. 1990; 4(2): p. 195–205.
Huang X. A systematic review and meta-analysis of metformin among patients with polycystic ovary syndrome undergoing assisted reproductive technology procedures. Int J Gynaecol Obstet. 2015; 131(2): p. 111–6.
Kjotrod SB, von During V, Carlsen SM. Metformin treatment before IVF/ICSI in women with polycystic ovary syndrome: A prospective, randomized, double-blind study. Hum Reprod. 2004. 19(6): 1315–22.
Lin, K. C. Coutifaris. In vitro fertilization in the polycystic ovary syndrome patient: An update. Clin Obstet Gynecol. 2007. 50(1): p. 268–76.
Legro R.S. Ovulation induction in polycystic ovary syndrome: Current options. Best Pract Res Clin Obstet Gynaecol. 2016. 37: p. 152–59.
Walls M.L. In vitro maturation as an alternative to standard in vitro fertilization for patients diagnosed with polycystic ovaries: A comparative analysis of fresh, frozen and cumulative cycle outcomes. Hum Reprod. 2015. 30(1): p. 88–96.
Pastore, L.M. Depression symptoms and body dissatisfaction association among polycystic ovary syndrome women. J Psychosom Res. 2011. 71(4): p. 270–6.
Teede HJ, Misso ML, Deeks AA, et al. Assessment and management of polycystic ovary syndrome: Summary of an evidence-based guideline. Med J Aust. 2011; 195: S65–112
Vause TD, Cheung AP, Sierra S, et al. Ovulation induction in polycystic ovary syndrome. J Obstet Gynaecol Can 2010; 32: 495–502.
Costello MF, Misso ML, Balen A, et al. Evidence summaries and recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome: Assessment and treatment of infertility Hum Reprod Open. 2019; 2019(1):hoy021.
Chapter 12: Unexplained Infertility
OVERVIEW
This guideline offers recommendations on the identification criteria for detection of unexplained infertility. It also gives an overview of few diagnostic tests and management recommended for patients with unexplained infertility.
1. Definition of unexplained infertility
A couple whose routine standard, basic investigations of infertility showed no abnormality can be labelled as having unexplained infertility (UI). Diagnostic terminology of UI is not used to describe presence of a medical condition, but a void or a negative. Negatives are however, practically impossible to prove
Diagnosis of UI was appropriate, as long as
Ovulation is confirmed but even apparently normally ovulating women may produce poor quality oocytes and embryos
Tubal patency has been proven but patent fallopian tubes do not necessarily function normally
Semen analysis is normal but fertilization potentials of sperm still may be affected
So subtle abnormalities need to identified before labelling the couple to be having unexplained infertility
Prevalence: 25%–30% of all infertility
Introduction
Infertility is unexplained when the following criteria are met:
-
Normal ovulatory function confirmed by basal body temperature measurement, cervical mucus changes, serum/urinary luteinizing hormone (LH) surge or mid–luteal progesterone levels, or evidence of follicular rupture during ultrasound
-
»
Normal semen analysis, as per the WHO 2010 criteria
-
»
Bilateral patent tubes
-
»
The above criteria definition does not include the normal semen analysis, and therefore consider the following definition to identify patients
Infertility in spite of normal ovarian function, tubes, uterus, cervix, and pelvis in female partner, with normal semen analysis and genitourinary anatomy in male partner with normal coitus and coital frequency
Although, the above definition provides an idea to identify unexplained infertility, more evidences are required to resolve the queries regarding change in nomenclature of unexplained infertility to sub–fertility or adding women with minimal and mild endometriosis and men with subtle abnormal semen parameters and duration of infertility in the definition.
-
Six common conditions when not diagnosed tend to be labeled as UI. These include:
-
»
Mild endometriosis
-
»
Subtle tubal pathology
-
»
Premature ovarian ageing
-
»
Age related infertility
-
»
Immunological infertility
-
»
Sperm dysfunction
-
»
2. Evaluation of a couple with unexplained infertility
Consider performing a thorough, systematic and physical examination along with detailed review of history of both male and female partners
-
Consider carrying out the following tests for the evaluation of unexplained infertility
-
»
Tests of ovulatory function
-
-
Consider performing serial trans-vaginal ultrasonography (TVS), mid–luteal serum progesterone estimation (>3 ng/ml) or use urinary luteinizing hormone (LH) kits
-
-
Assess the antral follicle count (AFC) while performing the baseline transvaginal USG
-
-
AMH to be done if AFC is less or if women is more than 35 years
-
-
-
»
2.1 Husband’s semen analysis
Consider assessment of sperm concentration, motility, morphology, and vitality of male partner as per WHO 2010 criteria
Testing for DFI may provide a possible explanation for UI, therefore, it is reasonable to offer the same to these infertile couples as these couples may be better served by IVF or ICSI sooner rather than later (grade of evidence C)
Sperm survival test – The number of spermatozoa recovered after swim–up and the percentage of spermatozoa that maintain their motility after 24 hours were both helpful in assessing fertility potential of the sperms
2.2 Tests to assess tubal patency (hysterosalpingography/laparoscopy/saline infusion sonography)
Consider hysterosalpingography (HSG) as a first–line investigation for tubal patency evaluation when there is no of suspicion of pelvic pathology. It is traditional, less expensive and less invasive method
When pelvic pathology is suspected from either history, pelvic examination or USG
(e.g. endometriotic cyst, hydrosalpinx), diagnostic laparoscopy/hysteroscopy should be advised as first line investigation for evaluation of tubes and pelvis.
Laparoscopy may prove beneficial in unexplained infertility as it evaluates fallopian tubes, ovaries, tubo–ovarian relationship, pelvic peritoneum, periovarian and peri–tubal adhesions and also in mild to minimal endometriosis
2.3 Detection of Ovulation
Documentation of ovulation can be done by
Urinary LH kit - determines the LH surge and therefore time of ovulation
Mid luteal progesterone levels - Values of > or = 10ng/ml are suggestive of normal progesterone production
Trans vagina USG - Serial scan from day 9 for follicular grown and ovulation after an baseline scan on day 2 or 3
BBT - Not used these days
3. Differential diagnosis of unexplained infertility : Six common conditions when not diagnosed tend to be labeled as UI
Mild endometriosis
Subtle tubal pathology
Premature ovarian
Age related infertility associated with change in fertilizability & implantation potential of oocytes and embryos, Increased risk of embryonic chromosomal abnormalities, and Spontaneous abortions–Assess AFC, AMH and FSH, PGT–A to rule out aneuploidy
Immunological infertility – Most autoimmune disorders may be etiologically associated with infertility and so require evaluation. Testing of antiphospholipid, antinuclear, antithyroid, and antisperm antibodies may help.
Sperm dysfunction – Despite normal count and motility there could be reduction in acrosome reaction, oocyte binding, and zona penetration or there could be ultrastructural abnormalities of head and neck
4. Management of unexplained infertility
UI may be associated with subtle abnormalities or pathologies unidentified making management difficult and controversial. Selection of treatment depends on the prediction models for occurrence of spontaneous pregnancy. Cut–off point between good and poor prognosis was 30% when women’s age, duration of sub–fertility, type of sub–fertility, referral status, sperm motility, and post–coital status were taken into account. Those having a chance of conceiving spontaneously being ≥30% (good prognosis) were offered expectant line of treatment where as those with a chance of conceiving spontaneously being <30% (poor prognosis) should be offered IUI if female age was <38 years, for three to six COH/ IUI cycles before IVF. If female age is ≥38 years, IVF was offered directly
4.1 Life style changes
Counsel patients to maintain normal BMI (18– 25 kg/m2) by conscious calorie intake and exercise, reduce caffeine intake, alcohol, smoking, and other illicit substances
Advise couples to increase coital frequency (at least 2–3 times a week)
4.2 Expectant management
Expectant management for 2 years is the best choice for good prognosis when the woman’s age is less than 35 years with less than 2 years of infertility and normal ovarian reserve test. When expectant management is offered women needs to be aware of their ovulation time and the best period for unprotected intercourse
Consider age factor for infertility treatment because as per published study, approx 60% couples with unexplained infertility of 3 years duration where woman’s age is less than 25 years, chances of pregnancy is improved in first 3 years of expectant management. However, if woman’s age is more than 31 years, chances of pregnancy reduce by 10% on each subsequent year
4.3 Ovulation induction y
Clomiphene citrate and aromatase inhibitors does not offer any benefit over expectant management and should not be offered to couples with UI (Level 1A)
There is insufficient evidence to recommend gonadotropin–OS alone in the management of UI (Level III C)
4.4 Superovulation with intrauterine insemination
Natural–cycle IUI does not offer any benefit over expectant management and should not be offered in UI (Level 1A)
Either letrozole or clomiphene citrate (CC) can be used for IUI with oral agents (Level 1A)
COS with IUI is the treatment of choice if there is no pregnancy with expectant management, no pregnancy with OI with CC/letrozole and TI, age is more than 30 years and less than 35 years
Gonadotropin/IUI can be offered to couples with UI (Level IB)
Patients should be aware that gonadotropin/IUI is associated with a higher pregnancy rate per cycle and a higher multiple pregnancy rate per cycle than IUI with oral agents (Level IA)
4.5 Assisted reproductive technology (ART)– In vitro fertilization (IVF)/intracytoplasmic sperm injection (ICSI)
ART may be offered as first–line treatment if women’s age is more than 35 years or when ovarian reserve is poor or infertility >4 years
Serves as a diagnostic method for assessing egg quality and embryogenesis and split IVF and ICSI for those with no male factor
IVF should be offered to couples with UI after three cycles of ovarian stimulation/IUI have failed (Level 1A)
Consider options of study of embryo morpho–kinetics through time lapse technology and pre–implantation genetic testing for aneuploidies for selection of good embryo(s) for transfer wherever possible
5. Laboratory management
Evaluation and selection of sperm
Advanced sperm selections techniques are not recommended as routine. These needs larger trials before being incorporated in routine clinical practice
-
Oocyte quality
-
-
Evaluate oocyte quality to minimize fertilization failure
-
-
Abnormal cleavage/development/embryo quality
Options of study of morphokinetics through time laspse technology and PGTA may be given to patients for selection of good embryo(s) for transfer where ever possible
Consider pre–implantation genetic testing for evaluation of oocyte quality
Summary
Perform a thorough and systematic history and physical examination of both female and male partner
Better effort should be undertaken to develop reliable tools to diagnose, often undiagnosed conditions of endometriosis, tubal disease, premature ovarian ageing, and immunological infertility, which are often misdiagnosed for UI
A range of treatment options is available for unexplained infertility; however, the right treatment strategy needs to be customized according to the individual situation. Factors like the age of the female partner, duration of infertility, and previous pregnancies should be considered in choosing the optimal treatment protocol
Use serial transvaginal USG, mid–luteal serum progesterone estimation (>3 ng/ml) or by urinary LH kits for tests of ovulation
Consider estimation of ovarian reserve based on female’s age, AFC, and AMH, which may help in avoiding inadvertent delay in definitive treatment
Consider performing diagnostic laparoscopy/hysteroscopy assessment as first–line investigation if there is suspicion of pelvic pathology
Sperm survival and DFI testing may provide some clue to sperm dysfunction
Expectant management may be offered for a women <30 year of age and normal ovarian reserve with duration of infertility being less than 3 years.
Perform controlled ovarian stimulation (with clomiphene/letrozole/gonadotropins) along with IUI for 3–4 cycles when expectant management has failed or as first line in case of >30 year old lady, poor ovarian reserve or longer duration of infertility (>3 years)
Consider IVF/ICSI if IUIs have failed
Perform split IVF/ICSI of sibling oocytes to prevent total fertilization failure in first cycle itself as current evidence about universal application of ICSI for unexplained infertility except in cases of previous history of total fertilization failure yields conflicting results
Use sperm DNA fragmentation testing to customize treatment
Do not completely rely on the use of advanced sperm selection techniques for routine assessments; these need larger trials before being incorporated in routine clinical practice
Consider options of study of embryo morpho–kinetics through time lapse technology and PGT A for selection of good embryo(s) OR for transfer wherever possible
Summary of management of unexplained Infertility (Figure 1)
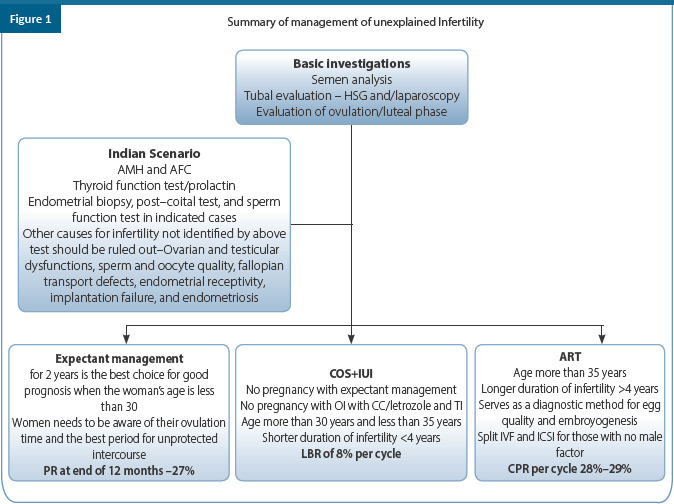
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| EBR | Perform a thorough and systematic history and physical examination of both female and male partner | B | II |
| EBR | Better effort should be undertaken to develop reliable tools to diagnose, often undiagnosed conditions of endometriosis, tubal disease, premature ovarian ageing, and immunological infertility, which are often misdiagnosed for UI | B | III |
| EBR | A range of treatment options is available for unexplained infertility; however, the right treatment strategy needs to be customized according to the individual situation. Factors like the age of the female partner, duration of infertility, and previous pregnancies should be considered in choosing the optimal treatment protocol | A | I |
| EBR | Use serial transvaginal USG, mid–luteal serum progesterone estimation (>3 ng/ml) or by urinary LH kits for tests of ovulation | B | III |
| EBR | Consider estimation of ovarian reserve based on female’s age, AFC and AMH which may help in avoiding inadvertent delay in definitive treatment | B | II |
| EBR | In the absence of evidence for tubal or other pelvic pathology, laparoscopy is not warranted in UI | B | II |
| EBR | Consider performing diagnostic laparoscopy/hysteroscopy assessment as first–line investigation if there is suspicion of pelvic pathology | A | II |
| EBR | Sperm survival and DFI testing may provide some clue to sperm dysfunction | D | IV |
| EBR | Expectant management may be offered for a women <30 year of age and normal ovarian reserve with duration of infertility being less than 3 years | A | I |
| EBR | Natural–cycleI UI does not offer any benefit over expectant management and should not be offered in UEI | A | I |
| EBR | Clomiphene citrate or letrozole alone does not offer any benefit over expectant management and should not be offered to couples with UI | A | I |
| EBR | Perform controlled ovarian stimulation (with clomiphene/letrozole/gonadotropins) along with IUI for 3–4 cycles when expectant management has failed or as first line in case of >30 year old lady, poor ovarian reserve or longer duration of infertility (>3 years) | A | I |
| EBR | Patients should be aware that gonadotropin/IUI is associated with a higher pregnancy rate per cycle and a higher multiple pregnancy rate per cycle than IUI with oral agents | A | I |
| EBR | Consider IVF/ICSI if IUIs have failed | A | I |
| EBR | IVF can be offered as an effective first–line treatment in unexplained infertility | B | I |
| EBR | There is insufficient evidence to recommend the routine addition of ICSI in couples with UEI undergoing IVF to increase the live birth rate, although the addition of ICSI in IVF for UEI may reduce the incidence of TFF | B | I |
| CCR | Perform split IVF/ICSI of sibling oocytes to prevent total fertilization failure in first cycle itself as current evidence about universal application of ICSI for unexplained infertility except in cases of previous history of total fertilization failure yields conflicting results | C | - |
| EBR | Use sperm DNA fragmentation testing to customize treatment | C | IV |
| EBR | Do not completely rely on the use of advanced sperm selection techniques for routine assessments; these need larger trials before being incorporated in routine clinical practice | C | III |
| EBR | Consider options of study of embryo morpho–kinetics through time lapse technology and PGT A for selection of good embryo(s) OR for transfer wherever possible | C | IV |
References
Ottardo F, Kliesch S; World Health Organization. [Semen analysis: spermiogram according to WHO 2010 criteria]. Urologe A. 2011 Jan;50(1):101-8.
Zegers-Hochschild F, Adamson DG, Dyer S, et al. The international glossary on infertility and fertility care, 2017. FertilSteril 2017; 108: 393–406.
National Institute for Health and Care Excellence. Fertility: Assessment and Treatment for People with Fertility Problems. NICE Clinical Guideline 156. London and Manchester: NICE; 2013
The Practice Committee of the American Society for Reproductive Medicine: Diagnostic evaluation of the infertile female: a committee opinion. FertilSteril 2012; 98: 302–7.
Simon A, Laufer N. Unexplained infertility: A reappraisal. Ass Reprod Rev 1993
John A. Collins, Elizabeth A. Burrows, Andrew R. Willan. The prognosis for live birth among untreated infertile couples. Fertility and Sterility 1995
Effectiveness and treatment for unexplained infertility. The Practice Committee of the American Society for Reproductive Medicine. 2006
Hughes E, Collins J, Vandekerckhove P. Clomiphene citrate for unexplained subfertility in women. Cochrane Database Syst Rev 2010
Pandian Z, Gibreel A, Bhattacharya S. In vitro fertilisation for unexplained subfertility. Cochrane Database Syst Rev. 2015 Nov 19;(11):CD003357
Bhattacharya S, Hamilton MP, Shaaban M, Khalaf Y, Seddler M, Ghobara T, et al. Conventional in-vitro fertilisation versus intracytoplasmic sperm injection for the treatment of non-male-factor infertility: A randomised controlled trial. Lancet 2001;357:2075-9.
Foong SC, Fleetham JA, O’Keane JA, Scott SG, Tough SC, Greene CA. A prospective randomized trial of conventional in vitrofertilization versus intracytoplasmic sperm injection in unexplained infertility. J Assist Reprod Genet 2006;23:137-40.
Practice Committees of the American Society for Reproductive Medicine and Society for Assisted Reproductive Technology. Intracytoplasmic sperm injection (ICSI) for non-male factor infertility: a committee opinion. FertilSteril. 2012 Dec;98(6):1395-9
Vitek WS, Galárraga O, Klatsky PC, Robins JC, Carson SA, Blazar AS. Management of the first in vitro fertilization cycle for unexplained infertility: A cost-effectiveness analysis of split in vitro fertilization-intracytoplasmic sperm injection. FertilSteril 2013;100:1381- 8.
Brandes M, Hamilton CJ, van der Steen JO, De Bruin JP, Bots RS, Nelen WL, Kremer JA. Unexplained infertility: overall ongoing pregnancy rate and mode of conception. Human Reproduction. 2011 Feb 1;26(2):360-8.
Buckett W, Sierra S, CFAS Clinical Practice Guideline Committee. The Management of Unexplained Infertility: A CFAS Evidenced-based Guideline. Reproductive biomedicine online. 2019 Jul 11
Reindollar RH, Regan MM, Neumann PJ, Levine BS, Thornton KL, Alper MM, et al. A randomized clinical trial to evaluate optimal treatment for unexplained fertility: the fast track and standard treatment (FASTT) trial. Fertil Steril. 2010; 94:888–99. [PubMed: 19531445]
Goldman MB, Thornton KL, Ryley D, Alper MM, Fung JL, Hornstein MD, et al. A randomized clinical trial to determine optimal infertility treatment in older couples: the Forty and Over Treatment Trial (FORT-T). Fertil Steril. 2014; 101:1574–81.
Van Eekelen R, Scholten I, Tjon-Kon-Fat RI, van der Steeg JW, Steures P, Hompes P, van Wely M, van der Veen F, Mol BW, Eijkemans MJ et al. Natural conception: repeated predictions over time. Hum Reprod 2017; 32:346–353.
European IVF-Monitoring Consortium (EIM), European Society of Human Reproduction and Embryology (ESHRE), Kupka MS, D’Hooghe T, Ferraretti AP, de Mouzon J, Erb K, Castilla JA, et al. Assisted reproductive technology in Europe, 2011: results generated from European registers by ESHRE. Human Reproduction 2016; 31(2):233–48.
Tjon-Kon-Fat RI, Wang R, Eijkemans MJ, Bossuyt PM, Mol BW, Van der Veen F, Bhattacharya S, van Wely M. Interventions for unexplained subfertility: a systematic review and network meta-analysis. The Cochrane database of systematic reviews. 2017 Jun;2017(6)
Gunn DD, Bates GW. Evidence-based approach to unexplained infertility: a systematic review. Fertility and sterility. 2016 Jun 1;105(6):1566-74
Nandi A, Bhide P, Hooper R, Gudi A, Shah A, Khan K, Homburg R. Intrauterine insemination with gonadotropin stimulation or in vitro fertilization for the treatment of unexplained subfertility: a randomized controlled trial. Fertility and sterility. 2017 Jun 1;107(6):1329-35.
Collins JA, Burrows EA, Willan AR. The prognosis for live birth among untreated infertile couples. Fertil Steril 1995;64:22-28.
Randolph Jr JF. Unexplained infertility. Clinical obstetrics and gynecology. 2000 Dec 1;43(4):897-901.
Soules MR. Unexplained infertility: the treatment dilemma. Inhuman Reproduction 2000 Jun 1 (Vol. 15, Pp. 85-86). Great Clarendon St, Oxford Ox2 6dp, England: Oxford Univ Press.
Chapter 13: Intrauterine Insemination
OVERVIEW
Intrauterine insemination (IUI) is an office procedure in which prepared semen sample with motile spermatozoa is placed directly into a woman’s uterus to produce pregnancy, with or without ovarian stimulation to produce multiple oocytes. This guideline offers recommendations on the rationale, indications for IUI, required pretreatment workup for female and male factors, contraindications for IUI, details regarding ovarian stimulation in IUI, and luteal phase support during IUI.
1. Introduction
Intrauterine insemination (IUI), with or without ovarian stimulation, is an indispensable part of infertility treatment because it is a noninvasive, cost effective and often successful treatment
2. Rationale
Deposition of a concentrated pellet of motile and mature sperms into the uterine cavity close to the tubal ostia, around the time of ovulation
Increases the density of sperm near the site of fertilization which increases the likelihood of pregnancy
3. Indications
IUI with partner’s sperm can be used as a potentially effective treatment for infertility of all causes in women under about age 40 except in women with tubal blockage, severe tubal damage, very poor egg quality, premature ovarian insufficiency, and severe male factor infertility
IUI with or without ovarian stimulation is considered to be indicated for a broad range of diagnostic conditions
3.1 IUI with husbands semen
Indications for IUI with husbands semen are highlighted in Table 1
Table 1.
IUI with husband semen
| Consider female factors such as |
| • Minimal or mild endometriosis |
| • Sexual dysfunction (vaginismus) |
| • Cervical hostility/factor |
| • Ovulatory dysfunction ? |
| • Unexplained Infertility (in stimulated cycles) (Grade of evidence A) |
| • Anatomic defects of vagina or cervix |
|
|
| Consider male factors such as |
| • Anatomic defect of penis, e.g. hypospadias |
| • Sexual or ejaculatory dysfunction |
| • Erectile dysfunction/impotence |
| • Mild to moderate male factor (Total motile sperm count (TMSC) of 3–10 million) (Grade of evidence A) • Immunological factors |
| • HIV/HBsAg/HCV discordant couples |
| • Cryopreservation of sperm in cases of cancer treatment |
|
|
|
Others • Unexplained infertility |
3.2 IUI with donor semen
Azoospermia
Genetic conditions (e.g. haemophilia, Huntington’s chorea)
Severe male factor (cannot afford assisted reproduction(ART)
Severe Rh incompatibility
4. Factors that will guide the choice of IUI as treatment modality
Semen Parameters (TMC >5 million/ml)
-
Other Factors which affect the chance to pregnancy
-
»
Presence or absence of cervical factor
-
»
Endometriosis
-
»
Tubal pathology
-
»
Uterine pathology – Congenital anomalies, polyp, sub-mucous myoma, IUA
-
»
Pelvic factor – History of previous pelvic or abdominal surgeries
-
»
Age of the women – above 37 years one should consider IVF early in the treatment protocol
-
»
Special situations
5. Contraindications
IUI is contraindicated in women with:
Cervical atresia
Acute cervicitis/vaginitis
Pelvic inflammatory disease
Severe endometriosis
Bilateral tubal obstruction
IUI is contraindicated in men with:
Severe male factor infertility
Heritable genetic disorders
6. Pre–treatment workup
Accurate detection of underlying reproductive abnormalities helps to guide individual management decisions and maximize treatment outcomes
6.1 Workup for female partner (Figure 1)

6.1.1 Baseline transvaginal sonography
For evaluation of the uterus, uterine cavity, endometrium, and adnexa
Measurement of antral follicle count (AFC) for ovarian reserve
Doppler in presence of any uterine and adnexal pathology
6.1.2 Hysterosalpingography (HSG)
Has low sensitivity but its high specificity thus, makes it a useful screening test for ruling out tubal obstruction
6.1.3 Laparoscopy
It is not cost effective to do diagnostic laparoscopy as part of the initial infertility evaluation when history, physical examination, TVS, HSG, and mid–luteal progesterone are all normal and should be done only if patient fails to conceive after 6 ovulatory cycles (Grade B). Laparoscopy has positive predictive value of 98.4 %
-
Laparoscopy is considered early if
-
»
Age >35 yrs
-
»
Married > 3 yrs
-
»
Presence of an abnormal HSG
-
»
History or symptoms suggestive of pelvic disease
-
»
Presence of dyspareunia and dysmenorrhea
-
»
History of previous pelvic surgery
-
»
6.1.4 Ultrasound for assessment of tubal factor
Assessment of tubal factor by USG can be done either by saline infusion sonosalpingography (SIS) or hysterosalpingo–contrast sonography (HyCoSy). Both have a good sensitivity and specificity but HyCOSy is more efficient than SSG in detecting tubal obstruction (Grade A) and has a better predictive value as compared to SIS. Results of SIS correlated positively with laparoscopy in 97% and with HSG in 94%
6.1.5 Hysteroscopy
-
Hysteroscopy is indicates as initial workup of infertility before IUI only in presence of
-
»
Abnormal HSG/USG
-
»
Unexplained infertility to detect any subtle endometrial abnormalities?
-
»
history or symptoms suggestive of endometrial or uterine pathology
-
»
6.1.6 Endocrine parameters
-
Offer analysis of endocrine parameters such as:
-
»
Thyroid stimulating hormone (TSH)
-
»
Antithyroid antibody
-
»
Prolactin
-
»
Anti–mullerian hormone (AMH) if AFC<5
-
»
Follicle stimulating hormone/luteinizing hormone (FSH/LH) on day 2–3 of menstrual cycle if indicated
-
»
Androgen profile – DHEAS, ASD, testosterone (total and free) and 17–OH progesterone in presence of signs of hyperandrogenemia, and PCOM at USG
-
»
6.1.7 Assessment of pelvic TB required when
Previous history of extragenital tuberculosis
Persistent thin endometrium despite good follicular cycles and E2 levels
USG suggestive of IU adhesions
HSG suggestive of IU adhesions or tubal pathology
Hysteroscopy suggestive of endometritis
6.1.8 Others
-
Offer workup for:
-
»
Hemoglobin
-
»
Blood sugar
-
»
OGTT if PCOS
-
»
Lipid profile if PCOS
-
»
Rubella screening
-
»
Thalassemia screening
-
»
Pap smear
-
»
Viral markers
-
»
Serum chlamydial antibodies
-
»
6.2 Workup for the male partner
6.2.1 Semen analysis
-
Consider the following for semen analysis:
-
»
Total motile sperm count (prewash): >5–10 million
-
»
Inseminating motile count (IMC) >1 million
-
»
Sperm morphology using strict criteria >4%
-
»
Total motility >30%
-
»
6.2.2 Viral markers
Couples and individuals undergoing IUI and males providing semen samples for IUI should be screened for infectious agents based on local, regional, and national standards and regulations. (Grade of evidence D)
7. Counselling
Consider counselling of the couples before the procedure begins regarding the indication of IUI, timing and number of visits required, cost involved, chances of success, what is sperm preparation, technique of insemination and complications
Offer reassurance to the couple about confidentiality and consent form by ICMR should be signed by both the partners
8. Ovarian stimulation in IUI
-
Consider using the following stimulating agents in IUI cycle
Oral ovulation induction agents: Clomiphene citrate/letrozole
Gonadotropins
Clomiphene citrate/letrozole+ gonadotropins
Gonadotropin releasing hormone (GnRH) agonists and antagonists with gonadotropins
8.1 Oral ovulation induction agents
8.1.1 Clomiphene citrate (CC)
Clomiphene is a selective estrogen receptor modulator (SERM) that binds to the estrogen receptors at multiple sites throughout the reproductive tract, and can act as an estrogen agonist or as an antagonist
Clomiphene binds to estrogen receptors in the hypothalamus, inhibiting negative feedback of estrogen on gonadotropin release
Subsequent up–regulation of the hypothalamic–pituitary–gonadal axis leads to growth of the ovarian follicle(s)
Consider the dose of 50–100 mg per day for five days up to a maximum of 150 mg per day, which can begin from day 2–5 of a normal period or a withdrawal bleed
8.1.2 Aromatase inhibitors
Aromatase inhibitors suppress estrogen production but do not have the anti–estrogenic effect of clomiphene citrate in the late follicular phase and they may have fewer side effects than clomiphene
Letrozole is the most commonly used aromatase inhibitor for ovulation induction
Consider the dose of 2.5 mg/day orally from day 2–3 of the cycle for 5 days
No significant difference in pregnancy rates between anti–estrogens with aromatase inhibitors, in non–PCOS women undergoing IUI
8.1.3 Gonadotropins
They stimulate follicular growth by acting directly on ovarian FSH receptors and have no anti–estrogenic effect on cervical mucus or endometrium such as clomiphene
Consider low dose regimens with 75 IU or lower because higher doses have similar pregnancy rates but increase the multiple pregnancy rates and risk of ovarian hyperstimulation (OHSS)
COS using gonadotrophins might be the most effective drug for IUI cycles
8.1.4 Clomiphene citrate/letrozole plus gonadotropins
Combination protocols reduce the cost of treatment and equally effective, with potentially fewer multiple births than with gonadotropins alone
Consider a sequential use of clomiphene citrate or Letrozole with gonadotropin. CC 50–100 mg/letrozole 2.5 mg from day 3 to day 7 followed by gonadotropins daily from day 8 till the size of the dominant follicle became 18 mm
8.1.5 Gonadotropin releasing hormone (GnRH) agonists and antagonists
Premature LH surges also occur in 25%–30% of stimulated IUI cycles
Antagonist or agonist use in IUI cycles did not show any significant increase in pregnancy rates and are not cost effective to use in all IUI cycles
8.2 Ideal ovarian stimulation for IUI
Clomiphene citrate/letrozole is considered to be the most cost effective, especially considering the cost of monitoring, and risk of ovarian hyperstimulation syndrome
| No. of follicles recruited | 2 – 4 follicles 18–20 mm |
| Endometrial thickness | ≥9 mm thick and trilaminar |
| Day of IUI | IUI between cycle Day 13–16 |
9. Consensus on OI in IUI (Figure 2)
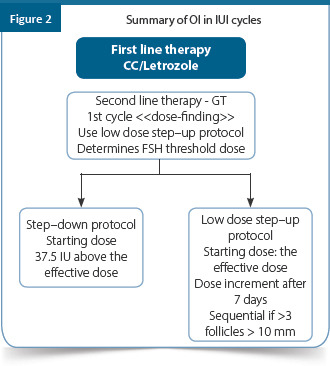
Anti–estrogens appear to be cost effective in IUI programs, although less effective compared to GT. (Grade of evidence B)
Both letrozole and CC have similar results
When GT used – given on daily basis
Low dose protocols do not differ significantly in success, when compared to high dose, which, increase risk of multiples and OHSS
In couples with unexplained infertility and men with a TMSC above 10 million, IUI should be combined with OS to improve live birth rates. (Grade of evidence B)
When gonadotrophins are used in IUI, regiments with 75 IU or lower should be used because higher doses have similar pregnancy rates but increase multiple pregnancy rates. (Grade of evidence A)
No difference in the probability of conception whether one uses urinary or Rec GT
Addition of GnRH agonist to gonadotrophins in IUI–OS is not recommended because there is no increase in pregnancy rate despite increased multiple pregnancy rates, OHSS and increased costs. (Grade of evidence B)
Role of GnRH–antagonists in mild COS/IUI programs needs to be determined (GPP)
10. Monitoring in IUI cycle
Different methods like luteinizing hormone (LH kits, serum estradiol levels, and ultrasonography (USG) to time IUI has been used
Ultrasonography and LH kits are the most economical form of monitoring
If ultrasonography is used for monitoring size of follicle, endometrial thickness should also be recorded
Normal Follicular growth correlates with E2 measurements and a mature follicle secrets 250 – 300 pg/ml of E2. Follicular size more accurate than E2 in predicting ovulation
10.1 Monitoring in natural cycle (Figure 3)
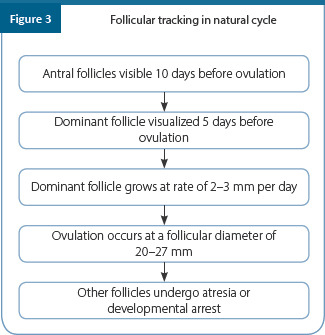
Natural cycles with IUI require least amount of monitoring. LH predictor kits are used to determine LH surge and ovulation and the IUI is timed accordingly
Alternatively, transvaginal ultrasound can be used between cycle days 10 –14 to determine development of mature follicle with administration of HCG for trigger at follicular diameter of 18–20 mm followed by IUI between 24 – 42 hours
10.2 Monitoring in stimulated cycle (Figure 4)
Figure 4A.
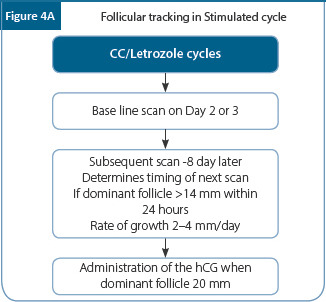
Figure 4B.
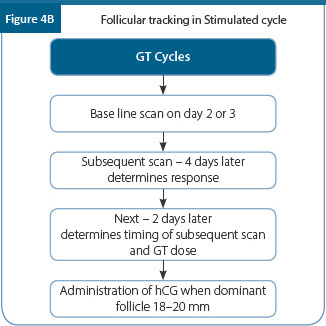
Perform an ultrasound on cycle days 2/3 in order to confirm that no ovarian cysts are present prior to starting the ovarian stimulating agents
Perform serial ultrasound scans from day 8 (gonadotropin stimulating cycle) or day 10 (oral ovulation induction drug cycle) till the day of trigger
11. When to cancel IUI cycle or convert to IVF
-
Consider cancelling the IUI cycle or converting to IVF in the following situations:
-
»
In order to prevent high rates of multiple gestation pregnancies in IUI–OS, IUI should be withheld when more than three dominant follicles >15 mm on the day of HCG injection or LH surge are present. (Grade of evidence B)
-
»
Estradiol ≥1500 pg/ml
-
»
12. Trigger and timing of IUI
Providers can determine the method of triggering in IUI stimulated with gonadotrophins as there is no evidence to recommend for or against a method while comparing hCG and natural LH surge (Grade of evidence B)
-
Human chorionic gonadotropin (hCG) 5000–10,000/recombinant human chorionic gonadotropin (rec–hCG) –250 mcg SC is used as trigger in stimulated cycle. No evidence to repeat the trigger in case of non–rupture of follicle.
-
»
Trigger should be given when dominant follicle (DF) is 20–22 mm in a clomiphene citrate/letrozole cycles and 18 mm for gonadotropin cycle
-
»
IUI should be performed 24 to 40 hours after administration of hCG trigger. (Grade of evidence B)
Perform IUI 1 day after detection of spontaneous LH surge in natural cycle or after confirmation of ovulation. (Grade of evidence B)
13. Efficacy of IUI varies widely because of different variables related to:
Use of technique
Environment in laboratory
Equipment’s
IUI catheters
Consumables
13.1 Semen collection
Semen collection should be done according to standard recommended procedure
13.2 Semen preparation techniques that are routinely used worldwide are as follows
A simple dilution and washing technique
Swim–up technique
Density gradient centrifugation
13.3 Choice of technique will depend on
Count
Motility
Morphology and TZI index
Source of sample
-
Debris & other cellular contamination
-
»
Sperm concentration >15 million/ml with good forward progressive motility, swim–up performed
-
»
Borderline samples, and samples with large amount of debris, extreme oilgozoospermia, severely compromised motility best prepared by gradient separation
-
»
Samples collected by electroejaculation – low motile sperm concentration best suited for gradient separation
-
»
According to the available evidence, it is not possible to recommend any semen preparation technique over another for a normal semen samples (swim–up, gradient, wash and centrifugation). (Grade of evidence C)
13.4 Environment in laboratory
Sperm preparation requires a clean room with air conditioning with no free access to toxic fumes and has sufficient space to accommodate necessary equipment’s
Equipment’s and consumables of highest quality and reliability should be used
Maintenance of equipment’s and optimal working environment in the lab is required for good IUI results. Special care should be taken to maintain the temperature at 37°C
-
Damage to the sperm from following factors must be minimized
-
»
Dilution – performed slowly
-
»
Temperature change – should be gradual
-
»
Centrifugation – Centrifugal forces should be low
-
»
Limit oxidative damage caused by free oxygen radicals released from leucocytes or abnormal sperms
-
»
Exposure to potentially toxic material
-
»
14. IUI procedure
Special dedicated room for the IUI procedure – with sterilized instruments which would give adequate exposure of cervix for insemination is needed. The factors that affect the IUI success rate are seen the table below
Table 2.
The factors that affect the IUI success rate
| Type of catheter (soft/firm) | • Open ended/rounded tip teflon catheters least traumatic and most efficient • No significant difference in PR with type of catheter • Gentle, atraumatic technique with no touch to fundus is the essence of successful IUI |
| Volume of insemination | 0.3–0.5 ml |
| Insemination | Immediately after the sample is ready and loaded in the syringe |
| Ultrasound guided | • No difference in cumulative pregnancy rates • Ultrasound guided helpful in cases of difficult IUIs |
| Single or double insemination | • Single well timed IUI recommended. (Grade of evidence B) • Double IUI in cases of male factor infertility may be performed but insufficient evidence. (Grade of evidence B) |
| Bed rest after IUI | • A 10–15 minutes bed rest after IUI has a positive effect on CPR. (Grade of evidence B) |
| Number of treatment IUI cycle | • Perform at least three consecutive IUI cycles in couples with an indication for IUI. (Grade of evidence B) • There is insufficient evidence to recommend a maximum number of IUI treatment cycles. (Grade of Evidence B) • Maximum PRs are seen in the first 4 IUI cycles |
15. Luteal phase support after IUI
Required definitely with use of gonadotrophins and GnRH analogs - Agonist and Antagonist (Figure 5)
Insufficient evidence to recommend use of LPS in natural or clomiphene/letrozole stimulated IUI cycle
Start from next day of IUI or after ovulation is confirmed on ultrasound
Offer for 2 weeks, if pregnant; continue till 8–10 weeks of gestation
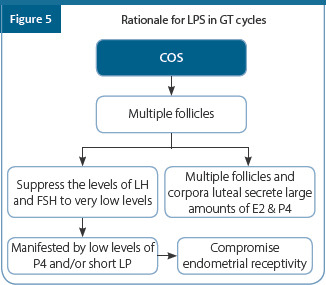
16. IUI outcome
The IUI outcome can be linked to female factor and semen parameter’s
16. 1 Female factor
Age of women
Ovarian reserve – Poor outcome with decreased ovarian reserve
Duration of infertility – Pregnancy rates decrease if duration. More than 4 years
Cause of infertility – best results in unexplained and mild male factor infertility and least with endometriosis
16.2 Semen parameters
It is not possible to define clear lower cut-off levels of pre–or post–wash sperm parameters below which IUI should be withheld. (Grade of evidence B–C)
High motile count before preparation (>15 million/ml)
-
High Inseminating Motile Count (IMC) ≥5 million/ml
-
»
CPR per couple TMS count
-
»
28.5% < 5 million
-
»
44.3% > 5 million
-
»
24 hour survival of processed sperm - > or = 70%
Better Sperm morphology (>4%) in unprocessed and processed sample
CPR per couple decreased from 40.7% to 21.4%, percentage of teratospermia was higher
TZI <1.85
HOS >60 %
DFI <15 %
Summary of recommendations
IUI is a simple and non–invasive technique it can be performed without expensive infrastructure with a reasonable success rate within three or four cycles
IUI is safe and easy treatment with minimal risks and monitoring with good couple compliancy (low drop–out rate) and a very low risk for complications such as OHSS
IUI is most cost–effective strategy especially in couples with mild male factor and unexplained infertility
In couples with unexplained infertility with a prognosis of becoming pregnant without assistance within the next 12 months (estimate >30%)
IUI could be postponed for at least 6 months (Grade of evidence A)
In couples with unexplained infertility and men with a total motile sperm count (TMSC) >10 million and a prognosis of spontaneous pregnancy <30% within a year, it is recommended that IUI plus ovarian stimulation (OS) is the treatment of first choice. (Grade of evidence A)
In couples with solely a poor sperm quality in the male partner, it is not recommended either for or against use of IUI. (Grade of evidence A)
In couples with unexplained infertility and men with a TMSC above 10 million, IUI should be combined with OS to improve live birth rates. (Grade of evidence B)
It is not possible to define clear lower cut–off levels of pre–or post–wash sperm parameters below, which IUI should be withheld. (Grade of evidence B–C)
Providers can determine the method of triggering in IUI stimulated with gonadotrophins as there is no evidence to recommend for or against a method. (Grade of evidence B)
Providers can determine the method of timing IUI in natural cycles (no OS) as there is no evidence to recommend for or against a method. (Grade of evidence B )
If a HCG injection is used, single IUI can be performed any time between 24 and 40 hours after HCG injection without compromising pregnancy rates. (Grade of evidence B )
IUI in a natural (not ovarian stimulated) cycle should be performed 1 day after LH rise. (Grade of evidence B )
The intervention FSP, when compared to IUI, should not be the treatment of choice. (Grade of evidence A)
In both unexplained and male infertility there is insufficient evidence that the intervention, a double IUI, within the same cycle will lead to better pregnancy rates than a single IUI within a cycle. (Grade of evidence B)
Women undergoing IUI should be offered a single insemination per cycle. (Grade of evidence B)
Women undergoing IUI, should have 10 to 15 minutes of bed rest after an insemination. (Grade of evidence B)
In couples with an indication for IUI at least three consecutive IUI cycles should be performed. (Grade of evidence B)
There is insufficient evidence to recommend a maximum number of IUI treatment cycles. (Grade of evidence B)
According to the available evidence, it is not possible to recommend any semen preparation technique over another (swim–up, gradient, wash and centrifugation). (Grade of evidence C )
In couples with unexplained infertility and men with a TMSC of >10 million and a prognosis of a pregnancy without assistance <30% within a year, at least three cycles of IUI–OS is the most effective option. (Grade of evidence A)
Good practice point: Couples and individuals undergoing IUI and males providing semen samples for IUI should be screened for infectious agents based on local, regional and national standards, and regulations. (Grade of evidence D)
In order to prevent high rates of multiple gestation pregnancies in IUI–OS, IUI should be withheld when more than two dominant follicles >15 mm or more than five follicles >10 mm at the time of HCG injection or LH surge are present. (Grade of evidence B)
When gonadotrophins are used in IUI, regiments with 75 IU or lower should be used because higher doses have similar pregnancy rates but increase multiple pregnancy rates. (Grade of evidence A )
Clomiphene citrate or tamoxifen are acceptable alternatives to low dose gonadotrophins for low multiple pregnancy and birth rates and with lesser costs, although at a lower live birth rate than with gonadotrophins. (Grade of evidence B)
Addition of GnRH agonist to gonadotrophins in IUI–OS is not recommended because there is no increase in pregnancy rate despite increased multiple pregnancy rates and increased costs. (Grade of evidence B)
Good practice point: As an alternative to cycle cancelation, aspiration of excess follicles at the time of HCG injection or LH surge might be additional options for reducing the risk of multiple pregnancy in IUI– OS. (Grade of evidence C)
Individuals with infertility undergoing treatment with IUI–OS should be informed about a possible increased risk for preterm birth and low birth weight in singletons and twin pregnancies when compared to pregnancies in fertile couples not requiring assistance. (IVF/ICSI outcome comparisons are assessed in the IVF/ICSI prioritized guideline.) (Grade of evidence D )
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CPP | IUI is a simple and non-invasive technique it can be performed without expensive infrastructure with a reasonable success rate within three or four cycles | - | |
| CPP | IUI is safe and easy treatment with minimal risks and monitoring with good couple compliancy (low drop–out rate) and a very low risk for complications such as OHSS | - | |
| CPP | IUI is most cost–effective strategy especially in couples with mild male factor and unexplained infertility | - | |
| EBR | In couples with unexplained infertility with a prognosis of becoming pregnant without assistance within the next 12 months (estimate >30%), IUI could be postponed for at least 6 months | A | I |
| EBR | In couples with unexplained infertility and men with a total motile sperm count (TMSC) >10 million with prognosis of spontaneous pregnancy <30% within a year, it is recommended that IUI plus ovarian stimulation (OS) is the treatment of first choice | A | I |
| EBR | In couples with solely a poor sperm quality in the male partner, it is not recommended either for or against use of IUI. | A | I |
| EBR | In couples with unexplained infertility and men with a TMSC above 10 million, IUI should be combined with OS to improve live birth rates | B | II |
| EBR | It is not possible to define clear lower cut–off levels of pre–or post– wash sperm parameters below which IUI should be withheld | B | III |
| EBR | Providers can determine the method of triggering in IUI stimulated with gonadotrophins as there is no evidence to recommend for or against a method | B | II |
| EBR | Providers can determine the method of timing IUI in natural cycles (no OS) as there is no evidence to recommend for or against a method | B | II |
| EBR | If a HCG injection is used, single IUI can be performed any time between 24 and 40 hours after HCG injection without compromising pregnancy rates | B | II |
| EBR | IUI in a natural (not ovarian stimulated) cycle should be performed 1 day after LH rise | B | II |
| EBR | The intervention FSP, when compared to IUI, should not be the treatment of choice | A | II |
| EBR | In both unexplained and male infertility there is insufficient evidence that the intervention, a double IUI, within the same cycle will lead to better pregnancy rates than a single IUI within a cycle | B | II |
| EBR | Women undergoing IUI should be offered a single insemination per cycle | B | II |
| EBR | Women undergoing IUI, should have 10 to 15 minutes of bed rest after an insemination | B | III |
| EBR | In couples with an indication for IUI at least three consecutive IUI cycles should be performed | B | II |
| EBR | There is insufficient evidence to recommend a maximum number of IUI treatment cycles | B | III |
| EBR | According to the available evidence, it is not possible to recommend any semen preparation technique over another (swim–up, gradient, wash and centrifugation) | C | III |
| EBR | In couples with unexplained infertility and men with a TMSC of >10 million and a prognosis of a pregnancy without assistance <30% within a year, at least three cycles of IUI–OS is the most effective option | A | II |
| EBR | Good practice point: Couples and individuals undergoing IUI and males providing semen samples for IUI should be screened for infectious agents based on local, regional and national standards and regulations. | D | IV |
| EBR | In order to prevent high rates of multiple gestation pregnancies in IUI–OS, IUI should be withheld when more than two dominant follicles >15 mm or more than five follicles >10 mm at the time of HCG injection or LH surge are present. | B | II |
| EBR | When gonadotrophins are used in IUI, regiments with 75 IU or lower should be used because higher doses have similar pregnancy rates but increase multiple pregnancy rates. | A | I |
| EBR | Clomiphene citrate or tamoxifen are acceptable alternatives to low dose gonadotrophins for low multiple pregnancy, and birth rates and with lesser costs, although at a lower live birth rate than with gonadotrophins | B | II |
| EBR | Addition of GnRH agonist to gonadotrophins in IUI–OS is not recommended because there is no increase in pregnancy rate despite increased multiple pregnancy rates and increased costs | B | II |
| CCR | Good practice point: As an alternative to cycle cancelation, aspiration of excess follicles at the time of HCG injection or LH surge might be additional options for reducing the risk of multiple pregnancy in IUI– OS | C | - |
| EBR | Individuals with infertility undergoing treatment with IUI–OS should be informed about a possible increased risk for preterm birth and low birthweight in singletons and twin pregnancies when compared to pregnancies in fertile couples not requiring assistance. (IVF/ICSI outcome comparisons are assessed in the IVF/ICSI prioritized guideline) | D | V |
References
ESHRE Capri Workshop Group. Intrauterine insemination. Hum Reprod Update. 2009; 15(3):265–77.
Omblelet W, Nathalie D, et al. Seman quality and prediction of IUI success in male subinfertility: A systematic review. Reprod Biomed Online. 2014; 28:300–9.
Cohlen B, Bijkerk A, Van der Poel S, Ombelet W. IUI: review and systematic assessment of the evidence that supports global recommendations. Human reproduction update. 2018 May 1;24(3):300-19.
Cantineau AEP, Cohlen BJ, Heineman MJ. Ovarian stimulation protocols (anti-oestrogens, gonadotrophins with and without GnRH agonists/antagonists) for intrauterine insemination (IUI) in women with subfertility. Cochrane Database Syst Rev2007; CD005356. doi: 10.1002/14651858.CD005356.pub2.
Jee, B.C., Ku, S.Y., Suh, C.S., Kim, K.C., Lee, W.D., and Kim, S.H. Use of letrozole versus clomiphene citrate combined with gonadotropins in intrauterine insemination cycles: a pilot study. Fertil Steril. 2006; 85: 1774–1777.
Merviel P, Heraud MH, Grenier N, Lourdel E, Sanguinet P, Copin H. Predictive factors for pregnancy after intrauterine insemination (IUI): an analysis of 1038 cycles and a review of the literature. Fertil Steril 2010; 93: 79–88.
Cantineau AEP, Janssen MJ, Cohlen BJ, et al. Synchronised approach for intrauterine insemination in subfertile couples. Cochrane Database Syst Rev 2014
Yavas Y, Selub MR. Intrauterine insemination (IUI) pregnancy outcome is enhanced by shorter intervals from semen collection to sperm wash, from sperm wash to IUI time, and from semen collection to IUI time. Fertil Steril. 2004; 82(6):1638–47
Boomsma CM, Heineman MJ, Cohlen BJ, et al. Semen preparation techniques for intrauterine insemination. Cochrane Database Syst Rev 2007; CD004507.doi: 10.1002/14651858.CD004507.pub3.
Potat I, Ekiz A, Yildirim G, et al. Ultrasound-guided intrauterine insemination versus blind intrauterine insemination: A randomized controlled trial. Clin Exp Obstet Gynecol. 2015; 42(5):657–62.
Cantineau AEP, Heineman MJ, Cohlen BJ. Single versus double intrauterine insemination (IUI) in stimulated cycles for subfertile couples. Cochrane Database Syst Rev 2003; CD003854. doi: 10.1002/14651858.CD003854.
Hill MJ, Whitcomb BW, Lewis TD, Wu M, Terry N et al. Progesterone luteal support after ovulation induction and intrauterine insemination: A systematic review and meta-analysis. Fertil Steril. 2013; 100(5):1373–80.
Chapter 14: IVF/ICSI
OVERVIEW
This guideline offers recommendations on assisted reproduction technologies (ART) such as in-vitro fertilization (IVF) and intracytoplasmic sperm Injection (ICSI) in couples with infertility problems. This guideline will act as a blueprint to the standard of care in ART and also overcome the technical challenges inappropriate management of infertility. The recommendations are aimed primarily at women aged 21 years or older presenting to healthcare professionals with infertility problems. This guideline may help fill the gap and help in the proper maintenance of ART procedures in India.
1. Introduction
Infertility is the inability to conceive after having regular unprotected intercourse at least for >1 year
The exact burden of infertility in India is unknown. However, a multinational study by the World Health Organization (WHO) including India showed that the incidence of infertility was found to be 10%–15%
Different types of infertility infections such as reproductive tract infections (RTI) and genital
2. Definitions
2.1 Assisted reproductive technology (ART)
ART envelops all the techniques involved in obtaining a pregnancy by manipulating the sperm and oocyte outside the body and transferring the gamete or embryo into the uterus for fertilization
IVF-ET (In vitro fertilization–embryo transfer)
IVF-ET is the fertilization of an oocyte in vitro and the transfer of the fertilized oocyte or embryo to the uterus of a woman
2.2 ICSI (Intracytoplasmic Sperm Injection)
In ICSI, a single sperm (ejaculated or extracted (PESA and TESA)) is injected directly into the cytoplasm of the oocyte to aid in fertilization
3. Factors that will guide the choice of treatment between IVF and ICSI will depend on
Semen Parameters – sperm count, motility, morphology, DFI
-
Other Factors which affect the chance to pregnancy
-
»
Presence or absence of cervical factor
-
»
Endometriosis
-
»
Tubal pathology
-
»
Uterine pathology – Congenital anomalies, polyp, sub–mucous myoma, IUA
-
»
Anti–sperm antibody in male and female partner
-
»
Pelvic factor – History of previous pelvic or abdominal surgeries
-
»
Age of the women – above 40 years should consider IVF early in the treatment protocol
-
»
Special situations
4. Indications
4.1 IVF –ET
Irreversible pathology of the fallopian tubes/blocked tubes
Ovulatory dysfunction who have failed to conceive with conventional methods
Subnormal malefactor
Unexplained infertility
Endometriosis.
Infertility of immunological origin
Fertility preservation
Candidates for preimplantation genetic diagnosis
4.2 ICSI with ejaculated spermatozoa
Oligoasthenoteratozoospermia
Fertilization failure after standard IVF treatment
The newer indications for ICSI include – poor-quality oocytes, low oocyte yield, PGT, IVM, fertilization of cryopreserved oocytes
Poor post-thaw parameters after sperm freezing
Increased DFI
Anejaculation because of spinal cord injury
Retrograde ejaculation
4.3 Indications for ICSI with testicular sperm (TESA)
Germ–cell hypoplasia (hypo spermatogenesis)
Germ–cell aplasia with focal spermatogenesis
4.4 Use of IVF as a first-line versus last resort in certain conditions is debatable and include
Unexplained infertility
Mild male factor infertility
Endometriosis without tubal disease
Unilateral tubal blockage
Diminished ovarian reserve
Age >40 years with good ovarian reserve
4.5 Contraindications to ART procedures
Any medical condition where pregnancy is contraindicated
5. Procedure
Recommended procedure for IVF, and ICSI
IVF
Oocytes are aspirated from mature Graafian follicle after controlled ovarian stimulation to produce multiple follicular developments. Oocytes must be aspirated and maintained in an environment that maintains the temperature at 370 C
5.1 Prerequisites
Female partner – age >21 –<45 years, 23–50 years in male
Investigations needed for administration of anesthesia must be done
Baseline scan
Counselling and consent for complete treatment plan, complications and adverse outcomes. The model consent forms are to be adapted from the ICMR guidelines
Fitness for general anesthesia and pregnancy
Back up semen sample is advisable
5.2 COS
The treatment protocol for COS can be individualized according to need of the couple. One need to decide on the dose and type of gonadotropin used and the GnRH analogue used to prevent LH surge
5.3 Procedure for lab preparation
All culture media, oil, hyaluronidase, PVP, vitrification and thaw solutions are to be maintained at 4°C and discarded upon expiry
All the consents in the checklist has to be verified before the patient is taken to OT for the procedure
All culture media should be appropriately equilibrated for temperature, pH and osmolarity
5.4 Oocyte retrieval procedure
-
Transvaginal follicle puncture under USG control
-
»
Method of choice worldwide
-
»
less invasive
-
»
Less complications
-
»
Time of retrieval–hCG or GnRH agonist is can be administered at any time 34 to 36 hours before OR without affecting the results of IVF
Patient ID checked
-
Oocyte pick has to be done under conducive conditions using standard procedures
-
»
Analgesia/anaesthesia
-
»
Cleaning of vagina
-
»
Use of TVS with a needle guide
-
»
Aspiration of all visible follicles from both ovaries with a suction pump delivering 100–120 mmHg pressure
-
»
Differentiating between follicle and internal iliac vessels important during OR and when in doubt turn the probe the vessel will become elongated, where as the follicle will remain round, and If still in doubt add color which will identify the internal iliac vessel
-
»
Follicular fluid containing oocytes is collected into sterile tubes maintained at 37°C and then rapidly transported to the laboratory
-
»
Confirming haemostasis at vaginal puncture sites
-
»
Follicular flushing results in no significant difference in the number of oocytes retrieved, fertilization rate, PR. It significant increases the operating and aspiration time
In the laboratory, oocytes are screened picked up, and incubated at 37°C for insemination
-
Complications of oocyte retrieval are rare but may occur
-
»
Severe intra–abdominal bleeding seems to occur in <1 in 1000 procedure
-
»
Infectious complications such as pelvic infections or pelvic abscesses, second most common complications with 2–6 cases per 1000 ORs
-
»
Injury of pelvic structures, such as the ureter, the bowel or the appendix, happens in 1 in 1000 procedures
-
»
3% of patients experience severe to very severe pain and 2% of patients still suffer from severe pain 2 days after the procedure
-
»
The pain level increases with the number of oocytes retrieved
-
»
5.5 Procedure for insemination
The procedure for insemination depends on the technique selected. In IVF, sperm and eggs are mixed and incubated together. Whereas, for ICSI, spermatozoa are injected into the cytoplasm of the oocyte
5.5.1 IVF
Sperm count and motility should be normal
Prepare semen as described and dilute to final concentration 1x106 per ml
Place in the incubator before use for capacitation and initiation of acrosome reaction
Insemination after 4–6 hours of OR
Inseminate with 10000 sperms per oocyte either in central well dish or micro droplets
5.5.2 ICSI
Done in patients with severe OAT, failed fertilization, high DFI; surgically retrieved sperm
Oocyte denudation is performed via enzymatic action of hyaluronidase, and mechanical pipetting
Injection of the sperm in the denuded oocyte should be done within 40 hours of ovulation induction trigger
Sperm immobilized, aspirated in injection needle, and then injected into the oocyte with polar body at either 6 or 12 O’ clock position
Injected oocytes washed and cultured in microdroplets
5.6 Fertilization check
Fertilization check occurs between 16–18 hours post insemination – Check for 2 PN or syngamy
5.7 Embryo evaluation and transfer
-
Embryos are analyzed for the rate of development, level of fragmentation, and quality using a quality score till embryo transfer
-
»
On the day of transfer, select embryo on the basis of embryo score for transfer, and the remaining good quality embryos are cryopreserved
-
»
The Table below shows the timeline of embryo development
-
»
Table.
Embryo check
| 2PN | 16–18 hours |
| 2 Cell | 25–27 hours |
| 4 Cell | 42–46 hours |
| 8 Cell | 66–72 hours |
| Morula | 90–100 hours |
| Blastocyst | 114–120 hours |
| Hatching Blastocyst | 1–140 ur |
5.8 Embryo transfer procedure
Patient ID checked
Number of embryos to be transferred decided – not more than 2 if women <35 years and not more than if women >35 years
Embryo transfer should be done under ultrasound guidance
Embryo transfer can be done at cleavage cell stage (4 or 8 cells) or blastocyst stage
6. Documentation
All IVF/ICSI procedures should also be documented in the EMR. These should clearly state the patients’ details; the number of oocytes collected and used, quality assessment of oocytes and embryos formed, number of embryos transferred, and cryopreserved and the transfer details.
7. Maternal risks
Maternal risks involved in ART are ovarian hyperstimulation syndrome (OHSS), increased risk of multiple pregnancy if more number of embryos are transferred, ectopic pregnancy, pre–eclampsia, placenta previa, placental abruption, gestational diabetes, and cesarean delivery
Summary of recommendations
Time of oocyte retrieval should be 34 to 36 hours after ovulation trigger without affecting the results of IVF
Transvaginal follicle puncture under USG control is the method of choice worldwide
Oocyte retrieval performed under intravenous sedation or under GA using intravenous fentanyl and propofol as well as assisted mask ventilation with oxygen
Aspiration pressure level should be maintained between 100–120 mm of Hg
Differentiating between follicle and internal iliac vessels important during OR
No benefit in total oocytes retrieved or oocyte yield with follicle flushing but associated with a significant increase in the procedure time for oocyte retrieval
Follicular fluid containing oocytes is collected into sterile tubes maintained at 37°C and then rapidly transported to the laboratory where it is screened for presence of cumulus oocyte complexes
At the end of the procedure, the vagina was thoroughly examined with a speculum and if necessary local compression was applied to allow haemostasis
Factors that will guide the choice of treatment between IVF and ICSI depend on semen parameters, other Factors which affect the chance to pregnancy, and special situations
OCCs are then transferred to media with bicarbonate and incubated/cultured for at least 4 hours
In IVF Insemination after 4-6 hours of OR and then inseminated with 10000 sperms per oocyte either in central well dish or micro droplets. Denude after 16–18 hours and check for fertilization
ICSI should be done after 40 hours after oocyte trigger. Injected oocytes washed and cultured in microdroplets and checked for fertilization after 16-18 hours
Embryos are analyzed for the rate of development, level of fragmentation, and quality using a quality score till embryo transfer
Embryo transfer can be done at cleavage or blastocyst stage and the remaining embryos cryopreserved.
Number of embryos depends on the age, cause of subfertility stage of transfer, quality of embryos, and policy
Use of USG guided soft catheter embryo transfer technique improve results and lower the variability of the results by making it less traumatic, standardized, and technically precise
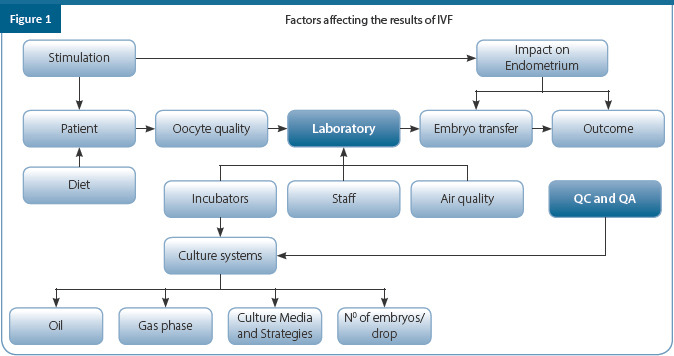
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| EBR | Time of oocyte retrieval should be 34 to 36 hours after ovulation trigger without affecting the results of IVF | A | II |
| EBR | Transvaginal follicle puncture under USG control is the method of choice worldwide | A | I |
| EBR | Oocyte retrieval performed under intravenous sedation or under GA using intravenous fentanyl and propofol as well as assisted mask ventilation with oxygen | B | III |
| EBR | Aspiration pressure level should be maintained between 100–120 mm of Hg | B | II |
| EBR | Differentiating between follicle and internal iliac vessels important during OR | A | I |
| EBR | No benefit in total oocytes retrieved or oocyte yield with follicle flushing but associated with a significant increase in the procedure time for oocyte retrieval | A | II |
| EBR | Follicular fluid containing oocytes is collected into sterile tubes maintained at 37°C and then rapidly transported to the laboratory where it is screened for presence of cumulus oocyte complexes | A | I |
| EBR | At the end of the procedure, the vagina was thoroughly examined with a speculum and if necessary local compression was applied to allow haemostasis | A | II |
| EBR | Factors that will guide the choice of treatment between IVF and ICSI depend on semen parameters, other factors which affect the chance to pregnancy and special situations | B | II |
| EBR | OCCs are then transferred to media with bicarbonate and incubated/cultured for at least 4 hours | A | I |
| EBR | In IVF Insemination after 4–6 hours of OR and then inseminated with 10000 sperms per oocyte either in central well dish or micro droplets. Denude after 16–18 hours and check for fertilization | A | I |
| EBR | ICSI should be done after 40 hours after oocyte trigger. Injected oocytes washed and cultured in microdroplets and checked for fertilization after 16–18 hours | A | II |
| EBR | Recommendation for routine prophylactic antibiotics before embryo transfer cannot be made | B | III |
| EBR | Embryos are analysed for the rate of development, level of fragmentation, and quality using a quality score till embryo transfer | A | I |
| EBR | Embryo transfer can be done at cleavage or blastocyst stage and the remaining embryos cryopreserved | A | I |
| EBR | Number of embryos depends on the age, cause of subfertility stage of transfer, quality of embryos and policy | B | II |
| EBR | Use of USG guided soft catheter embryo transfer technique improve results and lower the variability of the results by making it less traumatic, standardized, and technically precise | A | I |
References
Greil AL, Slauson-Blevins K, McQuillan J. The experience of infertility: a review of recent literature.
Sociol Health Illn. 2010; 32(1):140–62.
National guidelines for accreditation, supervision and regulation of ART clinics in India. Indian
Council of Medical Research and National Academy of Medical Sciences (India), 2005. Available at:
https://www.icmr.nic.in/sites/default/files/art/ART_Pdf.pdf. Accessed 24th October 2019. Accessed 24th October 2019.
NICE guidance (2017) Fertility problems: assessment and treatment. Available at: https://www.nice.org.uk/guidance/cg156/evidence/full-guideline-pdf-188539453. Accessed 24th October 2019.
Practice Committees of the American Society for Reproductive Medicine and Society for Assisted Reproductive Technology. Intracytoplasmic sperm injection for non-male factor infertility – committee opinion. Fertil Steril. 2012;98(6):1395–9.
Merchant R, Gandhi G, Allahbadia GN. In vitro fertilization/intracytoplasmic sperm injection for male infertility. Indian J Urol. 2011;27(1):121–32.
Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: proceedings of an expert meeting. Human Reproduction, Vol.26, No.6 pp. 1270–1283, 2011.
Rajfer J. TESA or TESE: Which Is Better for Sperm Extraction? Rev Urol. 2006;8(3):171.
Stephens SM, Arnett DM, Meacham RB. The use of in vitro fertilization in the management of male infertility: what the urologist needs to know. Rev Urol. 2013;15(4):154–60.
Kim HO, Sung N, Song IO. Predictors of live birth and pregnancy success after in vitro fertilization in infertile women aged 40 and over. Clin Exp Reprod Med. 2017;44(2):111–117.
Bhattacharya S, Hamilton MP, Shaaban M, Khalaf Y, Seddler M, et al. Con- ventional in-vitro fertilisation versus intracytoplasmic sperm injection for the treatment of non-male-factor infertility: a randomised controlled trial. Lan- cet 2001;357:2075–9.
Van der Westerlaken, Helmerhorst F, Dieben S, Naaktgeboren N. Intracytoplasmic sperm injection as treatment for unexplained total fertilization fail- ure or low fertilization after conventional in vitro fertilization. Fertil Steril 2005;83:612–7.
Human Fertilisation and Embryology Authority (HFEA). Fertility treatment 2017: Trends and figures.
Available at: https://www.hfea.gov.uk/media/2894/fertility-treatment-2017-trends-and-figures- may-2019.pdf. Accessed 24th October 2019.
Mohawash W, Bushaqer N, Alrakaf F, et al. Progesterone level on the day of triggering and pregnancy outcome in long GnRH agonist protocol. MMiddle East Fertil. Soc. J. 2018;23:14–18.
De Placido G, Wilding M, Strina I, et al. High outcome predictability after IVF using a combined score for zygote and embryo morphology and growth rate. Hum Reprod. 2002;17(9):2402-9.
Shevell T, Malone FD, Vidaver J, et al. Assisted reproductive technology and pregnancy outcome. Obstet Gynecol. 2005;106(5 Pt 1):1039–1045.
Wen J, Jiang, J, Ding, C, Dai, J, Liu, Y, Xia, Y et al. Birth defects in children conceived by in vitro fertilization and intracytoplasmic sperm injection: a meta-analysis. Fertil Steril 2012;97,1331–1337.
Davies MJ, Moore VM, Willson KJ, et al. Reproductive technologies and the risk of birth defects. N Engl J Med. 2012;366:1803–1813.
Davies MJ, Rumbold AR, Marino JL, et al. Maternal factors and the risk of birth defects after IVF and ICSI: a whole of population cohort study. BJOG. 2017;124(10):1537–1544.
Williams C, Sutcliffe A, Sebire NJ. Congenital malformations after assisted reproduction: risks and implications for prenatal diagnosis and fetal medicine. Ultrasound Obstet Gynecol 2010;35:255–9.
Chapter 15: Management of Poor Ovarian Responders
OVERVIEW
This guideline offers recommendations on the diagnostic tests, treatment regimens and health promotion principles needed for the effective management of poor ovarian response (POR) covering defining women with POR and its new classification, and a focus on the management options.
1. Introduction
The success of an ART cycle in most cases is directly proportional to the number of oocytes retrieved
Patients with a diminished ovarian reserve or poor ovarian response (POR) to exogenous gonadotropin stimulation have been a therapeutic challenge for reproductive specialists
Besides the limited understanding of the pathophysiology, there is wide heterogeneity in the definition of poor responders as well as overall disappointing outcomes in assisted reproductive technology
Various strategies have been employed for the management of poor responders which will be covered in this guideline
2. Definition of POR
-
Initially the Bologna criteria were used to define poor responders. At least two of the following three features must be present to label the patient as a poor responder
Advanced maternal age (≥40 years) or any other risk factor for POR
A previous POR – ≤3 oocytes with a conventional stimulation protocol
An abnormal ovarian reserve test – AFC <5–7 follicles or AMH – 0.5 – 1.1 ng/ml
Supplemental criteria includes two episodes of POR after maximal stimulation in the absence of advanced maternal age or abnormal ORT
Bologna criteria is not ideal as it does not address the heterogeneity of subgroups, specific profiles of abnormal ovarian response (hypo and sub–optimal) are not included, does not take into consideration age–related aneuploidies
To resolve the shortcomings in the Bologna criteria, recently, the POSEIDON group (Patient-Oriented Strategies Encompassing Individualized Oocyte Number) proposed a new classification and coined a new definition of poor ovarian responders (POR) as “Low Prognosis” to guide patient management based on the ability to retrieve the number of oocytes necessary to obtain at least one euploid embryo (Figure 1).
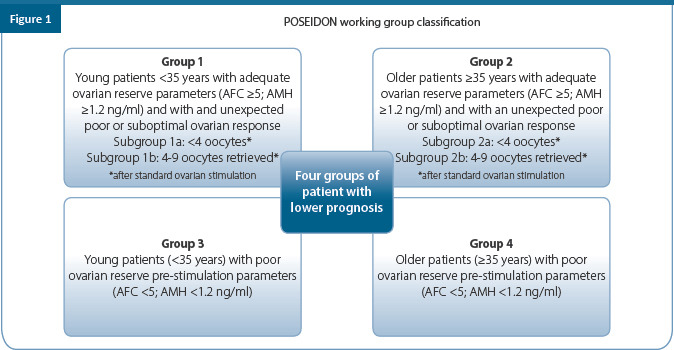
3. Diagnosis and investigations
For the diagnosis of poor ovarian response, the patient is required to have undergone controlled ovarian stimulation and oocyte retrieval
By now it is too late and no intervention can be done in the current cycle and therefore prediction of poor ovarian response is important
Although difficult, it is extremely important to predict poor response to individualize the stimulation protocol for the patient
Choice of marker used may depend on the organization, setting, availability of equipment or patient–related conditions
-
Offer tests to help in diagnosing and predicting response to ovarian stimulation. Tests are as follows:
-
»
High levels of serum FSH (>12 or >15 mIU/mL) on cycle days 2 or 3
-
»
Elevated levels of serum estradiol (>30 or 75 pg/mL) on cycle days 2 or 3
-
»
Decreased levels of serum inhibin B (45 pg/mL) on cycle days 2 or 3
-
»
Decreased serum concentrations of anti–mullerian hormone (AMH) of <0.5-1.1ng/ml
-
»
Decreased ovarian volume (OVVOL)
a. Ovarian volume measurement with a cut–off value of 3 cm3
-
»
Decreased antral follicle count (AFC)
b. Antral follicle count <5-7
-
»
Currently only serum AMH and AFC are to be considered as standard methods of diagnosing poor reserve which can be used to predict a poor response
It is possible to measure the submerged part of the iceberg of follicle growth, i.e. the intrinsic, so–called ‘acyclic’ ovarian activity by evaluating AMH
Single test is considered sufficient and AFC seems to be efficient and most used
4. Controlled ovarian stimulation (COS) protocols in poor responders
Despite a large number of papers over the last two decades on COS in poor responders, it remains an enigmatic task with the most efficient protocol yet to be defined
Consider using the following protocols for POR
A. GnRH analogues
4.1 Agonist protocol
4.1.1 Long protocol
Mid–luteal, lower dosage (0.1-0.5mg)
4.1.2 Flare–up–short
Follicular start of agonist, gonadotropins 2–3 days later
4.1.3 Ultra short
Stop after 2–3 days of gonadotropins
4.1.4 Stop agonist
Mid-luteal start and stopped on day of menses
4.1.5 Micro dose
4.2 Antagonist protocol
4.2.1 Fixed protocol
When GnRH antagonist is started on day 6 of stimulation
4.2.2 - Flexible protocol
When GnRH antagonist is started when dominant follicle is 14 mm
4.3 Evidence comparing protocols
4.3.1 Antagonist versus long agonist protocol
No difference in OR, embryos transferred, PR/ET, CPR
Antagonist protocol is shorter in duration and is associated with higher cancellation rate (hence, the agonist protocol is preferred)
Antagonist protocol is associated with fewer oocytes retrieved. Lower E2, thinner ET
Cancellation rate similar
4.3.2 Micro dose protocol vs. antagonist protocol
-
Micro dose protocol is associated with:
Significantly higher number of oocytes and peak E 2 levels
No significant difference is observed in fertilization rate, implantation rate, and PR
Antagonist protocol is associated with shorter duration of stimulation and lower gonadotropin requirement
4 RCT till date
4.3.3 Mild stimulation using oral ovulogens with gonadotiropins and GnRH anatagonist protocol vs long agonist protocol
Mild using CC protocol is comparable to GnRH-antagonist with
Significantly shorter duration and lower consumption of gonadotropins
IVF outcome in IR, CPR
Economical advantage
More cycle cancellation rate with mild stimulation
• Lower E2 peak and thin ET with CC use is observed in mild stimulation
4.3.4 Long agonist versus short (flare, ultrashort) agonist
No difference is observed in gonadotropins used, or number of embryos transferred between flare agonist and antagonist
CPR and live birth rate (LBR) are reported to be similar in both protocols
4.3.5 COH protocols (long agonist vs short flare vs stop vs antagonist)
No benefit of any COS protocol over the other
No trials (RCT/retrospective) comparing natural versus conventional stimulation
Dual stimulation (prospective non-inferiority observational study)– May be of benefit in POR
Recommendations
In women with low ovarian response, no differences exist in terms of safety and efficacy between the GnRH agonist and GnRH antagonist protocol
All protocols have similar outcome in terms of OR, embryos transferred, cancellation rate, PR, and LBR
Antagonist protocol is preferred for benefit of shorter duration
Natural/modified natural have no role in COS in POR
B. Gonadotropins (type and dosage) for POR
-
Conventional (150–300 IU) vs higher dosage (>300 IU)
-
»
Higher doses result in more oocytes and therefore more embryos for transfer but not higher IR or PR
-
»
No benefit of higher dosage > 300 IU is reported in POR
-
»
-
Recombinant versus urinary Gonadotropins
-
»
No RCT compares urinary and recombinant gonadotropins
-
»
Only small retrospective study compares hMG vs. rLH and rFSH
-
»
hMG vs. rLH and rLH (retrospective )
-
»
-
Addition of rLH to rFSH
-
»
Addition of r–LH to r–FSH has shown to offer benefit in women with:
-
-
Advanced age
-
-
Women defined as POR by Bolognas criteria and POSEIDON group 1 and 2 (hypo– responders)
-
-
-
»
Recommendations
-
Doses higher than 300 IU is of little advantage in increasing CPR and LBR
-
»
May give additional oocytes but data on cumulative LBR from surplus embryos lacking
-
»
Choosing Recombinant over urinary gonadotropins is not supported by strong evidence
Addition of rLH may benefit women with advanced age or hypo–responders
5. Management based on POSEIDON classification
5.1 Group 1
Adding LH and increasing rFSH are effective in improving FORT
Hypo-response may reflect polymorphisms of Gn and their receptors
Possible pharmacogenomic approach helpful
5.2 Group 2
LH can be effective in increasing oocyte/embryo quantity and competence
Blastocysts accumulation (double stimulation) can be an option
5.3 Group 3
-
iCOS Treatment
-
»
Long GnRHa protocol
-
»
GnRH antagonist (E2, OCP)
-
»
Stimulation with 300 IU/day GT
-
»
Androgens?
-
»
-
Embryo Transfer strategy
-
»
Fresh transfer
-
»
Oocyte/embryo accumulation and FET
-
»
Measure of success – Total of 4–7 oocytes needed to obtain 1 euploid blastocyst
-
»
5.4 Group 4
-
iCOS Treatment
-
»
Long GnRHa protocol
-
»
GnRH antagonist (E2, OCP)
-
»
Stimulation with 300 IU/day GT/addition of LH
-
»
Androgens?
-
»
-
Embryo Transfer strategy
-
»
Fresh transfer
-
»
Oocyte/embryo accumulation and FET
-
»
Measure of success – Total of 12 oocytes needed to obtain 1 euploid blastocyst
-
»
In group 3 and 4, if ovarian reserve is low and FORT is high, no GTs can compensate!!!
DuoStim can be an option in young patients where aneuoploidy rates are still low
6. Adjuvant therapy
6.1 Androgens
Testosterone in the form of gel/ spray/patch
Dehydroepiandrosterone (DHEA)
Rationale for use of androgens
Expression of IGF–1 in the serum improves the response to gonadotropins
Androgens modulate ovarian physiology, promote oocyte and follicle maturation.
Exerts local effects on the endometrium during ovulation, and implantation to improve pregnancy
Dosage of testosterone
Offer testosterone– Tablets 12.5 mg/day; 1% gel, spray, and patch
Consider the treatment to be started 5–21 days until stimulation is initiated
Evidences for testosterone
2 RCTs suggest that addition of testosterone increases CPR and LBR
Testosterone is reported to improve LBR compared to placebo (32% vs. 10%)
Recent meta–analysis showed significantly improved CPR (OR 2.41; 95% CI 1.16–5.04) and LBR (OR 2.18; 95% CI 1.01–4.68), but the number of oocytes retrieved was not statistically significant (mean difference 0.94; 95% CI 0.24–1.64)
ESHRE guidelines on COS indicates that use of testosterone before COS is probably not recommended in low responders (as quality of evidence from meta–analysis of low quality)
Dosage of DHEAS
Offer DHEAS 75 mg for 12 weeks prior to ovarian stimulation in poor responders
Evidences for DHEAS
-
A Cochrane database demonstrated that, DHEA compared to placebo revealed:
-
»
Higher LBR (12% vs. 15%–26%) and ongoing PR
-
»
No difference in miscarriage rate
-
»
However, in a sensitivity analysis removing trials at high risk of performance bias, the effect size was reduced and no longer reached significance (5 RCT, 1913 OR 1.50, 95% CI 0.88–2.56, 306 women)
-
»
The ESHRE Reproductive Endocrinology Guideline Group recommends:
-
-
Use of DHEAS before or during controlled stimulation is probably not recommended for low responders
-
-
-
»
6.2 Growth hormone (GH)
Rationale
High levels of GH in follicular fluid result in oocytes with good morphology, rapid cleavage, and therefore is considered to have better implantation potential
Evidences for GH use
-
A recent systematic review and meta–analysis reported
-
»
Significantly higher live birth rate (9 RCT, RR 1844 1.73, 95% CI 1.25–2.40, 562 women) in the GH group compared to control group in poor responders undergoing IVF treatment
-
»
Significantly higher number of oocytes retrieved (6 RCT, SMD 1.09, 95% CI 0.54 to 1.64, 523 women) and mature oocytes (5 RCT, 1847 SMD 1.48, 0.84 to 2.13, 469 women) in the GH group compared to control group in poor responders undergoing IVF treatment
-
»
-
An RCT, more recent than the above–mentioned meta–analysis, including 127 Bologna criteria poor 1850 responders, compared adjuvant GH with no adjuvant treatment in the GnRH antagonist protocol
-
»
No significant difference in ongoing pregnancy rate (8.1% (5/62) vs. 9.2% (6/65)) or number of retrieved oocytes (3.7±2.6 vs. 3.4±2.5) was observed with GH compared to control group
-
»
The ESHRE Reproductive Endocrinology Guideline Group recommends
6.3 Aspirin
-
Use of adjuvant GH during/before controlled ovulation stimulation is probably not recommended in low responders
-
»
Doses of aspirin used in the studies varied between 75 mg daily, 80 mg daily or 100 mg daily
-
»
Continue aspirin was until hCG administration for final oocyte maturation, 12 weeks of pregnancy or until delivery
-
»
Evidence for aspirin
-
A Cochrane meta–analysis combining 3 RCTs including 1053 women
-
»
No significant difference in the live birth rate (3 RCT, RR 0.91, 95% CI 0.72-1.15) or ongoing pregnancy rate (2 RCT, RR 0.94, 95% CI 1946 0.69-1.27) was observed between the aspirin and control group
-
»
-
The ESHRE Reproductive Endocrinology Guideline Group recommends:
-
»
Use of adjuvant aspirin during/before controlled ovulation stimulation is probably not recommended in low responders
-
»
6.4 Vasoactive substances like arginine
It is recommended that the empirical use of adjuvants should be avoided pending good quality evidence from well–designed studies
6.5 Antioxidants
Insufficient number of studies has examined the associations of nutritional factors and ovarian reserve, especially measuring AMH as a marker, and timing of menopause
The findings of some studies suggest modest associations of some single nutrients or food items with ovarian reserve and age at menopause
To better understand this issue, more studies examining the associations of dietary intakes and dietary patterns with concentrations of AMH and age at menopause are needed
7. Laboratory issues
ICSI for low oocyte yield
Low egg number is not an indication to perform ICSI in the presence of normal semen parameters
The use of ICSI over conventional IVF is not supported to improve proportion of embryos per obtained oocyte, cycle cancellation rate, fertilization rate, implantation rate, clinical pregnancy rate (PR), live birth rate (LBR), cumulative PR, and cumulative LBR
ICSI doesn’t show advantages over IVF even when only one oocyte was retrieved
8. Pre–implantation genetic screening or PGT–A for poor responders
Low oocyte numbers as well as rise in aneuploidy of embryos contribute to poor reproductive outcomes in advanced age women
Age–related effects on aneuploidy rates seem to be driven by impaired mitochondrial function, increased granulosa cell apoptosis, and increased levels of oxidative stress in germline cells
At least 12 oocytes would be required in order to produce one euploid embryo
PGT–A has shown to significantly decrease time to live birth by an average of three months in patients with diminished ovarian reserve
Further, PGS appears to have a decreased risk for ongoing aneuploid gestations
Offering embryonic screening paradigm to patients with POR serves as a way to decrease time to live birth and may decrease the risk of clinical miscarriage and abnormal ongoing gestations
Still there is no consensus related to employing blastocyst culture and PGS in poor responders
9. Ideal day of embryo transfer
Higher pregnancy and implantation rates have been reported with blastocyst compared to cleavage stage embryo transfers
The Cochrane review 2016 of 12 randomized controlled trials demonstrated that live birth rates can be optimized by performing blastocyst transfer compared to cleavage stage embryo transfers
Chromosomal abnormalities are largely reduced at the blastocyst stage compared to cleavage embryo stage
Even though the cancellation rate in the blastocyst (day 5) strategy is significantly higher than in the cleavage stage (day2/3) strategy, the PR, clinical PR, and even LBR per oocyte retrieval still remains significantly higher in the blastocyst
Women with POR can be offered blastocyst transfer after adequate counselling for possibilities of cancelation of transfer
10. Numbers of embryo transfer
Elective single embryo transfer allows less burden and complications (i.e., miscarriage and multiple gestations)
Success of eSET is comparable to double cleavage stage embryo transfer
The real focus in patients with poor ovarian response should be on strategies to obtain oocytes with genetic and cytoplasmic competence, rather than on strategies to obtain more oocytes
11. Oocyte donation
In patients with a clear depletion of the ovarian reserve, or in presence of recurrent IVF failures, especially after multiple euploid ETs, the only options left are adoption or ovum donation
The ethical and moral uncertainties are the main concerns related to the transfer of an embryo partially non–self
Despite the high success rate of OD, recent evidences from reviews and meta–analyses suggest that pregnancies achieved by this strategy show a significant increase in the likelihood of several obstetrics and maternal complications with respect to pregnancies achieved through IVF with own eggs
Interestingly, all these risks are independent of maternal age, suggesting that their causes might be ascribed to an immunological mechanism, e.g., host vs. graft rejection phenomenon
OD–derived embryos are in fact totally allogenic to the mother and may cause the onset of an immunologic reaction in the recipient that could impair the process of placentation
12. Newer advances
On a more experimental basis the future handling of the expected POR patient might include
Intra–ovarian androgen priming
In vitro activation
Stem cell therapy – intraovarian injection of stem cells
-
In vitro oogenesis
-
»
Development of oocytes from stem cells of the patient.
-
»
The successful reconstitute of oogenesis in vitro includes the initial phase of meiosis,
-
»
follicular assembly, and appropriate conditions to support sufficient oocyte growth, and complete maturation
-
»
This is probably the most promising future treatment
-
»
-
Autologous mitochondrial transfer
-
»
To improve the implantation potential and quality of the embryo
-
»
-
Pharmacogenomics
-
»
Taking the genome of the patient into consideration when designing drugs and planning a treatment
-
»
Summary of recommendations
Compared to Bologna criteria, POSEIDON gives a better overview of POR patients
The diagnosis is by AFC<5, AMH<1.2, and FSH>15
E2, and ovarian volume per say is not diagnostic
A single prior IVF cycle gives a lot of insight to POR
-
There is no ideal protocol for poor ovarian reserve and poor responder patients, hence a large no of protocols have been tried. The common used protocols seem to be:
Antagonist protocol
Agonist short protocol
Microdose flare protocol
Letrozole/ CC–HMG protocol
Agonist stop –antagonist protocol
Rec.FSH vs rFSH+rLH (this seems to help the subgroup POSEIDON Group 1 & 2)
Using more than 300 IU of gonadotrophin does not seem to increase the oocyte yield
Synchronize the follicle pool with premenstrual estrogen/P4 treatment or long protocol
Use a combination of FSH and LH
Dual stimulation or pooling when appropriate
-
Adjuvants:
-
»
Testosterone: Recent meta–analysis showed increased CPR and LBR, but the number of oocyte retrieved were not significant
-
»
ESHRE guidelines on COS indicates that use of testosterone before COS is probably not recommended in low responders (as quality of evidence from meta–analysis of low quality)
-
»
Role of DHEA and GH is debatable. The ESHRE Reproductive Endocrinology Guideline Group
Recommends: 1. Use of DHEAS before or during controlled stimulation is probably not recommended for low responders
Use of adjuvant GH during/before controlled ovulation stimulation is probably not recommended in low responders
ICSI does not show advantages over IVF even when only one oocyte was retrieved
There is no consensus related to employing blastocyst culture and PGS in poor responder
Day 3 vs. Day 5 transfer: Women with POR can be offered blastocyst transfer after adequate counselling for possibilities of cancelation of transfer
Oocyte donation: With a clear depletion of the ovarian reserve, or in presence of recurrent IVF failures, especially after multiple euploid ETs, the only options left are adoption or ovum donation
The newer advances like intraovarian activation, ovarian tissue freezing, activation and reimplantation, stem cell/PRP injection to ovarian cortex, autologous mitochondrial transfer are still experimental
Conclusion
Management of POR still represents a therapeutic challenge for the clinician. POR are a heterogeneous group with no uniform protocol and one cannot recruit follicles that do not exist in a case of DOR. Moreover, oocyte quality fundamentally cannot be altered with different treatment modalities
16 Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CPP | Compared to Bologna criteria, POSEIDON gives a better overview of POR patients | - | - |
| EBR | The diagnosis criteria used are AFC<5, AMH<1.1, and FSH>15 | A | II |
| EBR | E2 and ovarian volume per say is not diagnostic | C | III |
| EBR | A single prior IVF cycle gives a lot of insight to POR | B | II |
| CCR | There is no ideal protocol for poor ovarian reserve and poor responder patients, hence a large no of protocols have been tried. The common used protocols seem to be: 1. Antagonist protocol 2. Agonist short protocol 3. Microdose flare protocol 4. Letrozole/ CC–HMG protocol 5. Agonist stop–antagonist protocol 5. Rec.FSH vs rFSH+rLH (this seems to help the subgroup POSEIDON Group1 & 2) |
C | - |
| EBR | Using more than 300 IU of GTP does not seem to increase the oocyte yield | B | III |
| EBR | Synchronize the follicle pool with premenstrual estrogen/P4 treatment or long protocol | C | III |
| EBR | Use a combination of FSH and LH | B | II |
| EBR | Dual stimulation or pooling when appropriate | C | III |
| Adjuvants: | |||
| EBR | • Testosterone: Recent meta-analysis showed increased CPR and LBR, but the number of oocyte retrieved were not significantly higher | B | III |
| EBR | • ESHRE guidelines on COS indicates that use of testosterone before COS is probably not recommended in low responders (as quality of evidence from meta–analysis of low quality | C | III |
| EBR | • Role of DHEA and GH is debatable | B | III |
| EBR | • Use of DHEAS before or during controlled stimulation is probably not recommended for low responders | C | IV |
| EBR | • Use of adjuvant GH during/before controlled ovulation stimulation is probably not recommended in low responders | C | III |
| EBR | ICSI doesn’t show advantages over IVF even when only one oocyte was retrieved | B | II |
| EBR | There is no consensus related to employing blastocyst culture and PGS in poor responder | C | IV |
| DAY3 vs. D5 rransfer: | |||
| EBR | Consider day 3 embryo transfer to limit the culture time Women with POR can be offered blastocyst transfer after adequate counselling | B | II |
| EBR | for possibilities of cancelation of transfer. | C | IV |
| EBR | Limit the use of PGS in patients with very few available embryos | B | I |
| CPP | Oocyte donation: With a clear depletion of the ovarian reserve, or in presence of recurrent IVF failures, especially after multiple euploid ETs, the only options left are adoption or ovum donation | - | - |
| Research points | The newer advances like intra–ovarian activation, ovarian tissue freezing, activation and reimplantation, stem cell/PRP injection to ovarian cortex, autologous mitochondrial transfer are still experimental | - | - |
References
Ferraretti AP, La Marca A, Fauser BC et al. ESHRE working group on Poor Ovarian Response Definition, ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011; 26(7):1616–24.
Poseidon Group (Patient-Oriented Strategies Encompassing IndividualizeD Oocyte Number), Alviggi C, Andersen CY et al. A new more detailed stratification of low responders to ovarian stimulation: From a poor ovarian response to a low prognosis concept. Fertil Steril. 2016; 105(6):1452–3.
Humaidan P, Alviggi C, Fischer R, Esteves SC. The novel POSEIDON stratification of ‘Low prognosis patients in Assisted Reproductive Technology’ and its proposed marker of successful outcome. F1000Res. 2016; 5:2911. Published 2016 Dec 23. doi:10.12688/f1000research.10382.1
Gallos ID, Eapen A, Price MJ et al. Controlled ovarian stimulation protocols for assisted reproduction: a network meta-analysis. Cochrane Database of Systematic Reviews. Cochrane Systematic Review - Intervention - Protocol 2017 https://doi.org/10.1002/14651858.CD012586
Polyzos NP, Blockeel C, Verpoest W, et al. Live birth rates following natural cycle IVF in women with poor ovarian response according to the Bologna criteria. Hum Reprod. 2012; 27(12):3481–6.
Scott RT, Toner JP, Muasher SJ, et al. Follicle-stimulating hormone levels on cycle day 3 are
predictive of in vitro fertilization outcome. Fertil Steril. 1989;51(4):651–4.
Prapas Y, Petousis S, Dagklis T, et al. GnRH antagonist versus long GnRH agonist protocol in poor IVF responders: A randomized clinical trial. Eur J Obstet Gynecol Reprod Biol. 2013; 166(1):43–6.
Xiao J, Chang S, Chen S. The effectiveness of gonadotropin-releasing hormone antagonist in poor ovarian responders undergoing in vitro fertilization: A systematic review and meta- analysis. Fertil Steril. 2013; 100(6):1594–601.e1–9.
Schmidt DW, Bremner T, Orris JJ, et al. A randomized prospective study of microdose
leuprolide versus ganirelix in in vitro fertilization cycles for poor responders. Fertil Steril. 2005; 83(5):1568-71.
Mohamed KA, Davies WA, Allsopp J, et al. Agonist “flare-up” versus antagonist in the management of poor responders undergoing in vitro fertilization treatment. Fertil Steril. 2005; 83(2):331-5.
Demirol A, Gurgan T. Comparison of microdose flare-up and antagonist multiple-dose protocols for poor-responder patients: A randomized study. Fertil Steril. 2009; 92(2):481–5.
Revelli A, Chiadò A, Dalmasso P, et al. “Mild” vs. “long” protocol for controlled ovarian
hyperstimulation in patients with expected poor ovarian responsiveness undergoing in vitro fertilization (IVF): A large prospective randomized trial. J Assist Reprod Genet. 2014; 31(7):809-15.
ESHRE Reproductive Endocrinology Guideline Group. Controlled Ovarian Stimulation for
IVF/ICSI. 2019
Hill MJ, Levens ED, Levy G, et al. The use of recombinant luteinizing hormone in patients undergoing assisted reproductive techniques with advanced reproductive age: a systematic review and meta-analysis. Fertil Steril. 2012; 97(5):1108–14.e1.
Alviggi C, Conforti A, Esteves SC et al. Recombinant luteinizing hormone supplementation in assisted reproductive technology: a systematic review. Fertil Steril. 2018; 109(4):644–64.
Wong PC, Qiao J, Ho C et al. Current opinion on use of luteinizing hormone supplementation in assisted reproduction therapy: an Asian perspective. Reprod Biomed Online. 2011; 23(1):81-90.
Ubaldi F, Vaiarelli A, D’Anna R et al. Management of poor responders in IVF: Is there anything new? Biomed Res Int. 2014; 2014:352098.
Li XL, Wang L, Lv F, et al. The influence of different growth hormone addition protocols to
poor ovarian responders on clinical outcomes in controlled ovary stimulation cycles: A systematic review and meta-analysis. Medicine (Baltimore). 2017; 96(12):e6443.
Toner JP, Philput CB, Jones GS, et al. Basal follicle-stimulating hormone level is a better predictor of in vitro fertilization performance than age. Fertil Steril. 1991;55(4):784–91
Licciardi FL, Liu HC, Rosenwaks Z. Day 3 estradiol serum concentrations as prognosticators of ovarian stimulation response and pregnancy out-come in patients undergoing in vitro fertilization. Fertil Steril. 1995; 64(5):991–4.
Broekmans FJ, Kwee J, Hendriks DJ, et al. A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update. 2006; 12(6):685–718.
Broer SL, Mol B, Dólleman M, et al. The role of anti-Müllerian hormone assessment in assisted reproductive technology outcome. Curr Opin Obstet Gynecol. 2010; 22(3):193-201.
La Marca A, Sighinolfi G, Radi D, et al. Anti-Mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART). Hum Reprod Update. 2010; 16(2):113-30.
Gibreel A, Maheshwari A, Bhattacharya S, et al. Ultrasound tests of ovarian reserve; a systematic review of accuracy in predicting fertility outcomes. Hum Fertil (Camb). 2009; 12(2):95-106.
Broer SL, van Disseldorp J, Broeze KA, et al. Added value of ovarian reserve testing on patient characteristics in the prediction of ovarian response and ongoing pregnancy: An individual patient data approach. Hum Reprod Update 2013; 19; 26-36.
Chapter 16: Advances in Infertility
OVERVIEW
Infertility is a prevalent condition that affects over 80 million people globally. A variety of lifestyle choices and genetic issues have been implicated in the condition. These recommendations covers the advanced techniques for treating fertility problems. It aims to reduce variation in practice and improve the way fertility problems are investigated and managed.
1 Recommendations
1.1 Thin endometrium
Thin endometrium is defined as endometrial thickness <7 mm or <8 mm on the day of human chorionic gonadotropin (HCG) administration
Measurement of thin endometrium
Ultrasound is the ideal noninvasive tool to evaluate the endometrium
1.1.1 Platelet rich plasma (PRP) for thin endometrium
The definition and cut–off for thin endometrium differs between studies, although most studies use endometrial thickness <7 mm or <8 mm on the day of human chorionic gonadotropin (HCG) administration
PRP plays an active role in promoting endometrial proliferation improving embryo implantation rate and clinical pregnancy rates
The benefits of PRP for these infertile women with thin endometrium may be due to the 4 times higher platelets and significant greater amounts of growth factors as platelet–derived growth factor (PDGF)–AB, PDGF–BB, and transforming growth factor (TGF)–β in PRP than peripheral blood (p<0.01)
PRP is beneficial but further studies are required
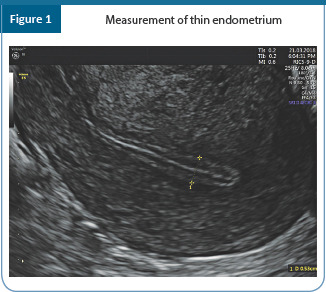
1.1.2 Intrauterine stem cell perfusion for thin endometrium
-
Bone marrow–derived cells are implicated as possible endometrial progenitors.
-
»
Origination of the cells from bone marrow mesenchymal stem cells or, alternatively, is circulating endometrial cells originally derived from the endometrium and harboured in bone marrow is unknown
-
»
Regardless of their origin, these cells may serve as a source of reparative cells for the reproductive tract
-
»
Both stromal and epithelial cells were derived from bone marrow origin
-
»
Researches show the potential for stem cells to have a role in the regeneration or repair of this tissue after injury
Significant engraftment of endometrium by bone marrow is likely to occur after endometrial injury or inflammatory insult
Severe Asherman’s syndrome cases involving damaged basal endometrium layer are reported to have better response with autologous stem cells than with PRP
Adipose tissue derived stem cells are also found to be very promising in one of the recent studies in cases of thin endometrium
As far as ethical aspect is concerned, as per The Gazette of India published in April 2018, use of autologous stem cells does not need any special licence by treating hospital
1.2 Summary of recommendations
| Category | Summary statements | Quality of evidence | Justification | |
|---|---|---|---|---|
| CCR | Various factors can limit the accuracy of endometrial measurements such as fibroids, adenomyosis, polyps, uterine orientation, body habitus, previous surgeries, uterine contractions, ultrasound machine quality, interobserver and intra–observer variability, and patient intolerance | II | ||
|
| ||||
| Recommendations | Strength | Quality of evidence | Justification | |
|
| ||||
| EBR | The endometrium should be measured transvaginally in the sagittal plane at the thickest portion near the fundus | B | III | Recommendation is based on commonly accepted practice and to ensure consistency in measurements to aid in clinical assessment, research, and reporting |
| EBR | Repeat any thin endometrium measurement. | D | IV | Recommendation is based on commonly accepted practice and intra–observer variability |
| EBR | Uterine cavity assessment by hysteroscopy or sonohysterogram may be performed in the assessment of a patient with thin endometrium to assess for pathological cause | D | IV | Consensus opinion from the Committee for Practice Guidelines: Although the incidence of intrauterine adhesions in patients with thin endometrium is unknown, uterine assessment may identify patients who may benefit from surgical management |
1.2 Poor ovarian reserve
1.2.1 Platelet rich plasma (PRP) in ovarian rejuvenation
Premature ovarian insufficiency (POI) affects around 1%–3% of women in the reproductive age below 40 years, and around 0.1% in women below 30 years of age
Only around 5%–10% of POI women conceive spontaneously due to fluctuations in ovarian functions. First data on intra–ovarian injection of calcium gluconate activated autologous platelet rich plasma was published in 2018. There is still a debate regarding volume of PRP that should be injected in cases of premature ovarian failure
-
Two different routes for injecting PRP are as follows:
-
»
Transvaginal under ultrasound guidance
-
»
Laparoscopy routes
-
»
There are scanty studies supporting use of PRP for ovarian rejuvenation therapy
1.2.2 Intra ovarian stem cells for premature ovarian failure and ovarian rejuvenation
Stem cell (SC) therapy has emerged enormously, particularly for indications where not much can be done medically or surgically to improve the condition
SCs are the foundation cells for every organ, tissue and cell in the body, and it can either reproduce into a SC or differentiate into specialized types of cells
-
Recently, Herraiz et al conducted a study to assess if infusion of human BMDSCs (bone marrow derived stem cells) could promote follicle development in the patients with impaired ovarian functions
-
»
The researchers conducted the experiments in mice and obtained promising results which raised the possibility that promoting ovarian angiogenesis by BMDSC infusion could be an alternative approach to improve follicular development in women with impaired ovarian function
-
»
The world’s first baby following use of intraovarian stem cells injection in a 45 year old lady is reported in India
Still larger studies and data are needed to support the use of stem cells in ovarian rejuvenation
1.3 Noninvasive chromosomal analysis of embryos
Chromosomal abnormalities are known to cause recurrent implantation failure, early pregnancy loss or severe chromosomal diseases. Around 50% of miscarriages are due to aneuploidy.
One of the major limitations of PGS–TE (preimplantation genetic screening-trophoectoderm) biopsy is not only its technically challenging and invasive procedure, there is still alarming presence of chromosomal mosaicism within the developing embryo
Although there appears to be a high concordance rate between TE cells and inner cell mass (ICM) cells in selected blastocysts, a TE biopsy may not always represent the remainder of the TE or the ICM
Detection of mosaicism can be up by 30% when next–generation sequencing (NGS) is applied for chromosomal analysis
Circulating cell–free embryonic DNA is present in the blastocoel fluid (BF) and spent culture media of blastocysts which can be used for non-invasive screening of chromosomes. Therefore, BF may represent a source of embryonic genetic material that is routinely discarded during vitrification
Obtaining BF is not only noninvasive but also technically easy and a very cost effective option. It is also found that the amount of DNA found in BF is of the same extent at times better than TE biopsy obtained DNA
Recently, cell–free embryonic DNA has also been found in blastocyst culture condition medium (BCCM) and has shown good results for preimplantation genetic diagnosis and preimplantation genetic screening were only recently published
1.4 Uterine transplant
Advise the women with uterine factor infertility (UFI) having a nonfunctional or absent uterus to explore in vitro fertilization (IVF) with a gestational carrier (where legal), adoption, foster parenting, or to lead a life without children
Uterus transplantation is currently considered an experimental procedure and should not be performed outside of an Institutional Review Board approved research protocol. These trials should be listed on Clinicaltrials.gov
Multidisciplinary transplantation team should include a transplant surgeon, gynaecologic surgeon, maternal–fetal medicine specialist, anesthesiologist, infectious disease specialist, psychiatrist or psychologist, neonatologist, pathologist, radiologist, bioethicist or professional with bioethics expertise, social worker, living donor advocate as described by United Network for Organ Sharing (UNOS) regulations, research nurse/coordinator transplant medicine specialist
As a surgical team prepares for transplantation attempts in human subjects, surgical practice specific to uterus transplantation is required
Surgical training and preparation may involve either large animal research or cadaver practice to optimize the surgical approach and team training for obtaining and implanting a uterus graft
1.4.1 Ethical concern
Human uterus transplantation is considered a vascularized composite allograft (VCA) similar to transplantation of the face, limbs, abdominal wall, and other non–lifesaving organs, and present unique ethical and logistical considerations
VCAs are regulated in a manner similar to other solid organs and require specialized consent to allow removal of the specified organ as well as its use in research or transported to donors in all series of living donors to date
Care should be taken to avoid undue emotional and psychological pressure in living donors, who are often family members of the recipient seeking transplantation
Inclusion and exclusion criteria should be strictly followed as per ASRM position statement on uterus transplantation, a committee opinion 2018
The organ used during uterus transplantation can be for living or deceased donors; with each approach having its own challenges and strengths
It is necessary for all donors to be blood–type compatible with their intended recipient. All recipients should be screened for preformed anti–human leukocyte antigen (HLA) antibodies prior to transplantation
1.5 Ovarian tissue transplant
Ovarian tissue transplant and cryopreservation is accepted. It still remains an option for patient undergoing gonadotoxic treatment especially for prepubertal girls
Do not offer ovarian tissue transplant for benign conditions or to women who want to delay their child bearing
Ovarian tissue can be stored as cortical biopsies or strips or whole ovaries
Ovarian tissue can be transplanted to pelvic (orthotopic) or extrapelvic site (heterotopic site)
No pregnancies have been obtained from thawed ovarian tissue transplanted to heterotopic site
Pregnancies have been documented from orthotopic site transplant
Clearly state that ovarian tissue transplant does carry a risk of reintroduction of malignancy
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| EBR | For patients with a history of thin endometrium in ART treatment undergoing endometrial preparation for embryo transfer, there is insufficient evidence that any specific protocol (natural cycle or hormone replacement) for endometrial preparation provides better pregnancy outcomes | C | III |
| EBR | In patients with thin endometrium undergoing embryo transfer Weak cycles, we suggest against the use of pentoxifylline, HCG, gonadotropin-releasing hormone agonists, platelet–rich plasma or stem cells to improve pregnancy rates | C | IV |
| EBR | PRP therapy is investigated in women with POF, infertile women more than 35 years of age, and women with low ovarian reserve | D | IV |
| CCR | Noninvasive preimplantation genetic testing (NIPGT) for chromosomal abnormalities assess ment has the potential to be an accurate and reliable option for preimplantation genetic testing of human embryos | D | - |
| CCR | Uterus transplantation from live donors became a reality to treat infertility for treatment of absolute uterine factor infertility | D | - |
| EBR | Ovarian tissue transplantation for: 1. Fertility preservation for cancer patients 2. Rare genetic diseases–confirmed potential in children 3. Known causes of POI 4. Endometriosis 5. Postponing menopause 6. Social freezing – alternative to mature oocytes 7. In combination with in vitro follicle activation 8. Anovulatory PCOS women – modern wedge resection Is no longer experimental and can be used in the above conditions |
B | III |
References
Chang Y, Li J, Li X, et al. Platelet-rich plasma administration has benefit for infertile women with thin endometrium in frozen blastocyst-stage embryo. Fertil Steril. O-190, 2017
Zadehmodarres S, Salehpour S, Saharkhiz N et al. Treatment of thin endometrium with
autologous platelet-rich plasma: a pilot study. JBRA Assist Reprod 2017; 21(1)54-56.
Du H, Taylor HS. Contribution of bone marrow-derived stem cells to endometrium and endometriosis. Stem Cells. 2007; 25:2082–6.
Azizi R, Aghebati-Maleki L, Mohd. Nouri, et al Stem cell therapy in Asherman syndrome and thin endometrium: Stem cell- based therapy. Biomedicine and Pharmacotherapy. 2018; 102:333–343.
Sudoma I, Pylyp L, Kremenska Y, et al. Application of autologous adipose derived stem
cells for thin endometrium treatment in patients with failed ART programs. Journal of stem cell therapy and Transplantation. Feb 2019.
Pouresmaeili F, Fazeli Z. Premature ovarian failure: A critical condition in the reproductive potential with various genetic causes. Int J Fertil Steril. 2014; 8:1–2.
Scott ES, Rickers NS, Xiang Li, et al. First data on in vitro fertilization and blastocyst
formation after intraovarian injection of calcium gluconate-activated autologous platelet rich plasma .Gynecological endocrinology. Feb 2018.1445219.
Toliopoulos IK ,Papageorgiou S. Ovarian rejuvenation therapy with PRP(Plasma rich in platelets)-an innovative solution for womens infertility. Journal of translational Science. 2018; 5:1–2
Herraiz S, Buigues A, Díaz-García C, et al. Fertility rescue and ovarian follicle growth promotion by bone marrow stem cell infusion. Fertil Steril. 2018; 109:90818.e2.
Gupta S, Lodha P, Karthick MS et al. Role of autologous bone marrow derived stem cell therapy for follicular recruitment in premature ovarian insufficiency: Review of
Literature and a case report of world’s first baby with ovarian autologous stem cell therapy in premenopausal woman of age 45 years. J Hum Reprod Sci 2018; 11(2):125– 30
Scott RT Jr, Galliano D. The challenge of embryonic mosaicism in preimplantation
genetic screening. FertilSteril. 2016; 32:337–8
Palini S, Galluzzi L, De Stefani S, Bianchi M, Wells D, Magnani M, et al. Genomic DNA in human blastocoelefluid. Reprod Biomed Online 2013; 26:603–10.
Galluzzi L, Palini S, De Stefani S, Andreoni F, Primiterra M, Diotallevi A, et al.Extracellular
embryo genomic DNA and its potential for genotyping applications. Future Science OA 2015: 1(4), FSO62. pmid:28031914
American Society for Reproductive Medicine position statement on uterus transplantation: A committee opinion. Fertil Steril 2018
Ovarian tissue cryopreservation: a committee opinion , Fertil Steril 2014
Chapter 17: Recurrent Implantation Failure
OVERVIEW
The guideline provides an overview of suggested treatments for RIF, and which of those are recommended. Furthermore, recommendations are made on the investigations that could be helpful to identify the origin of implantation failure and possible therapeutic targets. In addition, recommendations are written regarding organization of care for couples faced with RIF.
1. Scope of the guideline
To examine the causes, potential treatments, and recommendations for patients suffering from RIF
2. Definition of RIF
RIF is as the failure of clinical pregnancy after 4 good quality embryo transfers, with at least three fresh or frozen IVF cycles, in women under the age of 40
An internationally agreed consensus on the definition is yet to be reached
3. Incidence of RIF
Due to variations in definitions for recurrent implantation failure and biochemical pregnancy, there is scarce data that accurately represents the incidence or prevalence
4. Causes
4.1 Gamete/embryo factors
4.1.1 Oocyte quality
Age–related decline in oocyte quality is associated with increased chromosomal non–dysjunction, resulting in aneuploid embryos, decrease in mitochondrial membrane potential, and increase of mitochondrial DNA damage
There is evidence to suggest that aggressive ovarian stimulation protocols may lead to the production of poor–quality oocytes and a higher rate of fertilization failure
Co–culture of embryos with cumulus cells produced improved implantation and pregnancy in women with repeated implantation failure compared with conventional culture without cumulus cells
4.1.2 Poor quality embryos
Older women have more mitochondrial DNA mutations and increased incidence of aneuploidy may be responsible for poor embryonic development
COH and in vitro culture may contribute to poor or retarded embryonic development
4.1.3 Zona hardening
The zona pellucida, hardens naturally after fertilization to prevent polyspermic fertilization, and to protect the integrity of the preimplantation embryo
Increased zona thickness and sona hardening induced by in vitro culture or by in vivo ageing, affect hatching, and associated with lower implantation rates
4.1.4 Sperm quality
High DNA fragmentation may be associated with an increased risk of miscarriage, but its association with RIF has not yet been established
4.1.5 Suboptimal culture conditions
Sophisticated and tailored specific culture conditions and optimal laboratory facilities are needed for optimal embryonic development and lack of these conditions result in RIF
4.2 Parental chromosomal and genetic anomalies
Chromosomal abnormalities are significantly more likely in women who had RIF. The most common abnormality is translocation
4.3 Uterine factors – Anatomical abnormalities
Congenital uterine anomalies
-
Acquired intracavity conditions
-
»
Submucous fibroids
-
»
Intramural fibroids
-
»
Endometrial polyps
-
»
Intrauterine adhesions
-
»
Adenomyosis
-
»
4.4 Altered expression of adhesive molecules
Local dysregulation of normal expression or action of various cytokines, interlukins and integrins
Elevated endometrial NK cells
High levels of aromatase p450 mRNA
Changes in pinopode expression and high matrix metalloproteinases
4.5 Thin endometrium
Thin or hyperechogenic endometrium or persistent endometrial fluid impaired the outcome after ART
4.6 Hydrosalpinges
Hydrosalpinx fluid – alkaline and contains cytokines, PG or other inflammatory compounds – have direct embryo–toxicity or adversely affect the endometrium reflux of hydrosalpinx fluid into uterine cavity result in diminishing embryonic endometrial apposition
Hydrosalpinges can have a negative impact on implantation in women undergoing IVF
4.7 Immunological factors
Principal pathogenic mechanisms mediated by immunological factors are highlighted in the table below
Table1.
Principal pathogenic mechanisms mediated by immune factors
| Interference with: | |
|---|---|
| a) Soluble coagulation factors: | Protein C/S pathway inhibition fibrinolysis inhibition |
| b) Coagulation cells: | Induction of a pro–adhesive, pro–inflammatory and pro–coagulant endothelial phenotype induction of a procoagulant phenotype in monocytes |
| Interference with: | |
| a) Trophoblast cells: | Reduction of proliferation and differentiation GT secretion impairment |
4.8 Thrombophilic condition
A strong association exists between anti–β2 glycoprotein 1 and anti–nuclear antibodies and implantation failure9
But no evidence exists to suggest that these antibodies directly cause the implantation failure
Inherited thrombophilias such as methylene tetrahydrofolate reductase (MTHFR) deficiency, factor V leiden, prothrombin deficiency, and antithrombin III deficiency are seen in higher rate in women with RIF, but they do not have a significant role in IVF embryo transfer implantation failure
4.9 Infection
Diagnose chronic endometritis with on histological examination, on visualization with hysteroscopy, and by bacterial culture
Use immunohistochemistry stain for syndecan–1(CD 138), a plasma cell marker to provide a more accurate diagnosis
4.10 Suboptimal ovarian stimulation
COH associated with supraphysiological E2 –affect oocyte quality & endometrial receptivity
Altered endometrial receptivity due to premature expression of pinopodes and integrins, resulting in precocious luteal transformation
Abnormal luteal phase steroid secretion
4.11 Suboptimal embryo transfer
Suboptimal ET technique can reduce the implantation rate (IR) and pregnancy rate (PR) significantly
It is estimated that poor embryo transfertechnique may account for as much as 30% off all failures in assisted reproduction
5. Investigation of recurrent implantation failure
Table 2.
Investigation of recurrent implantation failure
| Recommended investigations | Investigations of research value |
|---|---|
| Hysteroscopy | Hereditable/acquired thrombophilia |
| Hysterosalpingography | Sperm DNA fragmentation |
| Pelvic ultrasonography | Endometrial receptivity markers |
| Parental karyotype | Embryo biopsy with PGT–A |
| Ovarian reserve and function: FSH, anti–Müllerian hormone, antral follicle count | |
| Thyroid antibody |
6. Management
Through history and examination
Transvaginal ultrasound (2d and 3D) to rule out uterine and adenexal pathology
Ovarian reserve testing
Hysteroscopy to evaluate uterine cavity
Thrombophilia and APLA screen
Karyotyping of both parents
Thyroid antibody evaluation
Sperm DNA fragmentation evaluation
Adopt a multidisciplinary approach in the management of a couple with RIF
Review couples with RIF by an experienced fertility specialist
Offer appropriate counselling of the couple with RIF, which is of the utmost importance prior to proceeding with further treatment
6.1 The uterus
6.1.1 Hysteroscopy
There is convincing evidence that hysteroscopy improves the outcome of women with RIF11
Intracavity lesions
-
Submucous fibroids
-
»
Submucous fibroids significantly reduced the implantation rate, clinical pregnancy rate and live birth rate and significantly increased the miscarriage rate12
-
»
Hysteroscopic removal of submucous fibroids distorting the uterine cavity recommended
-
»
Endometrial polyps
Remove the endometrial polyps in women with RIF.
Removal of endometrial polyps in women undergoing intrauterine insemination resulted in doubling of the clinical pregnancy rate.13
Uterine septum
Uterine septal resection in women with RIF, regardless of the size improves pregnancy rates and decreases miscarriage rate.14
Intrauterine adhesions
It is accepted that intrauterine adhesions would interfere with the implantation process and adversely affect the implantation rate and so, if present in women with RIF, should be removed (March, 2011)
Nevertheless, there are as yet no firm literature data to confirm that removal of intrauterine adhesions improves the implantation rate
6.2 Myometrial pathology
6.2.1 Intramural fibroids
The final decision of myomectomy must be individualized, and the involvement of a reproductive surgeon in the decision–making process is recommended.15
Removal of all intramural myomas close to junction zone alter endometrial peristalsis hampering implantation and therefore removal recommended
6.2.2 Adenomyosis
The role played by adenomyosis in reproductive failure is receiving increasing attention and is now recognized to be a cause of RIF16
6.3 Thin endometrium
Endometrial thickness, ≤7 mm is associated with compromised success rates.17
6.3.1 Treatment of Endometritis
-
Treatment of bacterial and tuberculosis endometritis
-
»
Antibiotics for infection
-
-
In patients who have had CE diagnosed via hysteroscopy and culture, antibiotic therapy has been shown that antibiotic therapy to be an effective intervention to improve endometrial thickness and implantation rate
-
-
-
»
5.3.4 Tuberculosis endometritis
-
-
Premenstrual endometrial sampling for smear, culture, PCR, and histopathology
-
-
Positive for TB requires treatment
-
#
Intensive phase treatment for 2 months with isoniazid, rifampicin, pyrazinamide, and ethambutol
-
#
Followed by 4 months of isoniazid, rifampicin
-
#
-
-
-
»
6.3.2 Adjuvant empirical therapies used to improve endometrial thickness
-
Low–dose aspirin
-
»
Low dose aspirin at least hypothetically might enhance endometrial growth and embryo implantation via a triple mechanism of actions reducing subendometrial contractility minimising inflammation by inhibiting cyclooxygenase and prostaglandin biosynthesis and improving uterine endometrial blood flow19
-
»
The evidence to support the beneficial impact of low dose aspirin in patient with a thin endometrium is scare and controversial as no effect on endometrial thickness or uterine blood has been demonstrated.
-
»
-
Heparin, corticosteroids
-
»
Not many studies on improving endometrial thickness
-
»
Drugs to increase uterine radial artery blood flow – sildenafil, L–arginine, and Vitamin E
-
»
-
Sildenafil
-
»
Sildenafil citrate has also been proposed in the women with RIF associated with a thin endometrium
-
»
The hypothesis behind the use of sildenafil is that it increases endometrial blood flow, but results of observation studies have not yet been confirmed by any RCT
-
»
-
L-arginine (no substrate)
-
»
Relaxes vascular smooth muscells by activating cGMP
-
»
-
Vitamin E
-
»
Increases capillary blood flow and protects endometrium from oxidative stress
-
»
-
Intrauterine injection of hCG
-
»
Intrauterine injection of 500 IU of hCG before embryo transfer improved pregnancy rate compared to control group but was not significantly different.
-
»
-
Granulocyte colony–stimulating factor (G–CSF)
-
»
Infusion of G–CSF in endometrial cavity is a safe and may be effective method to increasing endometrial thickness in patients with thin and unresponsive endometrium
-
»
-
Autologous platelet rich plasma
-
»
PRP intrauterine infusion might be a new alternative for patients with poor endometrial growth although still better solid evidence is expected
-
»
-
Stem cell treatment in implantation failure
-
»
Stem cell therapy may be effective for Asherman’s syndrome and thin endometrium (<5 mm) though the evidence is sparse
-
»
Stem cells used for treatment of a thin endometrium include mesenchymal stem cells, human embryonic stem cells, endometrial stem cells, and non–hematopoietic bone marrow–derived stem cells (BMDSCs) could induce endometrial regeneration
-
»
BMDSCs induce regeneration of endometrial cells by paracrine signalling and this effect is two fold higher if used during uterine injury
-
»
-
Luteal support with GnRHa
-
»
Administration of GnRHa on day of oocyte recovery, on the day of embryo transfer and 3 days later appeared to have significantly higher estradiol, progesterone concentrations, thicker endometrium, higher implantation and pregnancy rates, and may be advocated in women with RIF
-
»
6.3.3 Endometrial injury
The possibility that local injury of the endometrium in the cycle preceding IVF treatment increases the success rate of implantation.20
It is not exactly clear why the endometrial biopsies helps the implantation rate. It is speculated that the healing process following endometrial biopsy may release cytokines and growth factors which facilitate the process of implantation
6.3.4 Microbiota of the uterus
Uterine microbiota may contribute to healthy endometrial physiology and is responsible for receptive fertile endometrium
6.4 Salpingectomy
-
»
Salpingectomy and in some cases tubal occlusion procedures in the presence of hydrosalpinges have been shown to increase the likelihood of implantation success in future IVF cycles.22
-
»
Removal of USG visible unilateral or bilateral hydrosalpinges recommended
6.5 Optimal IVF treatment
6.5.1 Tailoring the stimulation protocols
Softer OI protocols, demonstrate improved IRs
Use of GnRH–antagonist protocols improved blastocyst quality and pregnancy outcome after RIF with GnRH–agonist protocols
Step–down protocol for OI where the FSH ‘window’ is shortened results in reduction in number of recruited and mature follicles and lower E2
In women with endometriosis and adenomyosis, the use of ultra–long protocol involving the administration of gonadotrophin–releasing hormone (GnRH) agonists for a few months prior to IVF or ICSI may increase the pregnancy rate
Optimal luteal phase support recommended
6.5.2 Embryo factor
-
Preimplantation genetic screening–Data suggests that patients with RIF have more chromosome abnormalities within their embryos
-
»
PGT–A for selecting chromosomally normal embryos for ET may increase IRs
-
»
Preimplantation genetic testing for monogenic (single gene) disorders (PGT–M) can be used to evaluate specific chromosomal diseases among IVF patients with specific risk factors
-
»
Preimplantation genetic testing for structural rearrangements (PGT–SR) is recommended in patients with balanced translocations
-
»
6.5.3 Assisted hatching
Hatching of the blastocyst plays an integral role in the implantation process and failure to hatch (due to intrinsic abnormalities in either the blastocyst or zona pellucida) is a possible cause of implantation failure
Assisted hatching involves the artificial thinning or breaching of the zona pellucida and has been proposed as one technique to improve implantation and pregnancy rates following IVF25
Available evidence does not support the routine application of assisted hatching in all IVF cycles
Assisted hatching may be clinically useful in patients with poor prognosis, including those with a history of two or more unsuccessful IVF cycles, poor embryo quality, thick zona, frozen embryo transfers and older women (38 years of age) and
6.5.4 Blastocyst transfer
Blastocyst transfer is more physiological, it examines the property of embryonic genome with improved embryo selection, and uterine receptivity
6.5.5 Frozen vs. fresh embryo transfer
Freeze–all policy is a potentially effective paradigm to improve RIF outcomes, in particular the rates of implantation and clinical and ongoing pregnancy in patients with risk of OHSS, progesterone rise, genetic testing, abnormal endometrium
6.6 Endometrial receptivity array
Transcriptomic signature of ERA test reveal that the endometrial factor is responsible for 25% of cases of patients with RIF. Thus WOI is displaced in 25% of RIF patients, and pET can normalize clinical results
ERA and pET were effective for a subset of patients with unexplained RIF, and by transferring euploid embryos in a personal WOI, with better PRs
It is still questionable whether ERA will be cost–effective as the first diagnostic line for the endometrial factor
6.7 Transfer methods
Improving ET technique – higher PRs obtained with USG guided atraumatic technique and embryos being deposited in middle part of the uterine cavity
Use of fibrin glue may improve pregnancy rates in RIF
A trial embryo transfer should be considered where a prior embryo transfer has been described as difficult or where difficulty may be anticipated
Cervical dilatation undertaken prior to COH in women with previous H/O difficult ET
Sequential embryo transfer
Sequential embryo transfer has been proposed as a means of improving implantation rates29
The concept behind this strategy is to overcome the problem of embryo–endometrium asynchronicity as a potential cause of implantation failure
Till date, there appears to be preliminary evidence to suggest that double–embryo transfer may be of benefit, but carefully designed randomized controlled trials are required to confirm its value, if any, in women with RIF
6.8 Luteal phase support
Progesterone therapy
Progesterone and specifically orally administered dydrogesterone used in IVF protocols, may have a significant role in improving pregnancy, and live birth rates among patients with RIF mainly when started in the luteal phase. More studies are needed to support this
6.9 Antithrombotic agents
-
Aspirin irreversibly inhibits cyclooxygenase activity and prostaglandin production, reduces the inflammatory response, promotes vasodilatation, and increases uterine blood flow but its use in RIF is still controversial
-
»
Heparin has been evaluated for use in RIF patients, though there is not yet evidence to recommend its use for improved pregnancy outcomes in these patients
-
-
A group of RIF patients treated with low molecular weight heparin had almost identical implantation, clinical pregnancy, and live birth rate outcomes when compared with controls31
-
-
-
»
6.10 Immunotherapy
6.10.1 Intravenous immunoglobulin (IVIG)
IVIG treatment has also been regarded as a possible immunological therapy for women suffering from repeated implantation failure with an elevated Th1/TH2 ratio, elevated NK cells, an abnormal TNFa/IL–10 ratio, and auto–antibodies
Expensive interventions, the optimal protocol for the administration of IVIG is undefined, and the overall benefits of IVIG are still controversial
6.10.2 Granulocyte colony-stimulating factor (G–CSF)
The subcutaneous injection of G–CSF can improve the outcome of patients with recurrent miscarriage
-
Intrauterine peripheral blood mononuclear cell (PBMC) administration:
-
»
Intrauterine administration of autologous PBMC activated by human chorionic gonadotropin (hCG) effectively improves embryo implantation and IVF outcomes in patients with RIF
-
»
Mechanism of intrauterine hCG–activated PBMC administration may be that it can promote trophoblast cell spreading and invasion into endometrium and can increase the expression of endometrial factors which facilitate implantation
-
»
There is insufficient evidence to recommend intrauterine infusion of autologous peripheral mononuclear cells prior to ET to improve IVF outcome
-
»
6.10.3 Steroids
Administration of a high dose of methylprednisolone for four consecutive days at the time of oocyte retrieval may improve IVF outcomes
6.10.4 Intralipid infusion
-
Intralipid infusion is a 20% fat emulsion that reduces the Th1/Th2 ratio and suppresses the abnormal NK cytotoxicity of peripheral NK cells, thereby increasing the likelihood of implantation and clinical pregnancy.
-
»
Further studies are needed to determine the efficacy of intralipid infusion in women with RIF
-
»
6.10.5 Tacrolimus: An immunosuppressive drug
Inhibits antigen–induced lymphocytic proliferation, cytotoxic T–cell formation, IL–2 receptor expression, and the production of IL–2 and interferon–gamma
1 to 3 mg tacrolimus 2 days prior to ET may improve clinical pregnancy and live birth rates
There is insufficient evidence to recommend tacrolimus to improve IVF–ET outcome in RIF
6.10.6 Adalimumab (tumor necrosis factor alpha [TNFa] blocking antibody)
Insufficient evidence to recommend adalimumab treatment to improve IVF outcome and should only be used in the context of research as Institutional Review Board (IRB)–approved studies
6.11 Treatment in the male
In addition to maternal factors playing a role in RIF, male factor, particularly spermatozoal morphology also can play a part
Antibody–free preparation of spermatozoa has been investigated to reduce the potential impact of anti–sperm antibodies on fertilization rates in couples with anti–sperm antibody–positive male partners. But there is insufficient evidence to support the recommendation either for or against antibody–free preparation of spermatozoa in improving IVF outcome in RIF
Intracytoplasmic morphologically selected sperm injection (IMSI) selects morphologically normal sperms for ICSI and may be of use in RIF but the evidence is sparse to recommend its use routinely in RIF
Role of PICSI to choose sperms with low DFI is controversial and should not be used
6.11.1 Lifestyle modifications
-
»
Evidence suggests that smoking, obesity, and high cortisol levels also play a role in implantation failure.
-
»
Achieving healthy BMI through exercise and diet
-
»
Cessation of Smoking is advised in both partners as it has a negative impact on sperm quality, fertilization rate, implantation rate, and live birth
-
»
Women with RIF should be advised to abstain from alcohol
6.12 Psychological assistance
-
»
Psychotherapy (group and individual) reduces anxiety and depression and enhances conception success
-
»
Psychological interventions and various relaxation techniques recommended
6.13 Gamete donation and surrogacy
-
»
Advice gamete donation if the likely source of the problem lies with the embryo
-
»
Discuss surrogacy if the problem lies in the uterus, for example multiple small fibroids or Asherman’s syndrome which has failed to respond to surgical treatment
Summary of recommendations
| Category | Recommendation | Grade of recommendation | Quality of evidence |
|---|---|---|---|
| CCR | Appropriate investigations should be carried out to determine the cause of RIF depending on the history and examination | C | - |
| CCR | Hysteroscopy should be carried out to exclude any intracavity uterine pathology; it has been shown to improve outcome | A | - |
| EBR | Submucosal fibroids have been shown to reduce implantation, pregnancy and live birth rates; removal of submucosal fibroids improves implantation rate | A | I |
| EBR | Endometrial polyps should be removed; although there is no data on its impact on women undergoing IVF, it has been shown to improve outcome in women undergoing intrauterine insemination | B | I |
| EBR | Appropriate investigations should be carried out to exclude hydrosalpinx as it has been shown to reduce implantation rate, increase miscarriage rate and reduce live birth rate; removal of hydrosalpinges has been shown to improve the outcome | A | I |
| EBR | Endometrial scratch should be considered in the luteal phase of the cycle immediately preceding IVF treatment; it improves implantation rate and outcome in women with unexplained RIF | B | III |
| EBR | Uterine septum increases miscarriage rate; its removal improves outcome | B | II |
| EBR | Intramural fibroid of more than 5 cm and those close to junctional zone should be removed | C | III |
| CCR | Intrauterine adhesions are a recognized cause of thin endometrium not responding to ovarian steroid stimulation; if present, intrauterine adhesions should be removed | D | - |
| EBR | The use of ultra–long protocol may improve outcome in women with endometriosis and adenomyosis | C | III |
| CCR | Softer OI protocols, demonstrate improved IRs | C | - |
| EBR | Use of GnRH–antagonist protocols improved blastocyst quality and pregnancy outcome after RIF with GnRH–agonist protocols | B | III |
| EBR | No clear evidences published yet about the real efficacy of IMSI and PICSI in improving CPR or LBR in RIF | C | III |
| EBR | PGT–A may increase IR in RIF by selecting euploid embryos for transfer | B | II |
| EBR | Assisted hatching may improve outcome in RIF | C | I |
| EBR | Soft catheters should be routinely used as statistically significant higher CPR and LBR reported | A | II |
| CCR | Removing cervical mucus at the time of embryo transfer to improves CPR and LBR | B | - |
| CCR | Ultrasound guidance during embryo transfer improve CPR and LBR and is recommended | A | - |
| EBR | Proper placement at a distance >10 mm to <20 mm seems to be the best site for embryo transfer to achieve higher PRs | A | II |
| EBR | Minimize embryo stress by mminimizing transfer time (<120 seconds), maintaining temperature/pH which is associated with significant increase in IR and PR | B | II |
| EBR | Easy, atraumatic and technically precise transfer without blood or mucus transfers improve IR | B | III |
| CCR | Optimize implantation, minimize contractions by performing day–5 ET, FET cycles and avoiding trauma to cervix or fundus Piroxicam 10 mg 2 hrs before ET reduces contractions | B | - |
| CCR | Adherence compounds such as hyaluronic acid are valuable in improving the success rate of assisted reproductive technologies such as IVF and ICSI with increase in LBRs in RIF | B | - |
| CCR | There is no evidence to suggest screening for immunological conditions in an asymptomatic population. | B | - |
| CCR | Immunotherapies reviewed in the present document are either not associated with improved live–birth outcome in IVF or have been insufficiently studied to make definitive conclusions regarding benefits and risks. In the absence of well–designed adequately powered RCTs, patients must be informed of uncertain benefits and risks associated with immunotherapy | B | - |
| CCR | Empirical therapies should, whenever possible, be considered only in the setting of carefully conducted clinical trials | D | - |
| CCR | PRP and stem cells Stem cell therapy may be effective treatment for Asherman’s syndrome and thin endometrium (<5 mm) though the evidence is sparse | D | - |
| CCR | Lifestyle changes may improve IR in RIF | D | - |
| CCR | A multidisciplinary approach should be adopted in the management of RIF | D | - |
References
Absalan F, Ghannadi A, Kazerooni M, et al. Value of sperm chromatin dispersion test in couples with unexplained recurrent abortion. J. Assist. Reprod. Genet. 29, 11–14
Azem F, et al. Increased rates of thrombophilia in women with repeated IVF failures. Hum Reprod. 2004; 19(2):368–70.
Ban-Frangez H, Tomazevic T, Virant-Klun I, et al. The outcome of singleton pregnancies after IVF/ICSI in women before and after hysteroscopic resection of a uterine septum compared to normal controls. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009; 146, 184–187.
Barash A, Dekel N, Fieldust S, et al. Local injury to the endometrium doubles the incidence of successful pregnancies in patients undergoing in vitro fertilisation. Fertil. Steril. 2003; 79, 1317–1322.
Benkhalifa M, Demirol A, Sari T, et al. Autologous embryo-cumulus cells co-culture and blastocyst transfer in repeated implantation failures: a collaborative prospective randomized study. Zygote. 2012; 20: 173–180
Berker B, et al. The role of low-molecular-weight heparin in recurrent implantation failure: a prospective, quasi-randomized, controlled study. Fertil Steril. 2011; 95(8):2499–502.
Bernard G, Darai E, Poncelet C, et al. Fertility after hysteroscopic myomectomy: effect of intramural myomas associated. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000; 88, 85–90.
Bosteels J, Weyers S, Puttemans P, et al. The effectiveness of hysteroscopy in improving pregnancy rates in subfertile women without other gynaecological symptoms: a systematic review. Hum. Reprod. Update 2010; 16, 1–11.
Brahem S, Mehdi M, Landolsi H, et al. Semen parameters and sperm DNA fragmentation as causes of recurrent pregnancy loss. Urology 78, 792–7966
C.B. Nagori, S.Y. Panchal, H. Patel, Endometrial regeneration using autologous adult stem cells followed by conception by in vitro fertilization in a patient of severe Asherman’s syndrome, J. Hum. Reprod. Sci. 4 (1) (2011) 43–48.
Cenksoy P, et al. Hysteroscopic findings in women with recurrent IVF failures and the effect of correction of hysteroscopic findings on subsequent pregnancy rates. Arch Gynecol Obstet. 2013; 287(2):357–60.
Coughlan C, et al. Recurrent implantation failure: definition and management. Reprod BioMed Online. 2014; 28(1):14–38.
Coughlan C, Yuan Xi, Demirol A, et al. Factors affecting the outcome of ‘Endometrial Scratch’in women with recurrent implantation filure. J Reprod Med. 2014; 59(1-2):39-43.
De Sutter P, Stadhouders RU, Dutré MA, Gerris J, Dhont M. Prevalence of chromosomal abnormalities and timing of karyotype analysis in patients with recurrent implantation failure (RIF) following assisted reproduction. Facts, views & vision in ObGyn. 2012;4(1):59.
Demirol A, Gurgan T, et al Effect of treatment of intrauterine pathologies with office hysteroscopy in patients with recurrent IVF failure. Reprod. Biomed. 2004; Online 8, 590– 594.
Glujovsky D, Farquhar C, Quinteiro Retamar A, et al. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. Cochrane Database Syst Rev. 2016; (6):CD002118.
Goto S, Takebayashi K, Shiotani M, et al. Effectiveness of 2-step (consecutive) embryo transfer. Comparison with cleavage-stage transfer. J. Reprod. Med. 2003; 48, 370–374.
Karimzadeh MA, Rozbahani M, Tabibnejad N, et al. Endometrial local injury improves the pregnancy rate among, recurrent implantation failure patients undergoing in vitro fertilisation/intra cytoplasmic sperm injection: A randomized clinical trial. Aust. N. Z. J. Obstet. Gynaecol. 2009; 49, 677–680.
Kasius A, Smit JG, Torrance HL, et al. Endometrial thickness and pregnancy rates after IVF: A systematic review and meta-analysis. Hum Reprod Update. 2014; 20(4):530-41.
Lo Monte G, et al. Focus on intracytoplasmic morphologically selected sperm injection (IMSI): A mini-review. Asian J Androl. 2013; 15:608.
Mansour RT, Rhodes CA, Aboulghar MA, et al. Transfer of zona-free embryos improves outcome in poor prognosis patients: a prospective randomized controlled study. Hum. Reprod. 15, 1061–1064.
N. Singh, S. Mohanty, T. Seth, M. Shankar, S. Bhaskaran, S. Dharmendra, Autologous stem cell transplantation in refractory Asherman’s syndrome: a novel cell based therapy, J. Hum. Reprod. Sci. 7 (2) (2014) 93–98.
Practice Committee of American Society for Reproductive Medicine in collaboration with Society of Reproductive Surgeons. Salpingectomy for hydrosalpinx prior to in vitro fertilization. Fertil Steril. 2008; 90(5 Suppl):S66–8.
Practice Committee of Society for Assisted Reproductive Technology; Practice Committee of American Society for Reproductive Medicine. The role of assisted hatching in in vitro fertilization: a review of the literature. Fertil Steril. 2008; 90(5 Suppl):S196-8.
Pritts EA, Parker WH, Olive DL, et al Fibroids and infertility: an updated systematic review ofthe evidence. Fertil.Steril. 2009; 91, 1215–1223.
Rasmark Roepke E, Hellgren M, Hjertberg R et al. Treatment efficacy for idiopathic recurrent pregnancy loss - a systematic review and meta-analyses. Acta Obstet Gynecol Scand. 2018;97(8):921–41
Simon A, Laufer N. Assessment and treatment of repeated implantation failure (RIF). J Assist Reprod Genet. 2012; 29(11):1227–39.
Stern C, et al. Antibodies to β2 glycoprotein I are associated with in vitro fertilization implantation failure as well as recurrent miscarriage: results of a prevalence study. Fertil Steril. 1998;70(5):938–44
Tremellen K, Russell P, et al. Adenomyosis is a potential cause of recurrent implantation failure during IVF treatment. Aust. N. Z. J. Obstet. Gynaecol. 2011; 51, 280–283.
Verberg MF, Eijkemans MJ, Macklon NS, et al. The clinical significance of the retrieval of a low number of oocytes following mild ovarian stimulation for IVF: A meta-analysis. Hum. Reprod. Update. 2009; 15: 5–12
Wada I, Hsu CC, Williams G, et al. The benefits of low-dose aspirin therapy in women with impaired uterine perfusionduring assisted concep- tion. Hum Reprod. 1994; 9:1954–1957
Wang LY, Wang DH, Zou XY et al. Mitochondrial functions on oocytes and preimplantation embryos. J. Zhejiang Univ. Sci. B. 2009; 10: 483–492.
Chapter 18: Third-Party Reproduction
OVERVIEW
This document highlights good practice recommendations on third–party reproduction for practicing gynecologists, embryologists, and infertility specialists in India. Third–party reproduction poses a constant challenge as it is socially, ethically, and legally complex. These recommendations are based on several guidelines from global societies, the Cochrane database, large meta–analysis, available Indian literature, prevalent practices in India, and consensus amongst experts in the field of third-party reproduction. These recommendations strengthen and promote meaningful research that will apply to Indian patients and Indian practice.
1. Sperm donation
1.1 Introduction
-
In couples with infertility, male infertility affects about 25% of couples. Therapeutic donor insemination (TDI) is the most widely used artificial reproductive technique (ART) to treat male infertility; until the availability of intracytoplasmic sperm injection (ICSI). TDI is best indicated when a male partner is likely to pass on an:
-
»
Inheritable genetic condition
-
»
Infections (e.g. human immunodeficiency virus [HIV])
-
»
Severe rhesus incompatibility
-
»
1.2 Indications for considering donor insemination
Male partner with azoospermia, severe oligospermia, or other significant sperm or seminal fluid abnormalities
Male partner with ejaculatory dysfunction or ineradicable sexually transmissible infection
If a male partner is Rh–positive and the female partner is Rh–negative
The partner is either affected or a carrier of genetic abnormality; or in cases where the partner’s history of carrier status is unknown
1.3 Information and counseling
Couples should be counseled about merits of ICSI and donor insemination that allows equal access to both the treatments
Counseling regarding the physical and psychological implications on the couples and their children must be considered from someone independent of the treatment unit
1.4 Screening of sperm donors
Gametes produced by a person aged <21 should not be used. Also, the accepted age of the sperm donor must be between 21 and 45 years
Individuals must be free of infections and diseases such as sexually transmitted diseases (HIV), hepatitis B and C infections, hypertension, diabetes, and other common genetic disorders (thalassemia)
An analysis of the semen of the individual must be done using a semen analyzer according to the world health organization (WHO) manual
Psychological assessment by a qualified healthcare professional is recommended for all sperm donors
Comprehensive medical history to be taken down
Sperm donation by relative or friend is not permitted
Donor samples should be taken from a registered gamete bank
1.5 Assessment of the female partner
To attain effective donor insemination, women must be ovulating with at least one patent tube. Factors affecting the donor insemination success rates such as age, history must be evaluated as the fertility declines with age. Before donor insemination, menstrual cycles and a mid–luteal phase progesterone assessment must be considered to confirm ovulation. In women with anovulation, appropriate treatment with ovulation agents must be considered
Tubal status should be evaluated either by HSG, SIS or laparoscopy
Recommendations
Therapeutic donor insemination is effective in male infertility associated with obstructive azoospermia, non–obstructive azoospermia, and severe defects in semen quality in couples that do not wish to undergo ICSI
-
Donor insemination should be considered when there is a:
-
»
High–risk of a genetic disorder or infectious disease to the offspring or mother from the father
-
»
Severe rhesus isoimmunization
-
»
ART procedures should not be considered without a spouse’s consent
Single women can undergo donor insemination
Anonymity of the donor should be maintained
Couples considering donor insemination should be offered counseling from someone independent of the treatment unit regarding all the physical and psychological implications of treatment for themselves and potential children.
-
ART banks should provide following information about donor to the recipient couple
-
»
Profile matching should be done
-
»
Colour of skin, eyes, hair, height, and weight
-
»
Record of blood group, major illness including any psychiatric and familial disorders genetic, and hereditary diseases
-
»
Screen for communicable disease including HIV, hepatitis, other sexually transmitted diseases, hypertension, diabetes
-
»
Educational qualification and profession
-
»
Ethnicity
-
»
Women undergoing DI should be tested for thalassemia
The data of every accredited ART clinic must be accessible to an appropriate authority of the ICMR for collation at the national level. An ART bank should not use the sperm from a single donor for multiple instances; there should be a limit in the number of sperm donation (25 times)
No splitting and mixing of the sample are allowed and intrauterine insemination (IUI) should be limited to 6–12 IUI cycles
All ART banks shall cryopreserve sperm donations after quarantine period before being used. After expiry, the sperm should not be supplied to any ART clinic unless the sperm donor is tested for sexually transmitted diseases, infections, or otherwise as may be prescribed
1.6 Welfare of children born after sperm donation
Addresses the risks associated with medically assisted conception and its implications on the mental and physical health of the child
Child will have identical legal rights as a legitimate child born through sexual intercourse
The birth certificate of a child born through ART shall contain the name or names of the parent or parents
The child born to a foreigner by sperm donation will not get Indian citizenship though he or she is born in India
A child may, upon reaching the age of 18, ask for any information, excluding personal identification, relating to the donor. Personal identification of the genetic parent may be released only in cases of life–threatening medical conditions, which require physical testing or samples of the genetic parent or parents. Such personal identification will not be released without the prior informed consent of the genetic parent or parents
2. Egg donation
2.1 Introduction
The recipient will have a biological but not genetic relationship to the child; her partner (if he provided the sperm) will be both biologically and genetically related
2.2 Indications
Premature ovarian failure
Diminished ovarian reserve
Ovarian failure due to iatrogenic causes
Prevent transmission of a genetic disorder
Repeated IVF failures
2.3 Pre-requisites of oocyte donors
The age of donors should be between 23 to 35 years. By restricting the oocyte donors to women <35 years, it decreases the risk of aneuploid offspring
The donor should be a married woman with at least 1 child of ≥3 years
A comprehensive history and physical examination is required
The gamete donor should be screened for the infectious profile, communicable disease (HIV, hepatitis B surface antigen [HbsAg], hepatitis C virus [HCV], and venereal disease research laboratory [VDRL])
A donor should be assessed for basic wellbeing and pre–anesthesia check before considering ovarian stimulation and oocyte isolation
Donors should be screened for HbA2 – to rule out any hemoglobinopathies or to avoid genetic transmission of any inheritable diseases
The psychological and mental wellbeing of the donor must be assured. The donor should be aware of the procedure and counseled about the same and a consent be taken
2.4 Ethics in occyte donation
Donor to be obtained from certified ART banks
Women should not be allowed to donate oocytes more than three times in her lifetime with at least 3 months gap between each donation
Eggs from one donor can be shared between 2 recipients only, provided that at least 7 oocytes are available for each recipient
If married, donor requires her spouse’s consent to donate eggs
2.5 Recipient characteristics and rights
The recipient couple or the commissioning couple should be healthy, mentally sound (man >21 years, and woman >18 years, married)
Either party seeking ART should be entitled to acquire specific information concerning donor of gametes (height, weight, ethnicity, skin color, educational qualifications, and medical history of the donor) provided that the details should be kept confidential
If the recipient mother belongs to an advanced reproductive age, she should be counseled about the increased medical risks related to pregnancy. The counseling process must involve a physician familiar with managing a high–risk pregnancy
The couple should be explained and counseled regarding the variation in the genetic make–up of the offspring resulting from the oocyte of a different parent. Oocyte donation should be strongly discouraged in the presence of obstetrical and neonatal risks (hypertension or diabetes)
Recommendations
The highest possible standards must be followed in storing and handling of gametes and embryos. All unused oocytes must be preserved by ART banks for use on the same recipient, or given for research organizations registered under ART act along with written consent from both partners of the commissioning couple
The gamete of a donor shall be stored for a period of > 5 years, and at expiry, the oocytes can be discarded or donated to research organizations registered under the ART act
The sale, transfer or use of gametes, zygotes, and embryos, or any part thereof or information related directly or indirectly to any party within and outside India is prohibited; except in the case of transfer of own gametes and embryos for personal use according to the rules of the land
-
Legal rights
-
»
Children born through ART shall be deemed a biological child of the commissioning couple, and the child shall be entitled to all the rights, and privileges available to a natural child only from the commissioning couple under any law for the time being in force
-
»
A donor shall relinquish all parental rights over the child or children born from his or her gamete
-
»
Identity of the recipient should not be revealed to the donor
-
»
-
Health issues: As donors can have following risk they should be counselled for the same and an informed consent is essential
-
»
OHSS
-
»
Pain and bleeding due to OR
-
»
Damage to adjacent structures
-
»
Infection
-
»
Long term health consequences
-
»
Psychological problems
-
»
Risk of Ca breast, endometrium, and ovaries
-
»
-
No ART clinic is allowed to:
-
»
Sell human gametes, run an agency, a racket or an organization for selling, purchasing or trading in human gametes
-
»
Import or shall help in acquiring imported gametes in any manner
-
»
Exploit the commissioning couple or the gamete donor in any form
-
»
3. Embryo donation
3.1 Introduction
National guidelines by ICMR suggest that embryo donation in ART should be used in the treatment of infertility only in indicated cases
Left over embroyos cannot be used for embroyo donation
3.2 Embryo donation with frozen embryos
In embryo donation, certain guidelines need to be considered such as anonymity, standards of screening, testing, and counseling of potential gamete donors and recipients
Financial compensation for gamete donors
Financial compensation to be provided to gamete donors through ART banks
Ethical, moral, and legal issues
The use of embryo donation in ART raises ethical, moral, and legal issues as it involves three different sides (donor, recipient, and the rights of the child)
-
The anonymity of the donor
-
»
An gamete donor has the right to remain anonymous under the Indian law. Thus it remains the duty of the ART clinic/bank to maintain the anonymity
-
»
ICMR consent forms for third party reproduction
According to ICMR, the consent forms that need to be signed by the gamete donor, recipients, are mentioned below
-
Consent forms for oocyte donors:
-
»
Along with form K (consent form for the egg donation), ART bank/clinic needs to keep a record of form R1 (contract between the ART bank and oocyte donor summarizing the payment details, risk issues, medico–legal concerns, and also weaving off the parental rights), and M1 (information on egg donor; physical, and pathological findings)
-
»
-
Consent forms for sperm donors:
-
»
Along with form L (consent form for the sperm donor), ART bank/clinic needs to keep a record of form R1 and M
-
»
Recommendations
The decision to proceed with donated gametes is complex, and both donors and recipients benefit from psychological counselling to aid in this decision
Psychological counselling offered by a qualified mental health professional to all couples and may require psychological consultation for those couples in whom there appear to be factors that warrant further evaluation
Before the onset of the treatment, the counselling should involves thorough explaining of, limitations, success rate of the treatment, possible side effects and risk to the women, psychological impact and the child born, possible disruption of the domestic life, cost of the treatment, alternative options etc.
The patient should be given the liberty to take the decision on their own and they should not be forced to opt for any treatment. The patient should give the consent for the treatment in writing before starting the treatment
-
Consent form signing and proper counseling of the treatment:
-
»
The recipient/donor should be explained in detail about the treatment and its medical implications which should be recorded
-
»
Record of all the notarized appropriate consent forms and counseling details should be attached to the patient’s file. Consent from both husband and wife is necessary for any procedures
-
»
-
Compulsory record keeping and track of all the embryos
-
»
According to ICMR, there should be a record of all gamete donors, along with the recipient’s information. The ICMR form N, O(a), O(b), O(c), and P helps in binding all the records and maintaining it easily
-
»
-
All ART clinics shall maintain detailed records, in the following manner:
-
»
As may be prescribed by ICMR of all IUI and ART cycles
-
»
Sperm, oocytes or embryos used
-
»
The manner and technique of their use
-
»
The individual or couple or surrogate mother in respect of whom it was used
-
»
Of all donor oocyte and embryo cycles
-
»
Records should be maintained for at least a period of ten years
-
»
ART clinic should obtain donor gametes from ART banks that have ensured that the donor has been medically tested for sexually transmitted and communicable diseases which may endanger the health of the parents, or any one of them, surrogate or child
The ART bank shall keep a record of all the gametes received, stored and supplied, and details of the use of the gametes of each donor. If not otherwise ordered by a court of competent jurisdiction, all ART banks shall ensure that all information about clients and donors is kept confidential and that information about gamete donation shall not be disclosed to anyone
Using sperm or oocyte donated by a relative or known friend of either of the parties seeking assisted reproductive technology treatment or procedures is prohibited
4. Surrogacy
Age of commissioning couple should be
Female – 23–50 years
Male 26–55 years
4.1 Indications for surrogacy
-
Indications can be both medical and social. In India, medical indications are accepted for surrogacy. These include:
-
»
Congenital absence of uterus (Mayer–Rokitansky–Kuster–Hauser syndrome)
-
»
Surgical removal of the uterus
-
»
Asherman’s syndrome
-
»
Woman with Rh incompatibility
-
»
Malformed uterus
-
»
Significant medical conditions in which carrying a pregnancy is a threat to life
-
»
-
Surrogacy is recommended as a last resort treatment when other modalities have been exhausted
-
»
Repeated failure of IVF treatment
-
»
Recurrent miscarriages
-
»
4.2 Types of surrogacy
4.2.1 Gestational surrogacy:
In India, gestational surrogacy is practiced gestational surrogate is a woman who carries a pregnancy for another couple or woman where pregnancy created by transferring an embryo created with the sperm and egg of the intended parents. It is an arrangement in which a woman agrees to a pregnancy, achieved through ART (IVF), in which neither of the gametes belongs to her or her husband, to carry the pregnancy and hand over the child to the person or persons for whom she is acting as a surrogate
4.2.2 Traditional surrogacy
Surrogate is inseminated with sperm from the male partner of the intended parent and is not allowed
4.3 Selection of a Gestational Carrier is based on
Known/anonymous
Minimum of 21 years of age and <38 years
Preferably in a stable marriage
Delivered a live–born child at term
STI–screening–once when she agrees and once before embryo transfer
Medical and psychological assessment
4.4 ICMR guidelines for surrogacy
Legal contract should be made between intending or commissioning parents by ART banks as the law
-
Agreement regarding
-
»
Fetal reduction
-
»
Therapeutic abortion
-
»
Declaration of parentage of child’s birth obviating the need for adoption proceedings
-
»
4.5 Counselling
4.5.1 Surrogate
Emotional Issues
Impact on family
Financial compensation
Possibility of hospitalization
Possibility of multiple pregnancy
4.5.2 Intended Parents
Maintaining a respectful relationship with surrogate
No. of embryos for transfer
Fetal reduction and abortion
Importance of obtaining legal advice
Success rate and cost
4.6 Legal aspects of surrogacy
Legal guidelines are necessary to safeguard the interests
Surrogate mother should be from same generation and between of 21–35 years
Woman can become a surrogate mother for upto 1 live birth excluding her own
Genetic parents legally bound to accept the custody of the child irrespective of any abnormality, and the refusal to do so shall constitute an offence
Surrogate mother shall not act as an oocyte donor for the couple or individual
If a surrogate is married, the consent of her spouse shall be required
A couple or an individual shall not have the service of more than one surrogate at any given time
A couple shall not have simultaneous transfer of embryos in the woman and in a surrogate
Surrogacy arrangement should provide for financial support for surrogate child in the event of death of the commissioning couple or individual before delivery of the child, or divorce
Surrogacy contract should necessarily take care of life insurance cover for surrogate mother for a total duration of 36 months
One of the intended parents should be a donor as well. In case the intended parent is single, he or she should be a donor
Legislation itself should recognize a surrogate child to be legitimate child of the commissioning parent(s) without there being any need for adoption
The birth certificate of the surrogate child should contain the name(s) of the commissioning parent(s) only
Right to privacy of donor as well as surrogate mother should be protected
Art clinics offering surrogacy services will not import human embryos for offering surrogacy services except for Indian residents who can import their own embroyos
Foreign nationals and overseas citizens of India (OCI) cannot commission surrogacy
Provide surrogacy only to married Indian couples
4.7 Financial transactions
The financial aspect of the process has to be decided upon independently by the woman and the couple and the ART center can in no way become involved in the money that the surrogate mother receives
Summary of recommendations
Infertility in couples with male infertility linked to obstructive azoospermia, non–obstructive azoospermia, and severe defects in semen quality can best be treated with therapeutic donor insemination in couples who do not wish to undergo ICSI
Therapeutic donor insemination is best indicated to avoid the high–risk of transmitting genetic disorders or infections to the offspring or mother from the father. Also during severe rhesus isoimmunization
All ART banks need to quarantine cryo-preserve sperm samples for at least 6 months. After this period it cannot be supplied to any ART clinic unless it is tested for sexually transmitted diseases and infections
Storing and handling of gametes must be carried out with the highest standards. The gametes of the donor can be stored for a period of >5 years; after, that the oocytes can be discarded or donated to research organizations registered under the ART act with consent
The sale, transfer or use of gametes, zygotes, and embryos, or any part thereof or information related directly or indirectly to any party within and outside India is prohibited; except in the case of transfer of own gametes and embryos for personal use with the permission of the National Registry.
Children born through ART must be entitled to all the rights. Children should be deemed a biological child of the commissioning couple
ART clinics or banks are not allowed to sell human gametes, zygotes, and embryos. Also, any ART clinic should not exploit the commissioning couple or the gamete donor in any form
In ART, clinical counseling with a trained and experienced counselor is a compulsion for the couple or anyone involved in the transfer of gametes, zygotes, or embryos
According to ICMR, there should be a record of all gamete donors along with the recipient’s information.
Also, notarized consent from the recipient and the donor should be emphasized.
Only gestational surrogacy is allowed.
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CCR | Infertility in couples with male infertility linked to obstructive azoospermia, non–obstructive azoospermia, and severe defects in semen quality can best be treated with therapeutic donor insemination in couples who do not wish to undergo ICSI | B | - |
| CCR | Therapeutic donor insemination is best indicated to avoid the high–risk of transmitting genetic disorders or infections to the offspring or mother from the father. Also during severe rhesus isoimmunization | C | - |
| CCR | All ART banks need to quarantine cryopreserve sperm samples for at least 6 months. After expiry, this period it cannot be supplied to any ART clinic unless it is tested for sexually transmitted diseases and infections | B | - |
| CCR | Storing and handling of gametes must be carried out with the highest standards. The gametes of the donor can be stored for a period of >5 years; after, that the oocytes can be discarded or donated to research organizations registered under the ART act with consent | B | - |
| CPP | The sale, transfer or use of gametes, zygotes, and embryos, or any part thereof or information related directly or indirectly to any party within and outside India is prohibited; except in the case of transfer of own gametes and embryos for personal use with the permission of the National Registry | - | - |
| CPP | Children born through ART must be entitled to all the rights. Children should be deemed a biological child of the commissioning couple | - | - |
| CPP | ART clinics or banks are not allowed to sell human gametes, zygotes, and embryos. Also, any ART clinic should not exploit the commissioning couple or the gamete donor in any form | - | - |
| CPP | In ART, clinical counselling with a trained and experienced counsellor is a compulsion for the couple or anyone involved in the transfer of gametes, zygotes, or embryos | - | - |
| CPP | According to ICMR, there should be a record of all gamete donors along with the recipient’s information. Also, notarized consent from the recipient and the donor should be emphasized | - | - |
| CPP | Only gestational surrogacy is allowed in India | - | - |
References
Donor insemination - Fertility - NCBI Bookshelf. Available at https://www.ncbi.nlm.nih.gov/books/NBK327777/ Accessed December 31, 2019.
Donor insemination | Information for the public | Fertility problems: assessment and treatment | Guidance | NICE. Available at https://www.nice.org.uk/guidance/cg156/ifp/chapter/Donor-insemination Accessed December 31, 2019.
Mathur R, Swaminathan S. National ethical guidelines for biomedical and health research involving human participants, 2017: A commentary. Indian J Med Ethics. 2018; 3(3):201–4.
National Institute for Clinical Excellence. Fertility: Assessment and Treatment for People with Fertility Problems. NICE Clinical Guidelines, No. 156. National Collaborating Centre for Women’s and Children’s Health (UK). RCOG 2013.
Daar J, Benward J, Collins L, et al. Oocyte or embryo donation to women of advanced reproductive age: An ethics committee opinion. Fertil Steril. 2016;106(5):e3-e7.
Fertility and Sterility. Chapter 8: Donation. American society for reproductive medicine. 2007; 87(4): S28–32.
Gleicher N, Weghofer A, Barad DH. Can egg donor selection be improved? A pilot study. Reprod Biol Endocrinol. 2010;8:76.
Department of health research. The assisted reproductive technology (regulation) bill. 2017. Available at https://dhr.gov.in/sites/default/files/Asssited%20Reproductive%20Technology%20%28Regulation%29%20Bill%2C2017.pdf Accessed January 1, 2020.
Indian Society for Assisted Reproduction. Chapter 8. Website: http://www.isarindia.net/ Accessed January 1, 2020.
Ethical guidelines for biomedical research, Indian council of medical research (ICMR), 2006. Chapter I. Statement of general principles on ethical considerations involving human participants. Published by: Director-General Indian Council of Medical Research. Available at http://www.cns.iisc.ac.in/wordpress/wp-content/uploads/2017/01/ethical_guidelines.pdf Accessed January 1, 2020.
The Supreme Court of India. Civil Original Jurisdiction. Written petition (c) no. 369 of 2008. Baby Manji Yamada petitioner vs. Union of India and Anr. Respondents judgment. 2008. 13 S.C.C. 518. Available at http://oscpcr.nic.in/sites/default/files/Baby_Manji_Yamada_vs_Union_Of_India_%26_Anr_on_29_September,_2008.PDF Accessed January 1, 2020.
The Assisted Reproductive Technologies (Regulation) Bill - 2010 (Draft), Ministry of Health and Family Welfare Govt. Of India, New Delhi and Indian Council of Medical Research New Delhi, available at https://icmr.nic.in/sites/default/files/guidelines/ART%20REGULATION%20Draft%20Bill1.pdf Accessed January 1, 2020.
The National Registry of Assisted Reproductive Technology (ART) Clinics and Banks in India, (NRACBI) 2013, ICMR, National Registry of Assisted Reproductive Technology (ART) Clinics and Banks in India. Available at https://www.icmr.nic.in/sites/default/files/art/Updated_list_Approved_ART_Clinics_30122019.pdf Accessed January 1, 2020.
Kusum S. Legal glitches facing surrogacy agreement in India. Indian Journal of Law and Public Policy. 2015; 1(2):26–57.
Indian Society for Third-Party Reproduction (INSTAR) Key Recommendation. 2013. Available at http://instarorg.blogspot.com/2013_10_01_archive.html Accessed January 1, 2020.
Government of India, Ministry of Health and Family Welfare (Department of Health Research). ART Bill 2014. Available at http://www.prsindia.org/uploads/media/draft/Draft%20Assisted%20Reproductive%20Technology%20(Regulation)%20Bill,%202014.pdf Accessed January 1, 2020.
Prohibition and regulation of surrogacy. India. Surrogacy regulations bill No. 257, 2016. available at http://www.prsindia.org/uploads/media/Surrogacy/Surrogacy%20(Regulation)%20Bill,%202016.pdf Accessed January 2, 2020.
Department of Health Research, Ministry of Health and Family Welfare, Government of India. Commissioning of surrogacy instructions. Circular number V.25011/119/2015/HR. Available at https://www.icmr.nic.in/sites/default/files/art/Document.pdf Accessed January 2, 2020.
Radha Sharma, No complaint received about surrogate exploitation’ Times News Network, Aug 27, 2016, Available at http://timesofindia.indiatimes.com/city/ahmedabad/No-complaint-received-about-surrogate-exploitation/articleshow/53886097.cms Accessed January 3, 2020.
Chapter 19: Fertility Preservation
OVERVIEW
The goal of this update is to provide health care providers and caregivers with recommendations regarding fertility preservation for patients with ocological and non– oncological conditions compromising fertility.
1. Introduction
The cancer burden in India is estimated to be 1.45 million new cases each year, as per the ICMR registry data
The most common female cancers are breast, and cervical cancers, and the most common male cancers are prostate, rectum and colon
Leukemias and lymphomas are the commonest malignancies encountered in childhood
-
Breast cancer which has the highest incidence of all cancers in females has also become frequent in a population younger than 50 years
-
»
In most hospital–based series reports, median age of breast cancer patients is a decade younger than the western series
-
»
At times, breast and ovarian cancer occurs due to inherited genetic mutations (called the hereditary breast and ovarian cancer syndrome) (ICMR).
More than 140,000 cancer patients are diagnosed in their reproductive years; up to the age of 45 years. Childhood cancer too seems to be increasing
2. What is meant by fertility preservation (FP)
Fertility preservation referes to the expansion of the reproductive window through preservation of gamete and gonadal tissue (oocyte, sperm, embryo, ovarian and testicular tissue) for use at a later date. It also includes fertility preserving reproductive surgeries.
3. Indications for fertility preservation
Ferility Preservation is offered to individuals at risk of losing their gametes (sperm/oocytes) prematurely due to disease or its treatment. This technology has been extended to women wanting to delay childbearing, and to overcome the effect of age on ovarian reserve.
3.1 Oncofertility – Patients in reproductive age
Undergoing gonadotoxic chemotherapy in cancer and noncancer conditions
Undergoing RT leading to gonadal damage
3.2 Prevention of age–related decline in fertility in women
3.3 Decline in fertility in autoimmune, genetic disorders, and ovarian pathology.
Autoimmune disease
SLE
Behcet’s disease
Steroid resistant glomerulonephritis
Inflammatory Bowel diseases
-
Rheumatoid arthritis
-
»
Pemphigus vulgaris
-
a.
Genetic disorders and ovarian pathology leading premature ovarian insufficiency
-
b.
Turner mosaic
-
c.
Beta–thalassaemia
-
d.
Galactosaemia
-
e.
Endometriosis
-
f.
Benign ovarian tumours
-
»
3.4 Patients undergoing hemopoitic stem cell transplantation
Autoimmune diseases unresponsive to immunosuppresants
-
Hematological diseases like:
-
»
Sickle cell anaemia
-
»
Thalassaemia major
-
»
Aplastic anaemia
-
»
4. Need for fertility preservation
4.1 Effect of cancer treatment on fertility
Approximately 40%–80% of females and 30%–70% males face possible infertility as a result of cancer treatments such as chemotherapy (CT), radiation (RT), and surgery
In men, CT leads to Leydig cell dysfunction, germ cell failure, and sexual and ejaculatory dysfunction
In women, CT can lead to ovarian failure, premature menopause, and premature ovarian insufficiency (POI) and infertility due to the apoptotic effect on oocytes. RT causes uterine damage by fibrosis and effect on vascularity, increasing the chances of subsequent infertility and adverse pregnancy outcome. These effects are drug and dose dependent
4.2 Effect of age on fertility
Decline in fertility is a result of the decrease in ovarian reserve (OR) or egg numbers that occurs with aging as well as the increased rate of aneuploidies seen in oocytes of women over 35 years
4.3 Relevance of FP
Modern cancer treatment has increased the survival rates in young cancer patients over the last two decades. Unfortunately, the gonadotoxic effects of these treatments can impair the reproductive ability in young cancer survivors
Preservation of gametes allows cancer survivors to fulfil their reproductive desires after completing treatment
Fertility preservation is becoming increasingly important to improve the ‘quality of life’ in cancer survivors
Despite guidelines suggesting that discussion of fertility preservation should be done prior to starting cancer therapies there is a lack of implementation in this area
Cryopreservation of sperm should be offered to all cancer patients in reproductive age regardless of the risk of gonadal failure
Individualize recommendation of fertility preservation in women based on as the urgency of starting cancer treatment, the drug and dosage of CT and age of the patient
5. Multidisciplinary team assessment prior to embarking on FP
-
Involve a multidisciplinary team, which includes
-
»
Oncologist for treatment regimen and oncological risk assessment
-
»
Reproductive medicine specialist to assess feasibility of FP
-
»
Counsellors and geneticist to discuss genetic and psychological issues
-
»
6. Assessment for Feasibility of procedure
-
Assessment of general condition is essential since General Anaesthesia is required for Fertility Preservation procedures in women
-
»
In women, carry out fertility assessment by ovarian reserve testing this includes antral foclicular count by vaginal ultrasound and AMH
-
»
In men,
-
-
Advise for semen analysis (same sample can be cryopreserved)
-
-
Need for assisted ejaculation
-
-
Testicular tissue CP
-
-
-
»
7. Fertility preservation in males–best practice recommendations
Research has shown that people with cancer are interested in discussing fertility preservation options
Patients should be made aware of the options of fertility preservation and future reproduction prior to initiation of treatment
Patients should be counseled on high risk of genetic damage in their sperm even after a single course of chemotherapy
The discussions regarding fertility preservation should be documented in the medical records
Efforts should be made to start and complete fertility preservation promptly, without causing any delay in the treatment of cancer
Cryopreservation of spermatozoa obtained via ejaculation or surgical sperm retrieval is the only established method of fertility preservation in males. If initial sperm count is below WHO standard, then preferably preserve 2–3 samples (to account for post thaw loss). If sperm counts are normal, 1 sample may suffice. However, 1–3 samples recommended
In sexually mature men unable to provide an ejaculate, sperm can be retrieved by epididymal or testicular aspiration or testicular biopsy
When ejaculation is not possible due to medical, social or religious reasons, suggest performing penile vibratory stimulation (PVS), electroejaculation under general anesthesia, or surgical retrival from the epididymis or the testis
In prepubertal boys, cryopreservation of immature testicular tissue (ITT) as cell suspension or whole testicular tissue followed by autografting, xenografting or in vitro spermatogenesis is an option. Consider ITT experimental and only perform under institutional review board–approved protocols
In patients who are minors, parents may consent for surgical sperm retrieval. However, assent of the child should be taken, if possible
New point – Concerns have been raised over the reintroduction of cancerous cells in the ITT after transplantation
Provide clear instructions duly signed by the patient about the disposition of stored sperm or testicular tissue in the event of the patient’s death, unavailability, or other contingency
Suggest discarding the gametes if the child does not survive to adulthood, unless there are written instructions to preserve it
7.1 Indian scenario
Current statistics
In 2018 over 1.1 million new cancer patients in India were registered, of which 0.57 million were males
The deaths due to cancer stood at 0.78 million
7.2 Challenges in management with solutions
The limitations are urgency to commence treatment, limited resources, and perceived high cost and ignorance on part of the medical provider
There is apprehension in the patients mind that fertility preservation will delay cancer treatment and worsen their prognosis
Fertility preservation does not contribute to a significant delay in the initiation of cancer treatment
8. Fertility preservation techniques in females
Options for fertility preservation are oocyte and embryo cryopreservation and ovarian tissue freezing
Ovarian tissue preservation is the only option for prepubescent girls
8.1 Oocyte cryopreservation
Mature oocyte cryopreservation by vitrification is a well–established technique
Similar success rates have been reported between IVF with vitrified warmed oocytes and IVF with fresh oocytes
Congenital abnormalities are reported to be similar in infants born, following oocyte vitrification to pregnancies by regular IVF, and natural conception
Mature oocyte cryopreservation is necessary which requires ovarian stimulation which can delay cancer treatment and is also contraindicated in patients with hormone receptive cancer
Alternative to mature oocyte cryopreservation in such patients is to cryopreserve immature oocytes
In vitro maturation of immature oocytes requires special culture media and expertise
Clinical efficiency of these techniques is yet to be proven and should be attempted under expert guidance only after counseling the patients regarding the survival and outcome
8.2 Embryo cryopreservation
Cryopreservation of cleavage and blastocyst stage embryos is a widely used
Vitrification has enabled the scope of maximizing pregnancy potential even from very few embryos
For women without a male partner, acceptance of donor sperm is the only option
8.3 Ovarian tissue cryopreservation
Technique involves slicing ovarian cortex tissue into thin slices and exposure to cryoprotectants, which negates the need for ovarian stimulation, male partner and can also be performed in prepubertal cancer patients
Successful freezing outcome has been reported both by slow freezing and vitrification
Immature oocytes are aspirated subject to IVM
The efficacy of ovarian tissue freezing is age dependent
8.4 Fertility preservation in gynecological cancers
8.4.1 Breast cancer
Current statistics reveal
Premenopausal women 11% to 15% of individuals are diagnosed annually
CT for breast cancer is damaging to the ovary, since most regimes use alkylating agents
Advise early referral to RM specialists should be advised as there is time available between surgery and CT to do FP
Ovarian tissue preservation for women requiring co–adjuvant CT should be offered keeping in mind the risk of concomitant ovarian cancer in BRCA mutated women
Ovarian stimulation protocols in estrogen-sensitive cancers
-
Ovarian stimulation protocols in estrogen-sensitive cancers
-
»
Tamoxifen, letrozole suppress plasma oestradiol levels
-
»
Avoid delay in stimulation (random start protocol)
-
»
Pregnancy after cancer
Recommended after 2 years because most disease recurrences occur within this time, 5 years for women with HR+ disease
Pregnancy in BC survivors does not increase risk of recurrence and does not decrease survival rates in long term followup studies
8.4.2 Ovarian tumours
Offer fertility sparing surgery may be offered for borderline tumours desiring fertility at a later date
Offer radical trachelectomy may be offered to women with early stage cervical cancer keen on completing their family
Offer unilateral salpingo–oophorectomy (USO) can be offered to women with early stage ovarian malignancy (ovarian epithelial cancer stage I, grade 1) though risk of recurrence is high. A completion surgery should be done as soon as possible
8.4.3 Cervical cancer
Current statistics
Cervical cancer is the second most common cancer in India in women accounting for 22.86% of all cancer cases in women.
Treatment often leads to sexual dysfunction, loss of fertility, and significant dysparunia
Options
Part of uterosacral lig, 1–2 cm of vaginal cuff, pelvis lymph nodes
Eligibility criteria
Lesion size <2.5 cm, no metastasis to regional lymph nodes
8.4.4 Endometrial cancer
Current statistics
Constitutes 7.1% of all new cancer in females
Proper myometrial evaluation by MRI is recommended
Definitive treatment includes hysterectomy with BLSO
Options
For early stage endometrial cancer fertility options can be considered after medical treatment of early stage (stage 1 wave 1)
FP can be offered to women subsequent to progesterone therapy or prior to surgery since definitive treatment needs to be carried out
Letrozole can be added for ovarian stimulation among women with estrogen–sensitive tumors
Summary of recommendations
Males
Semen cryopreservation is recommended for all post pubertal males scheduled for cancer treatment
Semen cryopreservation should be done prior to treatment
If initial sperm count is below WHO standard, then preferably 2–3 samples should be preserved (to account for post-thaw loss). If sperm counts are normal 1 sample may suffice. 1–3 samples recommended
Vibrators – mechanical or electrical can be used to collect the ejaculate
TESA can be offered to post–pubertal males when collection is not possible with any of the above methods
Immature testicular tissue should be offered to pre–pubertal males with the counselling that as yet it is an experimental procedure only
No role for gonadal protection by GnRH analog
Females
Effects of cancer therapy should be discussed with all women who need to undergo cancer therapy, in the reproductive age group
FP counselling should be done prior to start of cancer therapy in all women desirous of future fertility
FP procedures should be carried out prior to start of cancer therapy
FP procedures include oocyte, embryo and ovarian tissue CP
Use GnRH analogues are recommended along with CT to aid in preservation of ovarian reserve. It cannot be used as an effective method of FP
Post–pubertal females should be offered oocyte cryopreservation (CP)
Post–pubertal females who are married or have a partner may be offered embryo freezing though oocyte CP offers autonomy on subsequent use
Ovarian tissue cryopreservation (OTC) is the only procedure that can be offered to pre–pubertal girls.
Oocyte and embryo CP necessitates ovarian stimulation (OS) with gonadotrophins for 9–10 days and an approximate delay of 12–14 days is expected in starting cancer treatment
In ER+ve breast cancers letrozole or tamoxifen can be added to the OS regime
OTC is the only procedure that can be done after initial CT, though it may be less effective
Safety of OS in FP has been established
Pregnancy in cancer survivors is safe
There is no increased risk of birth defects or genetic diseases in infants delivered after previous CT treatment
9. Consent
Detailed consent for procedure should be taken
Consent form should include options for gamete disposition in the event of demise of the patient
10. Limitations and suggestions in the Indian context
10.1 Late diagnosis is a problem in India
Implementation of cancer screening for early detection is suggested
10.2 Poor survival rates due to late diagnosis
Early diagnosis will lead to early treatment
10.3 Cost of procedure – cancer treatment is expensive. Family wants to save all resources for treatment
Insurance should be made available – currently not given by majority of agencies for infertility treatment.
10.4 Reluctance of family to discuss or implement fertility preservation
Fertility preservation and genetic counseling should be made available in oncology centres and oncologists should encourage patients to discuss this aspect
10.5 Information about fertility preservation options
Through public awareness campaigns
10. 6 Many oncologists, gynaecologists and physicians do not have adequate knowledge of fertility preservation .
Enhancing knowledge of oncologists, gynaecologists and general physicians through CME programs
10.7 Availability of good centres performing fertility preservation
Training of RM specialists in counseling and managing such patients and embryologists in fertility preservation procedures
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| Males | |||
| EBR | • Semen cryopreservation is recommended for all post pubertal males scheduled for cancer treatment | A | III |
| EBR | • Semen cryopreservation should be done prior to treatment | A | II |
| EBR | • If initial sperm count is below WHO standard, then preferably 2-3samples should be preserved (to account for post–thaw loss). If sperm counts are normal 1 sample | B | III |
| CPP | may suffice. 1–3 samples recommended | - | - |
| CPP | • Vibrators – mechanical or electrical can be used to collect the ejaculate | - | - |
| CCR | • TESA can be offered to post-pubertal males when collection is not possible with any | C | - |
| CCR | of the above methods | C | - |
| CCR | • Immature testicular tissue should be offered to pre–pubertal males with the counselling that as yet it is an experimental procedure only | C | - |
| EBR | • No role for gonadal protection by GnRH analogue | D | IV |
| Female | |||
| EBR | • Effects of cancer therapy should be discussed with all women who need to undergo cancer therapy, in the reproductive age group | A | V |
| EBR | • FP counselling should be done prior to start of cancer therapy in all women desirous of future fertility | A | V |
| CPP | • FP procedures should be carried out prior to start of cancer therapy | - | - |
| EBR | • FP procedures include oocyte, embryo and ovarian tissue CP. | A | II |
| EBR | • Use GnRH analogues are recommended along with CT to aid in preservation of | B | II |
| EBR | ovarian reserve. It cannot be used as an effective method of FP | B | III |
| EBR | • Post–pubertal females should be offered oocyte cryopreservation (CP) | ||
| • Post–pubertal females who are married or have a partner may be offered embryo freezing though oocyte CP offers autonomy on subsequent use | B | II | |
| EBR | • Ovarian tissue cryopreservation (OTC) is the only procedure that can be offered to pre-pubertal girls | A | II |
| EBR | • Oocyte and embryo CP necessitates ovarian stimulation (OS) with gonadotrophins for 9-10days and an approximate delay of 12–14 days is expected in starting | C | III |
| EBR | cancer treatment. | ||
| CCR | • In ER +ve breast cancers letrozole or tamoxifen can be added to the OS regime | B | II |
| • OTC is the only procedure that can be done after initial CT, though it may be less effective | B | - | |
| EBR | • Safety of OS in FP has been established | B | II |
| EBR | • Pregnancy in cancer survivors is safe | A | III |
| EBR | • There is no increased risk of birth defects or genetic diseases in infants delivered after previous CT treatment | B | IV |
| CPP |
Consent • Detailed consent for procedure should be taken • Consent form should include options for gamete disposition in the event of demise of the patient |
- | - |
References
Sharma, D. C. (2016). Cancer data in India show new patterns. The Lancet Oncology, 17(7), e272.doi:10.1016/s1470-2045(16)30202-9.
Indian Journal of Cancer - 2016
National Centre for Disease Informatics and Research (NCDIR). Indian Council of Medical Research. Annual report 2016-17.
ASCO –Loren et al ASCO Fertility Preservation for Patients With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update J Clin Oncol 31:2500-2510. © 2013 by American Society of Clinical Oncology.
Kim S et al Recommendations for fertility preservation in patients with lymphoma, leukemia, and breast cancer. ISFP Practice Committee. J Assist Reprod Genet (2012) 29:465–468
Maltaris T, Seufert R, Fischl F, et al: The effect of cancer treatment on female fertility and strategies for preserving fertility. Eur J Obstet Gynecol Reprod Biol 130:148-155, 2007.
Stein DM, Victorson DE, Choy JT, Waimey KE, Pearman TP, Smith K, et al. Fertility Preservation Preferences and Perspectives Among Adult Male Survivors of Pediatric Cancer and Their Parents. J Adolesc Young Adult Oncol 2014.
Burns KC, Hoefgen H, Strine A, Dasgupta R. Fertility preservation options in pediatric and adolescent patients with cancer. Cancer 2018. doi:10.1002/cncr.3 1255.
Loren AW, Mangu PB, Beck LN, et al; American Society of Clinical Oncology. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013;31:2500-2510.
Yee S, Fuller-Thomson E, Dwyer C, et al: “Just what the doctor ordered”: Factors associated with oncology patients’ decision to bank sperm. Can Urol Assoc J 6:E174–E178, 2012.
Wyns C, Curaba M, Vanabelle B, van Langendonckt A, Donnez J. Options for fertility preservation in prepubertal boys. Hum Reprod Update 2010. doi:10.1093/humupd/dmp054.
Globocan India. Vol. 468; 2018. p. 1-2. https://www.gco.iarc.fr/today/data/factsheets/populations/356-india-fact-sheets.pdf. [Last accessed on 2018 Nov 04].
Quinn GP, Vadaparampil ST, Malo T, Reinecke J, Bower B, Albrecht T, et al. Oncologists’ use of patient educational materials about cancer and fertility preservation. Psychooncology 2012. doi:10.1002/pon.2022.
Picton HM, Wyns C, Anderson RA, Goossens E, Jahnukainen K, Kliesch S, et al. A European perspective on testicular tissue cryopreservation for fertility preservation in prepubertal and adolescent boys. Hum Reprod 2015. doi:10.1093/humrep/dev190
Katayama KP, Stehlik J, Kuwayama M, et al. High survival rate of vitrified human oocytes results in clinical pregnancy. Fertil Steril. 2003;80:223–224
Kuwayama M, Vajta G, Kato O, Leibo SP. Highly efficient vitrification method for cryopreservation of human oocytes. Reprod Biomed Online. 2005;11:300–308
Cobo A, Diaz C. Clinical application of oocyte vitrification: a systematic review and meta-analysis of randomized controlled trials. Fertil Steril 2011;96:277 –285.
Cobo A, Kuwayama M, Pe´rez S, Ruiz A, Pellicer A, Remohı´ J. Comparison of concomitant outcome achieved with fresh and cryopreserved donor oocytes vitrified by the Cryotop method. Fertil Steril 2008;89:1657 –1664.
Chian R, Huang JYJ, Tan SL, Lucena E, Saa A, Rojas A, Castello´n LAR, Amador MIG, Sarmiento JEM. Obstetric and perinatal outcome in 200 infants conceived from vitrified oocytes. Reprod Biomed Online 2008;16:608 –610
Kim SS, Klemp J, Fabian C. Breast cancer and fertility preservation. Fertil Steril 2011a; 95:1535– 1543.
Toth TL, Baka SG, Veeck LL, Jones HW Jr, Muasher S, Lanzendorf SE. Fertilization and in vitro development of cryopreserved human prophase I oocytes. Fertil Steril 1994; 61:891– 894
Oktay K, Buyuk E, Rodriguez-Wallberg KA, Sahin G. In vitro maturation improves oocyte or embryo cryopreservation outcome in breast cancer patients undergoing ovarian stimulation for fertility preservation. Reprod Biomed Online 2010;20:634–638
Cao YX, Chian RC Fertility preservation with immature and in vitro matured oocytes Semin Reprod Med. 2009 Nov; 27(6):456-64.
Rienzi L, Gracia C, Maggiulli R, LaBarbera AR, Kaser DJ, Ubaldi FM, Vanderpoel S, Racowsky C. Oocyte, embryo and blastocyst cryopreservation in ART: systematic review and meta-analysis comparing slow-freezing versus vitrification to produce evidence for the development of global guidance. Hum Reprod Update. 2017 Mar;23(2):139-155.
Donnez J, Dolmans MM, Demylle D, Jadoul P, Pirard C, Squifflet J, Martinez-Madrid B, van Langendonckt A . Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet. 2004 Oct 16-22; 364(9443):1405-10
Isachenko V, Isachenko E, Kreienberg R, Woriedh M, Weiss J Human ovarian tissue cryopreservation: quality of follicles as a criteria of effectiveness. Reprod Biomed Online. 2010 Apr; 20(4):441-2
Ladanyi C, Mor A, Christianson MS, Dhillon N, Segars JH. Recent advances in the field of ovarian tissue cryopreservation and opportunities for research. J Assist Reprod Genet. 2017 Jun;34(6):709-722.
Prasath EB, Chan ML, Wong WH, Lim CJ, Tharmalingam MD, Hendricks M, et al. First pregnancy and live birth resulting from cryopreserved embryos obtained from in vitro matured oocytes after oophorectomy in an ovarian cancer patient. Hum Reprod. 2014;29:276–278
Future Directions in Oncofertility and Fertility Preservation: A Report from the 2011 Oncofertility Consortium Conference.
Waimey KE, Duncan FE, Su HI, et al. J Adolesc Young Adult Oncol. 2013; 2(1):25-30
Fertility preservation during cancer treatment: clinical guidelines. Cancer Management and Research 2014:6 105–117. Kenny A Rodriguez- Wallberg and-Kutluk Oktay.
Chapter 20: Patient Factors Affecting Fertility Outcomes
OVERVIEW
Infertility is a relatively common condition, greatly affecting couples medically and psychologically. This guideline offers recommendations on the causes of Infertility and female, male and combined factors such as age, obesity, use of lubricants, body weight, occupation, drugs, and smoking affecting fertility outcomes.
1. Introduction
Infertility affects up to 15% couples of reproductive age worldwide
According to World Health Organization (WHO), the overall prevalence of primary infertility in India is between 3.9% to 16.8%
In Indian states, the prevalence of infertility varies from state to state such as 3.7% in Uttar Pradesh, Himachal Pradesh and Maharashtra, to 5% in Andhra Pradesh, and 15% in Kashmir, and the prevalence varies in same region across tribes and caste
Low fertility is becoming more common worldwide, particularly in many urban settings where women are planning their first babies at older age
2. Causes of infertility
Infertility can be caused by a number of underlying conditions including ovulatory disorders, tubal damage, male factors, and uterine or peritoneal problems
It is important to consider clinical assessment, namely history taking and physical examination before the treatment is started
Offer further diagnostic investigations in order to establish if a pathological condition is present in most cases
No cause of fertility problems can be established in approximately 25% of the cases, even after investigations, and it is termed as term ‘unexplained infertility’
Offer a management approach that can be established with an individual or the couple in an attempt to improve their chances of conception after the assessment and investigations are performed
Patient–related factors which affect fertility outcomes can be divided into female, male and combined causes
3. Female factors affecting fertility outcomes
3.1 Tubal factors
The tubal factor is reported to account for 25%–35% of sub–fertility in the western literature, but the prevalence appears to be higher in India due to the higher rates of unrecognized pelvic inflammatory disease (PID) and tuberculosis
PID may be responsible for more than 50% of the causes of tubal factor infertility
Other factors include cornual polyps, chronic salpingitis, endometriosis, salpingitis isthmica nodosa, intrauterine synechiae, and parasite infection
Key points
For women with mild tubal disease, tubal surgery may be more effective than no treatment
For women with proximal tubal obstruction, selective salpingography with tubal catheterisation, or hysteroscopic tubal cannulation, may be treatment option because these treatments improve the chance of pregnancy
Offer salpingectomy preferably by laparoscopy, to women with hydrosalpinges, before IVF treatment because this improves the chance of a live birth
3.2 Uterine Factors
Uterine abnormalities such as adhesions, polyps, submucous leiomyomas, and septae have been found in 10% to 15% of women seeking treatment for fertility problems
Compared with HSG, hysteroscopy is recognised as the ‘gold standard’ test for identifying uterine abnormalities
Congenital uterine anomalies (CUAs) do have reproductive implications. - infertility, recurrent miscarriages, preterm delivery and fetal malpresentation
A causal relationship between leiomyoma and infertility has not been established
In women undergoing assisted reproduction, the presence of submucous, intramural leiomyoma close to the junctional zone and multiple myoma is associated with a reduced chance of clinical pregnancy or delivery
However, the effectiveness of surgical treatment of uterine abnormalities to enhance pregnancy rates is not established
Key points
Offer hysteroscopic adhenolysis to women with amenorrhea or scanty menses who are found to have adhesions
Offer hysteroscopic resection in women with diagnosed uterine septum, submucous myoma, and polyps
3.3 Endometriosis
Endometriosis is a common, chronic disease. Although women may be asymptomatic, most women typically present with pelvic pain, infertility, or an adnexal mass
A reasonable body of evidence demonstrates an association between endometriosis and infertility
Endometriosis can result in adhesions or distorted pelvic anatomy that precludes fertility
The fecundity rate of untreated women with endometriosis is difficult to quantify, given the wide range reported in the literature (2% to 10%)
Key points
Consider female age, duration of infertility, and stage of endometriosis for formulating the management plan
Benefits of laparoscopy for diagnosis in minimal and mild endometriosis in not reported, however, if performed, ablation or excision should be done
Consider expectant management or superovulation and intrauterine insemination (SO/IUI), as first–line therapy in younger women (<37 years) with stage I/II endometriosis–associated infertility
Consider more aggressive treatment, such as SO/IUI or IVF for women more than 37 years of age or older
Conservative surgical therapy with laparoscopy or possible laparotomy followed by ART is beneficial in women with stage III/IV endometriosis-associated infertility
3.4 Ovulatory factors
Ovulatory dysfunction has been identified in approximately 15% of infertile couples and accounts for up to 40% of infertile women
It commonly results in obvious menstrual disturbances
The underlying cause should be sought because specific treatment may be indicated, and some conditions may have other implications and consequences
The most common cause of ovulatory dysfunction include PCOS, obesity, weight gain or loss, strenuous exercise, thyroid dysfunction, and hyperprolactinemia
4. Male factors affecting fertility outcomes
Approximately 1% of men are permanently sterile, with about 20% of men having sperm quality below the threshold compatible with normal fertility
In couples undergoing fertility treatment, male factor may solely be implicable from 20%–50% of cases
Impaired semen parameters alone cannot be used to predict fertility as these men still have a chance of being fertile, except when a man has azoospermia, necrospermia or globozoospermia
Abnormal semen characteristics are usually idiopathic. Idiopathic semen abnormalities occur in about 26% of infertile men
The spermatozoa are mostly dysfunctional and unable to fertilize but a proportion are often functionally normal. Sperm function may also be impaired by anti-sperm antibodies
4.1 Sexual disorder
Erectile dysfunction and anorgasmia may lead to decreased sexual pleasure and decreased frequency of sexual intercourse
Retrograde ejaculation can occur because of laxity of bladder neck muscle due to surgery on prostate, or retroperitoneal lymph node dissection
Depression as a side effect of medication used for prostate enlargement
Nerve damage by medical condition like diabetes, multiple sclerosis, Parkinson disease
Key points
Administer medical management and proper counselling for males with erectile dysfunction
Intercourse of 2–3 times a week is reported to improve chance of conception
Treat ejaculatory failure to restore fertility without the need for invasive methods of sperm retrieval or the use of assisted reproduction procedures. However, further evaluation of different treatment options is needed
4.2 Primary testicular dysfunction
The most common cause of male infertility is idiopathic primary testicular dysfunction with abnormal spermatogenesis
-
Other common causes include:
-
»
Testicular damage due to systemic chemotherapy for cancer
-
»
Klinefelter syndrome
-
»
Genetic mutations
-
»
Testicular cancer
-
»
Pelvic irradiation or surgery
-
»
Trauma
-
»
Cryptorchidism
-
»
Infection
-
»
Autoimmune destruction and drugs
-
»
Key points
Consider ART, as it represents the best or only chance for conception for men with subfertility due to primary testicular defects
Consider giving antibiotics only in cases of proved infection as there is no evidence that men with leukocytes in their semen after giving antibiotics show improve pregnancy rate
4.3 Endocrinopathies that are associated with reduced spermatogenesis
Hypothalamopituitary disorders are the most common cause of male subfertility due to an endocrinopathy
Because normal secretion of both FSH and LH is required for quantitatively and qualitatively normal spermatogenesis, any disease that affects hypothalamic secretion of GnRH or Pituitary secretion of FSH or LH will impair spermatogenesis
Tumors and infiltrative diseases of the hypothalamus, hyperprolactinemia, hemochromatosis, Kallmann syndrome, and idiopathic hypogonadotropic hypogonadism are classic endocrine causes of male subfertility
Hypothyroidism and hyperthyroidism and adrenal disorders also may cause male subfertility via a variety of mechanisms
Key points
Offer gonadotrophin drugs to men with hypogonadotrophic hypogonadism because these drugs are effective in improving fertility
Strong evidence does not exist that men with idiopathic semen abnormality will have any benefits from gonadotrophin antiestrogens, androgens, bromocriptine or kinin–enhancing drugs
5. Combined factors
5.1 Age
Fertility varies among populations and declines with age in both men and women, but the effects of age are much more pronounced in women
Although semen parameters in men also decline detectably after 35 years of age, male fertility does not appear to decrease appreciable before approximately age 50
Key points
Inform the couples that fertility potential decline with increasing age
Females above 35 years of age who has not conceived after 6 months of unprotected sex should consult a doctor for fertility evaluation
Inform men who are concerned about fertility that semen parameters decline with age
5.2 Frequency of intercourse
Although there are evidences which suggest that daily intercourse has some advantage on fecundity, it may unnecessarily lead to stress
Key point
Inform the couple that reproductive efficiency increases when intercourse occur every 1 or 2 days, however, optimum frequency of intercourse should be decided by their own preferences
5.3 Coital position and lubricants
There is no evidence that coital position affects fecundability
Sperm can be found in the cervical canal seconds after ejaculation, regardless of coital position
There is also no convincing evidence to indicate any relationship between specific coital practices and infant gender
Some vaginal lubricants may decrease fertility, based on their observed effects on sperm survival in vitro
Although there is no evidence to indicate that use of any vaginal lubricant decreases fertility, it seems prudent to recommend mineral oil, canola oil, or hydroxyethylcellulose–based lubricants when they are needed
Key points
Inform the patients that different coital position has no effect and fertility rate
Mineral oil, canola oil, or hydroxyethylcellulose– based vaginal lubricants can be used if needed
5.4 Obesity
Obesity impairs reproduction in both women and men, leading to infertility in couples trying to conceive, subsequent complications in pregnancy, and adverse effects on their offspring
The internationally accepted range for BMI is from less than 18 kg/m2 (underweight) to 25 kg/m2 or over (obese)
A BMI of 25 or over was reported to be an independent risk factor for spontaneous abortion in women who were oocyte recipients
An increased risk of miscarriage has been reported in moderately obese women (BMI 25–27.9 kg/m2) undergoing ovulation induction
5.4.1 In females
5.4.1.1 Menstrual cycle abnormalities
Menstrual irregularity is reported to occur more frequently in women above 175% of ideal body weight compared with women below 150% of ideal body weight (54% vs. 19%), respectively
5.4.1.2 Ovulatory dysfunction
Obese women with a BMI >28 kg/m2 are reported to have a relative risk (RR) of anovulatory infertility of 3.1 (95% CI, 2.2–4.4) compared with their lean counterparts with a BM 18–23 kg/m2. (put Indian reference here)
5.4.1.3 Altered ovarian responsiveness and oocyte quality
Obesity alters oocyte morphology, reduces fertilization, and impairs embryo quality in women >37 years of age
Specifically, women with a BMI >23 kg/m2 have smaller oocytes that are less likely to complete development post–fertilization, with embryos arrested before blastulation containing more triglycerides than those forming blastocysts
Moreover, the blastocysts developed from oocytes of high-BMI women are smaller, contain fewer cells, and have higher triglyceride content, lower glucose consumption, and altered amino acid metabolism compared with embryos from normal weight women (BMI)
5.4.1.4 Altered endometrial function
Obesity also appears to alter endometrial receptivity during IVF with a BMI more than 25
5.4.2 Obesity in males
Not all obese men have infertility, but those who do can have reduced semen quality, impaired erectile function, and other physical problems, including sleep apnea, and increased scrotal temperatures
Obesity in men is associated with an increased incidence of oligozoospermia and asthenozoospermia in some, but not all.
Moreover, increased abdominal adiposity in men of subfertile couples has been associated with reduced sperm count, concentration, and motility
-
An observational study reported an inverse relationship between BMI and the total number of normal–motile sperm cells
-
»
There was a significant reduced number of normal–motile sperm cells in men who were overweight (BMI 24–28) and obese (BMI greater than 28) when compared with men of normal weight
-
»
A higher incidence of sperm DNA fragmentation has also been observed in men with a BMI of over
-
»
Key Points
Inform women with BMI >25 that they may take longer to conceive
In women with high BMI >27, losing weight will improve ovulation and hence chances of conception
Advise women that exercise and dietary adjustment are effective in achieving pregnancy
Obese men are more likely to have reduced fertility and sexual dysfunction
5.5 Low bodyweight
Low bodyweight in female is a recognized cause of hypo–estrogenic amenorrhoea. Women having extremely low amounts of body fat have more chances of ovarian dysfunction and infertility
In women, weight loss of over 15% of ideal body weight is associated with menstrual dysfunction and secondary amenorrhoea when over 30% of body fat is lost
Restoration of body weight may help to resume ovulation and restore fertility
Men who are underweight are also at risk of infertility
Men who are underweight tend to have lower sperm concentrations than those who are at a normal BMI
As most of literature focuses on impact of obesity more research is needed to established role of low body weight on male fertility
Key points
Women who have a BMI of less than 18, and who have irregular menstruation, or are not menstruating should be advised that increasing body weight is likely to improve their chance of conception
5.6 Increased temperature
Increased scrotal temperature is related to reduction in semen quality
Important determinants of testicular temperature such as a sedentary work position and clothing have been associated with abnormal semen quality
There are some evidences stating altered semen parameters in men wearing tight underwear
Effect of impaired sperm quality on pregnancy outcome is not being established
Literature review concluded that sauna bathing does not decrease female fertility and is safe during uncomplicated pregnancy
In normal men, recommendations for behavioural modifications aimed at controlling or decreasing exposure of the testicles to heat is recommended
Key points
Inform men that there exists an association between elevated scrotal temperature and reduced semen quality
Inform women that sauna bathing does not decrease female fertility
5.7 Occupation and endocrine disruptors
Endocrine dysruptors like bisphenol A, pesticides, heavy metals, radiation and electromagnetic waves have an effect on male and female fertility
Key point
A specific enquiry about occupation and exposure to endocrine dysruptors should be made.
5.8 Drugs
5.8.1 Illicit drugs
Use of illicit drugs appears to have a negative impact on fertility, though more indepth research in this area is required to make a clear link
-
Marijuana is one of the most commonly used drugs around the world
-
»
It acts both centrally and peripherally. In males it is reported to reduce testosterone levels, spermatogenesis sperm motility, sperm capacitation, and acrosome reaction
-
»
Females using marijuana have increased risk of primary infertility
-
»
Similarly Cocaine and opiates show negative impact on male and female fertility potential
5.8.2 Prescription and over-the-counter drugs (Table 1)
Table 1.
Over-the-Counter Medications impacting spermatogenesis
| Drug category | Generic name of drug | Effect on spermatogenesis |
|---|---|---|
| Analgesic | Methadone hydrochloride | Decrease in sperm motility and seminal vesicle secretions, abnormal sperm morphology |
| Pregabalin | Epididymitis | |
| Anti-arrhythmic agent | Amiodarone | Inhibit spermatogenesis and increase sperm head abnormalities |
| Anti-bacterial agents | Nitrofurantoin | Spermatogenic arrest/decreased sperm count |
| Anti-convulsants | Lamotrigine | Epididymitis(rare) |
| Anti-depressants | Clomipramine | Reversible suppression of spermatogenesis |
| Paroxetine | Decreased sperm quality | |
| Fluoxamine maleate | Haematospermia | |
| Antihypertensive agent | Nifedipine | Reversible reduction in ability to fertilize ova |
| Anti-Inflammatory agents | Colchicine | Azoospermia or oligospermia |
| Cortisone acetate | Changes in motility and number of spermatozoa | |
| Dexamethasone | Changes in motility and number of spermatozoa | |
| Prednisone | Changes in motility and number of spermatozoa | |
| Sulfasalazine | Reversible oligospermia | |
| Anti-viral agents | Ganciclovir | Testicular hypertrophy and aspermatogenesis |
| Hormones | Methyl testosterone | Oligozoospermia and suppressed spermatogenesis |
| Testosterone enanthate/Testosterone undecanoate | Suppressed spermatogenesis/oligozospermia, Testosterone undecanoate may also cause spermatocele formation | |
| Treatment of peptic ulcer and gastroesophageal reflux disease (GERD) | Cimetidine Has anti-androgenic action | Reversible impotence Gynecomastia |
| PDE-5 Inhibitor | Tadalafil | Decreased sperm concentration |
| Chemotherapeutic agents | Methotrexate given for rheumatoid arthritis | Decreased sperm concentration |
| Other anticancer drugs | Decreased sperm concentration |
| Over-the-Counter Medications impacting female fertility | |
|---|---|
| Drug | Effect on female fertility |
| NSAID’s | Effect ovulation |
| Natural or herbal remedies | Contain substances that act like estrogen or progesterone |
| Over-the-Counter Medications to be avoided in Pregnancy | ||
|---|---|---|
| Drug Category | Drugs | Effects |
| Anti-diarrheal | Bismuth Subsalicylate | Salicylate absorption |
| Loperamide | Fetal cardiac malformations | |
| Atropine/diphenoxylate | Teratogenic in animal studies. Insufficient evidence in humans. | |
| Decongestants and expectorants | Chlorpheniramine | |
| Pseudoephedrine hydrochloride | Vasoconstriction of uterine arteries and decreased blood flow to the fetus. | |
| Guaifenesin | Neural tube defects | |
| Diphenhydramine | Oxytocin like effects in high doses | |
| Analgesics | Aspirin | Neonatal heamorrhage, low birth weight, prolonged gestation and labor. Low dose aspirin is found to be safe. |
| Ibuprofen | Avoid in third trimester | |
| Naproxen | Avoid in third trimester | |
| Indomethacin | Oligohydramnios, premature closure of ductus arteriosus, Fetal nephrotoxicity and periventricular hemorrhage | |
| Diclofenac | Premature closure of ductus arteriosus | |
A number of prescribed drugs and over–the–counter drugs impair fertility and sexual function. There use, benefits and adverse effects should be judged cautiously
Anti–inflammatory, immunosuppressive, anti–depressants, tranquilizer or asthma medications lead to increased anovulation in females
Medication such as cimetidine and sulfasalazine and long term daily use of some antibiotics and androgen injections can affect semen quality and cause oligozoospermia
The effect is generally reversible after three months following withdrawal of medication
Use of beta–blockers and psychotropic drugs may lead to impotence,
Chemotherapy treatment can induce azoospermia and reduce ovarian reserve
Key point
A number of prescriptions, over–the–counter and recreational drugs interfere with male and female fertility, and therefore a specific enquiry about these should be made to people who are concerned about their fertility and appropriate advice should be offered
5.9 Diet and lifestyle
5.9.1 Diet
Fertility rates clearly are decreased in women who are either very thin or obese, but data regarding the effects of normal variations in diet on fertility in ovulatory women are few
Whereas a healthy lifestyle may help to improve fertility for women with ovulatory dysfunction, there is little evidence that dietary variations such as vegetarian diets, low–fat diets, high–protein diet, vitamin– enriched diets, antioxidants, or herbal remedies improve fertility or affect infant gender
Advice women attempting to conceive to take a folic acid supplement (at least 400 mg daily) to reduce the risk for neural tube defects
Key Point
There is little evidence that diet variation affects fertility, however, healthy diet and life style does improved fertility in thin or obese men and women
5.9.2 Smoking
Female smoking decreases fecundity by accelerating ovarian follicular depletion
Active smoking by either partner had adverse effects, and the impact of passive cigarette smoke exposure alone was only slightly smaller than for active smoking by either partner
Key points
There is good evidence that semen parameters and results of sperm function tests are poorer in smokers than in non-smokers and the effects are dose dependent
There is good evidence that smokers require nearly twice the number of IVF attempts to conceive as nonsmokers
The adverse effects of side stream and passive smoking are now established, and there is good evidence that nonsmokers with excessive exposure to tobacco smoke may have reproductive consequences as great as those observed in smokers
5.6.3 Alcohol
The effect of alcohol on female fertility has not been clearly established
In men, alcohol consumption has no adverse effect on semen parameters. Three to four units per day for men is unlikely to affect their semen quality
Key Points
Avoid higher levels of alcohol consumption (>2 drinks/day, with 1 drink >10 g of ethanol) when attempting pregnancy, but there is limited evidence to indicate that more moderate alcohol consumption adversely affects fertility
Three to four units per day alcohol consumption for men is unlikely to affect their semen quality but excessive intake could be detrimental to sperm parameter
5.6.4 Caffeine
Caffeine is present in coffee, tea, colas, and chocolate. The association between caffeine and female infertility is inconsistent
High levels of caffeine consumption (500 mg; >5 cups of coffee/day or its equivalent) have been associated with decreased fertility
Key points
Moderate caffeine consumption (1 to 2 cups of coffee per day or its equivalent) before or during pregnancy has no apparent adverse effects on fertility or pregnancy outcomes
In men caffeine consumption has no effect on semen parameters
5.6.5 Stress
Stress has become prominent part of our society be it physical, social or psychological, there is a complex relationship between stress and fertility problems
Stress such as job, life events and even social strain have shown significant impact on sperm motility, count and morphology
Stress and depression leads to decreased libido, affects couple’s relationship leading to delayed conception
Physical and psychological stress has shown to influence female fertility
Psychological stress such as anxiety or depression can be reduced with counselling and holistic management
Key Points
When couples have fertility problems, inform both partners that stress in the male and/or female partner can affect the couple’s relationship and are likely to reduce libido and frequency of intercourse which can contribute to the fertility problems
Offer counselling to people who experience fertility problems because fertility problems themselves, and the investigations and treatment of fertility problems, may cause psychological stress.
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CPP | Lifestyle factors, including age when starting a family, nutrition, weight management, exercise, psychological stress, cigarette smoking, recreational and prescription drugs use, alcohol and caffeine consumption, preventative care, and other behaviours are modifiable and may impact fertility | - | - |
| EBR | Exposure to occupational and environmental disruptors is associated with reduced fertility in both males and females | C | III |
| CPP | Attempting pregnancy before the age of 30 for women and before 35 for men may provide the highest chances of success | - | - |
| CPP | Men and women who are underweight or overweight are also at risk for negative side effects, including changes in hormone levels that heavily influence their fertility | - | - |
| CPP | Overweight and obese women are at increased risk of infertility and their outcome after ART is not very optimistic. | - | - |
| CPP | Recreational and prescription substances also appear to have significant impact on fertility. Though clear links are yet to be determined, there are negative trends, including decreased semen parameters or decreased ovarian re–serve, associated with smoking and fertility | - | - |
| CPP | Caffeine appears to have a negative effect on fertility, additional research is needed to elucidate if there is a definitive relationship | - | - |
| CPP | Decreasing or ceasing alcohol consumption may provide a better chance of achieving a viable pregnancy for the couple | - | - |
| CPP | Identifying, eliminating, or minimizing even one factor of the many environmental exposures may have significant positive effects on fertility for both men and women | - | - |
| EBR | Thyroid disorders in both the male and female are associated with reduced fertility and in the female may affect the progress of pregnancy as well | B | II |
| CCR | Sexual dysfunction and frequency of coitus may also influence the occurrence of pregnancy | C | |
| EBR | Method of fertilisation, age, reactive oxygen species, sperm quality parameters and DNA fragmentation may influence ART outcome | B | II |
| EBR | ICSI for male factor infertility had a worse outcome for clinical pregnancy rate and trend for lower LBR than non–male factor infertility cycles and non–ICSI male factor infertility cycles | B | II |
| EBR | The ICSI cycles with ejaculated and aspirated sperm for male factor infertility had better pregnancy outcomes than non-male factor infertility cycles | B | II |
| EBR | After adjustments for female age, male and female race/ethnicity, day of ET, number of embryos transferred, and with non–ICSI cycles as the reference group, models showed ICSI to have a lower clinical pregnancy rate, but not a lower LB rate | B | III |
| EBR | Men suffering from NOA undergoing TESE are to be counselled that not only are the sperm recovery rates limited but also the fertilization, implantation and conception rates are decreased compared to men with normal spermatogenesis | B | II |
| EBR | Diminished ovarian reserve was likely associated with decreased chance of clinical pregnancy | A | II |
| EBR | The impact of endometriosis on assisted reproductive technology (ART) outcomes is variable Mild endometriosis ie, stage I/II disease does not appear to negatively impact ART outcomes whereas stage III/IV disease appears to negatively impacts ART outcomes | A | II |
| CPP | Severe endometriosis was associated with lower oocyte retrieval, implantation, and pregnancy rates in women undergoing IVF as compared with women with mild endometriosis | - | - |
| CPP | Women with endometriomas, often have lower ovarian reserve and produce fewer oocytes, which reduces ART success | - | - |
| EBR | In infertile women with endometrioma larger than 3 cm there is no evidence that cystectomy prior to treatment with ART to improves PRs | A | II |
| EBR | Endometriosis are associated with follicle number and oocytes retrieved but not on embryo quality or pregnancy outcomes | A | II |
| EBR | Presence of hydrosalpinx has a negative effect on ART outcome, salpingectomy or disconnection of tube at the cornua improves the outcome | A | I |
| EBR | Intramural myomas >5 cm and those close to the junctional zone have a negative impact on ART outcome and therefore should be removed | B | II |
| EBR | Uterine polyps and sub–mucous myoma can influence the ART outcome and therefore hysteroscopic surgery for polyps, sub–mucus myoma improves the outcome | A | I |
| EBR | IUA decrease the PRs significantly and adhesiolysis may improve the outcome | B | III |
| EBR | Congenital malformation of the uterus may influence the occurrence of infertility and increase the incidence of miscarriage, pre–term delivery, and fetal malformation | B | III |
| EBR | Septal resection improves fecundity significantly with increase in term delivery and decrease in spontaneous abortion rate improves the outcome | B | II |
| EBR | “T” shaped uterus may impact the success rate of ART, but lateral metroplasty may not improve the outcome | B | III |
| EBR | PCOS with obesityis associated with reduction in fertility which is multifactorial • Reduced fertilization, impaired embryo quality and blastocyst formation (higher intracellular triglycerides) • Altered Endometrial responsiveness • BMI is inversely related to intrafollicular HCG concentrations, embryo quality and IVF outcome |
B | II |
| EBR | Abnormalities in circulating hormones in PCOS women (high androgens, LH and insulin) is associated is associated with reduced pregnancy rates, and high miscarriage rate | B | II |
| EBR | There was no evidence of a significant difference in CPR, LBR or miscarriage rate in women with CC–resistant PCOS undergoing LOD compared to other medical treatments and ART | B | II |
References
Tayebi N, Ardakani SMY. Incidence and prevalence of the sexual dysfunctions in infertile women. European Journal of General Medicine. 2009;6(2):74-77.
Patil M. Assessing Tubal damage J Hum Reprod Sci. 2009; 2(1): 2–11.doi: 10.4103/0974- 1208.51335.
Reichman DE, Laufer MR. Congenital uterine anomalies affecting reproduction. Best Pract Res Clin Obstet Gynaecol 2010; 24:193–208.
Chan YY, Jayaprakasan K, Tan A, et al. Reproductive outcomes in women with congenital uterine anomalies: A systematic review. Ultrasound Obstet Gynecol. 2011;38:371–82.
Hughes EG, Fedorkow DM, Collins JA. A quantitative overview of controlled trials in endometriosis-associated infertility. Fertil Steril. 1993; 59:963–70.
Patel AS, Leong JY, Ramasamy R. Prediction of male infertility by the World Health Organization laboratory manual for assessment of semen analysis: A systematic review. Arab J Urol. 2017; 16(1):96-102.
Farley TMM, Belsey FH. The prevalence and aetiology of infertility. Proceedings of the African Population Conference, 7–12 November 1988, Dakar, Senegal. Liege: International Union for the Scientific Study of Population; 1988. 1, 2.1.15–30.
Anawalt BD. Approach to Male Infertility and Induction of Spermatogenesis. J Clin Endocrinol Metab. 2013; 98(9): 3532–3542.
Dunson DB, Baird DD, Colombo B. Increased infertility with age in menand women. Am J Obstet Gynecol 2004; 103:51–6.
Menken J, Trussell J, Larsen U. Age and infertility. Science 1986; 233:1389–94.
Wilcox AJ, Weinberg CR, Baird DD. Timing of sexual intercourse in relation to ovulation— effects on the probability of conception, survival of the preg-nancy, and sex of the baby. New Engl J Med 1995 333:1517–21.
Settlage DS, Motoshima M, Tredway DR. Sperm transport from the external cervical as to the fallopian tubes in women: a time and quantitation study. Fertil Steril 1973; 24:655–61.
Steiner AZ, Long DL, Tanner C, Herring AH. Effect of vaginal lubricants on natural fertility. Obstet Gynecol 2012; 120:44–51.
World Health Organization. Physical Status: The Use and Interpretation of Anthropometry. World Health Organization Technical Report Series 854. Geneva: World Health Organization; 1995.
Bellver J, Rossal LP, Bosch E, et al. Obesity and the risk of spontaneous abortion after oocyte donation. Fertil Steril 2003; 79:1136–40.
Hamilton-Fairley D, Kiddy D, Watson H, et al. Association of moderate obesity with a poor pregnancy outcome in women with polycystic ovary syndrome treated with low dose gonadotrophin. Br J Obstet Gynaecol. 1992; 99:128–31.
Castillo-Martinez L, Lopez-Alvarenga JC, Villa AR, et al. Menstrual cycle length disorders in 18- to 40-y-old obese women. Nutrition. 2003; 19:317–20.
Rich-Edwards JW, Goldman MB, Willett WC, et al. Adolescent body mass index and infertility caused by ovulatory disorder. Am J Obstet Gynecol. 1994;171:171–7
.Depalo R, Garruti G, Totaro I, et al. Oocyte morphological abnormalities in overweight women undergoing in vitro fertilization cycles. Gynecol Endocrinol 2011; 27:880–4.
Zhang D, Zhu Y, Gao H, et al. Overweight and obesity negatively affect the outcomes of ovarian stimulation and in vitro fertilisation: A cohort study of 2628 Chinese women. Gynecol Endocrinol. 2010; 26:325–32.
Orvieto R, Meltcer S, Nahum R, et al. The influence of body mass index on in vitro fertilization outcome. Int J Gynaecol Obstet 2009; 104:53–5.
Fedorcsak P, Dale PO, Storeng R, et al. Impact of overweight and underweight on assisted reproduction treatment. Hum Reprod 2004; 19:2523–8.
Metwally M, Cutting R, Tipton A, et al. Effect of increased body mass index on oocyte and embryo quality in IVF patients. Reprod Biomed Online 2007; 15:532–8.
Leary C, Leese HJ, Sturmey RG. Human embryos from overweight and obese women display phenotypic and metabolic abnormalities. Hum Reprod 2015; 30:122–32.
Deugarte D, Deugarte C, Sahakian V. Surrogate obesity negatively impacts pregnancy rates in third-party reproduction. Fertil Steril. 2010;93: 1008–10.
Cabler S, Agarwal A, Flint M, et al. Obesity: Modern man’s fertility nemesis. Asian J Androl 2010; 12:480–9.
Umul M, Kose SA, Bilen E, et al. Effect of € increasing paternal body mass index on pregnancy and live birth rates in couples undergoing intracytoplasmic sperm injection. Andrologia 2015; 47:360–4.
Thomsen L, Humaidan P, Bungum L, et al. The impact of male overweight on semen quality and outcome of assisted reproduction. Asian J Androl 2014;16:1–6.
Kort HI, Massey JB, Elsner CW, et al. Men with high body mass index values present with lower numbers of normal-motile sperm cells. Abstract no. P-355. Fertil Steril 2003; 80 Suppl 3;S238.
Wentz AC. Body weight and amenorrhea. Obstet Gynecol 1980; 56:482–7.
Knuth UA, Hull MG, Jacobs HS. Amenorrhoea and loss of weight. Br J Obstet Gynaecol. 1977; 84:801–7.
Chavarro JE, Toth TL, Wright DL, et al. Body mass index in relation to semen quality, sperm DNA integrity, and serum reproductive hormone levels among men attending an infertility clinic. Fertil Steril. 2010; 93:2222–22231.
Mieusset R, Bujan L. Testicular heating and its possible contributions to male infertility: a review. Int J Androl 1995; 18:169–84.
Thonneau P, Bujan L, Multigner L, et al. Occupational heat exposure and male fertility: A review. Hum Reprod 1998; 13:2122–5.
Tiemessen CH, Evers JL, Bots RS. Tight-fitting underwear and sperm quality. Lancet 1996; 347:1844–5.
Hannuksela ML, Ellahham S. Benefits and risks of sauna bathing. Am J Med 2001; 110:118–26.
Povey AC, Clyma JA, McNamee R, et al. Participating Centres of Chaps-uk. Modifiable and non-modifiable risk fac-tors for poor semen quality: a case- referent study. Hum Reprod 2012; 27: 2799–806.
Jung A, Schuppe HC. Influence of genital heat stress on semen quality in hu- mans. Andrologia 2007; 39:203–15.
Hruska K, Furth P, Seifer D, et al. Environmental factors in infertility. Clin Obstet Gynecol 2000; 43:821–9.
Swan SH. Semen quality in fertile US men in relation to geographical area and pesticide exposure. Int J Androl. 2006; 29:62, 8. discussion 105–108.
Sharma R, Biedenharn KR, Fedor JM, et al. Lifestyle factors and reproductive health: Taking control of your fertility. Reprod Biol Endocrinol. 2013; 11:66.
Hruska K, Furth P, Seifer D, et al. Environmental factors in infer-tility. Clin Obstet Gynecol. 2000; 43:821–9.
Mueller BA, Daling JR, Weiss NS, et al. Recreational drug use and the risk of primary infertility. Epidemiology. 1990; 1:195–200.
Janssen NM, Genta MS. The effects of immunosuppressive and anti-inflammatory medications on fertility, pregnancy, and lactation. Arch Intern Med. 2000; 160:610–9.
Fody EP, Walker EM. Effects of drugs on the male and female reproductive systems. Ann Clin Lab Sci. 1985; 15:451–8.
Beeley L. Drug-induced sexual dysfunction and infertility. Adverse Drug React Acute Poisoning Rev. 1984; 3:23–42.
Mutsaerts MA, Groen H, Huiting HG, et al. The influence of maternal and paternal factors on time to pregnancy–a dutch population-based birth-cohort study: The GECKO drenthe study. Hum Reprod. 2012; 27:583–593.
Hull MG, North K, Taylor H, et al. Delayed conception and active and passive smoking: The Avon Longitudinal Study of Pregnancy and Childhood Study Team. Fertil Steril. 2000; 74:725–33.
Smoking and infertility: A committee opinion, The Practice Committee of the American Society for Reproductive Medicine American Society for Reproductive Medicine, Birmingham, Alabama, (Fertil Steril 2012;98: 1400–6. 2012 by American Society for Reproductive Medicine)
Eggert J, Theobald H, Engfeldt P. Effects of alcohol consumption of female fertility during an 18-year period. Fertil Steril. 2004; 81:379–83.
Bolumar F, Olsen J, Rebagliato M, et al. Caffeine intake and delayed conception: a European multicenter study on infertility and subfecundity. Am J Epidemiol. 1997; 145(4):324-34.
Brkovich AM, Fisher WA. Psychological distress and infertility: forty years of research. JPsychosom Obstet Gynaecol. 1998; 19:218–28.
Gollenberg AL, Liu F, Brazil C, et al. Semen quality in fertile men in relation to psychosocial stress. Fertil Steril. 2010; 93:1104–1111.
Li Y, Lin H, Li Y, Cao J. Association between socio-psycho-behavioral factors and male semen quality: Systematic review and meta-analyses. Fertil Steril. 2011; 95:116–123.
Mutsaerts MA, Groen H, Huiting HG, et al. The influence of maternal and paternal factors on time to pregnancy–a dutch population-based birth-cohort study: the GECKO drenthe study. Hum Reprod. 2012; 27:583–593.
Peterson BD, Newton CR, Feingold T. Anxiety and sexual stress in men and women undergoing infertility treatment. Fertil Steril. 2007; 88:911–914.
Chapter 21: Long Term Safety
OVERVIEW
This guideline offers recommendations to highlight the long–term safety of assisted reproduction treatments in women with infertility and their children. It is aimed primarily at women aged 21 years or older presenting to healthcare professionals with infertility problems. The guideline also concentrates on the information regarding understanding the long–term impact of these treatments, which have been linked with several potential complications affecting both the mother and the child. The field of this study poses a constant challenge for the scientific community. We have to evaluate the patient to understand various other medical risk.
1. Introduction
The treatment of infertility for decades has seen the development of revolutionary new assisted reproductive technologies (ART)
The in vitro fertilization (IVF) was first achieved in 1978 with the birth of baby Louise Brown
Later on, microassisted reproduction using techniques such as intracytoplasmic sperm injection (ICSI) and the development of preimplantation genetic diagnosis (PGD) has emerged. Despite greater inventions, questions regarding the safety of ART persist
Understanding the long–term impact of these treatments, which have been linked with several potential complications affecting the mother and the child, poses a constant challenge for the scientific community
The treatment of infertility for decades has as seen the development of revolutionary new assisted reproductive technologies (ART)
There is a paucity of data in the literature and no adequate prospective randomized controlled trials (RCTs) of sufficient power available to assess the efficacy and safety of the various forms of assisted reproduction
There is a need for assessment of the safety of various forms of assisted reproduction technology, especially long–term safety
The definition of success in IVF started shifting from pregnancy rate per cycle towards achieving healthy singleton child per started course of treatment
For achieving this aim the first change had to be in the stimulation protocols with the aim of less pain or stress, less cost and complications, and obtaining a good oocyte/embryo/implantation rate
Further progression of technology aimed at minimizing complication rates yet maintaining optimal pregnancy rates
2. Long–term risks of ovulation induction and ovarian stimulation in mother
There is no evidence of transmission of prion disease by any presently used gonadotropin
-
Gynecological cancer: Carcinoma in women undergoing ovulation induction
-
»
It is not easy to be determined due to many confounding factors. These include the facts that–
-
»
Infertility
-
»
Age
-
»
Drugs for ovulation induction (either alone or in combination)
-
»
Ovulation induction does not increases the risk of gynecological cancer. Moreover, the risk of ovarian cancer is not increased with ovulation induction, even though few concerns are raised due to borderline ovarian tumors
-
»
More information is required about the relationship between ovulation induction and breast cancer before firm conclusions. Also, a higher risk of uterine cancer is related to infertility status rather than to the ovulation induction
-
»
-
Borderline ovarian tumor
-
»
There is no strong link between the use of fertility drugs and risk for borderline ovarian tumours
-
»
One cohort study concluded that ovarian stimulation for IVF may increase the risk of ovarian malignancies, especially borderline ovarian tumours
-
»
Infertility drugs could be used safely in patients who experience infertility after conservative management of an early–stage BOT
-
»
In patients with advanced stage BOT, the risk of lethal recurrence is increased
-
»
-
IVF and ovarian cancer
-
»
Collective data regarding the risk of developing cancer from use of fertility medications are reassuring
-
»
No association between fertility drug use and risk of ovarian cancer
-
»
Effects of long–term fertility drug use and the effects of fertility treatment on women who have a BRCA1 or BRCA2 gene mutation is currently scarce
-
»
-
IVF and breast cancer
-
»
There was no significant association between IVF and breast cancer in the infertility treated group
-
»
2.1 Recommendations for ovulation induction or ovarian stimulation
Provide up–to–date information about the long–term health outcomes
No direct association was found among IVF treatment and invasive cancer
No association was found in the short–to medium–term among IVF and adverse outcomes (including cancer) in children born from ovulation induction
Information regarding long–term health outcomes in women and children is still awaited
The use of ovulation induction or ovarian stimulation agents should be limited to the lowest effective dose and duration
Women subjected to IVF should be informed that the absolute risks of long–term adverse outcomes of IVF treatment, with or without intracytoplasmic sperm injection (ICSI), are low, a small increase in the ovarian stimulation for IVF may increase the risk of ovarian malignancies, especially borderline ovarian tumours
More large cohort studies are needed to confirm this findings and to examine the effect of IVF treatment characteristics
3. Long–term outcomes in children born after assisted reproduction
-
The outcomes that were included in various research publications were
-
»
Malformations in children
-
»
Chromosomal abnormalities in children
-
»
Childhood tumors growth disturbances
-
»
Neurological development disturbance
-
»
Autism spectrum disorders
-
»
Transmission of subfertility to male offspring
-
»
3.1 Congenital abnormality and major birth defects
NTD, esophageal atresia, omphalocele, hypospadias, and cardiac septal defects.
The incidence was 8% with a two–fold increased risk. This was due to reasons such as increased maternal age during IVF which involves exposure of the embryo to the mechanical, thermal and chemical alterations, ICSI, cryopreservation
Chromosomal anomalies: Slight increase in ICSI predominantly sex chromosomes
Imprinting disorders such as Beckwith–Wiedemann syndrome and Angelman syndrome
3.1.1 Congenital anomaly
ART was associated with 1.5 times increased risk when compared with spontaneously conceived pregnancy. The adjusted odds ratio (OR) for IVF was 1.07 and for ICSI 1.57. There were no differences among ICSI using ejaculated, testicular and epididymal sperm. Also, the ICSI Fresh embryo transfer has a greater risk than frozen transfers
The vast majority of births resulting from ART were free of birth defects, treatment with the use of ART has higher risk of birth defects compared with spontaneous conception which is attributed to sub fertility
3.1.2 ICSI and genetic abnormalities
“Y” chromosome micro deletions observed in 3%–15% of men with severe oligospermia may be transmitted to ICSI conceived male off springs
More boys conceived by ICSI were found to have undescended testes required urogenital surgery
3.1.3 Imprinting disorders
Genetic imprinting is rare with every 1 from 12000 births due to ART. The genetic imprinting disorders are Prader–Willi syndrome, Angelman syndrome, and Beckwith–Wiedeman syndrome (BWS)
Infants and children obtained through IVF/ICSI are associated with a higher risk of epigenetic diseases compared to naturally conceived children.
3.2 Oncogenic risk
There is very limited data and hence further research is needed. The possible mechanism may include structural similarity of antiestrogens with diethylstilbestrol (DES) and alteration of DNA methylation by gamete culture media resulting in embryonic cancers
Based on the evidence, patients should be counseled that infertile women may be at an increased risk of invasive ovarian, endometrial, and breast cancer; however, the use of infertility drugs does not appear to increase this risk
In children with IVF, there is a higher possibility of leukemia, lymphoma, neuroblastoma, retinoblastoma, and hepatoblastoma
ART–conceived children do not appear to have an increased cancer risk after a median follow–up of 20 years. However, more research work is needed to investigate the cancer risk in adults and children conceived by cryopreserved embryos and/or ICSI
3.3 Neurological/autistic risk
ART may be an independent risk factor for autism spectrum disorders (ASD)
3.4 Perinatal risks
Pre–term birth: Single and more so in multiple pregnancy is a clear risk factor for preterm birth. A statistically significant 23% increase in the relative risk of preterm birth occurs in IVF twins compared to natural twins. Similarly, in singletons, there is an estimated two–fold increased risk of preterm birth following IVF
Early term births (37–38 weeks) are associated with adverse neonatal outcomes primarily respiratory problems in comparison to the 39 weeks pregnancy
Low birth weight: singleton IVF pregnancies still demonstrate an increased risk of low birth weight compared with naturally conceived singletons (RR 1.6 95%, CI 1.29–1.98)
IVF twin pregnancies, this increased risk is still evident compared with natural twins
Perinatal mortality: Perinatal risks associated with ART and ovulation induction are higher in multifetal gestation. Even singleton pregnancies are at a higher risk compared to naturally conceiving spontaneous pregnancies
However, it is unclear to what extent these associations might be related to underlying causes of infertility
Before initiation ART, couples should undergo a thorough medical checkup and counsel about these risks
4. Recommendation for monitoring preterm delivery
Consideration of a transvaginal scan to determine the cervical length is recommended between 16 to 24 weeks
If cervical length is found to be <25 mm, prophylactic vaginal progesterone and prophylactic cerclage is recommended
Unless indicated routine cervical cerclage is not recommended
5. Multiple pregnancy
5.1 ART carries a substantial increase in the risk of multiple pregnancy
Multifetal gestation is associated with an increased risk of maternal and fetal morbidity and mortality as a result of preterm birth, preeclampsia, and other pregnancy complications recommend restricted number of embryos’ to be transferred
5.2 Monozygotic twinning is associated with increased perinatal morbidity and mortality
In ART, monozygotic twinning is a common condition, while it is rare in natural conception
ART has been associated with an increased risk of monozygotic twinning that increases the risk of growth abnormalities and twin–to–twin transfusion
Monozygotic twinning remains speculative. Given the possible complications, adequate pre–conception counseling is advocated
5.3 Guideline recommendations for an upper limit of embryos transferred
5.3.1 Patients with a favorable prognosis
-
»
The transfer of single euploid embryo should be single recommended
-
»
A single–embryo transfer is suggested in patients under the age of 37, regardless of the embryo stage
5.3.2 Patients with unfavorable prognosis
For patients between 38 and 40 years of age, no more than three cleavage–stage embryos or two blastocysts are recommended. In cases where euploid embryos are available, a single–blastocyst embryo transfer is suggested
In patients 41–42 years of age, no more than four cleavage–stage embryos or three blastocysts are suggested. In cases where euploid embryos are available, a single–blastocyst transfer is recommended
5.4 Recommendations
-
The risk of multiple pregnancy can be reduced by considering the Limitation of the number of transferred embryos to two or even one
-
»
Also, consideration of eSET helps in reducing the number of twin pregnancies in ART
-
»
6. Recommendations for follow–up
Both the mother and child should be requested to report to IVF centers as well as a pediatrician to assess physical health, mental health, and other complications
7. Recommendations for counseling before IVF
The etiology of risk in ART is likely multifactorial and the magnitude of this risk has not been precisely identified for all women or specific subgroups
-
Many questions remain including the magnitude of risk of ICSI in non–male factor infertility, the effect of prolonged embryo culture, the effect of embryo biopsy, and elucidation as to why risk is lower after a frozen embryo transfer
-
»
All patients considering ART should be informed of the risk
-
»
As scientists and physicians, it is our responsibility to provide safe care. Optimizing the environment at the time a woman conceives will likely have an effect on gestation as well as the health of children. Reproduction effects health and health effects reproduction
Summary of recommendations
ART exposes patients and professionals to delicate psychosocial issues and situations
Psychological counselling should be offered to all infertile couples independent of their individual diagnoses or the stage of medical treatment and independent of treatment
Giving basic information concerning individual treatment and the emotional implications helps patients to integrate the process which enhances quality patient care, personal and team satisfaction
Psychosocial care, infertility counselling and psychotherapy are not clearly distinct categories
Screening instruments are helpful for identifying patients which have to be referred into psychotherapy. Exact criteria when to refer have to be developed yet
Caring for the emotional needs of the patient demands continuity and should not be treated as a single event. Holistic patient care should be the aim whilst they undergo treatment
Important to discuss about options available, cost, success rate of different procedures and must emphasize that failures are more than successes
Recommendations for incident reporting
All IVF centers must maintain a follow-up of all their pregnancies by ART
Also, complications must be reported to a central database and records maintained for at least 10 years
The obstetrician should report any adverse events in an ART pregnancy to the centre concerned and records to be maintained or 10 years
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CPP | ART exposes patients and professionals to delicate psychosocial issues and situations | - | - |
| CCR | Psychological counselling should be offered to all infertile couples independent of their individual diagnoses or the stage of medical treatment and independent of treatment | B | - |
| CCR | Giving basic information concerning individual treatment and the emotional implications helps patients to integrate the process which enhances quality patient care, personal and team satisfaction | B | - |
| CPP | Psychosocial care, infertility counselling, and psychotherapy are not clearly distinct categories | - | - |
| CPP | Screening instruments are helpful for identifying patients which have to be referred into psychotherapy. Exact criteria when to refer have to be developed yet | - | - |
| CPP | Caring for the emotional needs of the patient demands continuity and should not be treated as a single event. Holistic patient care should be the aim whilst they undergo treatment | - | - |
| CPP | Important to discuss about options available, cost, success rate of different procedures, and must emphasize that failures are more than successes | - | - |
| Recommendations for incident reporting | |||
| CPP | • All IVF centers must maintain a follow–up of all their pregnancies by ART | - | - |
| CCR | • Also, complications must be reported to a central database and records maintained for at least 10 years | C | - |
| CCR | • The obstetrician should report any adverse events in an ART pregnancy to the centre concerned and records to be maintained or 10 years | C | - |
References
Sharma RS, Saxena R, and Singh R. Infertility & assisted reproduction: A historical & modern scientific perspective. Indian J Med Res. 2018; 148(1):S10–S14.
Alukal JP, Lamb DJ. Intracytoplasmic sperm injection (ICSI)--what are the risks? Urol Clin North Am. 2008; 35(2):277–88.
Metwally M, Ledger WL. Long-term complications of assisted reproductive technologies. Hum Fertil (Camb). 2011; 14(2):77–87.
Rao K. Nobel prize for scientist Professor Robert G Edwards. J Hum Reprod Sci. 2010;3(3):120.
NICE Clinical Guidelines, No. 156. National Collaborating Centre for Women’s and Children’s Health (UK). London: Royal College of Obstetricians & Gynecologists; 2013. Available at: https://www.ncbi.nlm.nih.gov/books/NBK327768/. Accessed 25th September 2019.
Sallam HN, Abdel-Bak M, Sallam NH. Does ovulation induction increase the risk of gynecological cancer? Facts Views Vis Obgyn. 2013; 5(4):265–273.
Diergaardea B, Kurta ML. Use of fertility drugs and risk of ovarian cancer. Curr Opin Obstet Gynecol. Author manuscript; available in PMC 2015.
Siristatidis C, Sergentanis TN, Kanavidis P, et al. Controlled ovarian hyperstimulation for IVF: Impact on ovarian, endometrial and cervical cancer--A systematic review and meta-analysis. Hum Reprod Update. 2013; 19(2):105–23.
Rizzuto I, Behrens RF, Smith LA. Risk of ovarian cancer in women treated with ovarian stimulating drugs for infertility. Cochrane Database Syst Rev. 2013; 2013(8):CD008215.
Sergentanis TN, Diamantaras AA, Perlepe C, et al. IVF and breast cancer: a systematic review and meta-analysis. Hum Reprod Update. 2014; 20(1):106-23.
Bonduelle M, Liebaers I, Deketelaere V, et al. Neonatal data on a cohort of 2889 infants born after ICSI (1991-1999) and of 2995 infants born after IVF (1983-1999). Hum Reprod. 2002; 17(3):671-94.
Davies MJ, Moore VM, Willson KJ, et al. Reproductive technologies and the risk of birth defects. N Engl J Med. 2012; 366(19):1803–13.
Hansen M, Kurinczuk JJ, Milne E, et al. Assisted reproductive technology and birth defects: a systematic review and meta-analysis. Hum Reprod Update. 2013; 19(4):330–53.
Yu HT, Yang Q, Sun XX, et al. Association of birth defects with the mode of assisted reproductive technology in a Chinese data-linkage cohort. Fertil Steril. 2018; 109(5):849–856.
Butler MG. Genomic imprinting disorders in humans: a mini-review. J Assist Reprod Genet. 2009; 26(9-10):477–486.
Uk A, Collardeau-Frachon S, Scanvion Q, et al. Assisted reproductive technologies and imprinting disorders: Results of a study from a French congenital malformations registry. Eur J Med Genet. 2018; 61(9):518–23.
ASRM Group. Fertility drugs and cancer: a guideline. Fertil Steril. 2016; 106(7):1617–1626.
Spaan M, van den Belt-Dusebout AW, van den Heuvel-Eibrink MM, et al. Risk of cancer in children and young adults conceived by assisted reproductive technology. Hum Reprod. 2019; 34(4):740–750.
Liu L, Gao J, He X, et al. Association between assisted reproductive technology and the risk of autism spectrum disorders in the offspring: a meta-analysis. Sci Rep. 2017; 7:46207.
Rumbold AR, Moore VM1, Whitrow MJ, et al. The impact of specific fertility treatments on cognitive development in childhood and adolescence: A systematic review. Hum Reprod. 2017; 32(7):1489–1507.
Vulliemoz NR, McVeigh E, Kurinczuk J. In vitro fertilisation: Perinatal risks and early childhood outcomes. Hum Fertil (Camb). 2012; 15(2):62–8.
NICE. Preterm labor and birth. NICE Guidelines. Available at: https://www.nice.org.uk/guidance/ng25/resources/preterm-labour-and-birth-pdf- 1837333576645. Published 2015.
BJOG. An International Journal of Obstetrics and Gynecology. Multiple Pregnancies Following Assisted Conception: Scientific Impact Paper No. 22. BJOG. 2018; 125(5):e12–e18.
American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice, et al.
Committee Opinion No 671: Perinatal Risks Associated With Assisted Reproductive Technology. Obstet Gynecol. 2016; 128(3):e61–8.
Aston KI, Peterson CM, Carrell DT. Monozygotic twinning associated with assisted reproductive
technologies: A review. Reproduction. 2008; 136(4):377–86.
Murray SR, Shenkin SD, McIntosh K, et al. Long term cognitive outcomes of early term (37-38 weeks) and late preterm (34-36 weeks) births: A systematic review. Wellcome Open Res. 2017; 2:101.
Sobek A, Prochazka M, Klaskova E, et al. High incidence of monozygotic twinning in infertility treatment. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2016; 160(3):358–62.
ASRM group, et al. Guidance on the limits to the number of embryos to transfer: A committee opinion. Fertil Steril. 2017; 107(4):901–903.
Practice committee of SART, ASRM. Elective single-embryo transfer. Fertil Steril. 2012; 97(4):835–42.
Barnhart KT. Assisted reproductive technologies and perinatal morbidity: Interrogating the association. Fertil Steril. 2013; 99(2):299–302.
Sarah Marie Bjørnholt, Susanne Krüger Kjaer, Thor Schütt Svane Nielsen, Allan Jensen, Risk for borderline ovarian tumours after exposure to fertility drugs: results of a population-based cohort study, Human Reproduction, Volume 30, Issue 1, January 2015, Pages 222–231,
Van Leeuwen FE, Klip H, Mooij TM, Van De Swaluw AM, Lambalk CB, Kortman M, Laven JS, Jansen CA, Helmerhorst FM, Cohlen BJ, Willemsen WN. Risk of borderline and invasive ovarian tumours after ovarian stimulation for in vitro fertilization in a large Dutch cohort. Human reproduction. 2011 Dec 1;26(12):3456-65.
Fortin A, Morice P, Thoury A, Camatte S, Dhainaut C, Madelenat P. Impact of infertility drugs after treatment of borderline ovarian tumors: results of a retrospective multicenter study. Fertility and sterility. 2007 Mar 1;87(3):591-6.
Daraï E, Fauvet R, Uzan C, Gouy S, Duvillard P, Morice P. Fertility and borderline ovarian tumor: a systematic review of conservative management, risk of recurrence and alternative options. Human reproduction update. 2013 Mar 1;19(2):151-66.
Diergaarde B, Kurta ML. Use of fertility drugs and risk of ovarian cancer. Current opinion in obstetrics & gynecology. 2014 Jun;26(3):125.
Lindsay K, Daniel D, Zain AS. Use of fertility medications and cancer risk: a review and update. Current opinion in obstetrics & gynecology. 2017 Aug;29(4):195.
Chapter 22: Ethical Issues: Assisted Reproductive Technologies
OVERVIEW
This guideline offers recommendations on the importance of assisted reproductive technologies in treating infertility. It also covers resolution on ethical issues encountered while providing ART benefits to respective patients.
1. Introduction
1.1 ART in Infertility
Infertility cases are increasing day by day throughout the world and create social and mental trouble to the suffering couple. The success ratios of pharmacological treat ments in improving the infertility problems are not up to the mark hence require an alternative.
Assisted reproductive technology (ART) majorly utilizing in vitro fertilization (IVF) technique for treating infertility has raised hopes for several couples throughout the world. Most ARTs are recommended because these do not treat the biological problems that give rise to infertility but circumvent them and offer ways to have children despite underlying fertility problems
1.2 Necessity of ethical issues and regulation
Specific clinical setup is required to provide such techniques for which regulatory guidelines has to be followed
Regulatory interference is mandatory as it is accompanied by ethical and societal concerns. The majority of new techniques, which provide infertility solutions, require gamete (spermatozoa or the oocytes) handling outside the body. This may result in unethical practices affecting the recipient of the treatment, medically, socially, and legally
-
Ethical issues which may arise during the use of ART are:
-
»
Bypassing the natural method of conception
-
»
Creating life in laboratory
-
»
Fertilizing more embryos than will be needed
-
»
Discarding excess embryos
-
»
Expensive technology, not affordable for common man
-
»
Creating embryos, freezing them, and storing
-
»
Destroying embryos for research
-
»
Selective selection of embryos for transfer
-
»
Currently, ART is recommended throughout the world for the treatment of infertility and therefore, the chances of ethical misconduct at the same time are also high. In such scenario, it is recommended to create certain regulatory policies for use of ART to protect he medical, social and legal rights of women and the unborn child
These regulations may advise in providing couples with the best possible management of their problems, while at the same time ensuring that there are no unnecessary risks or ineffective treatments
2. Best practice recommendations
2.1 Clinical facility registration
-
Register all ART clinics with central registration authority and provide all necessary details of techniques and procedures of ART practiced at clinics
-
»
Clinics performing IUI should also register
-
»
Only clinics that meet certain physical infrastructure requirements and have prescribed technical expertise are allowed to enroll in the registry
-
»
Monitor quality and quantity of all assisted reproduction procedures. It is recommended to submit annual reports of all treatment cycles and their outcome to central database
Monitor ART procedures data at individual clinics and with central registry to understand the improvement in efficacy, safety and success rates of the fertility treatments
2.2 Age, eligibility criteria, and ART treatments
Make ART treatments available to each needy person accordingly to the law of the land
Do not offer ART to women with age above 45 years and Men above 50 years
Do not suggest ART for the women with age below 21 years and men below 23 years
ART should be offered to the couple keeping in mind the best interests of a particular patient or their potential offspring to proceed with IVF because of
Associated safety issues
Older women are more prone to develop chronic disorders like diabetes which may affect off springs
Chances of chromosomal abnormalities particularly after 35 years of maternal age
2.3 Counseling during ART
Offer professional counseling to all patients undergoing fertility treatments
Explain various treatment alternatives available with reason for recommendation of particular treatment to arrive at informed decision
Counsel patients regarding the implications and chances of success of ART procedures in India and internationally from the available reference data being updated regularly (6–12 months)
Counsel patients about merits and demerits of ART procedures, side effects of drugs used during procedures, risks including the complications of multiple pregnancy, and ovarian hyperstimulation syndrome (OHSS)
Inform patients about the costs of proposed and alternative treatments. Do not hide any charges to be applied for treatment
Counsel patients about the associated benefits and loss of continuing treatment after a certain number of attempts
Discuss the possibility of adoption with patients whenever required
Counsel couples or individual about their rights of a child born through the use of ART
Provide clear, precise and honest information (in the form of pamphlets) about the procedures to patients in local language and English
The counseling should help the patient/s in taking an informed decision
2.4 Documentation, record keeping, and consenting
Obtain written informed consent from all individuals/ couples before initiating any ART treatment or procedures
Start freezing procedures of embryo only after obtaining informed consent from all individual seeking ART and also discuss about the management of frozen gametes or embryos in case of death or incapacity of any of the parties
Allow individual seeking ART to withdraw consent any time before embryos or the gametes are transferred to the woman’s uterus
Maintain detailed records of all procedures performed at clinic. These records should be maintained for a period of 10 years at least
This data will automatically get transferred to national ART registry to be set up by the Department of Health Research at the Headquarters of the ICMR
As may be prescribed by ICMR of all IUI and ART cycles
Sperm, oocytes or embryos used
The manner and technique of their use
The individual or couple or surrogate mother in respect of whom it was used
Of all donor oocyte and embryo cycles
Maintain the clinic’s data of all infertility and ART procedures including adverse outcomes
Record details of all the gametes or embryos received, used and stored
Maintain proper records along with its identification during and after storage of gametes and embryos. Security of the stored gametes and embryos should also be provided
Provide discharge certificate with details of ART performed
Maintain confidentiality of all the patients who have undergone ART procedures
-
Inform about legal right of born child and parents
-
»
In case of married couples, the child born to them through ART is considered legitimate child of couple
-
»
In case of a single woman the child should be considered as the legitimate child of the woman
-
»
In case a married couple separates or gets divorced, after both parties consented to the ART treatment but before the child is born, the child shall be the legitimate child of the couple
-
»
A child born to a woman artificially inseminated with the stored sperm of her dead husband with prior consent should be considered as the legitimate child of the couple
-
»
Unused embroyos can be used for research with approval of the couple
Mixing of sperms or oocytes from more than one person is not allowed
2.5 Gender selection in ART
Do not offer the facility to identify/predetermination of sex of child before birth to recipient of ART
Do not provide, prescribe or administer anything that would ensure or increase the probability that an embryo shall be of a particular sex except to diagnose a sex–linked disorder or disease
Do not perform any procedure to separate, or yield fractions enriched in sperm of X or Y variations
Human reproductive cloning is not allowed
2.6 HIV and ART
ART cannot be refused to a HIV discordant couples however it is recommended to have facilities available to prevent horizontal and vertical spread of HIV
Prevalence of HIV infected people is increasing day by day where majority of the infected patients are of reproductive age group. In such cases, couple should be counseled not opt for natural conception process because of associated risk to offspring
-
ART procedures are recommended for HIV positive couples because
-
»
When male partner is sero-positive, modified density–gradient centrifugation and swim–up method for sperm preparation coupled with either inseminations or in vitro fertilization (IVF) with intracytoplasmic sperm injection (ICSI) can be used as these techniques have proven to be highly effective in avoiding seroconversion of uninfected women and offspring
-
»
When female partner is seropositive, a healthy conception can be achieved with help of antiretroviral treatment followed by intrauterine insemination or IVF
-
»
Consider the preexposure prophylaxis of antiretroviral drugs before commencing fertility treatments, which may further reduce the susceptibility of the uninfected female partner and child. Research has shown that, once pregnant, the use of antiretroviral therapy and avoidance of breastfeeding in HIV infected women may reduce chance of newborn infection to approximately 2%
Ensure safety through evaluation of clinical part of the program (oocyte retrieval) and of the laboratory conditions during IVF cycle
Consider having separate tanks for storage of infected material
2.7 Multiple pregnancy and ART
The incidence of multiple pregnancies is higher in ART, hence it recommended to not transfer more than 2 embroyos in young women and note more than 3 in older women and in recurrent implantation failure
2.8 ART and welfare of the unborn child
Consider the medical risks, family environment, and social environment before initiating ART procedures
Consider the best interest of unborn child before proceeding for ART
2.9 ART and preimplantation genetic diagnosis
Inform and counsel couple undergoing (IVF/ICSI) preimplantation genetic diagnosis (PGD) cycle about its complexities and uncertainties, including possible dilemmas and conflicts regarding embryo transfer after PGD
Offer PGD only to screen the embryo for known, preexisting, heritable or genetic diseases. PGD in order to select for handicap/disability is morally unacceptable
Aneuploidy screening should be done in high risk patients
2.10 Ethical aspect of gamete donation:
Gamete donors should be free of all communicable diseases, sexually transmitted diseases, and identifiable genetic disorders
Semen donors should be between 21 to 45 years (both inclusive). Donor sperm should be cryopreserved for at least six months (quarantine period) before being used and, at the expiry of such period, the ART bank shall not supply the sperm to any assisted reproductive technology clinic unless the sperm donor is tested for such diseases, sexually transmitted disease or otherwise, as may be prescribed
Single donor sample can be used for 25 times
One sample of semen supplied by an ART bank shall be used by the assisted reproductive technology clinic only once on only one recipient
Oocyte donors should be between 23 to 35 years (both inclusive)
Oocyte donor can donate oocytes for maximum of one time in her lifetime
Eggs from one donor can be shared between two recipients only, provided that at least seven oocytes are available for each recipient
All unused oocytes would be either appropriately preserved by the assisted reproductive technology clinic for use on the same recipient(s), or given for research to a bonafide organization
An ART bank shall obtain all necessary information in respect of a sperm or oocyte donor, including the name, identity and address of such donor or surrogate, and shall undertake in writing to the donor to keep such information confidential
No ART bank shall divulge the name, identity, or address of any sperm or oocyte donor to any person or assisted reproductive technology clinic except in pursuance of an order or decree of a court of competent jurisdiction
Any person or ART bank who divulges the name, identity or address of a sperm donor shall be guilty of an offence
The collection of gametes from a person whose death is imminent shall only be permissible if such person’s spouse intends to avail assisted reproductive technology to have a child
2.11 Research & ART
Only those gametes and embryos donated for research purpose
Maintain prior regulatory approval (Department of Health Research) before conducting any research studies
2.12 Code of practice
Code of Practice deals with all aspects of the treatment provided and the research done at registered clinics.
Any information about clients and donors must be kept confidential, except with the consent of the person to whom the information relates, or in a medical emergency or a court order
All relevant information must be given to the patient before a treatment is given
No treatment should be given without the written consent of the couple
A standard consent form recommended by the accreditation authority should be used by all ART clinics
Specific consent must be obtained from couples who have their gametes or embryos frozen, in regard to what should be done with them if he/she dies or becomes incapable of varying or revoking his or her consent
People seeking registered treatment must be given a suitable opportunity to receive proper counseling about the various implications of the treatment
Summary of recommendations
| Category | Recommendations | Grade of Recommendation | Quality of Evidence |
|---|---|---|---|
| CPP | Accreditation and supervision of ART Clinics and Banks necessary to ensure that services provided by the ART Clinics and Banks are ethical | - | - |
| CPP | To ensure Medical, social and legal rights of all those concerned are protected with maximum benefit to the infertile couples or individuals within a recognized framework of ethics and good medical practice | - | - |
| CPP | All ART clinics handling gametes need to enroll in a national registry (ICMR) before they are allowed to operate, therefore clinics performing IUI are also included | - | - |
| CPP | Only clinics that meet certain physical infrastructure requirements and have prescribed technical expertise are allowed to enroll in the registry | - | - |
| CPP | Do not offer ART to women with age above 45 years and Men above 50 years because of • Associated safety issues • Older women are more prone to develop chronic disorders like diabetes which may affect off springs • Chances of chromosomal abnormalities particularly after 35 years of maternal age |
- | - |
| CPP | Do not suggest ART for the women with age below 21 years and men below 23 years | - | - |
| CPP | All infertile couples undergoing treatment especially those who are going to undertake third party procedures should have a psychosocial counselling | - | - |
| CPP | Counselling about the investigations, management, complications and cost will help the patient/s in taking an informed decision | - | - |
| CPP | No ART clinic shall perform any treatment or procedure of ART without the consent in writing of all the parties seeking ART | - | - |
| CPP | No ART clinic shall freeze any human embryos without specific instructions and consent in writing from all the parties seeking ART | - | - |
| CPP | All ART clinics shall maintain detailed records, in the following manner: • As may be prescribed • Of all donor oocytes • Sperm, oocytes or embryos used • The manner and technique of their use • The individual or couple or surrogate mother in respect of whom it was used |
- | - |
| CPP | All ART clinics will, as and when such central facilities are established ⊠ put online all information available to them in regard to progress of the patient (such as biochemical and clinical pregnancy), which should be done within seven days of the information being available,withholding the identity of the patient | - | - |
| CPP | Records maintained for at least a period of ten years, upon the expiry of which the ART clinic shall transfer the records to a central database of a, national ART registry to be set up by the Department of Health Research at the Headquarters of the ICMR | - | - |
| CPP | ART cannot be refused to a HIV discordant couples however it is recommended to have facilities available to prevent horizontal and vertical spread of HIV | - | - |
| CPP | The incidence of multiple pregnancies is higher in ART, hence it recommended to not transfer more than 2 embryos in young women and note more than 3 in older women and in recurrent implantation failure. | - | - |
| CPP | Sex selection No ART clinic shall offer to provide a couple with a child of a pre–determined sex No assisted reproductive technology clinic will carry out any ART procedure to separate, or yield fractions enriched in sperm of X or Y variations Any contravention of stipulation under subsection 1, 2, 3 and 4 of this section shall amount to an offence under this Act | - | - |
| CPP | Preimplantations genetics screening or diagnosis indicated for screen the embryo for known, pre-existing, heritable or genetic diseases or life–threatening condition Aneuploidy screening | - | - |
| CPP | Unused embryos should be destroyed or given for research only with the approval of the patient | - | - |
| CPP | Mixing of sperms or oocytes from more than one person not allowed | - | - |
| CPP | In the event of the closure ART bank immediately transfer the records to a central database of a, national ART registry to be set up by the Department of Health Research at the Headquarters of the ICMR | - | - |
| CPP | Sperm or semen, oocytes or oocyte donors and surrogate mothers should be obtained by the ART clinics or their patients from Assisted Reproductive Bank | - | - |
| CPP | Semen donors should be between 21 to 45 years (both inclusive). Donor sperm should be cryopreserved for at least six months (quarantine period) before being used and, at the expiry of such period, the ART bank hall not supply the sperm to any assisted reproductive technology clinic unless the sperm donor is tested for such diseases, sexually transmitted disease or otherwise, as may be prescribed | - | - |
| CPP | Single donor sample can be used for 25 times | - | - |
| CPP | Oocyte donors should be between 23 to 35 years (both inclusive). Oocyte donor can donate oocytes for maximum of one time in her life time | - | - |
| CPP | Eggs from one donor can be shared between two recipients only, provided that at least seven oocytes are available for each recipient | - | - |
| CPP | The collection of gametes from a person whose death is imminent shall only be permissible if such person’s spouse intends to avail assisted reproductive technology to have a child | - | - |
| CPP | Gamete donation from relatives and friends is not allowed | - | - |
| CPP | Surplus embryos cannot be used for embryo donation | - | - |
ICMR reference not added
References
Human immunodeficiency virus (HIV) and infertility treatment: a committee opinion. Ethics Committee of the American Society for Reproductive Medicine American Society for Reproductive Medicine, Birmingham, Alabama. Fertil Steril 2015.
Guidelines for infertility counselling in different countries: Is there an emerging trend? Eric Blyth, Human Reproduction, Volume 27, Issue 7, July 2012, Pages 2046–2057.
National Draft Guidelines for Accreditation, Supervision & Regulation of ART Clinics in India - Indian Council of Medical Research (ICMR) at www.icmr.nic.ins