

Abstract
Ventricular arrhythmias (VAs) are a group of heart rhythm disorders that can be life‐threatening and cause significant morbidity. VA in the presence of structural heart disease (SHD) has distinct prognostic implications and requires a comprehensive and multifaceted approach for investigation and management. Early specialist referral should be considered for all patients with VA. Particular urgency is recommended in patients with syncope, nonsustained/sustained VA on Holter monitor and SHD on cardiac imaging because of the heightened risk of sudden cardiac death. Comprehensive phenotyping is recommended for most patients with VA, encompassing noninvasive cardiac functional testing, multimodality imaging and genetic testing in select circumstances. Management of idiopathic VA is guided heavily by symptom burden and the presence of ventricular systolic impairment. In SHD, guideline‐directed heart failure therapy and device implantation are critical considerations. Whilst commonly used and well‐established, antiarrhythmic drugs can be hampered by toxicity and failure of adequate arrhythmia control. Catheter ablation is increasingly being considered a feasible first‐line alternative to medical therapy, where outcomes are influenced by disease aetiology and scar burden in SHD. Catheter ablation is associated with reduced arrhythmia recurrence and burden and improved quality of life at follow‐up.
Keywords: ventricular tachycardia, cardiomyopathies, catheter ablation, defibrillator, channelopathies
Introduction
Ventricular arrhythmias (VAs) are a heterogeneous group of heart rhythm disorders that account for approximately 30% of sudden cardiac death (SCD) globally, constituting a greater proportion in the younger population. 1 Beyond SCD, VAs are a major cause of morbidity, with debilitating symptoms that can impair quality of life, cause loss of social and economic productivity and precipitate heart failure. Furthermore, VAs are a major contributor to healthcare resource utilisation, often requiring frequent clinical encounters, protracted hospital admissions and multidisciplinary management. VAs occur as a result of an abnormal focus or conduction abnormalities through the ventricles. Their management hinges on early identification and treatment of underlying conditions, use of antiarrhythmic drugs (AADs), implantable cardioverter‐defibrillators (ICDs) and interventional catheter ablation (CA). This state‐of‐the‐art review aims to comprehensively cover the mechanistic basis, key clinical manifestations and treatment for patients with VA.
Pathophysiology
VA comprises: (i) premature ventricular complexes (PVCs), (ii) ventricular tachycardia (VT) and (iii) ventricular fibrillation (VF). Whilst overlap exists in their underlying mechanisms, each have distinct clinical presentations and management implications.
Premature ventricular complexes
PVCs occur as a result of abnormal automaticity of cardiomyocytes or from spontaneous oscillations in cell membrane potential after depolarisation, known as triggered activity. Whilst causes may be reversible, including electrolyte disturbances, hypoxia, heightened sympathetic tone and cardiac inflammation, the cause of most PVCs remains unknown. PVCs may occur in the presence or absence of underlying structural heart disease (SHD). Idiopathic PVCs (i.e. occurring in the absence of underlying SHD) do not occur from random sites, but rather have a proclivity for typical endocardial sites such as right ventricuar (RV) and left ventricular (LV) outflow tracts, papillary muscles, mitral/tricuspid annuli and the Purkinje network in the left and right ventricles (Fig. 1A). Rarely, they occur from the LV summit (the most basal aspect of the left ventricle) and may involve the epicardial surface.
Figure 1.

Mechanism of idiopathic vs reentrant ventricular arrhythmias (VAs). (A) Coronal cross‐section of both ventricles demonstrating common sites of idiopathic VA (yellow stars). These include the right ventricular (RV) and left ventricular (LV) outflow tracts, mitral and tricuspid annuli, LV papillary muscles and RV moderator band. (B) Coronal cross‐section of both ventricles demonstrating scar (grey) in the lateral LV wall in structural heart disease. Magnified panel demonstrates the concept of reentry, with loop‐like ventricular activation around a scar (thick arrowed line) and slow conduction through a critical channel/isthmus within the scar (blue).
Ventricular tachycardia
VT involves more sustained and repetitive ventricular activations. Mechanisms include abnormal automaticity or triggered activity in structurally normal hearts (‘idiopathic’ VT), commonly arising from critical sites similar to the location of idiopathic PVCs (Fig. 1A). However, reentry is the most common mechanism, especially in SHD (Fig. 1B). 2 Reentry involves continuous, loop‐like ventricular activation within a circuit that is created by slow, serpiginous conduction through cardiac tissue that is an admixture of surviving, damaged and poorly coupled myocytes interspersed within fibrotic regions. An exception to this rule is fascicular VT, which occurs in the absence of SHD and has a reentrant mechanism involving the LV conduction system (fascicles).
Microscopically, disruptions in intercellular connections cause slower electrical conduction, creating the milieu for the initiation of VT through opportunistically timed PVCs or variations in heart rate due to autonomic tone. Macroscopically, this reentrant circuit relies on slow conduction through a critical channel within the scar (isthmus). Scar can arise from prior myocardial infarction–driven fibrosis caused by coronary artery disease or nonischaemic causes such as cardiomyopathies or infiltrative heart disease. In ischaemic heart disease (IHD), scar distribution is typically just beneath the endocardial surface, with variable penetration to deeper midmyocardial and outer myocardial (epicardial) layers. In contrast, scar in nonischaemic cardiomyopathies (NICMs) tends to manifest within deep intramural and/or epicardial regions (Fig. 2) and can occur even when ventricular function is normal. 3 Early NICMs typically have scar subtending valve annuli, with reentrant circuits around the scar and valve annulus.
Figure 2.

Scar distribution in ischaemic vs nonischaemic cardiomyopathy. (A) Diagram with occluded middistal left anterior descending coronary artery and resultant ischaemic scar (grey). Magnified panel demonstrates a cross‐section through the ventricular wall in the region of scar. Note the subendocardial scar superiorly, followed by transmural scar inferiorly through the thickness of the ventricular wall. (B) Coronal cross‐section of both ventricles demonstrating mid‐wall, intramural scar within the interventricular septum and epicardial scar in the basal lateral wall.
Ventricular fibrillation
When critically timed, PVCs from regions such as the Purkinje conduction system can initiate VF. 4 Microstructural abnormalities can also cause VF in otherwise structurally normal hearts, requiring detailed invasive electroanatomic mapping for detection. VT, for extended durations, may also degenerate into VF. Like focal mechanisms, reversible causes include electrolytes disturbances, medication toxicities and acute myocardial ischaemia.
In the absence of SHD, genetic channelopathies are a large contributor to VF and SCD. The most common is long QT syndrome (LQTS), wherein mutations in cardiac cell membrane potassium, sodium or calcium channels result in prolongation of action potential repolarisation. This causes cardiac membrane instability, an increased risk of triggered activity and resultant VF. Catecholaminergic polymorphic ventricular tachycardia (CPVT) is another syndrome, where mutations in the genes encoding for the ryanodine receptor or calsequestrin protein result in intracellular calcium overload, increased triggered activity and VT/VF triggered by increased sympathetic tone.
Given the ubiquitous effect of these channelopathies on the ventricular myocardium, they traditionally lack an anatomic focus to target with CA. Instead, management is focused on ameliorating recurrent syncope and SCD risk with AADs and ICD implantation in refractory cases or patients deemed high risk on genetic testing. An exception is Brugada syndrome, originally thought to be a genetic channelopathy involving primarily loss of function mutations in the sodium channel. More recently, structural changes in the epicardial RV outflow have been identified in Brugada syndrome that may be amenable to CA in patients with recurrent syncope and ICD shocks. 5
Clinical presentation
PVCs can cause debilitating symptoms such as palpitations, chest discomfort, dyspnoea and presyncope; however, high‐burden PVCs can also be asymptomatic. PVC‐induced cardiomyopathy can occur with a higher PVC burden and is thought to be reversible with treatment (i.e. AAD or CA), although it can be difficult to differentiate from an underlying primary cardiomyopathy. SCD risk rises with higher PVC burden, multiple morphologies and coexistence with SHD. 6 , 7 When occurring close to the normal QRS (i.e. ‘closely coupled’), PVCs can be associated with a higher risk of SCD due to VF. PVC associated with mitral valve prolapse can also be associated with SCD, especially with multiple PVC morphologies.
VT can vary from being asymptomatic, syncope to SCD. Multiple factors can drive symptoms, including arrhythmia speed, duration and concomitant LV dysfunction. VF is a life‐threatening arrhythmia that, when sustained, can precipitate SCD because of its incompatibility with maintaining cardiac output. When nonsustained, VF may present with presyncope without palpitations. On 12‐lead electrocardiogram (ECG), it is characterised by irregular, disorganised ventricular activations at ≥300 per minute.
Assessment and diagnosis
Investigation of VA can be categorised into arrhythmia characterisation and investigation for SHD (Fig. 3). PVC can coexist with VT and VF and may not be related to the primary clinical arrhythmia. Careful clinical assessment is necessary to discriminate between potential bystander arrhythmias that may not be clinically significant.
Figure 3.
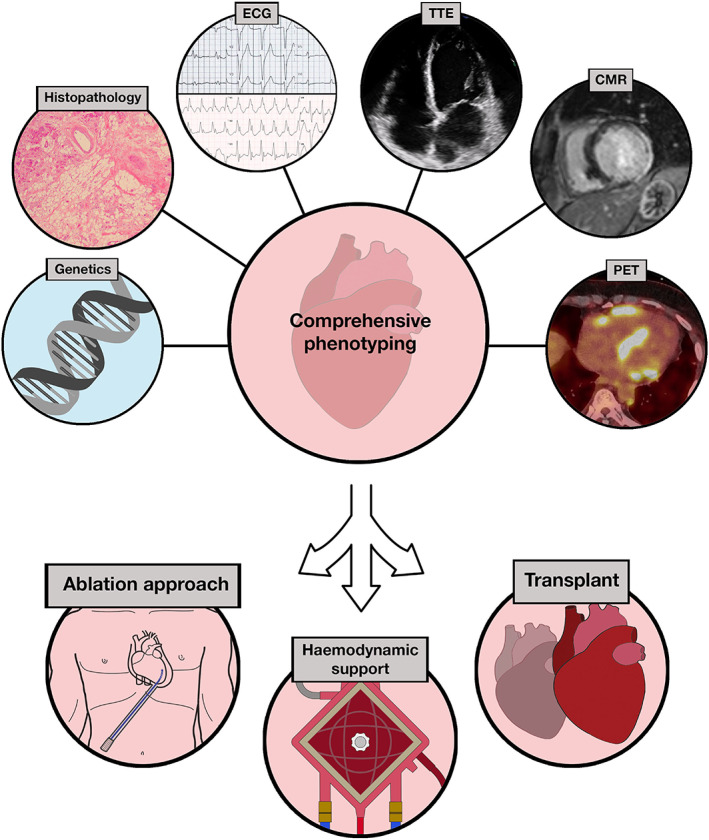
Comprehensive phenotyping workflow. Schematic demonstrating workflow for comprehensive phenotyping (top) with resultant management implications (bottom). Clockwise from top left – Genetics: histopathology slide showing fibrofatty replacement in a case of advanced LMNA cardiomyopathy; sinus rhythm electrocardiogram (ECG) (top) showing conduction disease (first‐degree heart block and left bundle branch block) suggesting septal substrate, and ECG during ventricular tachycardia (bottom) allowing for localisation based on morphology; transthoracic echocardiogram (TTE) showing biventricular enlargement and septal wall thinning; cardiac magnetic resonance imaging (CMR) showing late gadolinium enhancement of inferolateral left ventricle; positron emission tomography (PET) showing avid tracer uptake in basal septum in a case of cardiac sarcoidosis. Anticlockwise from bottom left – planning of ablation approach including upfront epicardial approach (depicted) with discussion of risks and surgeon‐assisted access if required; consideration of haemodynamic support, such as extracorporeal membrane oxygenation, to facilitate accurate mapping of ventricular tachycardia and minimise systemic sequelae from prolonged hypoperfusion; early consideration for transplant in suitable candidates, especially in advanced cases of cardiac sarcoidosis, myocarditis or irreversible disease pathologies such as LMNA cardiomyopathy.
12‐Lead electrocardiogram
The 12‐lead ECG provides insights into both the VA and underlying contributors. When captured, the VA morphology may permit localisation, using specific algorithms, to the right or left ventricles and inner (endocardial) or outer (epicardial) regions, which can facilitate greater informed discussions of management options.
Analysis of the native, sinus rhythm on 12‐lead ECG can raise the clinician's suspicion of underlying SHD through alterations of QRS and T‐wave morphology. In IHD, Q waves represent regions of infarction along coronary vascular territories that may harbour substrate for reentrant VT. Increased QRS voltages with marked T‐wave inversion may suggest hypertrophic cardiomyopathy. Often overlooked, the presence of conduction disease, including atrioventricular and/or bundle branch block may suggest septal scar that is intramural and difficult to target with CA without causing pacemaker dependence. Another common NICM subtype is an inferolateral scar, which can be inferred through low QRS voltages in the inferior leads or the presence of lateral Q waves (Fig. 2B). 3
Channelopathies may be detected purely by 12‐lead ECG, either at rest or with provocation manoeuvres. LQTS has distinct clinical subtypes, each accompanied by characteristic situational triggers and T‐wave architecture alterations associated with QT interval prolongation. Accurate QT interval measurement is critical, with correction of the measurement relative to the heart rate (Bazzett formula), where QTc >450 ms in men and >460 ms in women is considered to be abnormal. Occasionally, a standing ECG may unmask LQTS because of lack of QT interval shortening induced by a sudden increase in heart rate (from heightened sympathetic tone) with standing. Brugada syndrome is characterised by distinct precordial coved‐shaped ST elevation in leads V1–3 at baseline or provoked with fever (type I). Intravenous sodium channel blockade with flecainide or ajmaline can unmask these changes where clinical suspicion is high because of atypical, noncoved‐shaped ST elevation in the precordial leads (types II/III).
Functional electrocardiography
Exercise stress ECG may provide functional insights into VA. Inducibility with peak exercise can suggest an idiopathic VA with sudden onset and offset at a critical heart rate. It also plays an important role in diagnosing concealed channelopathies. LQTS may be unmasked through insufficient QT interval shortening during exercise‐induced tachycardia and in prolonged recovery for up to 7 min. CPVT is also classically diagnosed through exercise‐induced ‘bidirectional’ VT or PVC with alternating ECG morphology.
Holter monitoring allows for the assessment of arrhythmia burden, temporal associations and symptom correlation. A specific threshold for PVC burden has been difficult to establish because of their variable association with symptoms and underlying cardiomyopathy. 8 However, in general, a cutoff of >20% is considered to be associated with PVC‐induced cardiomyopathy. A longer PVC QRS duration may indicate an epicardial focus and a greater risk of PVC‐induced cardiomyopathy. 9 Multiday Holter monitoring may also increase yield and provide a more accurate assessment of burden than 24‐h monitoring.
Cardiac imaging
There are multiple imaging modalities available for comprehensive phenotyping of patients with VA, summarised in Table 1. In this clinical setting, imaging may be categorised into assessment of myocardial and valvular function and ventricular tissue characterisation. In IHD, LV systolic dysfunction, measured as ejection fraction, has been well established in international guidelines as a predictive threshold for SCD, although its sensitivity and specificity remain limited. 10 , 11 Regional wall motion abnormalities, detected on transthoracic echocardiography and cardiac magnetic resonance imaging (CMR) may help localise reentrant, monomorphic VT to regions of scar.
Table 1.
Diagnostic cardiac imaging modalities
| Modality | Advantages | Limitations |
|---|---|---|
| Transthoracic echocardiography |
|
|
| Cardiac magnetic resonance |
|
|
| Position emission tomography |
|
|
| Multidetector cardiac computed tomography |
|
|
More specific is assessment of scar burden and distribution on CMR through late gadolinium enhancement (LGE), where its presence, or absence, can assist in risk stratification of SCD in NICM in the primary prevention setting. The absence of LGE despite impaired LV systolic function carries a much lower annual risk of SCD (0.7%) than LGE and higher ejection fraction (3%, P = 0.007). 12 The distribution of LGE can indicate the aetiology of cardiomyopathy. Subendocardial and transmural scar in coronary territories is more suggestive of IHD. Patchy intramural and epicardial scar are more suggestive of nonischaemic causes, including infiltration, postmyocarditis and cardiac sarcoidosis. Thus, CMR can assist with preprocedural planning for CA, including the decision for an upfront epicardial approach.
Tissue characterisation may also be performed using multidetector cardiac computed tomography (MDCT), where regions of wall thinning and reduced perfusion are surrogate markers of scar. Scar architecture from CMR and MDCT may be integrated into electroanatomic maps to guide CA procedures and increase procedural efficiency. Positron emission tomography (PET) is an additional modality that can diagnose cardiac sarcoidosis through avid myocardial uptake of 18‐fluorodeoxyglucose.
Electrophysiology study (diagnostic, electroanatomic substrate mapping)
Invasive electrophysiology study (EPS) provides both diagnostic insights, through the mode of induction and discrimination between the type of VA, as well as risk stratification. It can also induce nonclinical arrhythmias, which must be interpreted with caution. Programmed electrical stimulation to induce VT during EPS has long been established as a prognostic tool in patients with IHD. On principle, it relies on the reproducibility of sustained VT with the introduction of paced ventricular beats (extrastimuli) to simulate PVCs that initiate reentrant VT. Although probabilistic, a lack of inducible sustained VT is a robust marker in ischaemic cardiomyopathy with negative predictive values of 94% to 96% for future VAs for up to 24 months. 13 Its utility in NICM is less clear, driven by smaller cohort sizes and arrhythmia event rates in previous studies. 14
Electroanatomic substrate mapping is a more advanced form of EPS performed during CA. Multielectrode catheters placed in the ventricles create three‐dimensional reconstructions of the ventricle. Catheter contact with chamber walls allows for the assessment of electrogram voltage, which can then be displayed as a colour‐coded electroanatomic voltage map (Fig. 4). The presence of low voltage, signifying scar, provides prognostic value in ischaemic cardiomyopathy and NICM. 15
Figure 4.

Three‐dimensional electroanatomic substrate mapping. Screenshot of live workflow during electroanatomic substrate mapping of the left ventricle (LV) in a patient with ischaemic cardiomyopathy and previous inferior infarction. (A) Three‐dimensional bipolar voltage map of the LV from the right anterior oblique view with inferior tilt. Large region of inferoseptal low voltage scar denoted by red colour, compared with healthy myocardium with normal voltage denoted by purple colour. Intracardiac echocardiography (ICE) catheter tip (white arrow) positioned in the right ventricle (RV) with ultrasound beam transecting the septum and LV. (B) Corresponding live ICE image demonstrating echobright scar (pink arrow) in the inferoseptal LV with associated wall thinning. MV, mitral valve.
Voltage‐guided substrate mapping can help localise the critical conducting channels forming isthmi for reentrant VT. Voltage mapping identifies bipolar and unipolar scar, representing subendocardial scar or intramural/epicardial scar, respectively. Bipolar voltage mapping can also be performed from an epicardial approach to guide CA of reentrant circuits in the epicardium.
Additional properties of these intracardiac electrograms can provide insights into myocardial tissue properties and assist with VT localisation. Beyond low voltage, the fractionation of electrograms into high frequency, low amplitude, multicomponent signals of prolonged duration denotes delayed conduction through a heterogeneous admixture of viable myocardium and scar. 16 The timing of local signals relative to the onset of the surface ECG QRS complex can also facilitate activation mapping in reentrant and idiopathic VT and PVC to provide targets for ablation.
Tissue diagnostics – endomyocardial biopsy and genetic testing
Endomyocardial biopsy is considered the gold standard for diagnosing several NICM aetiologies, especially in patients presenting with concomitant atrioventricular block including cardiac sarcoidosis and giant cell myocarditis. Detailed phenotypic evaluation is critical to maximising diagnostic yield, especially considering the invasive nature of endomyocardial biopsy and potential complications, including myocardial perforation and irreversible heart block. Yield may be increased when guided by electroanatomic substrate mapping to obtain specimens from scar‐border zones.
Whilst genetic testing has long been established in the diagnosis of channelopathies, its value in patients with VA and NICM has been increasingly recognised. In NICM, genetic testing has profound impacts on management decisions, prognostication, and cascade testing of family members. Most inherited cardiomyopathies have autosomal dominant inheritance, although they may have variable penetrance and expressivity. Thus, a detailed family history, coupled with clinical phenotyping, is crucial in raising the clinician's suspicion. Hypertrophic, arrhythmogenic and Lamin cardiomyopathies are well‐described examples of NICM with genetic associations that can present with VT and an increased risk of SCD.
Management
General principles
Correction of reversible contributors to VAs is imperative prior to more definitive therapies. Electrolyte disturbances can contribute to VAs, especially in idiopathic VF through QT interval prolongation and cardiomyocyte membrane instability. Acute myocardial ischaemia may also be a trigger for PVC, VF and, more rarely, sustained VT. Careful clinical assessment for objective evidence of coronary‐related ischaemia is imperative in expediting revascularisation. Symptoms, ECG changes and troponin elevation can often fail to distinguish between active coronary‐related ischaemia and arrhythmia‐related sequelae.
Management of the underlying cardiomyopathy is another important principle in patients with VA. Those with impaired LV function and severe contributory coronary disease should undergo revascularisation to prevent disease and substrate progression. In patients with NICM, all efforts should be made to phenotype and ensure that reversible pathologies are treated, including cardiac sarcoidosis, giant cell myocarditis and cardiac amyloidosis. Disease processes without specific treatments are worth identifying because of significant prognostic implications, including hypertrophic, arrhythmogenic and Lamin cardiomyopathies.
Guideline‐directed medical therapy for any cardiomyopathy is critical to prevent progressive LV dysfunction, improve prognosis and reduce heart failure–related symptoms. This includes: (i) β‐blockade with agents specifically associated with a mortality benefit; (ii) renin‐angiotensin‐aldosterone axis blockade with an angiotensin‐converting enzyme inhibitor/angiotensin receptor blocker and mineralocorticoid receptor blocker; (iii) consideration for valsartan/sacubitril; (iv) consideration for SGLT2 inhibition even in the absence of type 2 diabetes; (v) consideration for implantation of a cardiac resynchronisation therapy (CRT) device; (vi) consideration for restoration of sinus rhythm in patients with persistent atrial fibrillation.
The use of CRT with VA is particularly relevant. Not infrequently, VA and the substrate that harbours them may be colocalised to the native conduction system (atrioventricular node). CA can result in permanent atrioventricular block and ventricular pacing dependence. In the setting of existing SHD and impaired systolic function, nonphysiologic RV pacing can accelerate biventricular dysfunction, thereby necessitating device upgrade to CRT.
Device therapy
The use of an ICD remains a cornerstone in the prevention of SCD. ICDs can be inserted for the primary prevention of SCD in high‐risk individuals or for the secondary prevention of SCD in whom a cardiac arrest event has already occurred and aborted spontaneously or with resuscitative efforts. Several randomised controlled trials have demonstrated this in ischaemic cardiomyopathy. Early studies highlighted a mortality benefit with primary prevention ICD therapy when compared with optimal medical therapy in patients with a persistently reduced LV ejection fraction ≤35%. 17 However, more recent trials have delineated that ICDs more specifically reduce the risk of cardiac arrest–related death. 18 Primary prevention ICD therapy is now a class I guideline indication for those with ischaemic cardiomyopathy and a persistently reduced LV ejection faction ≤35% despite optimal medical therapy. 10 , 11 However, ICD therapy does not treat the underlying substrate for VA and does not prevent their recurrence, thereby necessitating combination with AADs and/or CA.
ICD therapy for primary prevention in NICM has not been as clearly demonstrated, reflecting the greater heterogeneity within this disease group. Multiple early randomised controlled trials failed to demonstrate any significant mortality benefit when compared with optimal medical therapy or amiodarone. 19 , 20 The more recent DANISH (Danish Study to Assess the Efficacy of ICDs in Patients With Non‐ischemic Systolic trial again did not demonstrate an overall mortality benefit from ICD therapy; however, it did show a significant reduction in SCD (4.3% vs 8.4%) in younger patients. This could be explained by improvements in guideline‐directed medical therapy for cardiomyopathy. 21 ICD insertion for secondary prevention is a class I indication in current guidelines.
Antiarrhythmic drugs
A wide range of AAD may be used to manage VA, with differing mechanisms and efficacy depending on the underlying aetiology. AAD exert their effects through selective ion channel inhibition in the cardiomyocyte cell membrane and adrenoceptor modulation, thereby influencing action potential duration and repolarisation. Their specific mechanisms are best described using the conventional Vaughn‐Williams classification system (Table 2), although overlap exists between their effects on ion channels.
Table 2.
Antiarrhythmic drugs and their properties
| Name | Class | Effect | Use | Caution |
|---|---|---|---|---|
| Quinidine | Ia |
Na+ blocker K+ blocker |
First‐line for recurrent VA in Brugada syndrome | Gastrointestinal disturbance, myelosuppression, drug‐induced lupus, hepatotoxicity |
| Lignocaine | Ib | Na+ blocker | Second‐line intravenous agent for sustained VT in SHD. Short half‐life (8 min) | Neurotoxicity, hepatotoxicity, myocardial depressant |
| Mexiletine | Ib | Na+ blocker | Third‐line oral agent for recurrent VT in SHD. Oral equivalent of lignocaine | Neurotoxicity, gastrointestinal disturbance |
| Flecainide | Ic | Na+ blocker | Idiopathic PVC and VT in absence of structural heart disease | Risk of pro‐arrhythmia by facilitating re‐entry |
| Metoprolol | II | β‐adrenoceptor blocker | Idiopathic PVC/VT | Bradycardia, hypotension, fatigue, sleep disturbance, bronchospasm |
| Esmolol | II | β‐adrenoceptor blocker | Intravenous agent for sustained VT. Short half‐life (9 min) | Bradycardia, hypotension, bronchospasm, heart failure |
| Nadolol | II | β‐adrenoceptor blocker | Oral, long‐acting, first‐line agent for LQTS and CPVT | Bradycardia, hypotension, fatigue, sleep disturbance, bronchospasm |
| Amiodarone | III |
Multiple effects Dominant K+ blocker |
First‐line for sustained VT, especially in SHD. Can be given oral or IV | Multiple toxicities (thyroid, liver, pulmonary, corneal, cutaneous), QT prolongation |
| Sotalol | III |
K+ blocker β‐adrenoceptor blocker |
Considered first‐line oral agent in SHD | Bradycardia, fatigue, bronchospasm, QT prolongation and pro‐arrhythmia |
|
Diltiazem Verapamil |
IV | Ca2+ blocker | Idiopathic PVC/VT, bundle branch re‐entry (fascicular) VT | Bradycardia, hypotension, peripheral oedema, gastrointestinal disturbance |
CPVT, catecholaminergic polymorphic ventricular tachycardia; IV, intravenously; LQTS, long QT syndrome; PVC, premature ventricular complex; SHD, structural heart disease; VA, ventricular arrhythmias; VT, ventricular tachycardia.
Whilst AAD are considered first‐line therapy by reducing VA burden, ICD shocks, and improving quality of life, there is growing recognition of their limitations. In idiopathic VA, β‐blockers (e.g. metoprolol) and nondihydropyridine calcium channel blockers (e.g. diltiazem and verapamil) are common first‐line agents, however they can be limited by side effects (Table 2). The sodium channel blocker flecainide can be used in select circumstances provided exclusion of SHD due to the pro‐arrhythmic risk of VT and VF.
In SHD, Class III agents such as sotalol and amiodarone are most frequently used for VT. Uniquely, sotalol provides both β‐adrenoceptor and potassium channel blockade with resultant Class III anti‐arrhythmic effects. Despite this, sotalol does not offer the same mortality benefit of cardiomyopathy‐specific β‐blockers. Its proarrhythmic effects arise owing to QT prolongation, exacerbated in renal failure due to its renal excretion.
Whilst amiodarone is more effective in the control of VA, its dose‐ and time‐dependent toxicities limit long‐term use, especially in younger patients. These include liver dysfunction, pulmonary fibrosis, thyrotoxicosis, corneal deposits, peripheral neuropathy and skin discolouration. When administered intravenously, it carries the risk of thrombophlebitis, necessitating central venous access. Moreover, amiodarone can cause VT to become slower and more hemodynamically tolerated acutely. As a result, these arrhythmias can fall below the detection zones of ICD, which can lead to subacute heart failure and hospitalisation.
AAD are crucial in the management of channelopathies despite the relative paucity of multicentre data. In LQTS, QT‐prolonging agents must be avoided, which include certain AAD, antibiotics and psychotropic drugs. β‐Blockade remains the first‐line therapy in LQTS in those with significant QT prolongation and recurrent syncope. Nadolol, a long‐acting nonselective β‐blocker, has been found to be the most effective agent when compared with propranolol and metoprolol. 22 Nadolol also has efficacy in reducing arrhythmic events in CPVT. In Brugada syndrome, sodium channel blockers should be avoided because of the risk of potentiating arrhythmic events. Avoidance of hot temperatures and fever can also reduce the risk of sudden cardiac arrest. Quinidine can be beneficial in patients with recurrent arrhythmias in Brugada syndrome.
Catheter ablation
Over the past 2 decades, there has been a national and global trend of increasing utilisation of CA for VA, with greater growth compared with CA for atrial fibrillation and percutaneous coronary intervention in Australia (18% vs 12.7% vs 1.3% per year). 23 The vast heterogeneity between idiopathic VA, compared with SHD, underpins the current evidence on procedural outcomes and safety. Moreover, there has been a trend towards the use of CA as first‐line therapy, especially for idiopathic VA (Supporting Information Video S1).
The vast majority of idiopathic VA arise from the RV and LV outflow tracts. Ablation success rates exceed 80% with <1% risk of procedural complications in experienced centres. 24 More rarely, VA can arise from the LV papillary muscles and RV moderator band (Fig. 1A). These intracavitary structures can be challenging for ablation, because of catheter instability, difficult mapping of multiple arrhythmia exit sites and deep, intramural foci, resulting in lower success rates. Approximately 12% of idiopathic VAs can arise from epicardial regions, which can be difficult to access percutaneously for CA because of overlying epicardial adipose tissue and proximity with coronary arteries.
The outcomes of patients with SHD are significantly different owing to the presence of scar, which harbours channels that support multiple arrhythmias. Thus, more extensive ablation throughout the scar is often performed beyond targeting the clinical VT alone. Various strategies have been proposed, with the most widely adopted being scar homogenisation – ablation throughout regions of scar to abolish all possible channels that may give rise to future VAs. Acute procedural success is defined by the inability to induce any VA following ablation and is the strongest available predictor for long‐term arrhythmia recurrence. Nonetheless, its correlation with VA recurrence is limited because of the suppressive effects of general anaesthesia on VA inducibility.
Scar homogenisation provides the greatest acute and long‐term arrhythmia freedom. Despite this, patients with NICM have a higher VA recurrence and lower arrhythmia‐free survival when compared with ischaemic cardiomyopathy, regardless of the ablation strategy adopted. This is likely a reflection of the heterogeneity of NICM pathologies, progression of underlying substrate and deeper, more inaccessible scar when targeted for CA.
Multiple randomised trials have now been conducted on the utility of ablation; however, study designs and patient populations significantly differ (Table 3). Early trials failed to show a significant mortality benefit, although findings were relatively limited by the use of all‐cause mortality in the primary end points. More recent trials have shown reductions in VT recurrence and device shocks, potentially a reflection of improving mapping and ablation technologies. Beyond arrhythmia recurrence, CA has a significant impact on reducing arrhythmia burden, 34 reducing/discontinuing AAD and improving quality of life and cost‐effectiveness. 35 CA is also shown to be effective in the management of electrical storm, with freedom from recurrent electrical storm in >90% in patients with acute postablation arrhythmia noninducibility. 36
Table 3.
Randomised controlled trials of catheter ablation for VT
| Study | Population | Study design | Findings | Insights |
|---|---|---|---|---|
|
SMASH VT (2007) Reddy et al. 25 (n = 128) |
|
ICD + ablation (64) vs ICD only (64) No AAD prior to 1° end point 24 months follow‐up |
1°: survival free of any appropriate ICD therapy
2°:
|
|
|
VTACH (2010) Kuck et al. 26 (n = 110) |
|
Ablation + ICD (52) vs ICD only (55) Amiodarone used – 26% vs 31% 22.5 ± 9 months follow‐up |
1°: time to recurrence of sustained VT/VF (months)
2°:
|
|
|
CALYPSO (2014) Al‐Khatib et al. 27 (n = 27) |
|
Ablation (13) vs ICD + AAD (14) n = 216 excluded after screening 6 months follow‐up AAD – amiodarone/sotalol firstline, mexiletine, ranolazine and dofetilide second line |
|
|
|
VANISH (2016) Sapp et al. 28 (n = 259) |
|
Escalated AAD only (127) vs AAD + ablation (132) 27.9 ± 17.1 months follow‐up AAD – amiodarone first line, mexiletine second line |
1°: composite of death, appropriate ICD shock and storm
2°:
|
|
|
SMS (2017) Kuck et al. 29 (n = 111) |
|
ICD + ablation (54) vs ICD only (57) 26.4 ± 12 months follow‐up Amiodarone used – 26% vs 32% at 2 years follow‐up |
1°: time to first recurrence of VT/VF, P = 0.84 2°:
|
|
|
BERLIN VT (2020) Willems et al. 30 (n = 159) |
|
Ablation before ICD (76) vs deferred ablation (after 3 shocks) (83) 12 months follow‐up Amiodarone used – 41% vs 27% Recruitment terminated early because of futility margin being reached on interim analysis |
1°: composite of death or unplanned cardiac hospitalisation
2°:
|
|
|
PARTITA (2022) Della Bella et al. 31 (n = 47) |
|
Ablation after ICD shock (23) vs standard therapy (including AAD) (24) 24 months follow‐up Amiodarone used – 5% vs 21% |
1°: composite of death or heart failure hospitalisation
2°:
|
|
|
SURVIVE VT (2022) Arenal et al. 32 (n = 144) |
|
Ablation (71) vs AAD (73) 24 months follow‐up |
1°: composite of cardiac death, appropriate ICD shock, heart failure hospitalisation or severe treatment‐related complication
2°:
|
|
|
PAUSE SCD Tung et al. 33 (n = 121) |
|
Ablation vs medical therapy 31.3 (20.1–40) months follow‐up Amiodarone used – 28.6% vs 32.8% |
1°: composite of VT recurrence, cardiac hospitalisation or death
2°:
|
|
Values in parentheses are 95% confidence intervals. 1°, primary; 2°, secondary; AAD, antiarrhythmic drug; ARVC, arrhythmic right ventricular cardiomyopathy; HR, hazard ratio; ICD, implantable cardioverter‐defibrillator; ICM, ischemic cardiomyopathy; LVEF, left ventricular ejection fraction; NICM, nonischemic cardiomyopathy; SHD, structural heart disease; VF, ventricular fibrillation; VT, ventricular tachycardia.
In real‐world practice, the perceived invasive nature and procedural risks of CA may contribute to delays in referral by treating physicians. Earlier referral for CA has been associated with improved outcomes, including reduced VA recurrence and greater recurrence‐free survival. The exact definition of early versus late referral differs between studies, with late referral defined as two or more episodes of VT or failure of more than one AAD. The presence of syncope, nonsustained or sustained VT on Holter monitoring, and the presence of SHD should prompt earlier specialist or hospital referral.
Stereotactic cardiac radioablation
An emerging therapy for VT in SHD is the use of radiation therapy on the ventricular myocardium in a noninvasive manner. After comprehensive invasive or noninvasive electroanatomic mapping and imaging, radiation therapy is delivered in a similar manner to that in cancer treatment, with patients remaining awake and ambulating immediately posttreatment. Suitable patients may include those with VT refractory to multiple CA procedures, those in incessant electrical storm or those with limited endocardial access (e.g. metallic mitral and aortic valve replacements) or prohibitively high risk for an invasive CA procedure. Early data have shown significant short‐term reductions in VT burden and ICD shocks with minimal effects on surrounding structures. 37 , 38 However, long‐term sustained VT recurrence remains high at >50% at 6 months. 39 Several randomised clinical trials are underway to corroborate these findings.
Conclusion
VAs are a diverse group of cardiac disorders that are intimately linked to underlying disease processes. Understanding their probable mechanism and relevant anatomy is critical in influencing investigative pathways and navigating the breadth of management decisions for patients. In particular, the assessment for underlying myocardial substrate for reentrant VT with multiple modalities carries significant prognostic value. CA of VA is one well‐established treatment modality that can offer cure and improve symptoms and long‐term outcomes. Novel technologies and progressive refinement of existing techniques will continue the trajectory to improving procedural safety and efficacy.
Supporting information
Video S1. Live workflow during catheter ablation and three‐dimensional electroanatomic mapping. Videoclip of live workflow during catheter ablation of an idiopathic ventricular arrhythmias (VAs) arising from the left ventricular (LV) summit, part of the LV outflow tract. Electroanatomic map with posteroanterior view (left panel) demonstrates localisation of the arrhythmia to the LV summit region (red shading) based on activation mapping. Contact force‐sensing ablation catheter (red tip) positioned at this region with force vector (grey arrow with green tip) directing 20 to 30 g of force from the catheter tip to the endocardium. Live intracardiac echocardiography (ICE) (ultrasound beam with green border) transecting this region, corresponding with right hand panel with live ICE image. On ICE image, ablation catheter (white arrow) with tip positioned at LV summit and echobright ablation lesion formation during active radiofrequency ablation (red arrow).
Acknowledgements
Open access publishing facilitated by The University of Sydney, as part of the Wiley ‐ The University of Sydney agreement via the Council of Australian University Librarians.
Funding: Dr Kumar is supported by the NSW Early‐Mid Career Fellowship. He has received research grants from Abbott Medical and Biotronik. Dr Bhaskaran and Dr Silva are supported by the National Health and Medical Research Council Postgraduate Scholarship.
Conflict of interest: Dr Kumar has received honoraria from Biosense Webster, Abbott Medical, Biotronik and Sanofi Aventis.
References
- 1. Hayashi M, Shimizu W, Albert CM. The spectrum of epidemiology underlying sudden cardiac death. Circ Res 2015; 116: 1887–906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Stevenson WG, Friedman PL, Sager PT, Saxon LA, Kocovic D, Harada T et al. Exploring postinfarction reentrant ventricular tachycardia with entrainment mapping. J Am Coll Cardiol 1997; 29: 1180–9. [DOI] [PubMed] [Google Scholar]
- 3. Oloriz T, Silberbauer J, Maccabelli G, Mizuno H, Baratto F, Kirubakaran S et al. Catheter ablation of ventricular arrhythmia in nonischemic cardiomyopathy: anteroseptal versus inferolateral scar sub‐types. Circ Arrhythm Electrophysiol 2014; 7: 414–23. [DOI] [PubMed] [Google Scholar]
- 4. Haissaguerre M, Shah DC, Jais P, Shoda M, Kautzner J, Arentz T et al. Role of Purkinje conducting system in triggering of idiopathic ventricular fibrillation. Lancet 2002; 359: 677–8. [DOI] [PubMed] [Google Scholar]
- 5. Nademanee K, Veerakul G, Chandanamattha P, Chaothawee L, Ariyachaipanich A, Jirasirirojanakorn K et al. Prevention of ventricular fibrillation episodes in Brugada syndrome by catheter ablation over the anterior right ventricular outflow tract epicardium. Circulation 2011; 123: 1270–9. [DOI] [PubMed] [Google Scholar]
- 6. Ataklte F, Erqou S, Laukkanen J, Kaptoge S. Meta‐analysis of ventricular premature complexes and their relation to cardiac mortality in general populations. Am J Cardiol 2013; 112: 1263–70. [DOI] [PubMed] [Google Scholar]
- 7. Lin CY, Chang SL, Lin YJ, Lo LW, Chung FP, Chen YY et al. Long‐term outcome of multiform premature ventricular complexes in structurally normal heart. Int J Cardiol 2015; 180: 80–5. [DOI] [PubMed] [Google Scholar]
- 8. Dukes JW, Dewland TA, Vittinghoff E, Mandyam MC, Heckbert SR, Siscovick DS et al. Ventricular ectopy as a predictor of heart failure and death. J Am Coll Cardiol 2015; 66: 101–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Del Carpio MF, Syed FF, Noheria A, Cha YM, Friedman PA, Hammill SC et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J Cardiovasc Electrophysiol 2011; 22: 791–8. [DOI] [PubMed] [Google Scholar]
- 10. Al‐Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2018; 72: 1677–749. [DOI] [PubMed] [Google Scholar]
- 11. Priori SG, Blomstrom‐Lundqvist C. 2015 European Society of Cardiology Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death summarized by co‐chairs. Eur Heart J 2015; 36: 2757–9. [DOI] [PubMed] [Google Scholar]
- 12. Di Marco A, Brown PF, Bradley J, Nucifora G, Claver E, de Frutos F et al. Improved risk stratification for ventricular arrhythmias and sudden death in patients with nonischemic dilated cardiomyopathy. J Am Coll Cardiol 2021; 77: 2890–905. [DOI] [PubMed] [Google Scholar]
- 13. De Ferrari GM, Rordorf R, Frattini F, Petracci B, De Filippo P, Landolina M. Predictive value of programmed ventricular stimulation in patients with ischaemic cardiomyopathy: implications for the selection of candidates for an implantable defibrillator. Europace 2007; 9: 1151–7. [DOI] [PubMed] [Google Scholar]
- 14. Grimm W, Hoffmann J, Menz V, Luck K, Maisch B. Programmed ventricular stimulation for arrhythmia risk prediction in patients with idiopathic dilated cardiomyopathy and nonsustained ventricular tachycardia. J Am Coll Cardiol 1998; 32: 739–45. [DOI] [PubMed] [Google Scholar]
- 15. Dinov B, Schratter A, Schirripa V, Fiedler L, Bollmann A, Rolf S et al. Procedural outcomes and survival after catheter ablation of ventricular tachycardia in relation to Electroanatomical substrate in patients with nonischemic‐dilated cardiomyopathy: the role of unipolar voltage mapping. J Cardiovasc Electrophysiol 2015; 26: 985–93. [DOI] [PubMed] [Google Scholar]
- 16. Cassidy DM, Vassallo JA, Buxton AE, Doherty JU, Marchlinski FE, Josephson ME. The value of catheter mapping during sinus rhythm to localize site of origin of ventricular tachycardia. Circulation 1984; 69: 1103–10. [DOI] [PubMed] [Google Scholar]
- 17. Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002; 346: 877–83. [DOI] [PubMed] [Google Scholar]
- 18. Steinbeck G, Andresen D, Seidl K, Brachmann J, Hoffmann E, Wojciechowski D et al. Defibrillator implantation early after myocardial infarction. N Engl J Med 2009; 361: 1427–36. [DOI] [PubMed] [Google Scholar]
- 19. Strickberger SA, Hummel JD, Bartlett TG, Frumin HI, Schuger CD, Beau SL et al. Amiodarone versus implantable cardioverter‐defibrillator: randomized trial in patients with nonischemic dilated cardiomyopathy and asymptomatic nonsustained ventricular tachycardia – AMIOVIRT. J Am Coll Cardiol 2003; 41: 1707–12. [DOI] [PubMed] [Google Scholar]
- 20. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R et al. Amiodarone or an implantable cardioverter‐defibrillator for congestive heart failure. N Engl J Med 2005; 352: 225–37. [DOI] [PubMed] [Google Scholar]
- 21. Kober L, Thune JJ, Nielsen JC, Haarbo J, Videbæk L, Korup E et al. Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med 2016; 375: 1221–30. [DOI] [PubMed] [Google Scholar]
- 22. Chockalingam P, Crotti L, Girardengo G, Johnson JN, Harris KM, van der Heijden JF et al. Not all beta‐blockers are equal in the management of long QT syndrome types 1 and 2: higher recurrence of events under metoprolol. J Am Coll Cardiol 2012; 60: 2092–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Anderson RD, Lee G, Prabhu M, Patrick CJ, Trivic I, Campbell T et al. Ten‐year trends in catheter ablation for ventricular tachycardia vs other interventional procedures in Australia. J Cardiovasc Electrophysiol 2019; 30: 2353–61. [DOI] [PubMed] [Google Scholar]
- 24. Ling Z, Liu Z, Su L, Zipunnikov V, Wu J, du H et al. Radiofrequency ablation versus antiarrhythmic medication for treatment of ventricular premature beats from the right ventricular outflow tract: prospective randomized study. Circ Arrhythm Electrophysiol 2014; 7: 237–43. [DOI] [PubMed] [Google Scholar]
- 25. Reddy VY, Reynolds MR, Neuzil P, Richardson AW, Taborsky M, Jongnarangsin K et al. Prophylactic catheter ablation for the prevention of defibrillator therapy. N Engl J Med 2007; 357: 2657–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Kuck KH, Schaumann A, Eckardt L, Willems S, Ventura R, Delacrétaz E et al. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): a multicentre randomised controlled trial. Lancet 2010; 375: 31–40. [DOI] [PubMed] [Google Scholar]
- 27. Al‐Khatib SM, Daubert JP, Anstrom KJ, Daoud EG, Gonzalez M, Saba S et al. Catheter ablation for ventricular tachycardia in patients with an implantable cardioverter defibrillator (CALYPSO) pilot trial. J Cardiovasc Electrophysiol 2015; 26: 151–7. [DOI] [PubMed] [Google Scholar]
- 28. Sapp JL, Wells GA, Parkash R, Stevenson WG, Blier L, Sarrazin JF et al. Ventricular tachycardia ablation versus escalation of antiarrhythmic drugs. N Engl J Med 2016; 375: 111–21. [DOI] [PubMed] [Google Scholar]
- 29. Kuck KH, Tilz RR, Deneke T, Hoffmann BA, Ventura R, Hansen PS et al. Impact of substrate modification by catheter ablation on implantable cardioverter‐defibrillator interventions in patients with unstable ventricular arrhythmias and coronary artery disease: results from the multicenter randomized controlled SMS (substrate modification study). Circ Arrhythm Electrophysiol 2017; 10: e004422. [DOI] [PubMed] [Google Scholar]
- 30. Willems S, Tilz RR, Steven D, Kääb S, Wegscheider K, Gellér L et al. Preventive or deferred ablation of ventricular tachycardia in patients with ischemic cardiomyopathy and implantable defibrillator (BERLIN VT): a multicenter randomized trial. Circulation 2020; 141: 1057–67. [DOI] [PubMed] [Google Scholar]
- 31. Della Bella P, Baratto F, Vergara P, Bertocchi P, Santamaria M, Notarstefano P et al. Does timing of ventricular tachycardia ablation affect prognosis in patients with an implantable cardioverter defibrillator? Results from the multicenter randomized PARTITA trial. Circulation 2022; 145: 1829–38. [DOI] [PubMed] [Google Scholar]
- 32. Arenal A, Avila P, Jimenez‐Candil J, Tercedor L, Calvo D, Arribas F et al. Substrate ablation vs antiarrhythmic drug therapy for symptomatic ventricular tachycardia. J Am Coll Cardiol 2022; 79: 1441–53. [DOI] [PubMed] [Google Scholar]
- 33. Tung R, Xue Y, Chen M, Jiang C, Shatz DY, Besser SA et al. First‐line catheter ablation of monomorphic ventricular tachycardia in cardiomyopathy concurrent with defibrillator implantation: the PAUSE‐SCD randomized trial. Circulation 2022; 145: 1839–49. [DOI] [PubMed] [Google Scholar]
- 34. Bennett R, Turnbull S, Kotake Y, Campbell T, Kumar S. Ventricular arrhythmia burden as a marker of success following catheter ablation of ventricular arrhythmias in patients with structural heart disease. Korean Circ J 2021; 51: 455–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Coyle K, Coyle D, Nault I, Parkash R, Healey JS, Gray CJ et al. Cost effectiveness of ventricular tachycardia ablation versus escalation of antiarrhythmic drug therapy: the VANISH trial. JACC Clin Electrophysiol 2018; 4: 660–8. [DOI] [PubMed] [Google Scholar]
- 36. Vergara P, Tung R, Vaseghi M, Brombin C, Frankel D, di Biase L et al. Successful ventricular tachycardia ablation in patients with electrical storm reduces recurrences and improves survival. Heart Rhythm 2018; 15: 48–55. [DOI] [PubMed] [Google Scholar]
- 37. Cuculich PS, Schill MR, Kashani R, Mutic S, Lang A, Cooper D et al. Noninvasive cardiac radiation for ablation of ventricular tachycardia. N Engl J Med 2017; 377: 2325–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Robinson CG, Samson PP, Moore KMS, Hugo GD, Knutson N, Mutic S et al. Phase I/II trial of electrophysiology‐guided noninvasive cardiac radioablation for ventricular tachycardia. Circulation 2019; 139: 313–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Kovacs B, Mayinger M, Schindler M, Steffel J, Andratschke N, Saguner AM. Stereotactic radioablation of ventricular arrhythmias in patients with structural heart disease ‐ a systematic review. Radiother Oncol 2021; 162: 132–9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video S1. Live workflow during catheter ablation and three‐dimensional electroanatomic mapping. Videoclip of live workflow during catheter ablation of an idiopathic ventricular arrhythmias (VAs) arising from the left ventricular (LV) summit, part of the LV outflow tract. Electroanatomic map with posteroanterior view (left panel) demonstrates localisation of the arrhythmia to the LV summit region (red shading) based on activation mapping. Contact force‐sensing ablation catheter (red tip) positioned at this region with force vector (grey arrow with green tip) directing 20 to 30 g of force from the catheter tip to the endocardium. Live intracardiac echocardiography (ICE) (ultrasound beam with green border) transecting this region, corresponding with right hand panel with live ICE image. On ICE image, ablation catheter (white arrow) with tip positioned at LV summit and echobright ablation lesion formation during active radiofrequency ablation (red arrow).